

Does Frontal Recess Cell Variation Associate with the Development of Frontal Sinusitis? A Narrative Review
 , , ,
, , , 
Abstract
1. Introduction
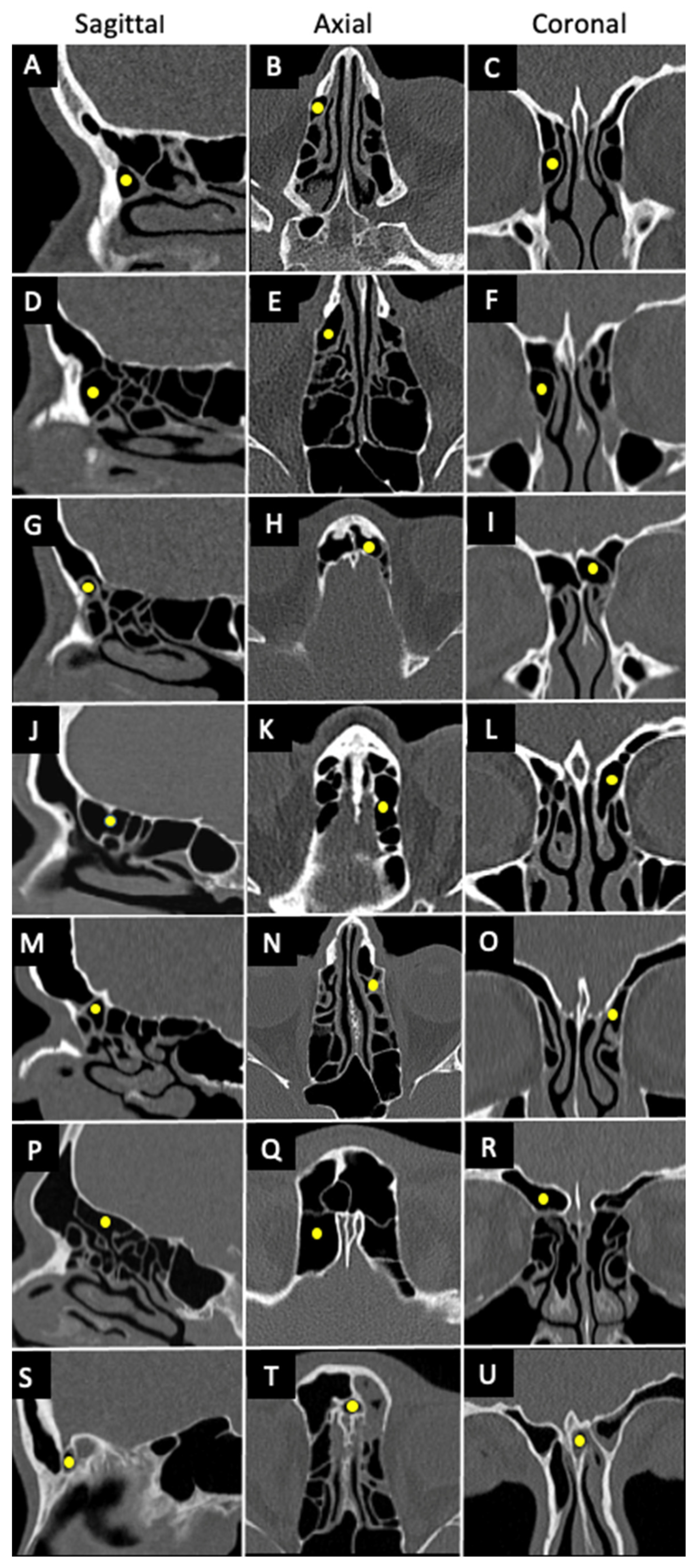
1.1. Frontal Sinus Anatomy
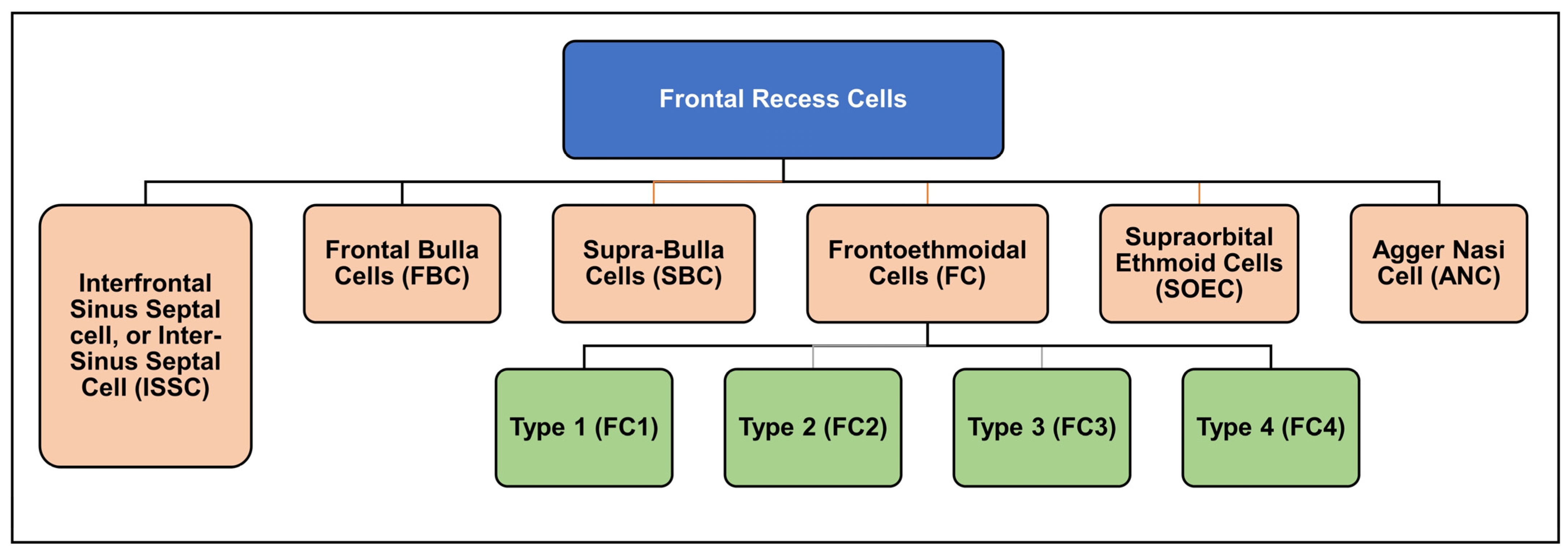
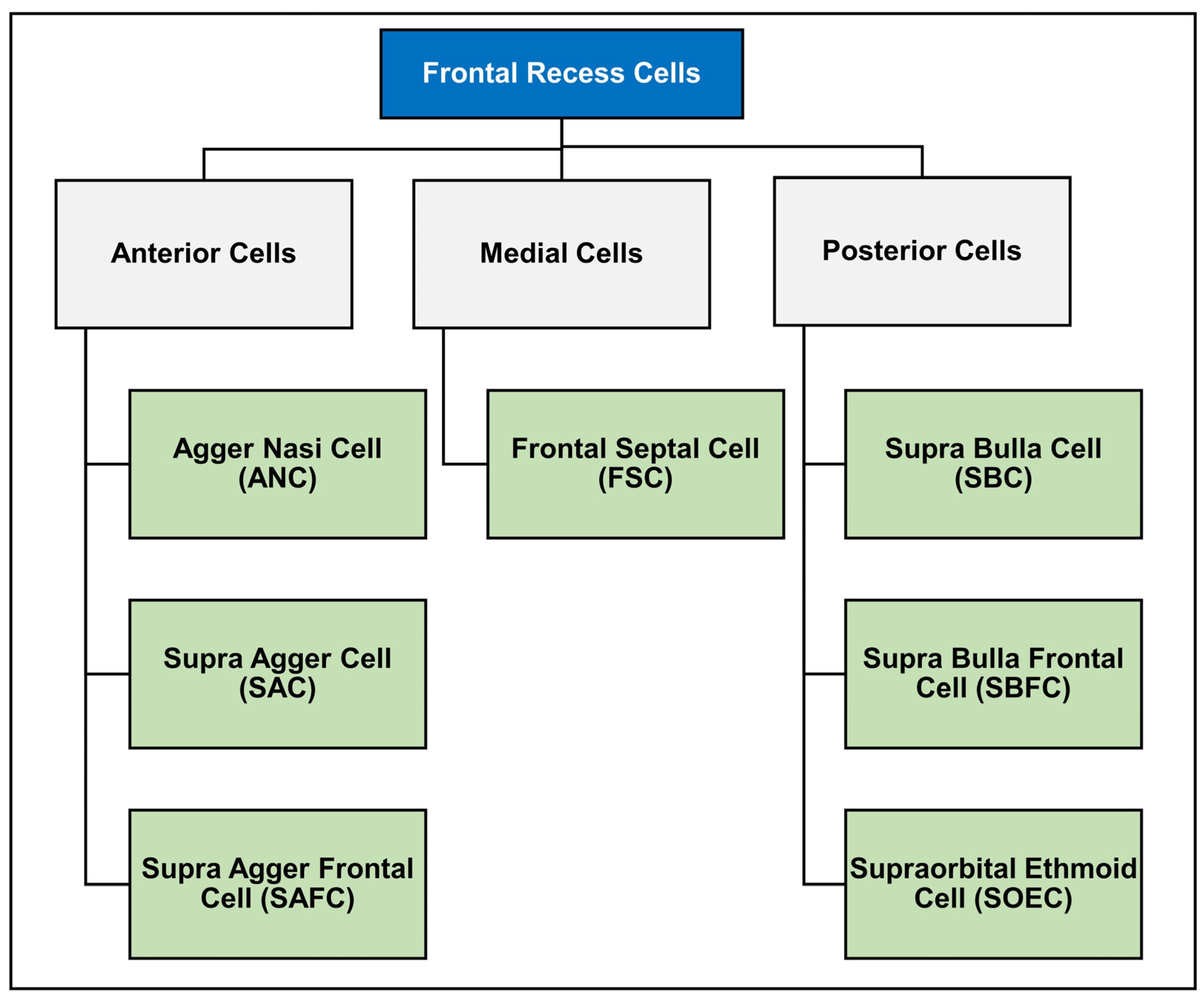
1.2. The History of Frontal Recess Cell Classification
1.3. International Frontal Sinus Anatomy Classification (IFAC)
2. Frontal Recess Cells’ Prevalence in Different Populations
3. Frontal Recess Cells and Their Association with Sinusitis
Other Factors Associated with Sinusitis
4. Surgical Approaches with Anatomical Variations in Frontal Sinus Anatomy
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Erskine, S.E.; Verkerk, M.M.; Notley, C.; Williamson, I.G.; Philpott, C.M. Chronic Rhinosinusitis: Patient Experiences of Primary and Secondary Care–A Qualitative Study. Clin. Otolaryngol. 2016, 41, 8–14. [Google Scholar] [CrossRef]
- Fokkens, W.J.; Lund, V.J.; Hopkins, C.; Hellings, P.W.; Kern, R.; Reitsma, S.; Toppila-Salmi, S.; Bernal-Sprekelsen, M.; Mullol, J.; Alobid, I.; et al. European Position Paper on Rhinosinusitis and Nasal Polyps 2020. Rhinology 2020, 58, 1–464. [Google Scholar] [CrossRef] [PubMed]
- DeConde, A.S.; Smith, T.L. Outcomes after Frontal Sinus Surgery: An Evidence-Based Review. Otolaryngol. Clin. N. Am. 2016, 49, 1019–1033. [Google Scholar] [CrossRef] [PubMed]
- Korban, Z.R.; Casiano, R.R. Standard Endoscopic Approaches in Frontal Sinus Surgery: Technical Pearls and Approach Selection. Otolaryngol. Clin. N. Am. 2016, 49, 989–1006. [Google Scholar] [CrossRef] [PubMed]
- El-Anwar, M.W.; Khazbak, A.O.; Eldib, D.B.; Algazzar, H.Y. Anterior Ethmoidal Artery: A Computed Tomography Analysis and New Classifications. J. Neurol. Surg. Part B Skull Base 2020, 82, e259–e267. [Google Scholar] [CrossRef] [PubMed]
- Ko, Y.B.; Kim, M.G.; Jung, Y.G. The Anatomical Relationship between the Anterior Ethmoid Artery, Frontal Sinus, and Intervening Air Cells; Can the Artery Be Useful Landmark. Korean J. Otorhinolaryngol. Head Neck Surg. 2014, 57, 687–691. [Google Scholar] [CrossRef]
- Wormald, P.; Hoseman, W.; Callejas, C.; Weber, R.K.; Kennedy, D.W.; Citardi, M.J.; Senior, B.A.; Smith, T.L.; Hwang, P.H.; Orlandi, R.R. The International Frontal Sinus Anatomy Classification (IFAC) and Classification of the Extent of Endoscopic Frontal Sinus Surgery (EFSS). In International Forum of Allergy & Rhinology; Wiley Online Library: Hoboken, NJ, USA, 2016; Volume 6, pp. 677–696. [Google Scholar]
- Gotlib, T.; Kołodziejczyk, P.; Kuźmińska, M.; Bobecka-Wesołowska, K.; Niemczyk, K. Three-dimensional Computed Tomography Analysis of Frontoethmoidal Cells: A Critical Evaluation of the International Frontal Sinus Anatomy Classification (IFAC). Clin. Otolaryngol. 2019, 44, 954–960. [Google Scholar] [CrossRef]
- Van Alyea, O.E. Frontal Cells: An Anatomic Study of These Cells with Consideration of Their Clinical Significance. Arch. Otolaryngol. 1941, 34, 11–23. [Google Scholar] [CrossRef]
- Shokri, A.; Faradmal, M.J.; Hekmat, B. Correlations between Anatomical Variations of the Nasal Cavity and Ethmoidal Sinuses on Cone-Beam Computed Tomography Scans. Imaging Sci. Dent. 2019, 49, 103–113. [Google Scholar] [CrossRef]
- Drake, R.; Vogl, A.W.; Mitchell, A.W.M. Grays Anatomy for Students, 3rd ed.; Churchill Livingstone: London, UK, 2014; ISBN 978-0-7020-5131-9. [Google Scholar]
- Lund, V.J.; Stammberger, H.; Fokkens, W.J.; Bernal-Sprekelsen, M. European Position Paper on the Anatomical Terminology of the Internal Nose and Paranasal Sinuses. Rhinol. Suppl. 2014, 24, 1–34. [Google Scholar]
- Bent, J.P.; Guilty-Siller, G.; Kuhn, F.A. The frontal Cell as a Cause of Frontal Sinus Obstruction. Am. J. Rhinol. 1994, 8, 185–192. [Google Scholar] [CrossRef]
- Kuhn, F.A. Chronic frontal sinusitis: The endoscopic frontal recess approach. Oper. Tech. Otolaryngol. Head Neck Surg. 1996, 7, 222–229. [Google Scholar] [CrossRef]
- Wormald, P.-J. Three-Dimensional Building Block Approach to Understanding the Anatomy of the Frontal Recess and Frontal Sinus. Oper. Tech. Otolayngol. Head Neck Surg. 2006, 17, 2–5. [Google Scholar] [CrossRef]
- Pianta, L.; Ferrari, M.; Schreiber, A.; Mattavelli, D.; Lancini, D.; Bottazzoli, M.; Maroldi, R.; Rodella, L.F.; Ravanelli, M.; Nicolai, P. Agger-Bullar Classification (ABC) of the Frontal Sinus Drainage Pathway: Validation in a Preclinical Setting. Int. Forum Allergy Rhinol. 2016, 6, 981–989. [Google Scholar] [CrossRef] [PubMed]
- Villarreal, R.; Wrobel, B.B.; Macias-Valle, L.F.; Davis, G.E.; Prihoda, T.J.; Luong, A.U.; McMains, K.C.; Weitzel, E.K.; Yao, W.C.; Brunworth, J. International Assessment of Inter-and Intrarater Reliability of the International Frontal Sinus Anatomy Classification System. In International Forum of Allergy & Rhinology; Wiley Online Library: Hoboken, NJ, USA, 2019; Volume 9, pp. 39–45. [Google Scholar]
- Sommer, F.; Hoffmann, T.K.; Harter, L.; Döscher, J.; Kleiner, S.; Lindemann, J.; Leunig, A. Incidence of Anatomical Variations According to the International Frontal Sinus Anatomy Classification (IFAC) and Their Coincidence with Radiological Sings of Opacification. Eur. Arch. Oto-Rhino-Laryngol. 2019, 276, 3139–3146. [Google Scholar] [CrossRef] [PubMed]
- Drake, R.L. Terminologia Anatomica—International Anatomical Terminology; Thieme Medical Publishers, Inc.: New York, NY, USA, 2011. [Google Scholar]
- Dassi, C.S.; Demarco, F.R.; Mangussi-Gomes, J.; Weber, R.; Balsalobre, L.; Stamm, A.C. The Frontal Sinus and Frontal Recess: Anatomical, Radiological and Surgical Concepts. Int. Arch. Otorhinolaryngol. 2020, 24, 364–375. [Google Scholar] [CrossRef] [PubMed]
- Howser, L.A.; Jones, A.J.; Sreenath, S.B.; Ting, J.Y.; Illing, E.A. Frontal Sinus Anatomy Variations in Race and Sex Using the International Frontal Sinus Anatomy Classification. Ear Nose Throat J. 2023, 1–8, 01455613231185701. [Google Scholar] [CrossRef]
- Köksal, A.; Tuğtağ Demir, B.; Çankal, F. Change of Frontal Sinus in Age of According to the International Frontal Sinus Anatomy Classification. Acta Radiol. 2023, 64, 2424–2430. [Google Scholar] [CrossRef]
- Nofal, A.A.B.; El-Anwar, M.W. Frontal Recess Cells in International Frontal Sinus Anatomy Classification (IFAC); Prevalence, Infection Incidence, and Relation to Frontal Sinus Infection in Chronic Sinusitis Patients. Indian J. Otolaryngol. Head Neck Surg. 2022, 74, 4748–4755. [Google Scholar] [CrossRef]
- Fawzi, N.E.A.; Lazim, N.M.; Aziz, M.E.; Mohammad, Z.W.; Abdullah, B. The Prevalence of Frontal Cell Variants According to the International Frontal Sinus Anatomy Classification and Their Associations with Frontal Sinusitis. Eur. Arch. Oto-Rhino-Laryngol. 2022, 279, 765–771. [Google Scholar] [CrossRef]
- Seth, N.; Kumar, J.; Garg, A.; Singh, I.; Meher, R. Computed Tomographic Analysis of the Prevalence of International Frontal Sinus Anatomy Classification Cells and Their Association with Frontal Sinusitis. J. Laryngol. Otol. 2020, 134, 887–894. [Google Scholar] [CrossRef] [PubMed]
- Tran, L.V.; Ngo, N.H.; Psaltis, A.J. A Radiological Study Assessing the Prevalence of Frontal Recess Cells and the Most Common Frontal Sinus Drainage Pathways. Am. J. Rhinol. Allergy 2019, 33, 323–330. [Google Scholar] [CrossRef] [PubMed]
- Choby, G.; Thamboo, A.; Won, T.; Kim, J.; Shih, L.C.; Hwang, P.H. Computed Tomography Analysis of Frontal Cell Prevalence According to the International Frontal Sinus Anatomy Classification. In International Forum of Allergy & Rhinology; Wiley Online Library: Hoboken, NJ, USA, 2018; Volume 8, pp. 825–830. [Google Scholar]
- Abraham, Z.S.; Kahinga, A.A. Prevalence of Frontal Cells and Their Relation to Frontal Sinusitis among Patients Who Underwent Functional Endoscopic Sinus Surgery: A Prospective Cross-Sectional Study in Tanzania. Ann. Med. Surg. 2022, 84, 104907. [Google Scholar] [CrossRef] [PubMed]
- Johari, H.H.; Mohamad, I.; Sachlin, I.S.; Aziz, M.E.; Mey, T.Y.; Ramli, R.R. A Computed Tomographic Analysis of Frontal Recess Cells in Association with the Development of Frontal Sinusitis. Auris Nasus Larynx 2018, 45, 1183–1190. [Google Scholar] [CrossRef] [PubMed]
- Kubota, K.; Takeno, S.; Hirakawa, K. Frontal Recess Anatomy in Japanese Subjects and Its Effect on the Development of Frontal Sinusitis: Computed Tomography Analysis. J. Otolaryngol. Head Neck Surg. 2015, 44, 21. [Google Scholar] [CrossRef]
- Lien, C.; Weng, H.; Chang, Y.; Lin, Y.; Wang, W. Computed Tomographic Analysis of Frontal Recess Anatomy and Its Effect on the Development of Frontal Sinusitis. Laryngoscope 2010, 120, 2521–2527. [Google Scholar] [CrossRef]
- Han, J.K.; Ghanem, T.; Lee, B.; Gross, C.W. Various Causes for Frontal Sinus Obstruction. Am. J. Otolaryngol. 2009, 30, 80–82. [Google Scholar] [CrossRef]
- Cho, J.H.; Citardi, M.J.; Lee, W.T.; Sautter, N.B.; Lee, H.-M.; Yoon, J.-H.; Hong, S.-C.; Kim, J.K. Comparison of Frontal Pneumatization Patterns between Koreans and Caucasians. Otolaryngol. Head Neck Surg. 2006, 135, 780–786. [Google Scholar] [CrossRef]
- Lee, W.T.; Kuhn, F.A.; Citardi, M.J. 3D Computed Tomographic Analysis of Frontal Recess Anatomy in Patients without Frontal Sinusitis. Otolaryngol. Head Neck Surg. 2004, 131, 164–173. [Google Scholar] [CrossRef]
- Brunner, E.; Jacobs, J.B.; Shpizner, B.A.; Lebowitz, R.A.; Holliday, R.A. Role of the agger nasi cell in chronic frontal sinusitis. Ann. Otol. Rhinol. Laryngol. 1996, 105, 694–700. [Google Scholar]
- Meyer, T.K.; Kocak, M.; Smith, M.M.; Smith, T.L. Coronal Computed Tomography Analysis of Frontal Cells. Am. J. Rhinol. 2003, 17, 163–168. [Google Scholar] [CrossRef] [PubMed]
- Eweiss, A.Z.; Khalil, H.S. The Prevalence of Frontal Cells and Their Relation to Frontal Sinusitis: A Radiological Study of the Frontal Recess Area. Int. Sch. Res. Not. 2013, 2013, 687582. [Google Scholar] [CrossRef] [PubMed]
- DelGaudio, J.M.; Hudgins, P.A.; Venkatraman, G.; Beningfield, A. Multiplanar Computed Tomographic Analysis of Frontal Recess Cells: Effect on Frontal Isthmus Size and Frontal Sinusitis. Arch. Otolaryngol. Head. Neck Surg. 2005, 131, 230–235. [Google Scholar] [CrossRef] [PubMed]
- Turgut, S.; Ercan, I.; Sayın, I.; Bas¸ak, B. The Relationship Between Frontal Sinusitis and Localization of the Frontal Sinus Outflow Tract A Computer-Assisted Anatomical and Clinical Study. Arch. Otolaryngol. Head. Neck Surg. 2005, 131, 518–522. [Google Scholar] [CrossRef] [PubMed]
- Langille, M.; Walters, E.; Dziegielewski, P.T.; Kotylak, T.; Wright, E.D. Frontal Sinus Cells: Identification, Prevalence, and Association with Frontal Sinus Mucosal Thickening. Am. J. Rhinol. Allergy 2012, 26, e107–e110. [Google Scholar] [CrossRef] [PubMed]
- House, L.K.; Stringer, S.P.; Seals, S. Correlation of Frontal Sinus Recess Anatomy with Ethnicity, Gender, and Pathology. Am. J. Otolaryngol. 2017, 38, 452–455. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, K.; Tsuzuki, K.; Okazaki, K.; Sakagami, M. Influence of Opacification in the Frontal Recess on Frontal Sinusitis. J. Laryngol. Otol. 2017, 131, 620–626. [Google Scholar] [CrossRef]
- Lai, W.S.; Yang, P.L.; Lee, C.H.; Lin, Y.Y.; Chu, Y.H.; Wang, C.H.; Wang, H.W.; Shih, C.P. The Association of Frontal Recess Anatomy and Mucosal Disease on the Presence of Chronic Frontal Sinusitis: A Computed Tomographic Analysis. Rhinology 2014, 52, 208–214. [Google Scholar] [CrossRef]
- Jaremek-Ochniak, W.; Sierdziński, J.; Popko-Zagor, M. Three-Dimensional Computed Tomography Analysis of Frontal Recess Cells According to the International Frontal Sinus Anatomy Classification (IFAC)—Difficulties in Identification of Frontal Recess Cells in Patients with Diffuse Primary Chronic Rhinosinusitis? Otolaryngol. Pol. 2022, 76, 7–14. [Google Scholar]
- April, M.M.; Zinreich, S.J.; Baroody, F.M.; Naclerio, R.M. Coronal CT Scan Abnormalities in Children with Chronic Sinusitis. Laryngoscope 1993, 103, 985–990. [Google Scholar] [CrossRef]
- Kim, H.J.; Cho, M.J.; Lee, J.W.; Kim, Y.T.; Kahng, H.; Kim, H.S.; Hahm, K.H. The Relationship between Anatomic Variations of Paranasal Sinuses and Chronic Sinusitis in Children. Acta Otolaryngol. 2006, 126, 1067–1072. [Google Scholar] [PubMed]
- Lusk, R.P.; McAlister, B.; el Fouley, A. Anatomic Variation in Pediatric Chronic Sinusitis: A CT Study. Otolaryngol. Clin. N. Am. 1996, 29, 75–91. [Google Scholar] [CrossRef]
- Al-Qudah, M. The Relationship between Anatomical Variations of the Sino-Nasal Region and Chronic Sinusitis Extension in Children. Int. J. Pediatr. Otorhinolaryngol. 2008, 72, 817–821. [Google Scholar] [CrossRef] [PubMed]
- Kendall, K.A.; Senders, C.W. Orbital and Intracranial Complications of Sinusitis in Children and Adults. In Diseases of the Sinuses: A Comprehensive Textbook of Diagnosis and Treatment; Springer: Berlin/Heidelberg, Germany, 1996; pp. 247–271. [Google Scholar]
- Goldsmith, A.J.; Rosenfeld, R.M. Treatment of Pediatric Sinusitis. Pediatr. Clin. 2003, 50, 413–426. [Google Scholar] [CrossRef]
- Seresirikachorn, K.; Sit, A.; Png, L.H.; Kalish, L.; Campbell, R.G.; Alvarado, R.; Harvey, R.J. Carolyn’s Window Approach to Unilateral Frontal Sinus Surgery. Laryngoscope 2023, 133, 2496–2501. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| First Author | Year | Population | Screening Method | Number of Sides | Cell Prevalence (%) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| ANC | SAC | SAFC | SBC | SBFC | SOEC | FSC | |||||
| Howser et al. [21] | 2023 | White | maxillofacial or sinus CT | 100 | 96.0 | 57.0 | 26.0 | 64.0 | 17.0 | 12.0 | 20.0 |
| Black | 100 | 95.0 | 40.0 | 31.0 | 56.0 | 17.0 | 8.0 | 18.0 | |||
| Asian | 78 | 94.9 | 37.2 | 23.1 | 55.1 | 11.5 | 21.8 | 24.4 | |||
| Latino | 90 | 97.8 | 35.6 | 25.6 | 54.4 | 7.8 | 7.8 | 16.7 | |||
| Koksal et al. [22] | 2023 | Turkish | paranasal sinus CT | 160 (Adults) | 86.3 | 35.0 | 44.4 | 54.4 | 46.9 | 19.4 | 3.4 |
| 160 (Pediatrics) | 93.1 | 41.9 | 60.0 | 76.3 | 58.5 | 18.8 | 0 | ||||
| Nofal & El-Anwar [23] | 2022 | Egyptian | maxillofacial CT | 200 | 97.0 | 48.0 | 11.0 | 72.0 | 23.0 | 42.0 | 21.0 |
| Fawzi et al. [24] | 2022 | Malaysian | paranasal sinus CT | 400 | 95.5 | 50.0 | 36.0 | 60.8 | 53.0 | 5.5 | 8.3 |
| Seth et al. [25] | 2020 | Indian | maxillofacial or sinus CT | 180 | 95.5 | 33.3 | 22.2 | 36.1 | 21.1 | 39.4 | 21.1 |
| Gotlib et al. [8] | 2019 | Caucasian | paranasal sinus CT | 206 | 86.9 | 34.0 | 17.5 | 77.2 | 22.8 | 5.8 | 27.2 |
| Tran et al. [26] | 2019 | Vietnamese | sinus CT | 208 | 95.7 | 16.3 | 13 | 46.2 | 4.3 | 17.3 | 10.6 |
| Sommer et al. [18] | 2019 | German | sinus CT | 498 | 95.2 | 49 | 24.9 | 88.8 | 26.5 | 9.2 | 27.7 |
| Choby et al. [27] | 2018 | North American | sinus CT | 200 | 96.5 | 30 | 20 | 72 | 5.5 | 28.5 | 30 |
| First Author | Year | Population | Screening Method | Number of Sides | Cells Prevalence (%) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ANC | FC1 | FC2 | FC3 | FC4 | SBC | SOEC | FBC | IFSSC | |||||
| Abraham & Kahinga [28] | 2022 | Tanzanian | paranasal sinus CT | 90 | 83.3 | 22.2 | 35.6 | 11.1 | 3.3 | N/A | N/A | N/A | N/A |
| Johari et al. [29] | 2018 | Malaysian | paranasal sinus CT | 312 | 98.1 | 28.8 | 31.1 | 14.4 | 0 | 40.3 | 16.7 | 33.0 | 10.8 |
| Kubota et al. [30] | 2015 | Japanese | Spiral CT scans | 300 | 88.0 | 37.0 | 6.3 | 4.3 | 1.3 | 37.0 | 6.0 | 7.0 | 8.6 |
| Lien et al. [31] | 2010 | Taiwanese | Spiral CT scans | 363 | 89.0 | 21.5 | 10.5 | 7.7 | 0 | 39.1 | 7.7 | 6.3 | 9.6 |
| Han et al. [32] | 2008 | Chinese | Spiral CT scans | 404 | 94.1 | 24.4 | 7.0 | 8.2 | 0 | 36.6 | 5.4 | 9.0 | 12.4 |
| Cho et al. [33] | 2006 | Korean | sinus CT | 114 | 94.0 | 22.8 | 14.0 | 7.9 | 0 | 39.5 | 2.6 | 14.0 | 8.8 |
| Caucasian | 82 | 86.6 | 35.4 | 20.7 | 8.5 | 0 | 11.0 | 64.6 | 6.1 | 7.3 | |||
| Study | Year | Method of Classification Used | Frontal Recess Cell Variation Association with Sinusitis | Sinus Cell Type Associated with Sinusitis |
|---|---|---|---|---|
| Meyer et al. [36] | 2003 | Bent | Yes | type III and IV |
| Delgaudio et al. [38] | 2005 | Bent | No | N/A |
| Eweiss & Khalil [37] | 2013 | Bent | No | N/A |
| Abraham & Kahinga [28] | 2022 | Bent | No | N/A |
| Lien et al. [31] | 2010 | Kuhn | Yes | SBC, FBC, and SOEC |
| Langille et al. [40] | 2012 | Kuhn | Yes | type I, II, and III |
| Lai et al. [43] | 2014 | Kuhn | No | N/A |
| Kubota et al. [30] | 2015 | Kuhn | Yes | FBC |
| Hashimoto et al. [42] | 2017 | Kuhn | No | N/A |
| House et al. [41] | 2017 | Kuhn | Yes | type III and IV |
| Johari et al. [29] | 2018 | Kuhn | Yes | FBC |
| Sommer et al. [18] | 2019 | IFAC | No | N/A |
| Seth et al. [25] | 2020 | IFAC | No | N/A |
| Fawzi et al. [24] | 2022 | IFAC | Yes | SOEC and FSC |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al Habsi, T.; Al-Ajmi, E.; Washahi, M.A.; Lawati, M.A.; Maawali, S.A.; Mahajan, A.; Sirasanagandla, S.R. Does Frontal Recess Cell Variation Associate with the Development of Frontal Sinusitis? A Narrative Review. Diagnostics 2024, 14, 103. https://doi.org/10.3390/diagnostics14010103
Al Habsi T, Al-Ajmi E, Washahi MA, Lawati MA, Maawali SA, Mahajan A, Sirasanagandla SR. Does Frontal Recess Cell Variation Associate with the Development of Frontal Sinusitis? A Narrative Review. Diagnostics. 2024; 14(1):103. https://doi.org/10.3390/diagnostics14010103
Chicago/Turabian StyleAl Habsi, Tariq, Eiman Al-Ajmi, Mohammed Al Washahi, Maitham Al Lawati, Shihab Al Maawali, Amit Mahajan, and Srinivasa Rao Sirasanagandla. 2024. "Does Frontal Recess Cell Variation Associate with the Development of Frontal Sinusitis? A Narrative Review" Diagnostics 14, no. 1: 103. https://doi.org/10.3390/diagnostics14010103
APA StyleAl Habsi, T., Al-Ajmi, E., Washahi, M. A., Lawati, M. A., Maawali, S. A., Mahajan, A., & Sirasanagandla, S. R. (2024). Does Frontal Recess Cell Variation Associate with the Development of Frontal Sinusitis? A Narrative Review. Diagnostics, 14(1), 103. https://doi.org/10.3390/diagnostics14010103