






Study of Motion Sickness Model Based on fNIRS Multiband Features during Car Rides



Abstract
1. Introduction
2. Materials and Methods
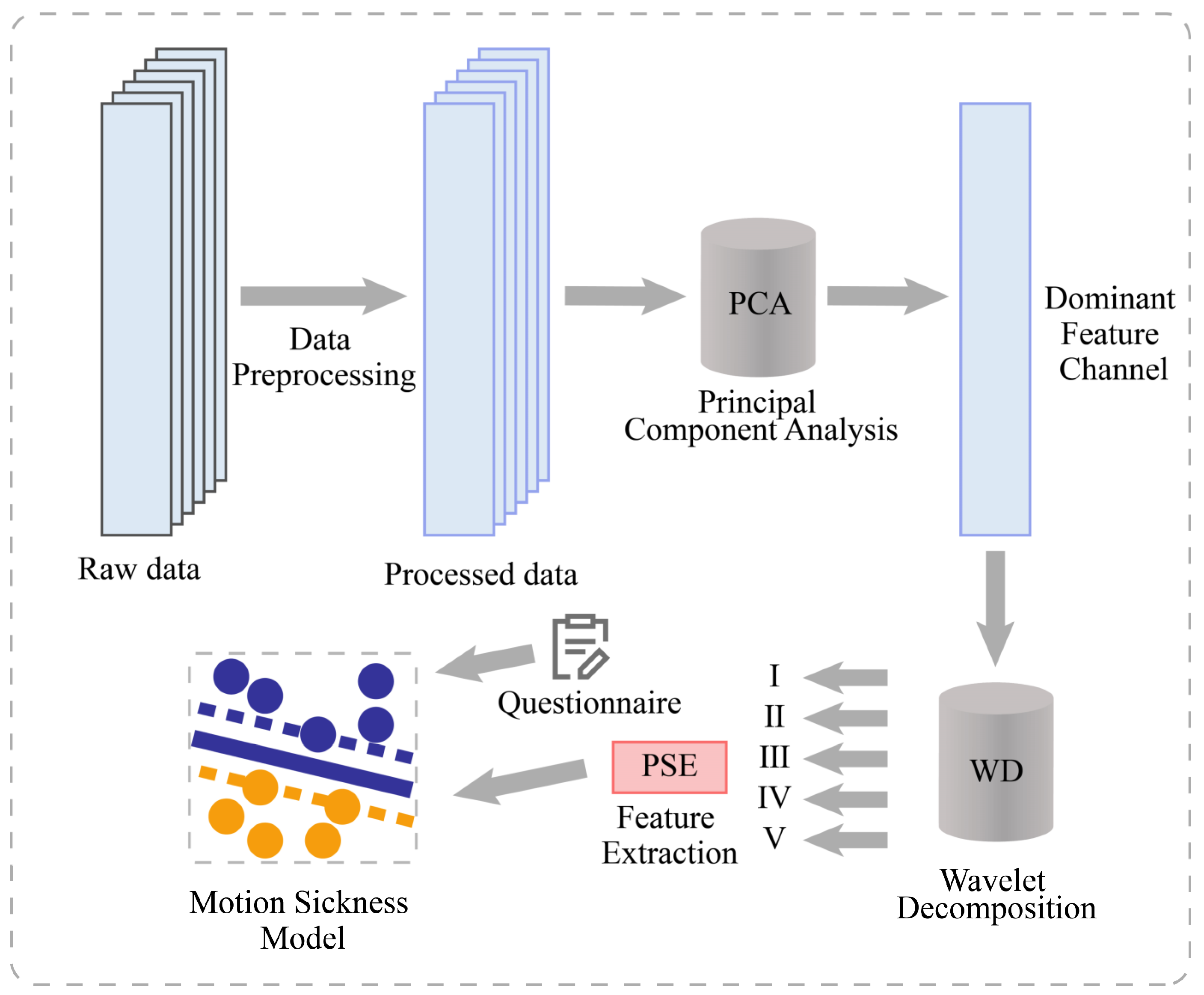
2.1. System Architecture Diagram
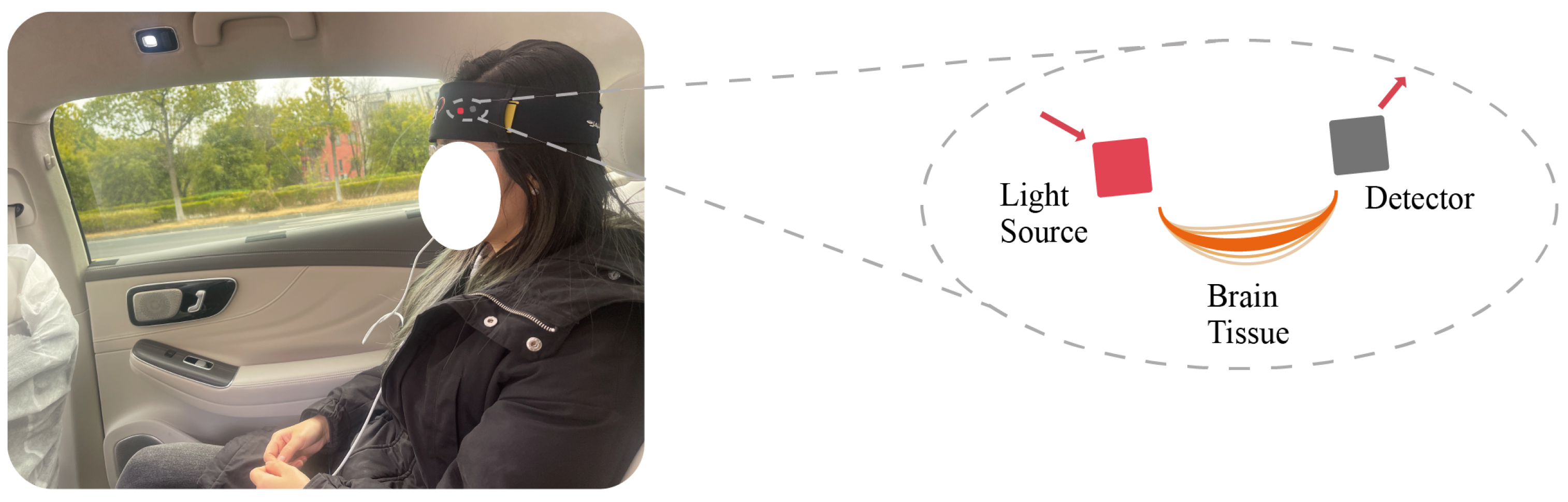
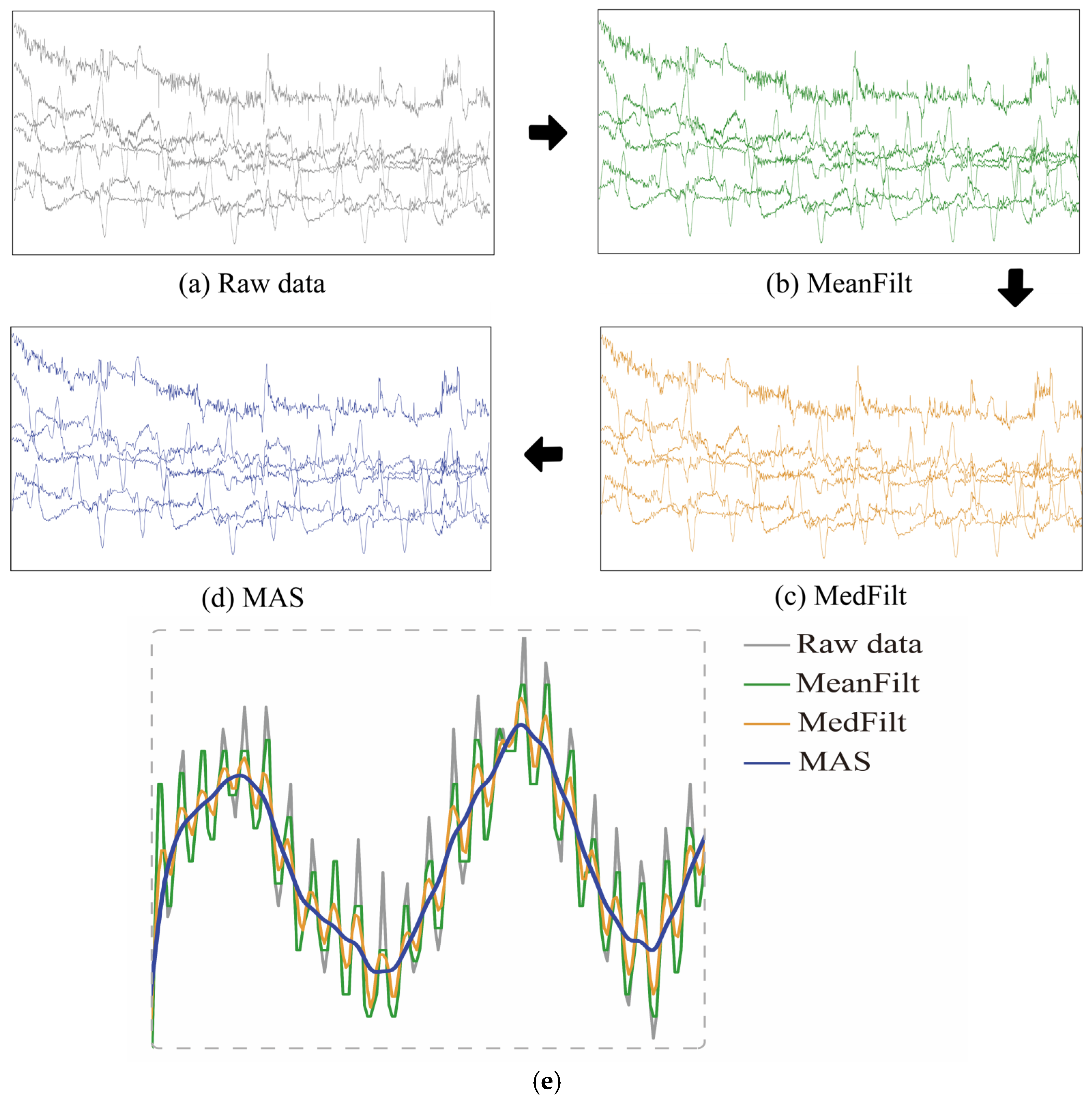
2.2. fNIRS Signal and Preprocessing
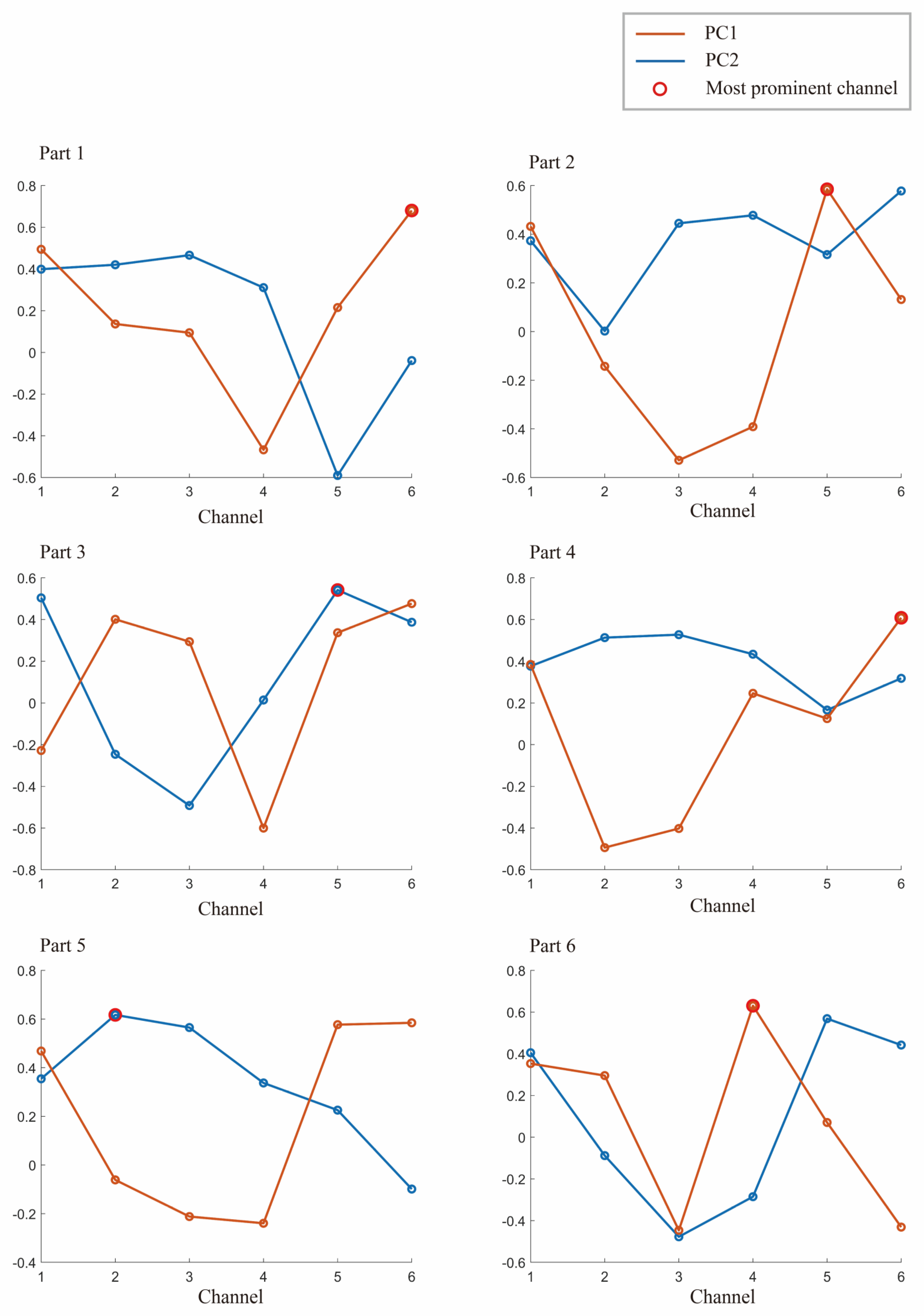
2.3. Channel Dimensionality Reduction Based on PCA
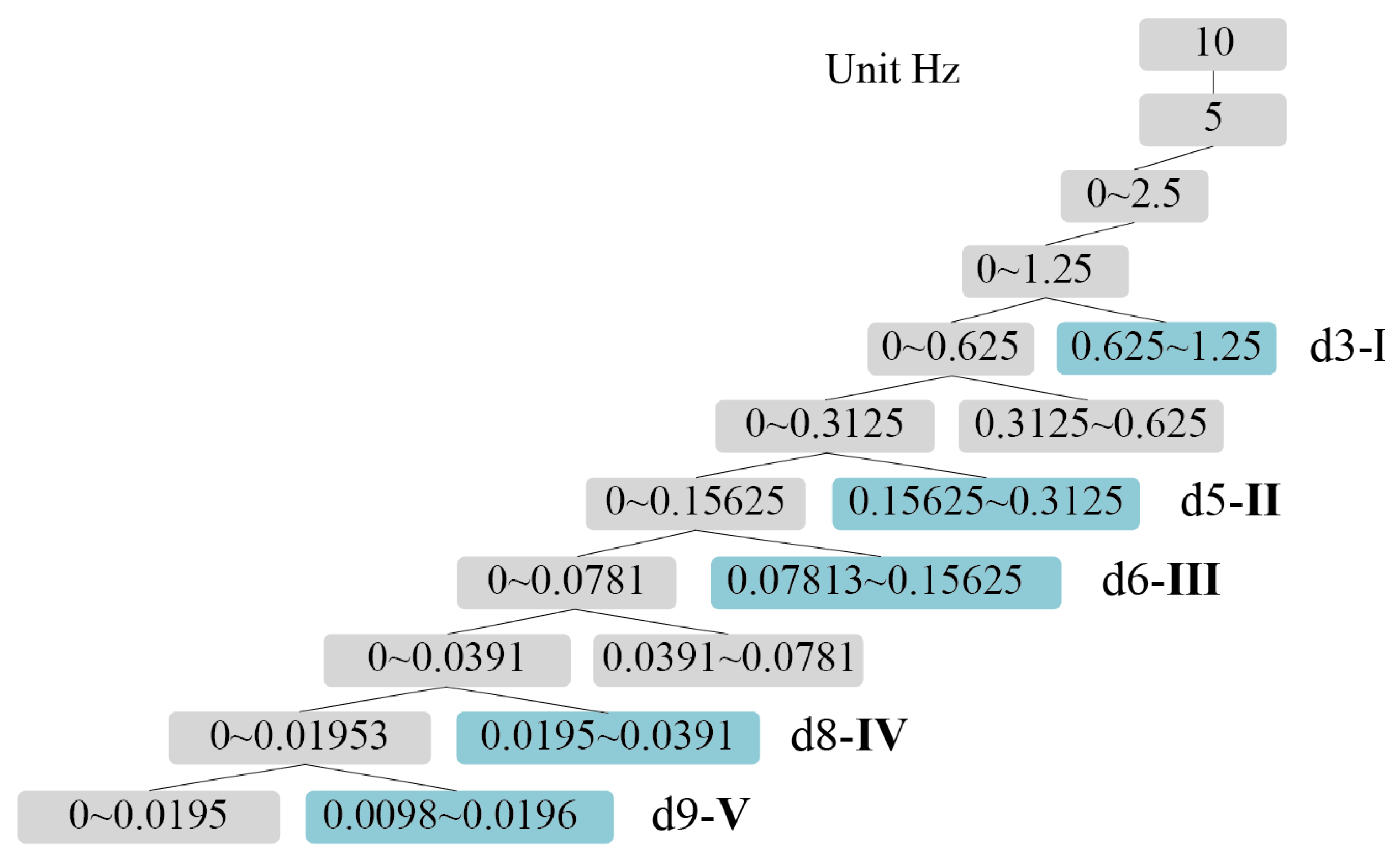
2.4. Feature Extraction of Multiband PSE
2.5. Motion Sickness Model Construction Combined with Subjective Evaluation
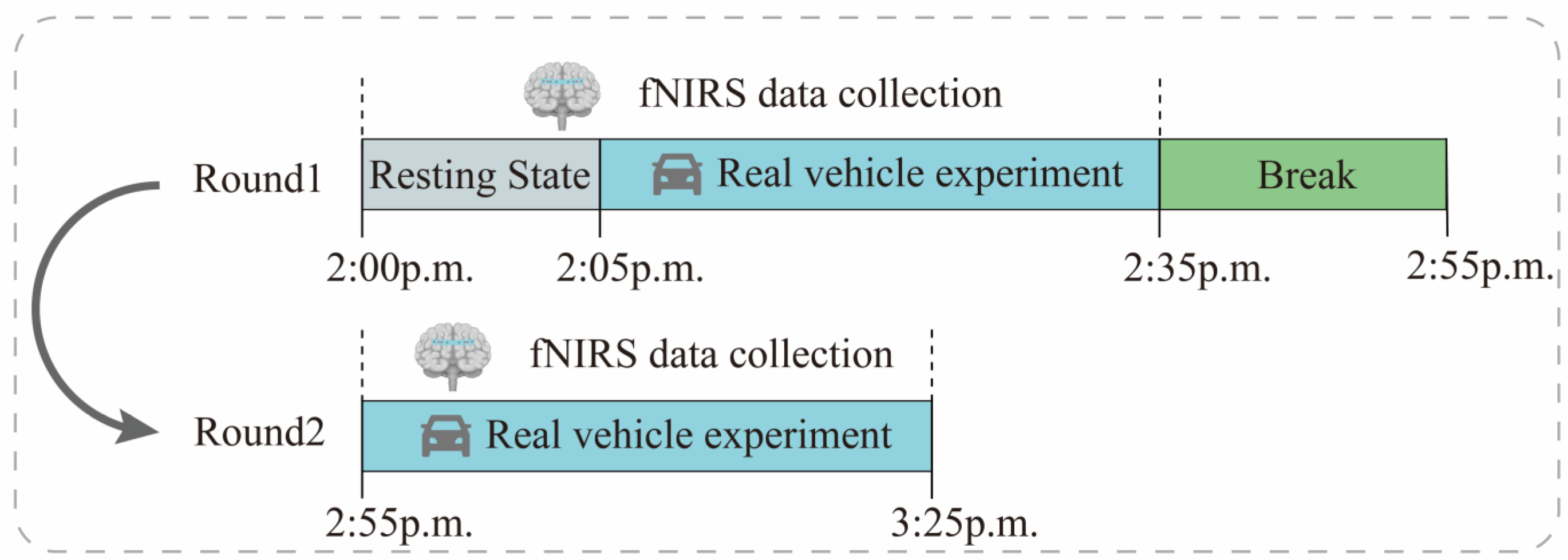
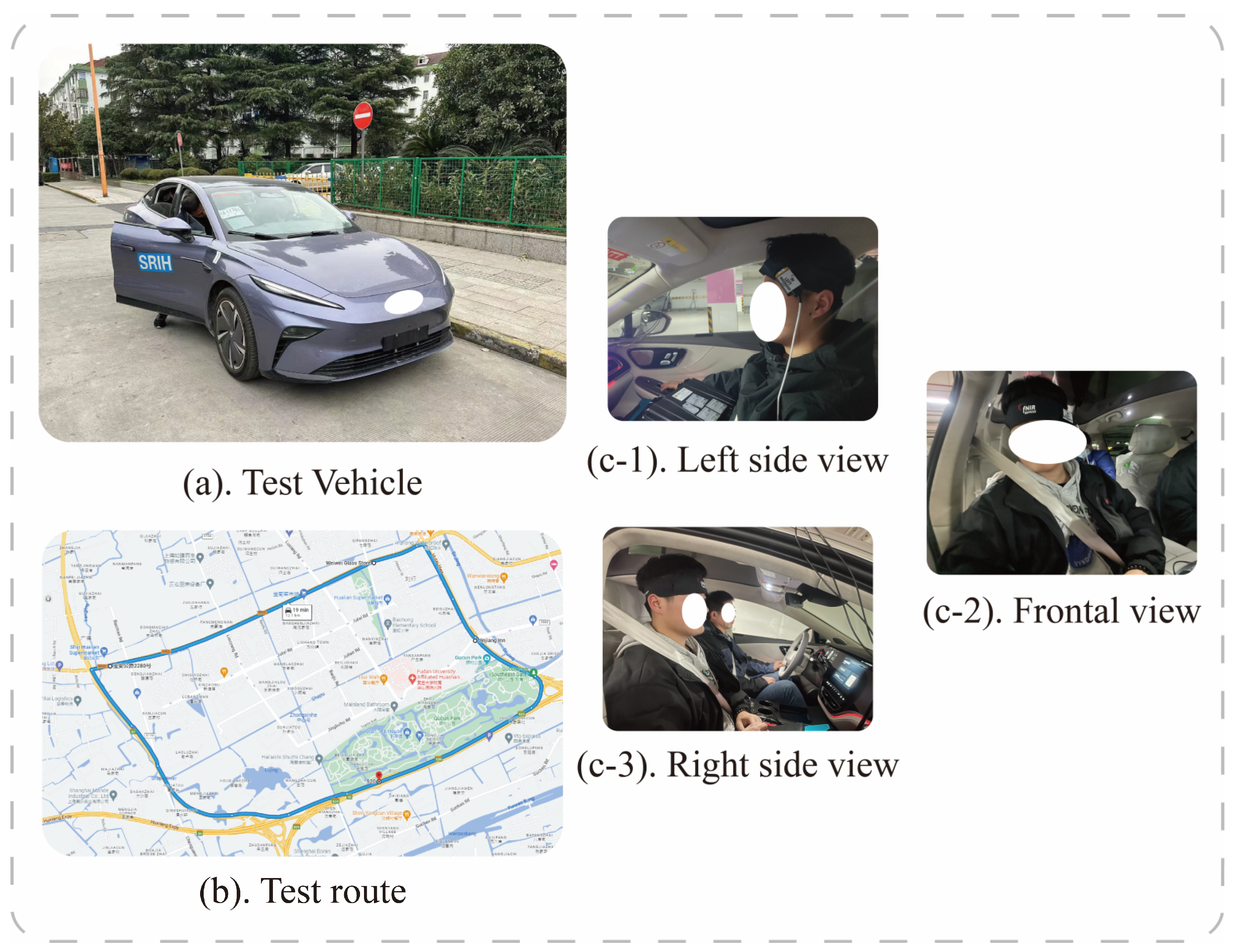
3. Passenger Motion Sickness Experimental Design
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Thompson, D.J.; Kouroussis, G.; Ntotsios, E. Modelling, Simulation and Evaluation of Ground Vibration Caused by Rail Vehicles. Veh. Syst. Dyn. 2019, 57, 936–983. [Google Scholar] [CrossRef]
- Shen, Y.; Qi, X. Update on Diagnosis and Differential Diagnosis of Vestibular Migraine. Neurol. Sci. 2022, 43, 1659–1666. [Google Scholar] [CrossRef] [PubMed]
- Ugur, E.; Konukseven, B.O. The Potential Use of Virtual Reality in Vestibular Rehabilitation of Motion Sickness. Auris Nasus Larynx 2022, 49, 768–781. [Google Scholar] [CrossRef] [PubMed]
- Reason, J.T.; Brand, J.J. Motion Sickness; Academic Press: Cambridge, MA, USA, 1975. [Google Scholar]
- Oka, N.; Yoshino, K.; Yamamoto, K.; Takahashi, H.; Li, S.; Sugimachi, T.; Nakano, K.; Suda, Y.; Kato, T. Greater Activity in the Frontal Cortex on Left Curves: A Vector-Based FNIRS Study of Left and Right Curve Driving. PLoS ONE 2015, 10, e0127594. [Google Scholar] [CrossRef] [PubMed]
- Gavgani, A.M.; Wong, R.H.X.; Howe, P.R.C.; Hodgson, D.M.; Walker, F.R.; Nalivaiko, E. Cybersickness-Related Changes in Brain Hemodynamics: A Pilot Study Comparing Transcranial Doppler and near-Infrared Spectroscopy Assessments during a Virtual Ride on a Roller Coaster. Physiol. Behav. 2018, 191, 56–64. [Google Scholar] [CrossRef]
- Zhang, C.; Li, S.; Li, Y.; Li, S.E.; Nie, B. Analysis of Motion Sickness Associated Brain Activity Using FNIRS: A Driving Simulator Study. IEEE Access 2020, 8, 207415–207425. [Google Scholar] [CrossRef]
- Zhao, L.; Li, C.; Ji, L.; Yang, T. EEG Characteristics of Motion Sickness Subjects in Automatic Driving Mode Based on Virtual Reality Tests. J. Tsinghua Univ. (Sci. Technol.) 2020, 60, 993–998. [Google Scholar]
- Lim, H.K.; Ji, K.; Woo, Y.S.; Han, D.; Lee, D.-H.; Nam, S.G.; Jang, K.-M. Test-Retest Reliability of the Virtual Reality Sickness Evaluation Using Electroencephalography (EEG). Neurosci. Lett. 2020, 743, 135589. [Google Scholar] [CrossRef]
- Li, Z.; Zhao, L.; Chang, J.; Li, W.; Yang, M.; Li, C.; Wang, R.; Ji, L. EEG-Based Evaluation of Motion Sickness and Reducing Sensory Conflict in a Simulated Autonomous Driving Environment. In Proceedings of the 2022 44th Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Glasgow, UK, 11 July 2022; IEEE: New York, NY, USA, 2022; pp. 4026–4030. [Google Scholar]
- Hwang, J.-U.; Bang, J.-S.; Lee, S.-W. Classification of Motion Sickness Levels Using Multimodal Biosignals in Real Driving Conditions. In Proceedings of the 2022 IEEE International Conference on Systems, Man, and Cybernetics (SMC), Prague, Czech Republic, 9 October 2022; IEEE: New York, NY, USA, 2022; pp. 1304–1309. [Google Scholar]
- Irmak, T.; Pool, D.M.; Happee, R. Objective and Subjective Responses to Motion Sickness: The Group and the Individual. Exp. Brain Res. 2021, 239, 515–531. [Google Scholar] [CrossRef]
- Tan, R.; Li, W.; Hu, F.; Xiao, X.; Li, S.; Xing, Y.; Wang, H.; Cao, D. Motion Sickness Detection for Intelligent Vehicles: A Wearable-Device-Based Approach. In Proceedings of the 2022 IEEE 25th International Conference on Intelligent Transportation Systems (ITSC), Macao, China, 8 October 2022; IEEE: New York, NY, USA; pp. 4355–4362. [Google Scholar]
- Koch, A.; Cascorbi, I.; Westhofen, M.; Dafotakis, M.; Klapa, S.; Kuhtz-Buschbeck, J.P. The Neurophysiology and Treatment of Motion Sickness. Dtsch. Ärzteblatt Int. 2018, 115, 687. [Google Scholar] [CrossRef]
- Fuster, J.M. The Prefrontal Cortex Makes the Brain a Preadaptive System. Proc. IEEE 2014, 102, 417–426. [Google Scholar] [CrossRef]
- Acharya, D.; Mukherjea, A.; Cao, J.; Ruesch, A.; Schmitt, S.; Yang, J.; Smith, M.A.; Kainerstorfer, J.M. Non-Invasive Spectroscopy for Measuring Cerebral Tissue Oxygenation and Metabolism as a Function of Cerebral Perfusion Pressure. Metabolites 2022, 12, 667. [Google Scholar] [CrossRef] [PubMed]
- Boushel, R.; Langberg, H.; Olesen, J.; Gonzales-Alonzo, J.; Bülow, J.; Kjaer, M. Monitoring Tissue Oxygen Availability with near Infrared Spectroscopy (NIRS) in Health and Disease. Scand. J. Med. Sci. Sports 2001, 11, 213–222. [Google Scholar] [CrossRef]
- Chitnis, D.; Airantzis, D.; Highton, D.; Williams, R.; Phan, P.; Giagka, V.; Powell, S.; Cooper, R.J.; Tachtsidis, I.; Smith, M.; et al. Towards a Wearable near Infrared Spectroscopic Probe for Monitoring Concentrations of Multiple Chromophores in Biological Tissue in Vivo. Rev. Sci. Instrum. 2016, 87, 065112. [Google Scholar] [CrossRef] [PubMed]
- Eastmond, C.; Subedi, A.; De, S.; Intes, X. Deep Learning in FNIRS: A Review. Neurophotonics 2022, 9, 041411. [Google Scholar] [CrossRef] [PubMed]
- Rocco, G.; Lebrun, J.; Meste, O.; Magnie-Mauro, M.-N. A Chiral FNIRS Spotlight on Cerebellar Activation in a Finger Tapping Task. In Proceedings of the 2021 43rd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Virtual Conference, 1 November 2021; IEEE: New York, NY, USA, 2021; pp. 1018–1021. [Google Scholar]
- Golding, J.F.; Gresty, M.A. Pathophysiology and Treatment of Motion Sickness. Curr. Opin. Neurol. 2015, 28, 83–88. [Google Scholar] [CrossRef]
- Ayaz, H.; Shewokis, P.A.; Bunce, S.C.; Onaral, B. Functional Near Infrared Spectroscopy Based Brain Computer Interface. U.S. Patent No. 9,946,344, 10 July 2018. [Google Scholar]
- Cao, N.; Gao, T. Noninvasive Tissue Blood Oxygenation Measurement Based on Near Infrared Spectroscopy (NIRS). In Proceedings of the 2009 3rd International Conference on Bioinformatics and Biomedical Engineering, Beijing, China, 11–13 June 2009; IEEE: New York, NY, USA, 2009; pp. 1–4. [Google Scholar]
- Molavi, B.; Dumont, G.A. Wavelet-Based Motion Artifact Removal for Functional near-Infrared Spectroscopy. Physiol. Meas. 2012, 33, 259–270. [Google Scholar] [CrossRef]
- Lin, C.-T.; King, J.-T.; Chuang, C.-H.; Ding, W.; Chuang, W.-Y.; Liao, L.-D.; Wang, Y.-K. Exploring the Brain Responses to Driving Fatigue Through Simultaneous EEG and FNIRS Measurements. Int. J. Neural Syst. 2020, 30, 1950018. [Google Scholar] [CrossRef]
- Zhou, X.; Sobczak, G.; McKay, C.M.; Litovsky, R.Y. Comparing FNIRS Signal Qualities between Approaches with and without Short Channels. PLoS ONE 2020, 15, e0244186. [Google Scholar] [CrossRef]
- Giller, C.A.; Hatab, M.R.; Giller, A.M. Giller Oscillations in Cerebral Blood Flow Detected with a Transcranial Doppler Index. J. Cereb. Blood Flow Metab. 1999, 19, 452–459. [Google Scholar] [CrossRef]
- Obrig, H.; Neufang, M.; Wenzel, R.; Kohl, M.; Steinbrink, J.; Einhäupl, K.; Villringer, A. Spontaneous Low Frequency Oscillations of Cerebral Hemodynamics and Metabolism in Human Adults. Neuroimage 2000, 12, 623–639. [Google Scholar] [CrossRef] [PubMed]
- Bertolini, G.; Straumann, D. Moving in a Moving World: A Review on Vestibular Motion Sickness. Front. Neurol. 2016, 7, 14. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Ma, L.-C.; Shahdadian, S.; Wu, A.; Truong, N.C.D.; Liu, H. Metabolic Connectivity and Hemodynamic-Metabolic Coherence of Human Prefrontal Cortex at Rest and Post Photobiomodulation Assessed by Dual-Channel Broadband NIRS. Metabolites 2022, 12, 42. [Google Scholar] [CrossRef] [PubMed]
- Arie, R.; Brand, A.; Engelberg, S. Compressive Sensing and Sub-Nyquist Sampling. IEEE Instrum. Meas. Mag. 2020, 23, 94–101. [Google Scholar] [CrossRef]
- Kameyama, M.; Fukuda, M.; Yamagishi, Y.; Sato, T.; Uehara, T.; Ito, M.; Suto, T.; Mikuni, M. Frontal Lobe Function in Bipolar Disorder: A Multichannel near-Infrared Spectroscopy Study. Neuroimage 2006, 29, 172–184. [Google Scholar] [CrossRef]
- Huang, W.; Li, X.; Xie, H.; Qiao, T.; Zheng, Y.; Su, L.; Tang, Z.-M.; Dou, Z. Different Cortex Activation and Functional Connectivity in Executive Function Between Young and Elder People During Stroop Test: An FNIRS Study. Front. Aging Neurosci. 2022, 14, 864662. [Google Scholar] [CrossRef]
- Gao, T.; Zou, C.; Li, J.; Han, C.; Zhang, H.; Li, Y.; Tang, X.; Fan, Y. Identification of Moyamoya Disease Based on Cerebral Oxygen Saturation Signals Using Machine Learning Methods. J. Biophotonics 2022, 15, e202100388. [Google Scholar] [CrossRef]
- Ni, Y.; Sun, F.; Luo, Y.; Xiang, Z.; Sun, H. A Novel Heart Disease Classification Algorithm Based on Fourier Transform and Persistent Homology. In Proceedings of the 2022 IEEE International Conference on Electrical Engineering, Big Data and Algorithms (EEBDA), Changchun, China, 25 February 2022; IEEE: New York, NY, USA, 2022; pp. 116–122. [Google Scholar]
- Li, M.; Liu, Y.; Zhi, S.; Wang, T.; Chu, F. Short-Time Fourier Transform Using Odd Symmetric Window Function. J. Dyn. Monit. Diagn. 2021, 1, 37–45. [Google Scholar] [CrossRef]
- Zhang, D.; Zhang, D. Wavelet Transform. In Fundamentals of Image Data Mining: Analysis, Features, Classification and Retrieval; Springer: Cham, Switzerland, 2019; pp. 35–44. [Google Scholar]
- Subasi, A.; Saikia, A.; Bagedo, K.; Singh, A.; Hazarika, A. EEG-Based Driver Fatigue Detection Using FAWT and Multiboosting Approaches. IEEE Trans. Ind. Inf. 2022, 18, 6602–6609. [Google Scholar] [CrossRef]
- Yan, H.; Xu, T.; Wang, P.; Zhang, L.; Hu, H.; Bai, Y. MEMS Hydrophone Signal Denoising and Baseline Drift Removal Algorithm Based on Parameter-Optimized Variational Mode Decomposition and Correlation Coefficient. Sensors 2019, 19, 4622. [Google Scholar] [CrossRef]
- Pooja; Pahuja, S.; Veer, K. Recent Approaches on Classification and Feature Extraction of EEG Signal: A Review. Robotica 2022, 40, 77–101. [Google Scholar] [CrossRef]
- Zhang, A.; Yang, B.; Huang, L. Feature Extraction of EEG Signals Using Power Spectral Entropy. In Proceedings of the 2008 International Conference on BioMedical Engineering and Informatics, Sanya, China, 28–30 May 2008; IEEE: New York, NY, USA, 2008; pp. 435–439. [Google Scholar]
- Choukèr, A.; Kaufmann, I.; Kreth, S.; Hauer, D.; Feuerecker, M.; Thieme, D.; Vogeser, M.; Thiel, M.; Schelling, G. Motion Sickness, Stress and the Endocannabinoid System. PLoS ONE 2010, 5, e10752. [Google Scholar] [CrossRef] [PubMed]
- Mareta, S.; Thenara, J.M.; Rivero, R.; Tan-Mullins, M. A Study of the Virtual Reality Cybersickness Impacts and Improvement Strategy towards the Overall Undergraduate Students’ Virtual Learning Experience. Interact. Technol. Smart Educ. 2022, 19, 460–481. [Google Scholar] [CrossRef]
- Dadgostar, M.; Setarehdan, S.K.; Shahzadi, S.; Akin, A. Classification of schizophrenia using SVM via fNIRS. Biomed. Eng. 2018, 30, 1850008. [Google Scholar] [CrossRef]
- Liu, S.; Wang, S.; Hu, C.; Qin, X.; Wang, J.; Kong, D. Development of a New NIR-Machine Learning Approach for Simultaneous Detection of Diesel Various Properties. Measurement 2022, 187, 110293. [Google Scholar] [CrossRef]
- Suthaharan, S. Support Vector Machine. In Machine Learning Models and Algorithms for Big Data Classification; Springer: Boston, MA, USA, 2016; pp. 207–235. [Google Scholar]
- Naji, M.A.; El Filali, S.; Aarika, K.; Benlahmar, E.H.; Abdelouhahid, R.A.; Debauche, O. Machine Learning Algorithms For Breast Cancer Prediction And Diagnosis. Procedia Comput. Sci. 2021, 191, 487–492. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Frequency Band | Frequency (Hz) | Physiological Meaning |
|---|---|---|
| I | 0.6–2.0 | Heart rate activity |
| II | 0.145–0.6 | Respiratory activity |
| III | 0.052–0.145 | Myogenic activity |
| IV | 0.021–0.052 | Neurogenic activity |
| V | 0.0095–0.021 | Endothelial cell metabolic activity |
| Score | Description |
|---|---|
| 0 | No motion sickness at all: participants have no sensation of motion sickness and feel normal. |
| 1 | Slight motion sickness: participants have slight motion sickness but can still carry on with normal activities. |
| 2 | Some motion sickness: participants experience motion sickness symptoms and may feel some discomfort but can still carry on with normal activities. |
| 3 | Much motion sickness: participants experience moderate motion sickness symptoms such as dizziness and nausea, which affect their ability to carry on with normal activities. |
| 4 | Extreme motion sickness: participants experience severe motion sickness symptoms such as severe dizziness and nausea, which prevent them from carrying on with normal activities. |
| 5 | Unbearable motion sickness: participants experience extremely severe motion sickness symptoms such as unbearable dizziness, nausea, and vomiting, which require immediate cessation of the activity and medical attention. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ren, B.; Guan, W.; Zhou, Q. Study of Motion Sickness Model Based on fNIRS Multiband Features during Car Rides. Diagnostics 2023, 13, 1462. https://doi.org/10.3390/diagnostics13081462
Ren B, Guan W, Zhou Q. Study of Motion Sickness Model Based on fNIRS Multiband Features during Car Rides. Diagnostics. 2023; 13(8):1462. https://doi.org/10.3390/diagnostics13081462
Chicago/Turabian StyleRen, Bin, Wanli Guan, and Qinyu Zhou. 2023. "Study of Motion Sickness Model Based on fNIRS Multiband Features during Car Rides" Diagnostics 13, no. 8: 1462. https://doi.org/10.3390/diagnostics13081462
APA StyleRen, B., Guan, W., & Zhou, Q. (2023). Study of Motion Sickness Model Based on fNIRS Multiband Features during Car Rides. Diagnostics, 13(8), 1462. https://doi.org/10.3390/diagnostics13081462