
Simultaneous Super-Resolution and Classification of Lung Disease Scans

 , , ,
, , ,  , ,
, , 
Abstract
1. Introduction
- Presenting a DL framework for diagnosis of lung diseases from chest X-ray and CT images.
- Studying the impact of image SR on lung disease diagnosis.
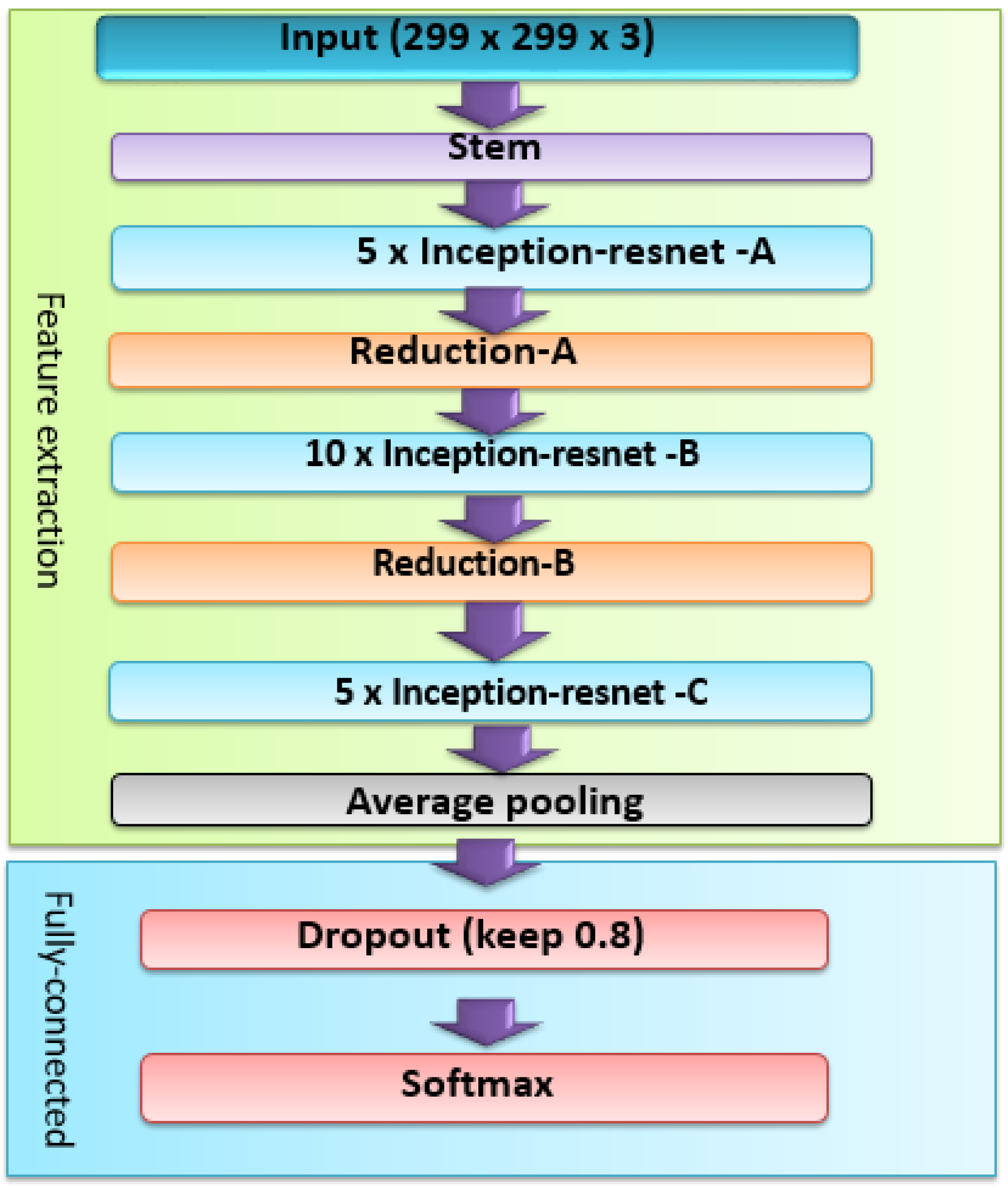
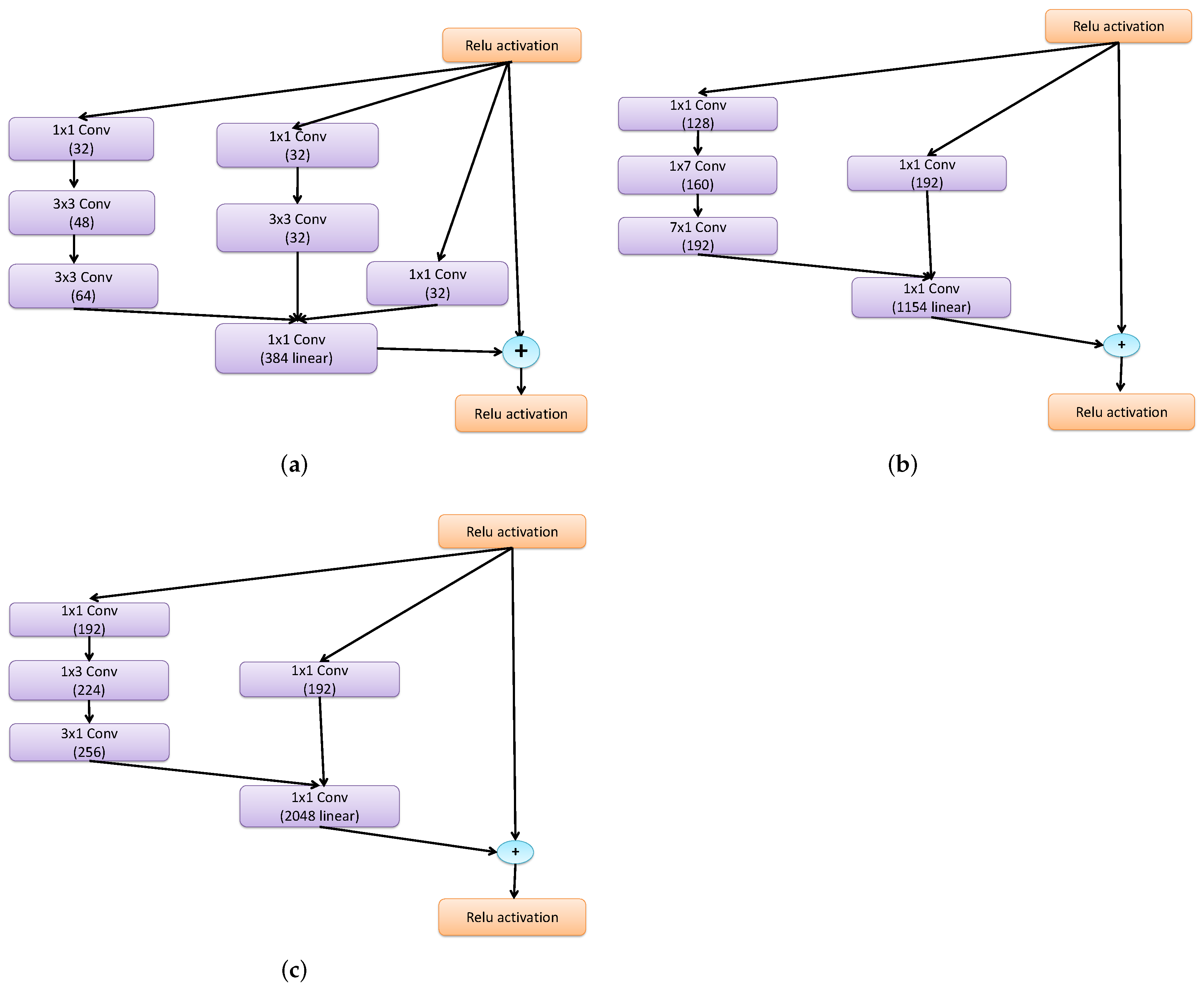
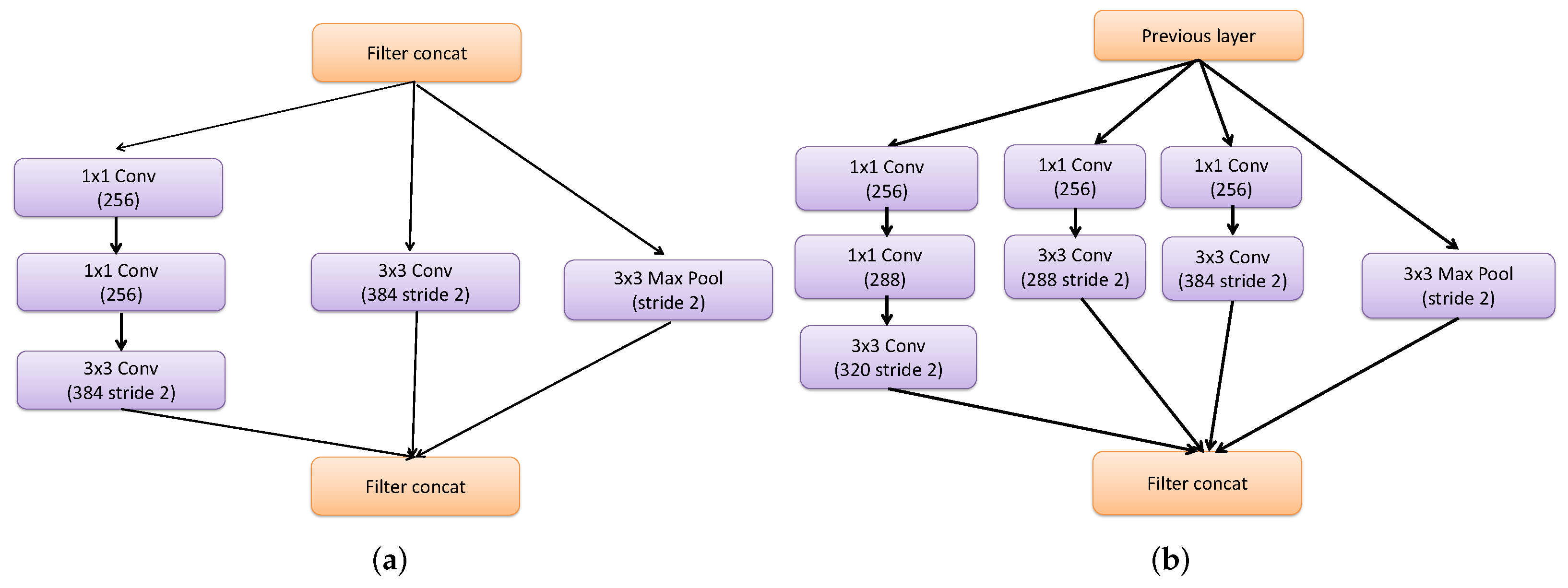
- Presentation of InceptionResNetv2 as a feature extractor and comparing its results with those of Resnet101 and Inceptionv3 models.
- Investigation of the proposed framework in five-class and six-class scenarios using softmax and MCSVM classifiers.
2. Related Work
3. Materials and Methods
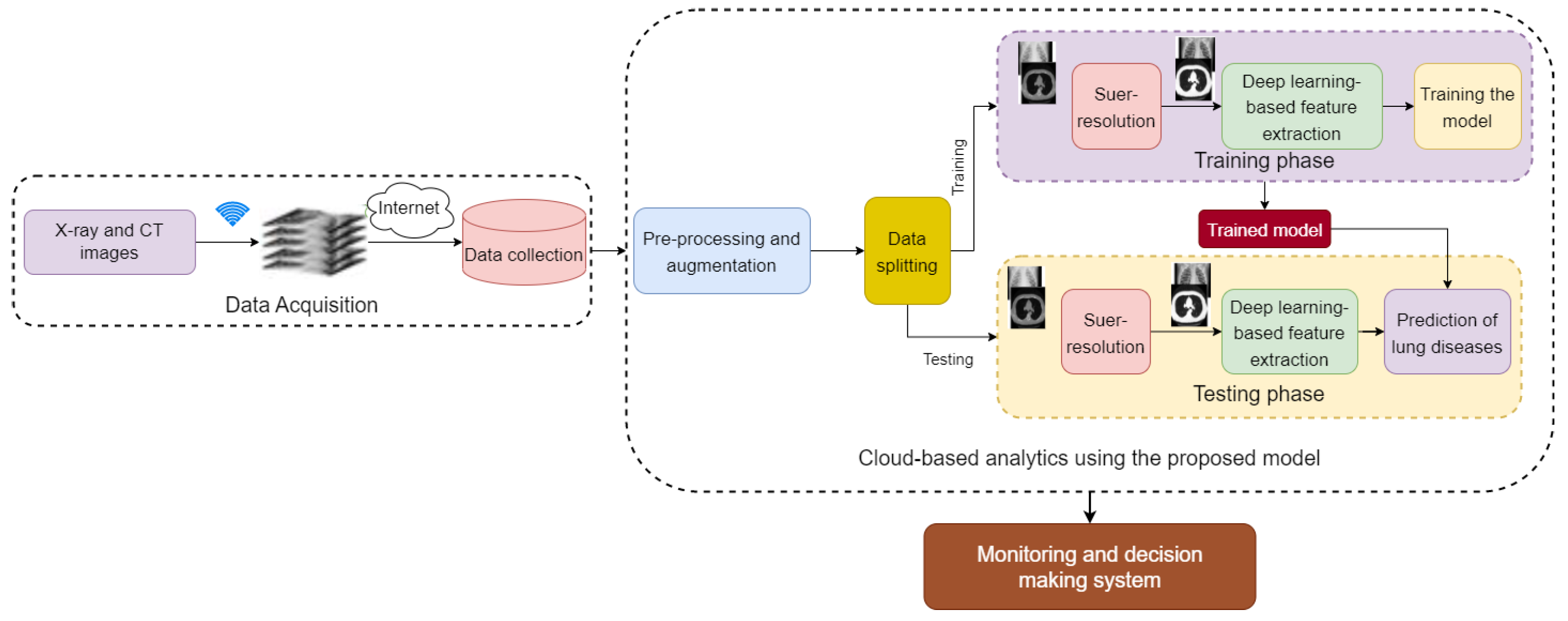
3.1. The Proposed Framework
3.2. Data Acquisition
3.3. Cloud-Based Analysis Using the Proposed Models
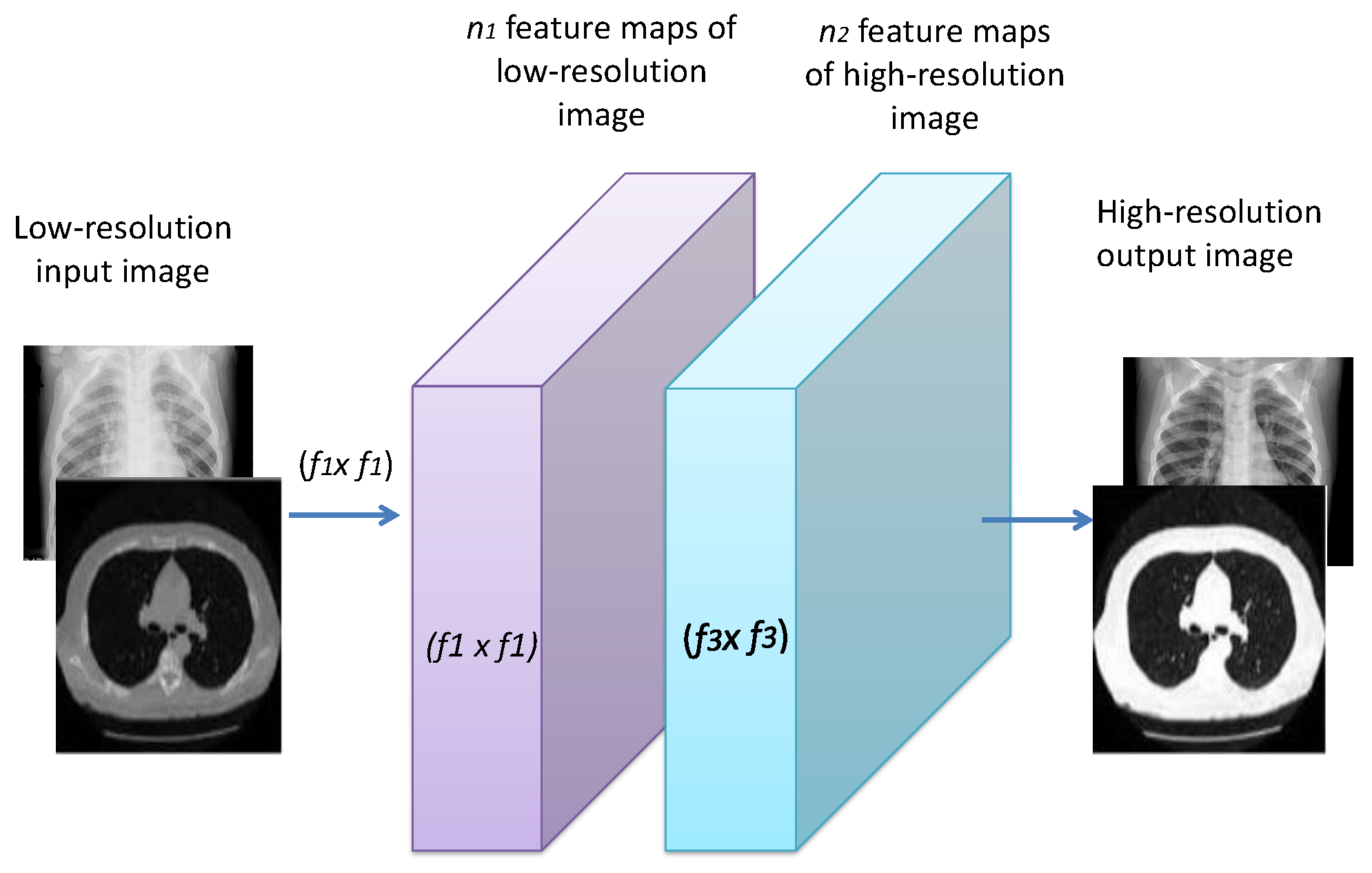
3.3.1. Image Super-Resolution
- Patch extraction and representation: Patches from the LR image Y are extracted, and then each patch is represented as a high-dimensional vector. This can be expressed as:where represents the weights for the first convolution layer, which has a size of . c, , and are the numbers of channels for the input image, the spatial filter size, and the number of filers, respectively. A rectified linear unit (ReLU) is applied on the output to add non-linearity.
- Non-linear mapping: An -dimensional feature vector is extracted for each patch from the first layer. Then, these -dimensional feature vectors are mapped as -dimensional vectors. This mapping can be represented as:where has a size of . Each of the output -dimensional vectors are used for reconstruction.
- Reconstruction: A pre-defined filter that acts as an averaging filter for the reconstruction process is used. The last convolutional layer is exploited to obtain the final HR image. The reconstruction process can be expressed as:Mean squared error (MSE) is used as the loss function .where k represents the number of training samples.

3.3.2. DL-Based Feature Extraction
3.3.3. Proposed Classification Frameworks
- (1)
- Softmax is the final layer at the network end. It generates the actual probability scores for each class label. In this paper, five-class and six-class classification problems are introduced. The softmax layer has n nodes marked as , where . represents the discrete probability distributions. The input to the softmax layer can be represented as follows:Then, can be calculated as:Then, the predicted class can be obtained as follows:where h and W represent the activation and the weight of the layer nodes that precede the softmax layer, respectively.
- (2)
- Multi-class Support Vector Machine Classifier: The SVM is a commonly used classifier for binary classification problems. It constructs decision hyperplanes that best divide the dataset into classes. For multi-class classification problems, the number of classes M is greater than two. The SVM uses several strategies to solve multi-class classification problems such as binary tree (BT), one-against-one (OAO), directed acyclic graph (DAG), and one-against-all (OAA) classifiers [70]. In this work, the OAASVM classifier with polynomial kernels is used as in [71]. M SVM models have been constructed, one for each class. The mth classifier is trained with all samples for class m and marked with positive labels, whereas the remaining classes are marked with negative labels. This gives advantages in terms of the short training time. The training of a single sub-classifier becomes much simpler.For n training data where and is the class of . The class m SVM solves the following [72]:where is the mapping function. For nonlinear separation, a penalty term is added for error reduction, where C represents the penalty parameter. In order to minimize the term , the margin between two groups of data should be maximized. After solving Equation (8), there are M decision functions , ............, .where is the decision boundary function. We can say that x belongs to a specific class that has the largest decision function value. The parameters of the SVM are presented in Table 2.
4. Experimental Results
4.1. Evaluation Metrics
4.2. Results
4.2.1. Results for Dataset #1
4.2.2. Results for Dataset #2
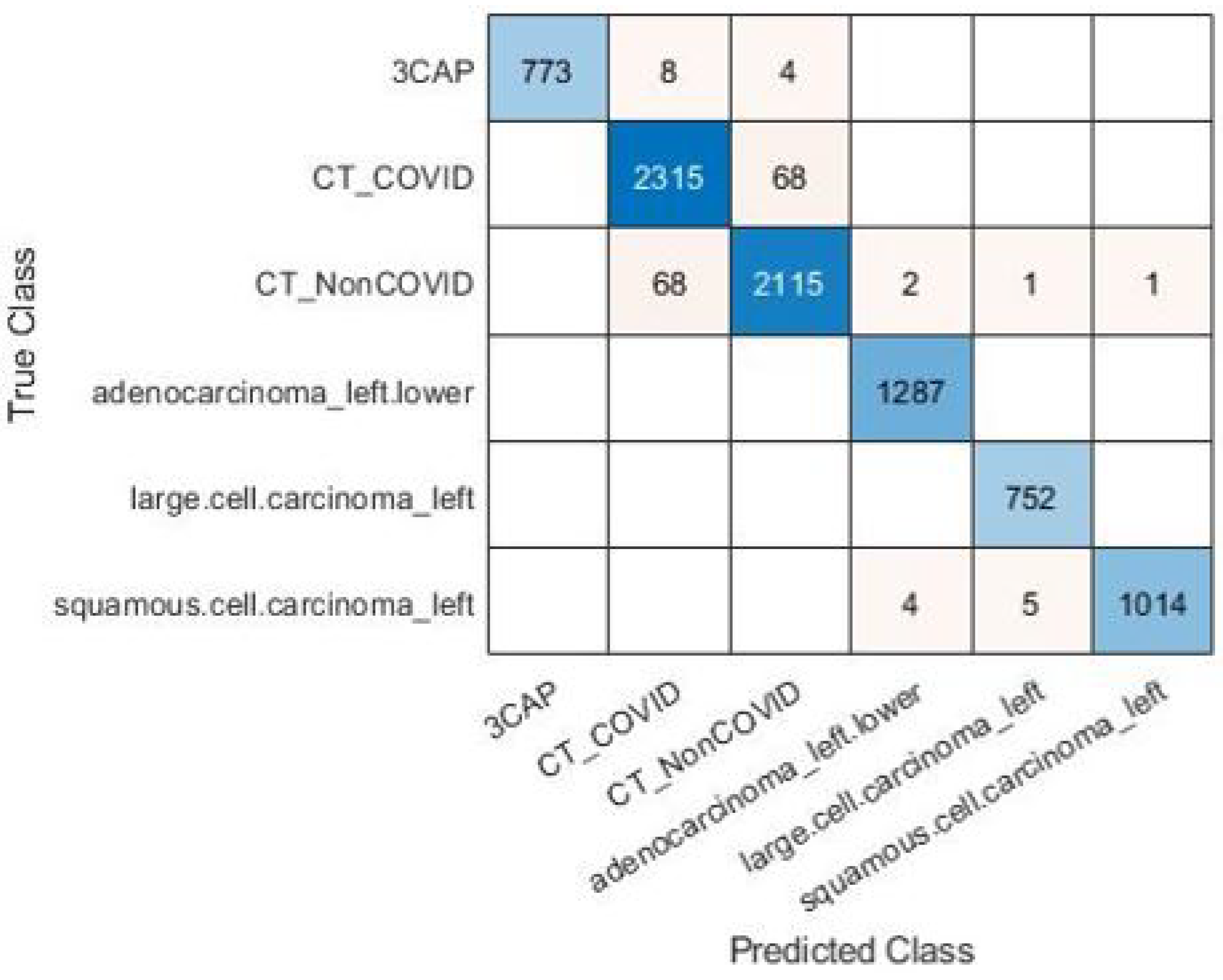
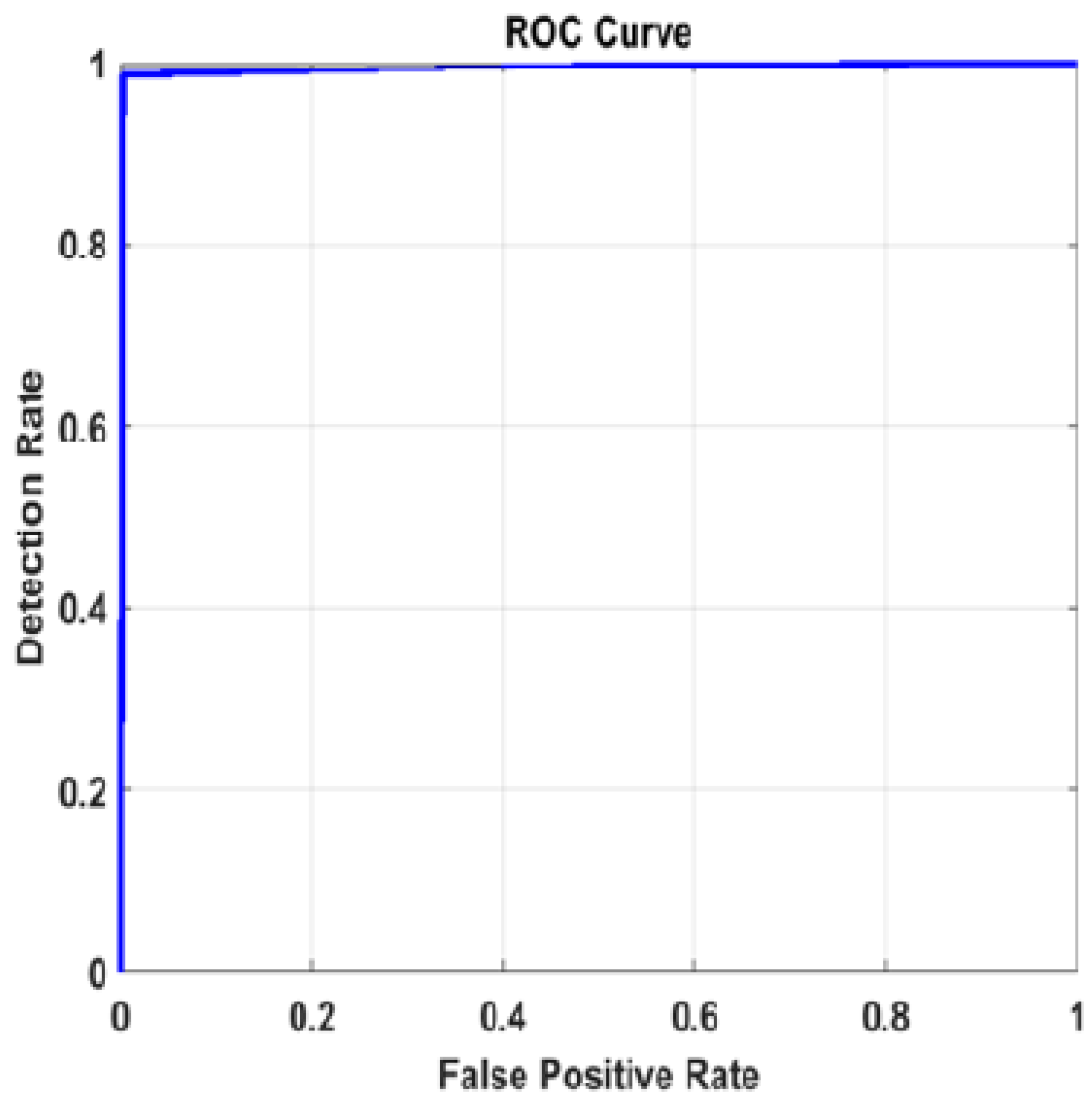
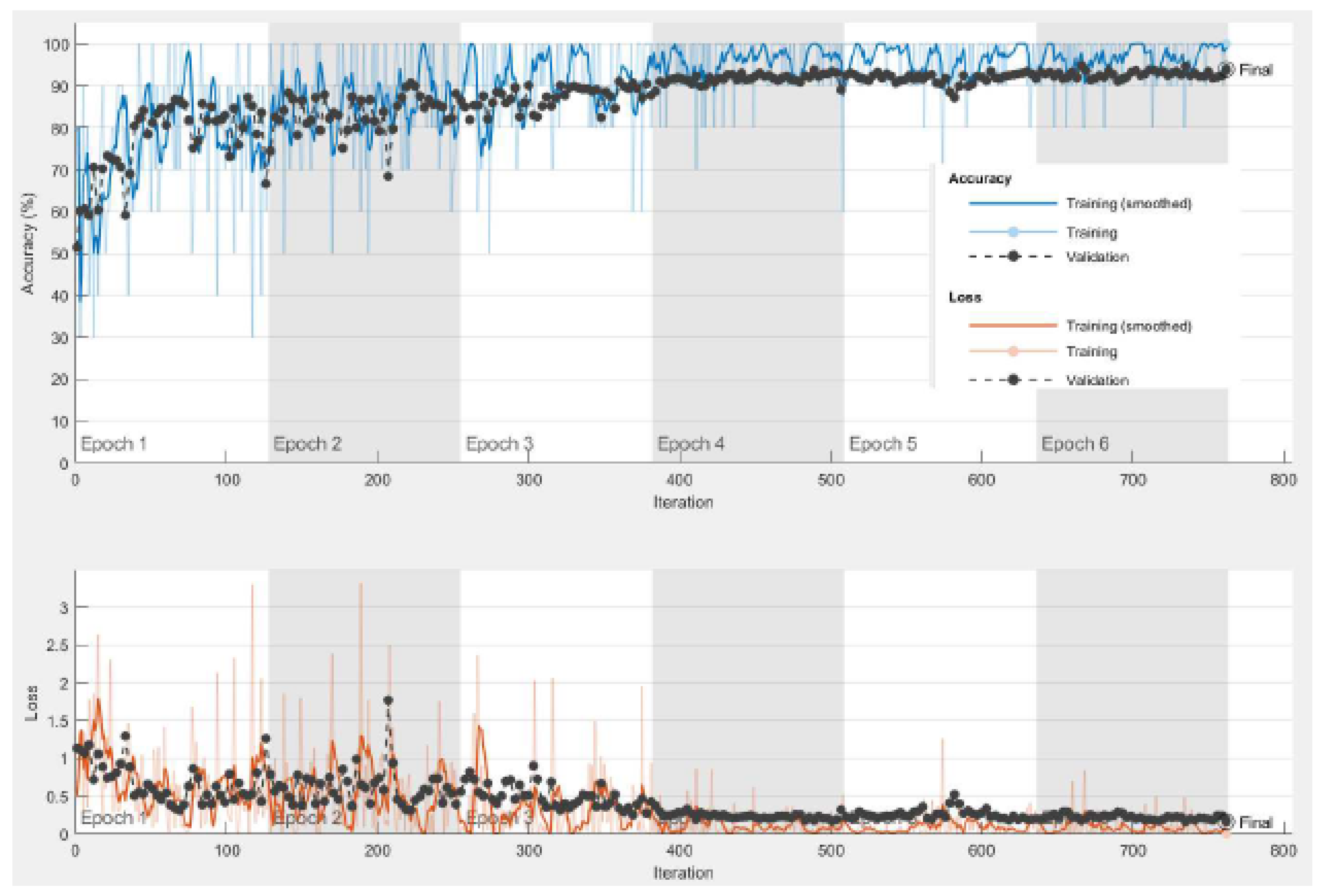
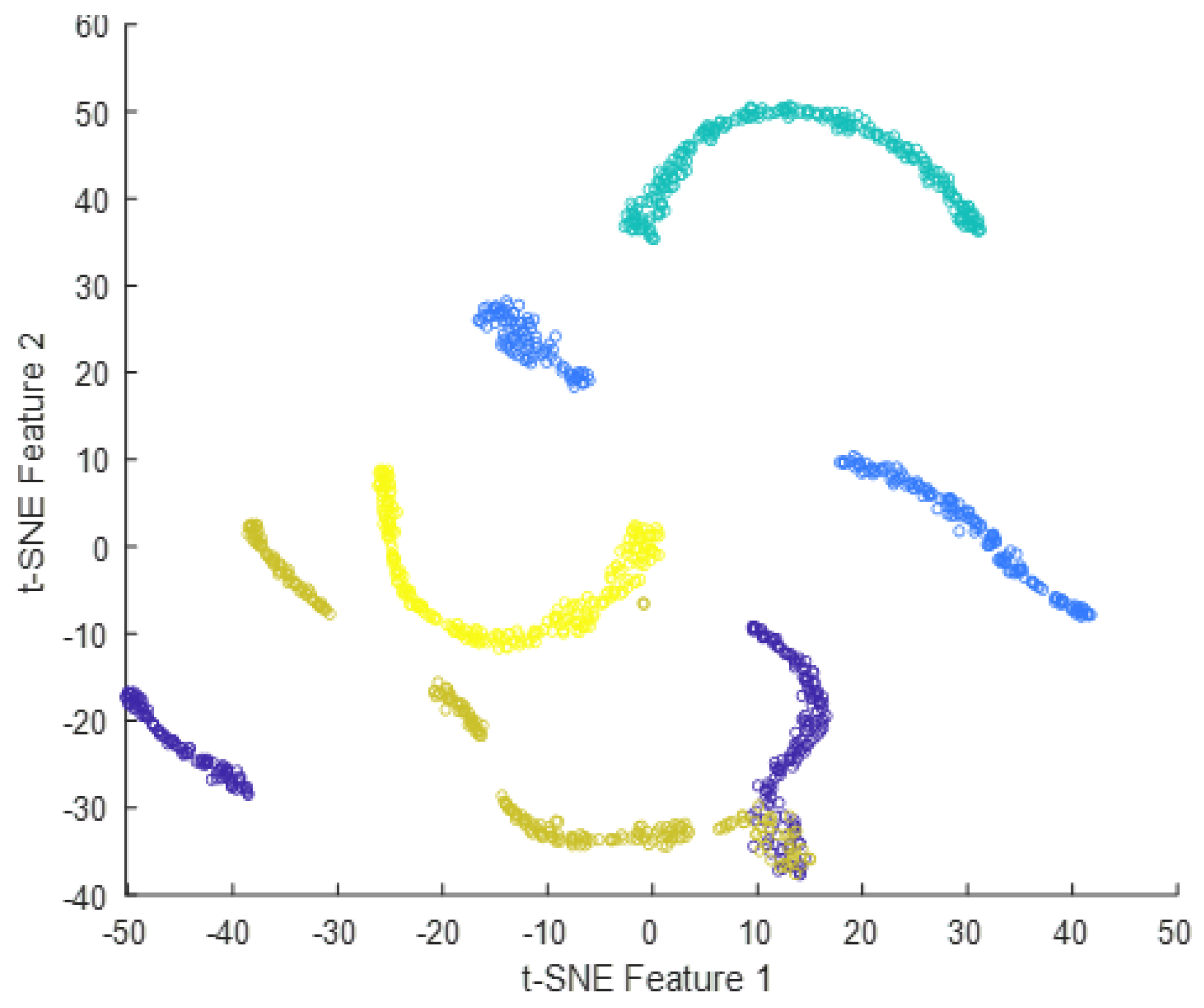
4.2.3. Results for Dataset #3
5. Discussion and Comparison with the-State-of-the-Art Methods
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cruz, A.A. Global Surveillance, Prevention and Control of Chronic Respiratory Diseases: A Comprehensive Approach; World Health Organization: Geneva, Switzerland, 2007.
- GBD Chronic Respiratory Disease Collaborators. Prevalence and attributable health burden of chronic respiratory diseases, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet Respir. Med. 2020, 8, 585–596. [Google Scholar] [CrossRef]
- WHO. World Health Organization Coronavirus Disease 2019 (COVID-19) Situation Report; World Health Organization: Geneva, Switzerland, 2020.
- Rahaman, M.M.; Li, C.; Yao, Y.; Kulwa, F.; Rahman, M.A.; Wang, Q.; Qi, S.; Kong, F.; Zhu, X.; Zhao, X. Identification of COVID-19 samples from chest X-Ray images using deep learning: A comparison of transfer learning approaches. J. X-ray Sci. Technol. 2020, 28, 821–839. [Google Scholar] [CrossRef]
- Alqudah, A.; Alqudah, A.M. Sliding window based deep ensemble system for breast cancer classification. J. Med. Eng. Technol. 2021, 45, 313–323. [Google Scholar] [CrossRef] [PubMed]
- Alquran, H.; Alsleti, M.; Alsharif, R.; Qasmieh, I.A.; Alqudah, A.M.; Harun, N.H.B. Employing texture features of chest x-ray images and machine learning in COVID-19 detection and classification. Mendel 2021, 27, 9–17. [Google Scholar] [CrossRef]
- Ahmed, S.T.; Kadhem, S.M. Using Machine Learning via Deep Learning Algorithms to Diagnose the Lung Disease Based on Chest Imaging: A Survey. Int. J. Interact. Mob. Technol. 2021, 15, 95–112. [Google Scholar] [CrossRef]
- Joshi, R.C.; Yadav, S.; Pathak, V.K.; Malhotra, H.S.; Khokhar, H.V.S.; Parihar, A.; Kohli, N.; Himanshu, D.; Garg, R.K.; Bhatt, M.L.B.; et al. A deep learning-based COVID-19 automatic diagnostic framework using chest X-ray images. Biocybern. Biomed. Eng. 2021, 41, 239–254. [Google Scholar] [CrossRef]
- Qasmieh, I.A.; Alquran, H.; Alqudah, A.M. Occluded iris classification and segmentation using self-customized artificial intelligence models and iterative randomized Hough transform. Int. J. Electr. Comput. Eng. 2021, 11, 4037. [Google Scholar] [CrossRef]
- Alqudah, A.M.; Qazan, S.; Masad, I.S. Artificial intelligence framework for efficient detection and classification of pneumonia using chest radiography images. J. Med. Biol. Eng. 2021, 41, 599–609. [Google Scholar] [CrossRef]
- American Thoracic Society. Diagnostic standards and classification of tuberculosis in adults and children. Am. J. Respir. Crit. Care Med. 2000, 161, 1376–1395. [Google Scholar] [CrossRef]
- Setio, A.A.A.; Traverso, A.; De Bel, T.; Berens, M.S.; van den Bogaard, C.; Cerello, P.; Chen, H.; Dou, Q.; Fantacci, M.E.; Geurts, B.; et al. Validation, comparison, and combination of algorithms for automatic detection of pulmonary nodules in computed tomography images: The LUNA16 challenge. Med. Image Anal. 2017, 42, 1–13. [Google Scholar] [CrossRef]
- Dong, D.; Tang, Z.; Wang, S.; Hui, H.; Gong, L.; Lu, Y.; Xue, Z.; Liao, H.; Chen, F.; Yang, F.; et al. The role of imaging in the detection and management of COVID-19: A review. IEEE Rev. Biomed. Eng. 2020, 14, 16–29. [Google Scholar] [CrossRef] [PubMed]
- Abdulkareem, K.H.; Mohammed, M.A.; Salim, A.; Arif, M.; Geman, O.; Gupta, D.; Khanna, A. Realizing an effective COVID-19 diagnosis system based on machine learning and IOT in smart hospital environment. IEEE Internet Things J. 2021, 8, 15919–15928. [Google Scholar] [CrossRef] [PubMed]
- Silva, P.; Luz, E.; Silva, G.; Moreira, G.; Silva, R.; Lucio, D.; Menotti, D. COVID-19 detection in CT images with deep learning: A voting-based scheme and cross-datasets analysis. Inform. Med. Unlocked 2020, 20, 100427. [Google Scholar] [CrossRef] [PubMed]
- Santos, A.M.; Pererira, B.B.; Seixas, J.M.; Mello, F.C.Q.; Kritski, A.L. Neural networks: An application for predicting smear negative pulmonary tuberculosis. In Advances in Statistical Methods for the Health Sciences; Springer: Berlin/Heidelberg, Germany, 2007; pp. 275–287. [Google Scholar]
- Er, O.; Yumusak, N.; Temurtas, F. Chest diseases diagnosis using artificial neural networks. Expert Syst. Appl. 2010, 37, 7648–7655. [Google Scholar] [CrossRef]
- El-Solh, A.A.; Hsiao, C.B.; Goodnough, S.; Serghani, J.; Grant, B.J. Predicting active pulmonary tuberculosis using an artificial neural network. Chest 1999, 116, 968–973. [Google Scholar] [CrossRef]
- Velichko, E.; Shariaty, F.; Orooji, M.; Pavlov, V.; Pervunina, T.; Zavjalov, S.; Khazaei, R.; Radmard, A.R. Development of computer-aided model to differentiate COVID-19 from pulmonary edema in lung CT scan: EDECOVID-net. Comput. Biol. Med. 2022, 141, 105172. [Google Scholar] [CrossRef]
- Shen, D.; Wu, G.; Suk, H.I. Deep learning in medical image analysis. Ann. Rev. Biomed. Eng. 2017, 19, 221–248. [Google Scholar] [CrossRef]
- Alqudah, A.M.; Alquraan, H.; Qasmieh, I.A.; Al-Badarneh, A. Employing image processing techniques and artificial intelligence for automated eye diagnosis using digital eye fundus images. J. Biomim. Biomater. Biomed. Eng. Trans. Tech. Publ. 2018, 39, 40–56. [Google Scholar] [CrossRef]
- Taher, F.; Shoaib, M.R.; Emara, H.M.; Abdelwahab, K.M.; El-Samie, F.E.A.; Haweel, M.T. Efficient framework for brain tumor detection using different deep learning techniques. Front. Public Health 2022, 10, 959667. [Google Scholar] [CrossRef]
- Alqudah, A.M.; Algharib, H.M.; Algharib, A.M.; Algharib, H.M. Computer-aided diagnosis system for automatic two stages classification of breast mass in digital mammogram images. Biomed. Eng. Appl. Basis Commun. 2019, 31, 1950007. [Google Scholar] [CrossRef]
- Wu, C.; Luo, C.; Xiong, N.; Zhang, W.; Kim, T.H. A greedy deep learning method for medical disease analysis. IEEE Access 2018, 6, 20021–20030. [Google Scholar] [CrossRef]
- Alqudah, A.M.; Alqudah, A. Improving machine learning recognition of colorectal cancer using 3D GLCM applied to different color spaces. Multimed. Tools Appl. 2022, 81, 10839–10860. [Google Scholar] [CrossRef]
- Shoaib, M.R.; Elshamy, M.R.; Taha, T.E.; El-Fishawy, A.S.; Abd El-Samie, F.E. Efficient deep learning models for brain tumor detection with segmentation and data augmentation techniques. Concurr. Comput. Pract. Exp. 2022, 34, e7031. [Google Scholar] [CrossRef]
- Wang, S.; Chen, Z.; Sheng, B. Convergence rate of SVM for kernel-based robust regression. Int. J. Wavelets Multiresolution Inf. Process. 2019, 17, 1950004. [Google Scholar] [CrossRef]
- Hu, S.; Gao, Y.; Niu, Z.; Jiang, Y.; Li, L.; Xiao, X.; Wang, M.; Fang, E.F.; Menpes-Smith, W.; Xia, J.; et al. Weakly supervised deep learning for covid-19 infection detection and classification from ct images. IEEE Access 2020, 8, 118869–118883. [Google Scholar] [CrossRef]
- Liu, Q.; Leung, C.K.; Hu, P. A two-dimensional sparse matrix profile DenseNet for COVID-19 diagnosis using chest CT images. IEEE Access 2020, 8, 213718–213728. [Google Scholar] [CrossRef]
- Emara, H.M.; Shoaib, M.R.; Elwekeil, M.; El-Shafai, W.; Taha, T.E.; El-Fishawy, A.S.; El-Rabaie, E.S.M.; Alshebeili, S.A.; Dessouky, M.I.; Abd El-Samie, F.E. Deep convolutional neural networks for COVID-19 automatic diagnosis. Microsc. Res. Tech. 2021, 84, 2504–2516. [Google Scholar] [CrossRef]
- Ibrahim, F.E.; Emara, H.M.; El-Shafai, W.; Elwekeil, M.; Rihan, M.; Eldokany, I.M.; Taha, T.E.; El-Fishawy, A.S.; El-Rabaie, E.S.M.; Abdellatef, E.; et al. Deep Learning-based Seizure Detection and Prediction from EEG Signals. Int. J. Numer. Methods Biomed. Eng. 2022, 38, e3573. [Google Scholar] [CrossRef]
- Shoaib, M.R.; Emara, H.M.; Elwekeil, M.; El-Shafai, W.; Taha, T.E.; El-Fishawy, A.S.; El-Rabaie, E.S.M.; El-Samie, F.E.A. Hybrid classification structures for automatic COVID-19 detection. J. Ambient. Intell. Humaniz. Comput. 2022, 13, 4477–4492. [Google Scholar] [CrossRef]
- Emara, H.M.; Elwekeil, M.; Taha, T.E.; El-Fishawy, A.S.; El-Rabaie, E.S.M.; Alotaiby, T.; Alshebeili, S.A.; El-Samie, A.; Fathi, E. Hilbert transform and statistical analysis for channel selection and epileptic seizure prediction. Wirel. Pers. Commun. 2021, 116, 3371–3395. [Google Scholar] [CrossRef]
- Shoaib, M.R.; Elshamy, M.R.; Taha, T.E.; El-Fishawy, A.S.; Abd El-Samie, F.E. Efficient brain tumor detection based on deep learning models. J. Phys. Conf. Ser. 2021, 2128, 012012. [Google Scholar] [CrossRef]
- Xu, X.; Jiang, X.; Ma, C.; Du, P.; Li, X.; Lv, S.; Yu, L.; Ni, Q.; Chen, Y.; Su, J.; et al. A deep learning system to screen novel coronavirus disease 2019 pneumonia. Engineering 2020, 6, 1122–1129. [Google Scholar] [CrossRef] [PubMed]
- Chandra, T.B.; Verma, K.; Singh, B.K.; Jain, D.; Netam, S.S. Coronavirus disease (COVID-19) detection in Chest X-Ray images using majority voting based classifier ensemble. Expert Syst. Appl. 2020, 165, 113909. [Google Scholar] [CrossRef] [PubMed]
- Alqudah, A.M.; Qazan, S.; Alqudah, A. Automated systems for detection of COVID-19 using chest X-ray images and lightweight convolutional neural networks. Res. Sq. 2020. [Google Scholar] [CrossRef]
- Alqudah, A.M.; Qazan, S.; Alquran, H.; Qasmieh, I.A.; Alqudah, A. COVID-19 detection from x-ray images using different artificial intelligence hybrid models. Jordan J. Electr. Eng. 2020, 6, 168–178. [Google Scholar] [CrossRef]
- Bhowmik, R.T.; Most, S.P. A Personalized Respiratory Disease Exacerbation Prediction Technique Based on a Novel Spatio-Temporal Machine Learning Architecture and Local Environmental Sensor Networks. Electronics 2022, 11, 2562. [Google Scholar] [CrossRef]
- Kim, S.; Rim, B.; Choi, S.; Lee, A.; Min, S.; Hong, M. Deep Learning in Multi-Class Lung Diseases’ Classification on Chest X-ray Images. Diagnostics 2022, 12, 915. [Google Scholar] [CrossRef]
- Al Shehri, W.; Almalki, J.; Mehmood, R.; Alsaif, K.; Alshahrani, S.M.; Jannah, N.; Alangari, S. A Novel COVID-19 Detection Technique Using Deep Learning Based Approaches. Sustainability 2022, 14, 12222. [Google Scholar] [CrossRef]
- Rasheed, J.; Shubair, R.M. Screening Lung Diseases Using Cascaded Feature Generation and Selection Strategies. Healthcare 2022, 10, 1313. [Google Scholar] [CrossRef]
- Hong, M.; Rim, B.; Lee, H.; Jang, H.; Oh, J.; Choi, S. Multi-class classification of lung diseases using CNN models. Appl. Sci. 2021, 11, 9289. [Google Scholar] [CrossRef]
- Pradhan, K.; Chawla, P.; Rawat, S. A deep learning-based approach for detection of lung cancer using self adaptive sea lion optimization algorithm (SA-SLnO). J. Ambient. Intell. Humaniz. Comput. 2022, 1–15. [Google Scholar] [CrossRef]
- Pradhan, K.S.; Chawla, P.; Tiwari, R. HRDEL: High ranking deep ensemble learning-based lung cancer diagnosis model. Expert Syst. Appl. 2023, 213, 118956. [Google Scholar] [CrossRef]
- Souid, A.; Sakli, N.; Sakli, H. Classification and predictions of lung diseases from chest x-rays using mobilenet v2. Appl. Sci. 2021, 11, 2751. [Google Scholar] [CrossRef]
- Biswas, S.; Chatterjee, S.; Majee, A.; Sen, S.; Schwenker, F.; Sarkar, R. Prediction of COVID-19 from chest CT images using an ensemble of deep learning models. Appl. Sci. 2021, 11, 7004. [Google Scholar] [CrossRef]
- Akter, S.; Shamrat, F.J.M.; Chakraborty, S.; Karim, A.; Azam, S. COVID-19 detection using deep learning algorithm on chest X-ray images. Biology 2021, 10, 1174. [Google Scholar] [CrossRef] [PubMed]
- Rahman, T.; Chowdhury, M.E.; Khandakar, A.; Islam, K.R.; Islam, K.F.; Mahbub, Z.B.; Kadir, M.A.; Kashem, S. Transfer Learning with Deep Convolutional Neural Network (CNN) for Pneumonia Detection using Chest X-ray. Appl. Sci. 2020, 10, 3233. [Google Scholar] [CrossRef]
- Ferreira, J.R.; Cardenas, D.A.C.; Moreno, R.A.; de Sá Rebelo, M.D.F.; Krieger, J.E.; Gutierrez, M.A. Multi-View Ensemble Convolutional Neural Network to Improve Classification of Pneumonia in Low Contrast Chest X-Ray Images. In Proceedings of the 2020 42nd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Montreal, QB, Canada, 20–24 July 2020; pp. 1238–1241. [Google Scholar]
- Raina, A.; Mahajan, S.; Vanipriya, C.; Bhardwaj, A.; Pandit, A.K. COVID-19 Detection: An Approach Using X-Ray Images and Deep Learning Techniques. In Advances in Intelligent Computing and Communication; Springer: Berlin/Heidelberg, Germany, 2021; pp. 7–16. [Google Scholar]
- Zhang, Y.D.; Zhang, Z.; Zhang, X.; Wang, S.H. MIDCAN: A multiple input deep convolutional attention network for COVID-19 diagnosis based on chest CT and chest X-ray. Pattern Recognit. Lett. 2021, 150, 8–16. [Google Scholar] [CrossRef]
- Wang, S.H.; Nayak, D.R.; Guttery, D.S.; Zhang, X.; Zhang, Y.D. COVID-19 classification by CCSHNet with deep fusion using transfer learning and discriminant correlation analysis. Inf. Fusion 2021, 68, 131–148. [Google Scholar] [CrossRef]
- He, Z.; Cao, Y.; Du, L.; Xu, B.; Yang, J.; Cao, Y.; Tang, S.; Zhuang, Y. Mrfn: Multi-receptive-field network for fast and accurate single image super-resolution. IEEE Trans. Multimed. 2019, 22, 1042–1054. [Google Scholar] [CrossRef]
- Mehrrotraa, R.; Ansari, M.; Agrawal, R.; Tripathi, P.; Heyat, M.B.B.; Al-Sarem, M.; Muaad, A.Y.M.; Nagmeldin, W.A.E.; Abdelmaboud, A.; Saeed, F. Ensembling of efficient deep convolutional networks and machine learning algorithms for resource effective detection of tuberculosis using thoracic (chest) radiography. IEEE Access 2022, 10, 85442–85458. [Google Scholar] [CrossRef]
- Mehrotra, R.; Agrawal, R.; Ansari, M. Diagnosis of hypercritical chronic pulmonary disorders using dense convolutional network through chest radiography. Multimed. Tools Appl. 2022, 81, 7625–7649. [Google Scholar] [CrossRef] [PubMed]
- Masad, I.S.; Alqudah, A.; Alqudah, A.M.; Almashaqbeh, S. A hybrid deep learning approach towards building an intelligent system for pneumonia detection in chest X-ray images. Int. J. Electr. Comput. Eng. 2021, 11, 5530–5540. [Google Scholar] [CrossRef]
- Al-Issa, Y.; Alqudah, A.M.; Alquran, H.; Al Issa, A. Pulmonary diseases decision support system using deep learning approach. Comput. Mater. Contin. 2022, 73, 311–326. [Google Scholar] [CrossRef]
- Kaggle. Paultimothymooney. Available online: https://www.kaggle.com/paultimothymooney/chest-xray-pneumonia (accessed on 19 October 2020).
- Kaggle. Abnormalities. Available online: https://www.kaggle.com/kmader/pulmonary-chest-xray-abnormalities (accessed on 19 October 2020).
- Kaggle. Paultimothymooney. Available online: hhttps://www.kaggle.com/datasets/paultimothymooney/chest-xray-pneumonia (accessed on 19 April 2022).
- Kaggle. Datasets. Available online: https://www.kaggle.com/datasets/tawsifurrahman/tuberculosis-tb-chest-xray-dataset (accessed on 19 April 2022).
- Kaggle. Code. Available online: https://www.kaggle.com/code/sana306/detection-of-covid-positive-cases-using-dl/data (accessed on 19 April 2022).
- Kaggle. Datasets. Available online: https://www.kaggle.com/datasets/luisblanche/covidct (accessed on 19 April 2022).
- Kaggle. Datasets. Available online: https://www.kaggle.com/datasets/mohamedhanyyy/chest-ctscan-images (accessed on 19 April 2022).
- Kaggle. Datasets. Available online: https://www.kaggle.com/datasets/maedemaftouni/large-covid19-ct-slice-dataset (accessed on 19 April 2022).
- Ilesanmi, A.E.; Ilesanmi, T.O. Methods for image denoising using convolutional neural network: A review. Complex Intell. Syst. 2021, 7, 2179–2198. [Google Scholar] [CrossRef]
- Szegedy, C.; Ioffe, S.; Vanhoucke, V.; Alemi, A. Inception-v4, inception-resnet and the impact of residual connections on learning. In Proceedings of the AAAI Conference on Artificial Intelligence, San Francisco, CA, USA, 4–9 February 2017; Volume 31. [Google Scholar]
- Gonwirat, S.; Surinta, O. Improving Recognition of Thai Handwritten Characters with Deep Convolutional Neural Networks. In Proceedings of the 2020 The 3rd International Conference on Information Science and System, Cambridge, UK, 19–20 March 2020; pp. 82–87. [Google Scholar]
- Xu, P.; Chan, A.K. Support vector machines for multi-class signal classification with unbalanced samples. In Proceedings of the International Joint Conference on Neural Networks, Hong Kong, China, 1–8 June 2003; Volume 2, pp. 1116–1119. [Google Scholar]
- Chamasemani, F.F.; Singh, Y.P. Multi-class support vector machine (SVM) classifiers–an application in hypothyroid detection and classification. In Proceedings of the 2011 Sixth International Conference on Bio-Inspired Computing: Theories and Applications, Penang, Malaysia, 27–29 September 2011; pp. 351–356. [Google Scholar]
- Hsu, C.W.; Lin, C.J. A comparison of methods for multiclass support vector machines. IEEE Trans. Neural Netw. 2002, 13, 415–425. [Google Scholar] [PubMed]
- Taha, A.A.; Hanbury, A. Metrics for evaluating 3D medical image segmentation: Analysis, selection, and tool. BMC Med. Imaging 2015, 15, 29. [Google Scholar] [CrossRef]
- Tharwat, A. Classification assessment methods. Appl. Comput. Inform. 2020, 17, 168–192. [Google Scholar] [CrossRef]
- Jaiswal, A.; Gianchandani, N.; Singh, D.; Kumar, V.; Kaur, M. Classification of the COVID-19 infected patients using DenseNet201 based deep transfer learning. J. Biomol. Struct. Dyn. 2020, 39, 5682–5689. [Google Scholar] [CrossRef]



















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dataset | Lung Disease | |||||
|---|---|---|---|---|---|---|
| Dataset #1 X-ray images | COVID-19 | TB | Pneumonia-bacterial | Pneumonia-viral | Normal | |
| 259 | 800 | 900 | 800 | 1000 | ||
| Dataset #2 X-ray images | COVID-19 | Lung opacity | TB | Pneumonia-viral | Normal | |
| 3616 | 6012 | 8624 | 3080 | 10,192 | ||
| Dataset #3 CT images | COVID-19 | Adenocarcinoma | Large cell carcinoma | Squamous cell carcinoma | CAP | Normal |
| 7942 | 4290 | 2508 | 3410 | 2618 | 7290 | |
| Parameter | Value |
|---|---|
| Penalty parameter C | 1.0 |
| Kernel | Polynomial |
| Degree | 3.0 |
| Gamma | Scale |
| Tolerance | 0.001 |
| Decision function shape | One versus rest |
| Number of iteration |
| Models | Evaluation Metrics | |||||||
|---|---|---|---|---|---|---|---|---|
| Accuracy | Sensitivity | Speci city | Precision | MCC | F1 Score | Fpr | ||
| Without Augmentation | Resnet101 | 77.24 | 74.53 | 80.77 | 72.19 | 65.85 | 75.16 | 0.197 |
| Inceptionv3 | 78.52 | 75.12 | 80.97 | 73.43 | 67.37 | 77.98 | 0.158 | |
| InceptionResNetv2 | 80.86 | 78.23 | 84.67 | 75.72 | 69.57 | 78.12 | 0.148 | |
| With Augmentation | Resnet101 | 78.25 | 75.43 | 82.37 | 73.29 | 67.15 | 76.86 | 0.094 |
| Inceptionv3 | 80.12 | 77.67 | 86.05 | 75.72 | 70.21 | 78.08 | 0.088 | |
| InceptionResNetv2 | 81.86 | 79.58 | 86.57 | 78.78 | 70.56 | 78.84 | 0.084 | |
| Models | Evaluation Metrics | ||||||
|---|---|---|---|---|---|---|---|
| Acc | Sen | Spec | Preci | Mcc | F1 Score | Fpr | |
| Resnet101 | 83.21 | 83.03 | 90.37 | 81.89 | 80.15 | 81.02 | 0.074 |
| Inceptionv3 | 85.34 | 85.34 | 95.11 | 85.12 | 82.21 | 82.36 | 0.0489 |
| InceptionResNetv2 | 86.80 | 87.47 | 96.78 | 87.01 | 83.98 | 86.86 | 0.0322 |
| Models | Evaluation Metrics | ||||||
|---|---|---|---|---|---|---|---|
| Acc | Sen | Spec | Prec | Mcc | F1 Score | Fpr | |
| ResNet101 | 90.16 | 89.34 | 95.478 | 90.32 | 89.11 | 90.78 | 0.0314 |
| Inceptionv3 | 92.85 | 91.44 | 96.56 | 92.76 | 90.17 | 92.31 | 0.0278 |
| InceptionResnetv2 | 95.24 | 95.76 | 96.38 | 96.51 | 92.18 | 95.36 | 0.0157 |
| Models | Evaluation Metrics | ||||||
|---|---|---|---|---|---|---|---|
| Acc | Sen | Spec | Preci | Mcc | F1 Score | Fpr | |
| Resnet101 | 91.24 | 91.22 | 97.08 | 91.20 | 88.29 | 91.08 | 0.0292 |
| Inceptionv3 | 93.15 | 93.14 | 97.72 | 93.14 | 90.85 | 93.11 | 0.0228 |
| InceptionResnetv2 | 96.80 | 97.47 | 98.78 | 97.01 | 93.98 | 96.86 | 0.0122 |
| Models | Evaluation Metrics | ||||||
|---|---|---|---|---|---|---|---|
| Acc | Sen | Spec | Prec | Mcc | F1 Score | Fpr | |
| ResNet101 | 92.441 | 92.513 | 98.153 | 89.10 | 88.711 | 90.35 | 0.0601 |
| Inceptionv3 | 93.85 | 92.64 | 96.86 | 92.20 | 90.02 | 92.56 | 0.0534 |
| InceptionResnetv2 | 96.309 | 96.39 | 99.22 | 96.41 | 96.39 | 95.62 | 0.0369 |
| Models | Evaluation Metrics | ||||||
|---|---|---|---|---|---|---|---|
| Acc | Sen | Spec | Prec | Mcc | F1 Score | Fpr | |
| ResNet101 | 91.78 | 92.80 | 97.13 | 90.10 | 89.821 | 91.455 | 0.0172 |
| Inceptionv3 | 91.99 | 91.94 | 97.08 | 92.45 | 90.98 | 92.87 | 0.0132 |
| InceptionResnetv2 | 93.45 | 92.76 | 98.58 | 92.51 | 92.78 | 90.56 | 0.0131 |
| Models | Evaluation Metrics | ||||||
|---|---|---|---|---|---|---|---|
| Acc | Sen | Spec | Prec | Mcc | F1 Score | Fpr | |
| ResNet101 | 94.51 | 90.23 | 98.57 | 91.32 | 90.41 | 92.25 | 0.0132 |
| Inceptionv3 | 94.54 | 90.62 | 98.69 | 93.21 | 92.13 | 92.34 | 0.0118 |
| InceptionResnetv2 | 98.028 | 98.513 | 99.55 | 98.64 | 98.57 | 98.13 | 0.0044 |
| Models | Evaluation Metrics | ||||||
|---|---|---|---|---|---|---|---|
| Acc | Sen | Spec | Prec | Mcc | F1 Score | Fpr | |
| ResNet101 | 91.51 | 92.23 | 97.57 | 90.32 | 89.41 | 91.25 | 0.0168 |
| Inceptionv3 | 91.54 | 91.62 | 97.69 | 92.21 | 91.13 | 92.87 | 0.0131 |
| InceptionResnetv2 | 92.56 | 92.16 | 98.52 | 92.31 | 92.67 | 90.78 | 0.0128 |
| Dataset | Models | Evaluation Metrics | ||||||
|---|---|---|---|---|---|---|---|---|
| Accuracy | Sensitivity | Specicity | Precision | MCC | F1 Score | Fpr | ||
| #1 | Resnet101 + MCSVM | 91.24 | 91.22 | 97.08 | 91.20 | 88.29 | 91.08 | 0.0292 |
| Inceptionv3 + MCSVM | 93.15 | 93.14 | 97.72 | 93.14 | 90.85 | 93.11 | 0.0228 | |
| InceptionResNetv2 + MCSVM | 96.80 | 97.47 | 98.78 | 97.01 | 93.98 | 96.86 | 0.0122 | |
| #2 | Resnet101 + Softmax | 92.441 | 92.513 | 98.153 | 89.10 | 88.711 | 90.35 | 0.0601 |
| Inceptionv3 + Softmax | 93.85 | 92.64 | 96.86 | 92.20 | 90.02 | 92.56 | 0.0534 | |
| InceptionResNetv2 + Softmax | 96.309 | 96.39 | 99.22 | 96.41 | 96.39 | 95.62 | 0.0131 | |
| #3 | Resnet101 + Softmax | 94.51 | 90.23 | 98.57 | 91.32 | 90.41 | 92.25 | 0.0132 |
| Inceptionv3 + Softmax | 94.54 | 90.62 | 98.69 | 93.21 | 92.13 | 92.34 | 0.0118 | |
| InceptionResNetv2 + Softmax | 98.028 | 98.513 | 99.55 | 98.64 | 98.57 | 98.13 | 0.0044 | |
| Laptop Specifications | Core 10th Generation, 32 bit RAM, Nvidia RTX 2070, Gpu and Hard Tera SSD with Matlab 2020b Version |
|---|---|
| Method | Computational Time (s) |
| ResNet101 Features + MCSVM | 139.9 |
| Inceptionv3 Features + MCSVM | 130.9 |
| InceptionResNetv2 Features + MCSVM | 136.7 |
| Resnet101 + Softmax | 221.7 |
| Inceptionv3 + Softmax | 199.4 |
| InceptionResNetv2 + Softmax | 216.2 |
| ResNet101 Features + MCSVM + SR | 298.2 |
| Inceptionv3 Features + MCSVM + SR | 221.5 |
| InceptionResNetv2 Features + MCSVM + SR | 230.7 |
| Authors | Task | Technique | Accuracy (%) |
|---|---|---|---|
| Xu et al. [35] | Viral Pneumonia, Normal, and COVID-19 | 3D DL model | 86.7 |
| Chandra et al. [36] | Normal and COVID-19 | Automatic COVID screening (ACoS) | 98.06 |
| COVID-19 and Pneumonia | 91.23 | ||
| Rahman et al. [49] | Normal and Pneumonia | CNN-AlexNet, ResNet18, DenseNet201, and SqueezeNet TL-based models | 98 |
| Normal, Bacterial pneumonia and Viral pneumonia | 93.3 | ||
| Bacterial pneumonia and Viral pneumonia | 95 | ||
| Ferreira et al. [50] | Normal and Pneumonia | Histogram equalization+ VGG16 CNN +MLP classifier | 97.4 |
| Bacterial pneumonia and Viral pneumonia | 92.1 | ||
| Jaiswal et al. [75] | Normal and COVID-19 | DenseNet201 TL-based model | 96.23 |
| Proposed model | Normal, COVID-19, Viral pneumonia Bacterial pneumonia and TB | SR + Inceptioesnetv2+Softmax | 95.24 |
| SR + Inceptioesnetv2+MCSVM | 96.80 | ||
| Normal, COVID-19, Viral pneumonia Lung opacity, Pneumonia and TB | SR + Inceptioesnetv2+Softmax | 96.309 | |
| SR + Inceptioesnetv2+MCSVM | 93.45 | ||
| COVID-19, Non-COVID-19, Large cell carcinoma, Squamous cell carcinoma and CAP | SR + Inceptioesnetv2+Softmax | 98.028 | |
| SR + Inceptioesnetv2+MCSVM | 92.56 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Emara, H.M.; Shoaib, M.R.; El-Shafai, W.; Elwekeil, M.; Hemdan, E.E.-D.; Fouda, M.M.; Taha, T.E.; El-Fishawy, A.S.; El-Rabaie, E.-S.M.; El-Samie, F.E.A. Simultaneous Super-Resolution and Classification of Lung Disease Scans. Diagnostics 2023, 13, 1319. https://doi.org/10.3390/diagnostics13071319
Emara HM, Shoaib MR, El-Shafai W, Elwekeil M, Hemdan EE-D, Fouda MM, Taha TE, El-Fishawy AS, El-Rabaie E-SM, El-Samie FEA. Simultaneous Super-Resolution and Classification of Lung Disease Scans. Diagnostics. 2023; 13(7):1319. https://doi.org/10.3390/diagnostics13071319
Chicago/Turabian StyleEmara, Heba M., Mohamed R. Shoaib, Walid El-Shafai, Mohamed Elwekeil, Ezz El-Din Hemdan, Mostafa M. Fouda, Taha E. Taha, Adel S. El-Fishawy, El-Sayed M. El-Rabaie, and Fathi E. Abd El-Samie. 2023. "Simultaneous Super-Resolution and Classification of Lung Disease Scans" Diagnostics 13, no. 7: 1319. https://doi.org/10.3390/diagnostics13071319
APA StyleEmara, H. M., Shoaib, M. R., El-Shafai, W., Elwekeil, M., Hemdan, E. E.-D., Fouda, M. M., Taha, T. E., El-Fishawy, A. S., El-Rabaie, E.-S. M., & El-Samie, F. E. A. (2023). Simultaneous Super-Resolution and Classification of Lung Disease Scans. Diagnostics, 13(7), 1319. https://doi.org/10.3390/diagnostics13071319