
FcRn Expression in Endometrial Cancer and Its Association with Clinicopathologic Features

 ,
,
Abstract
:1. Introduction
2. Material and Methods
2.1. Patients
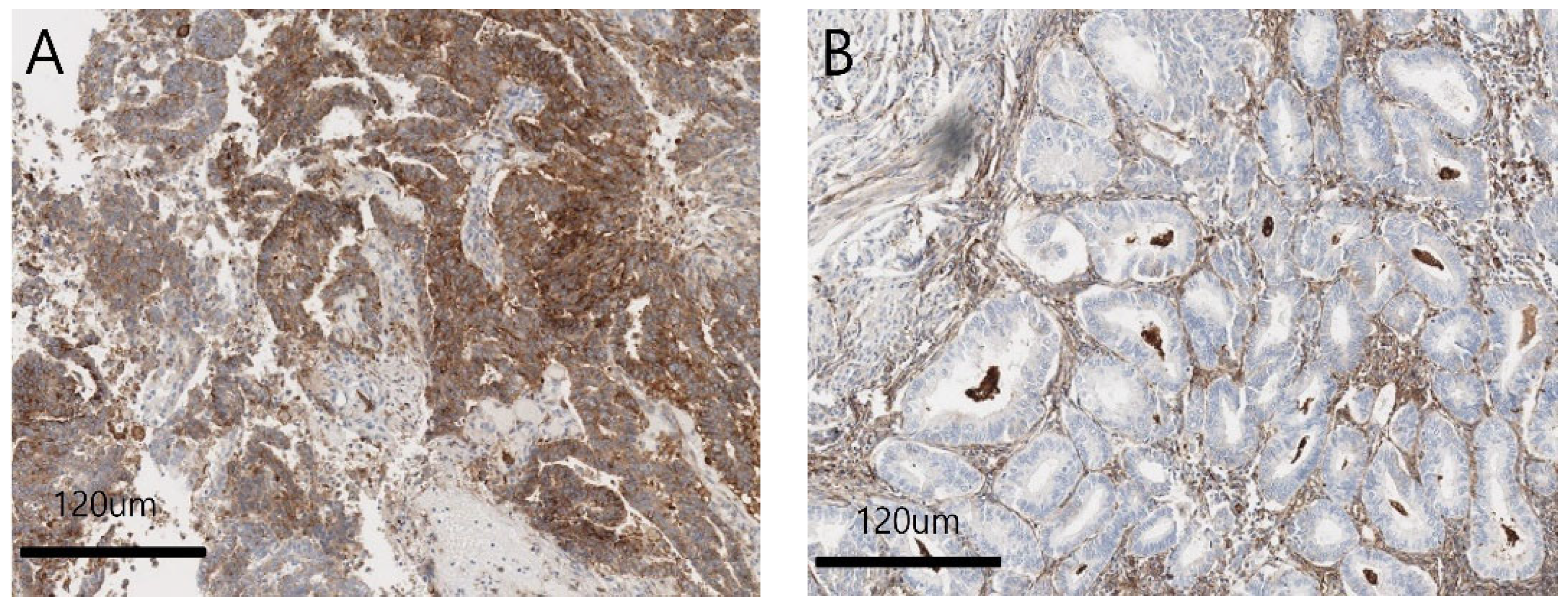
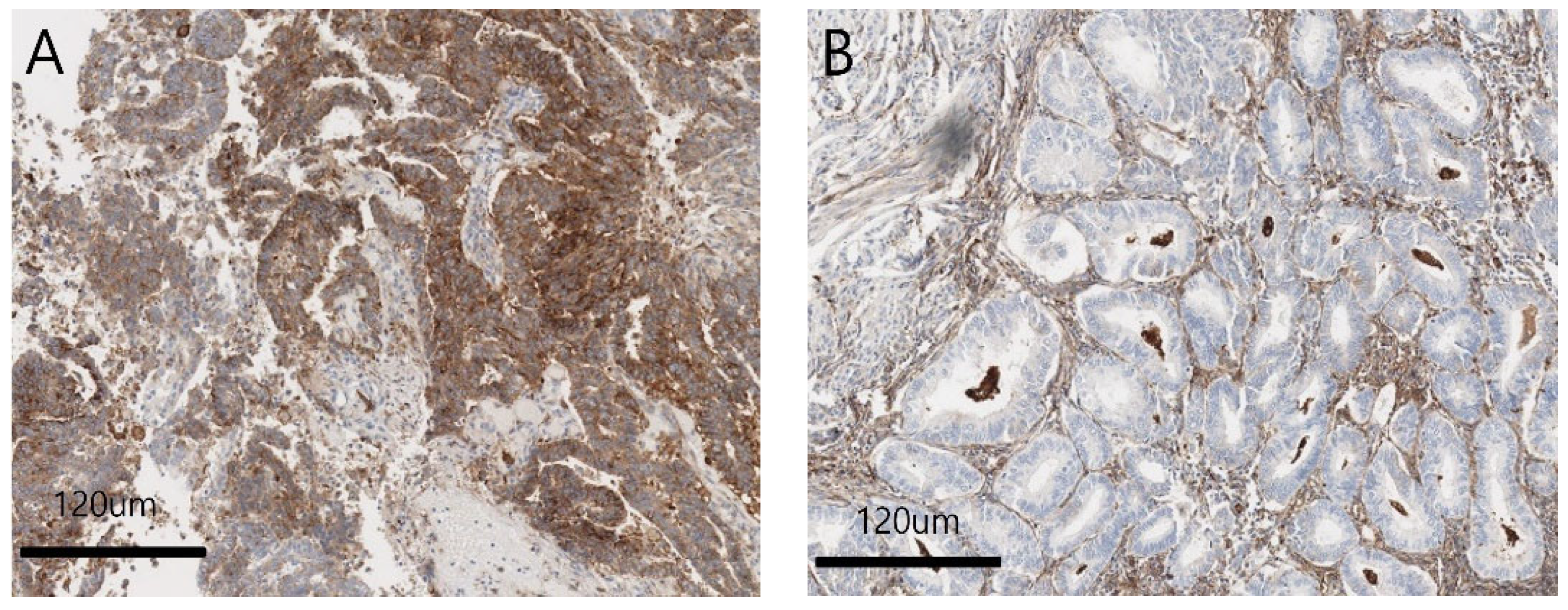
2.2. TMA and Immunohistochemical Analysis
2.3. Ishikawa Cell Line Experiments
2.3.1. Cell Culture
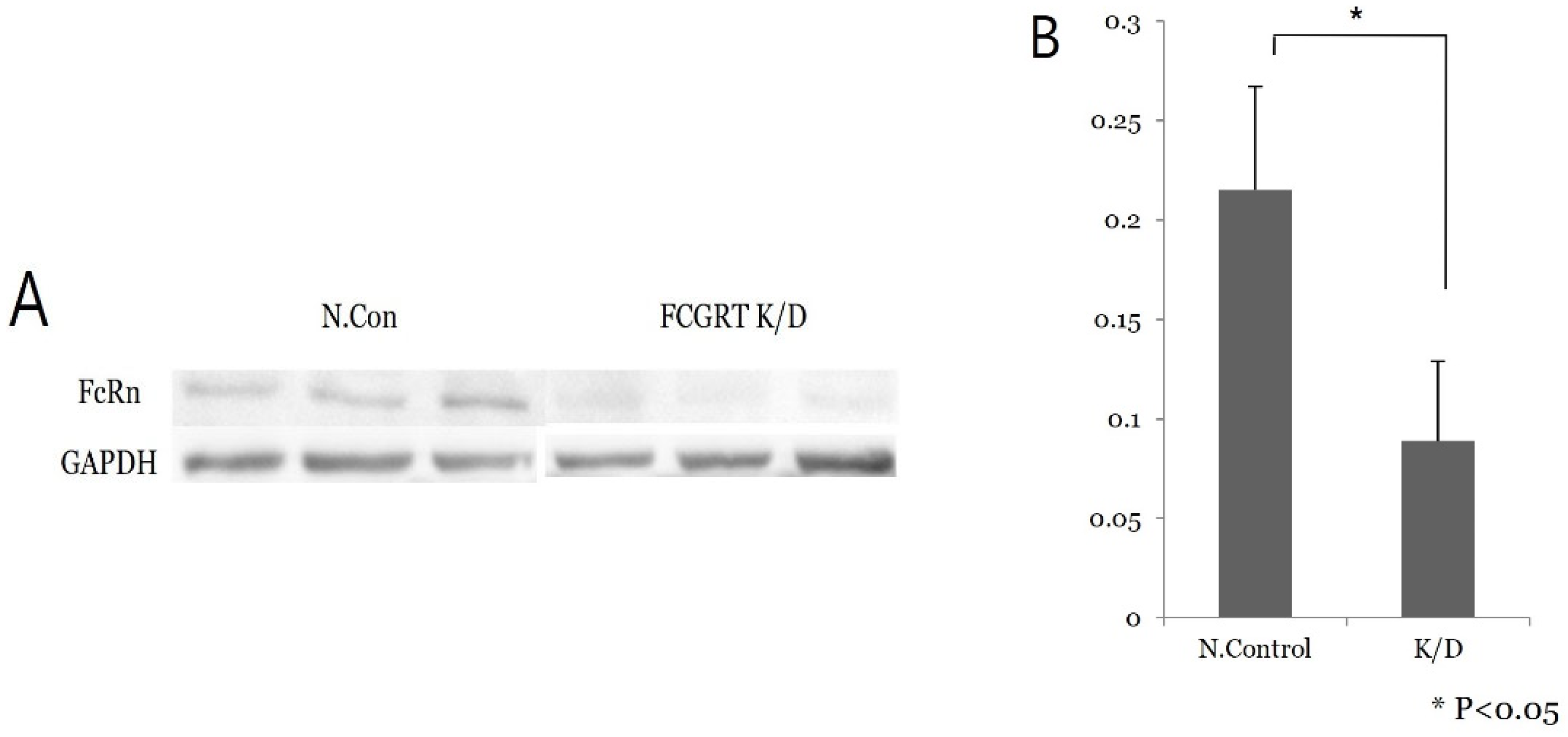
2.3.2. Knock-Down of FcRn
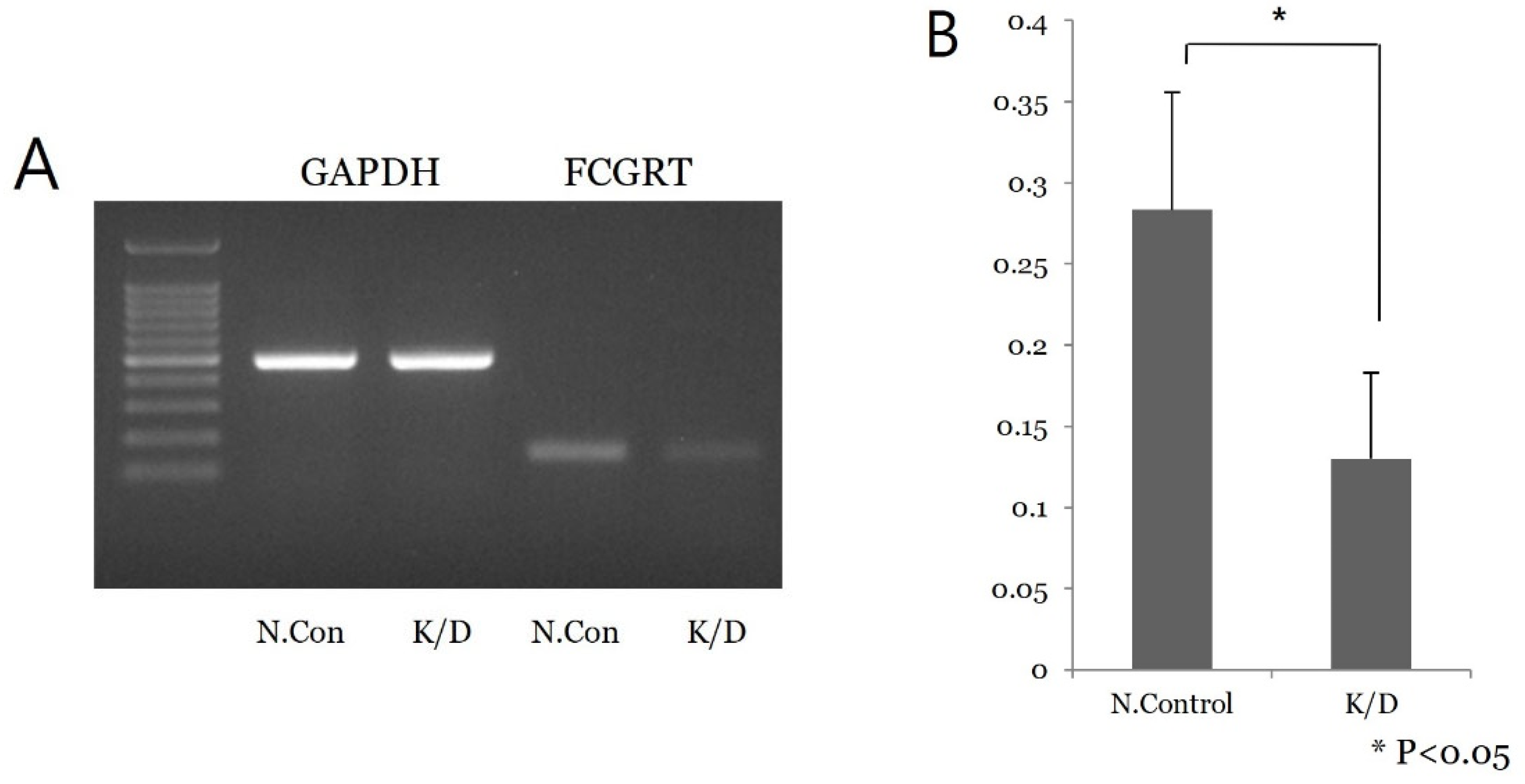
2.3.3. Semiquantitative PCR Analysis
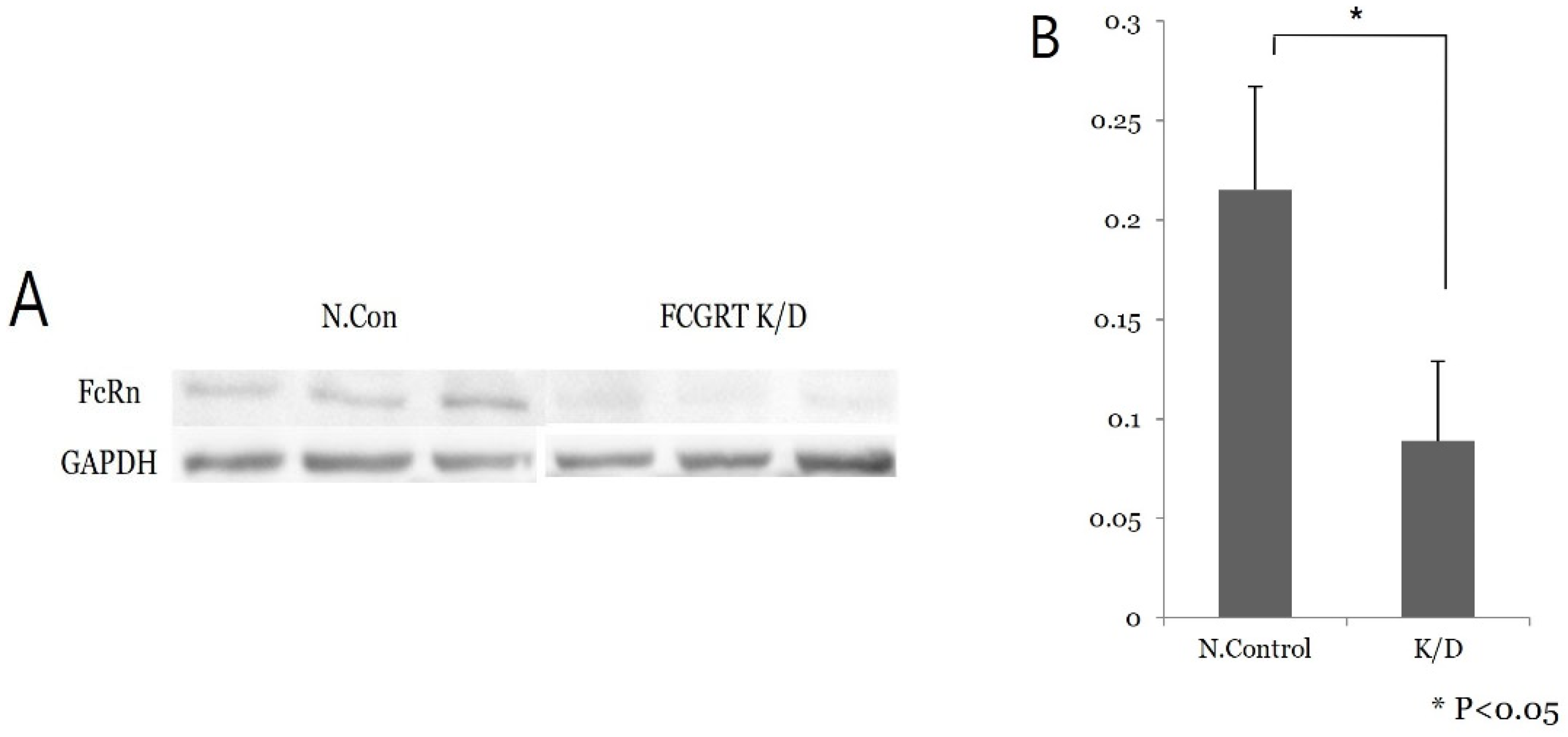
2.3.4. Western Blot Analysis
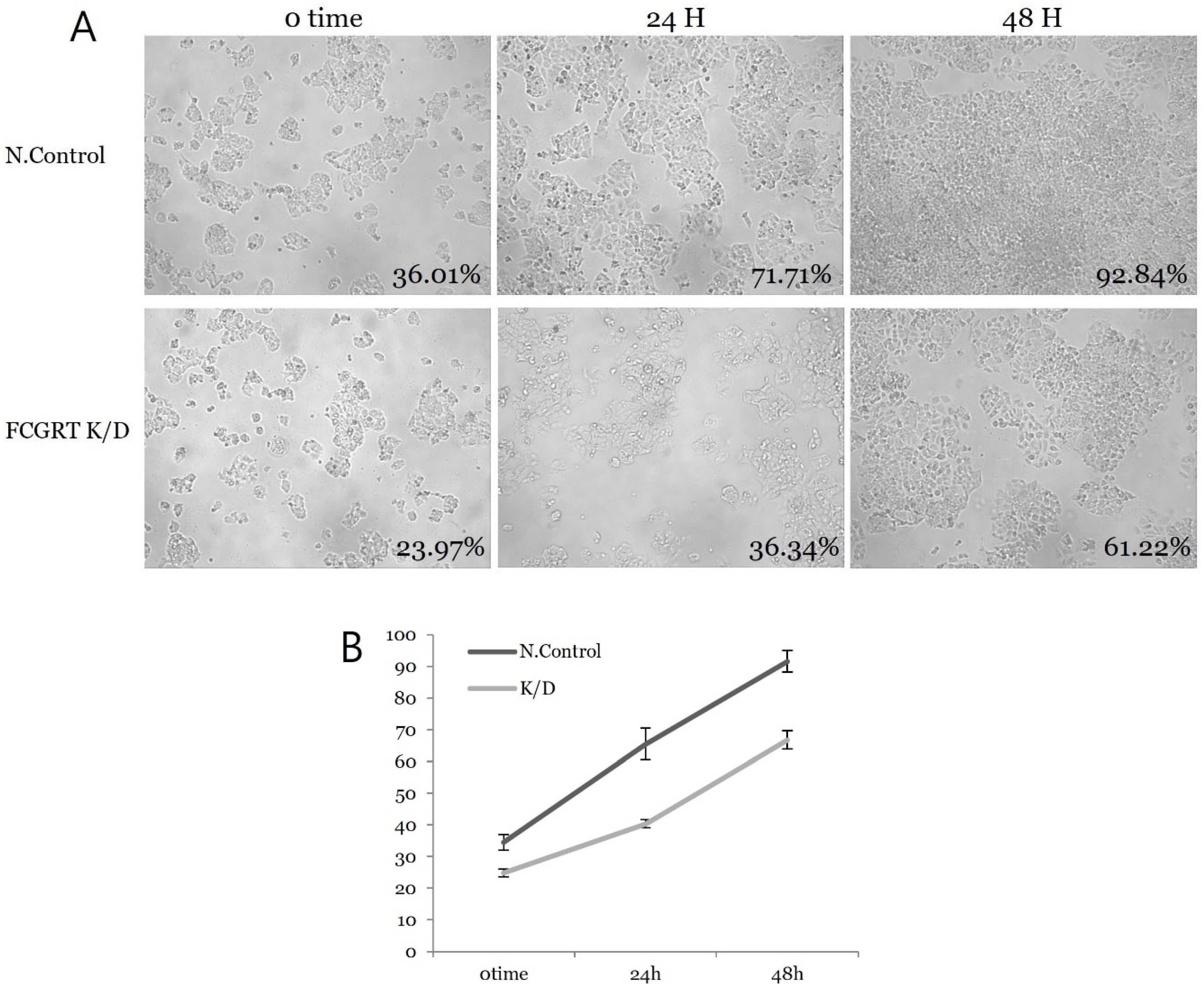
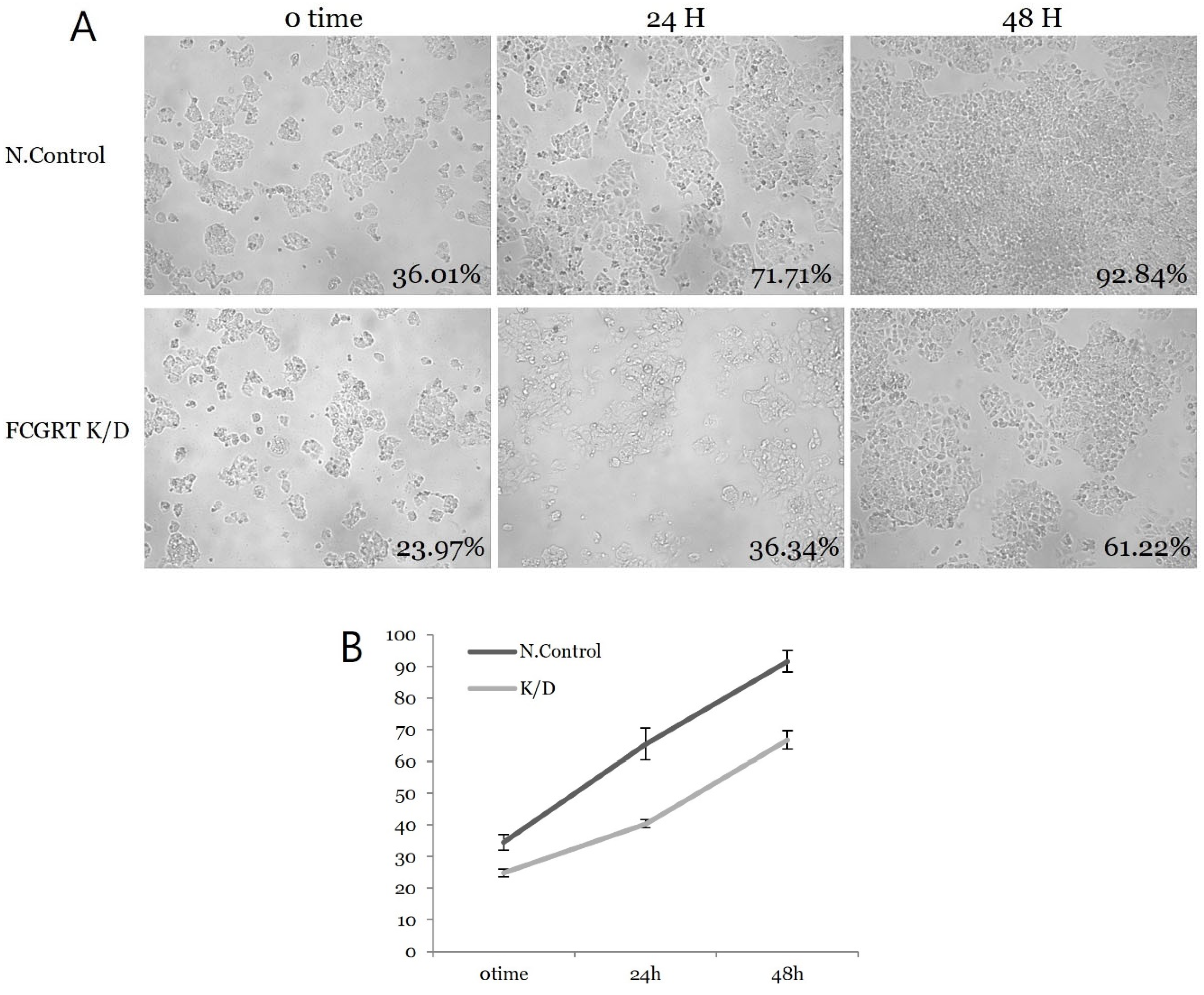
2.3.5. Cell Proliferation
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Correlation of FcRn Expression with Clinicopathological Features
3.3. FcRn Expression in Ishikawa Cell Culture
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F.; Bsc, M.F.B.; Me, J.F.; Soerjomataram, M.I.; et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Gu, B.; Shang, X.; Yan, M.; Li, X.; Wang, W.; Wang, Q.; Zhang, C. Variations in incidence and mortality rates of endometrial cancer at the global, regional, and national levels, 1990–2019. Gynecol. Oncol. 2021, 161, 573–580. [Google Scholar] [CrossRef]
- Cancer Genome Atlas Research Network; Kandoth, C.; Schultz, N.; Cherniack, A.D.; Akbani, R.; Liu, Y.; Getz, G.; Gabriel, S.B.; Cibulskis, K.; Lander, E.; et al. Integrated genomic characterization of endometrial carcinoma. Nature 2013, 497, 67–73. [Google Scholar] [PubMed]
- Concin, N.; Matias-Guiu, X.; Vergote, I.; Cibula, D.; Mirza, M.R.; Marnitz, S.; Ledermann, J.; Bosse, T.; Chargari, C.; Fagotti, A.; et al. ESGO/ESTRO/ESP guidelines for the management of patients with endometrial carcinoma. Int. J. Gynecol. Cancer 2021, 31, 12–39. [Google Scholar] [CrossRef] [PubMed]
- Walsh, C.S.; Hacker, K.E.; Secord, A.A.; DeLair, D.F.; McCourt, C.; Urban, R. Molecular testing for endometrial cancer: An SGO clinical practice statement. Gynecol. Oncol. 2023, 168, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Jamieson, A.; Barroilhet, L.M.; McAlpine, J.N. Molecular classification in endometrial cancer: Opportunities for precision oncology in a changing landscape. Cancer 2022, 128, 2853–2857. [Google Scholar] [CrossRef] [PubMed]
- Berek, J.S.; Matias-Guiu, X.; Creutzberg, C.; Fotopoulou, C.; Gaffney, D.; Kehoe, S.; Lindemann, K.; Mutch, D.; Concin, N.; Endometrial Cancer Staging Subcommittee; et al. FIGO staging of endometrial cancer: 2023. J. Gynecol. Oncol. 2023, 34, e85. [Google Scholar] [CrossRef]
- Simister, N.E.; Rees, A.R. Isolation and characterization of an Fc receptor from neonatal rat small intestine. Eur. J. Immunol. 1985, 15, 733–738. [Google Scholar] [CrossRef]
- van der Vusse, G.J. Albumin as fatty acid transporter. Drug Metab. Pharmacokinet. 2009, 24, 300–307. [Google Scholar] [CrossRef]
- Larsen, M.T.; Kuhlmann, M.; Hvam, M.L.; Howard, K.A. Albumin-based drug delivery: Harnessing nature to cure disease. Mol. Cell Ther. 2016, 4, 3. [Google Scholar] [CrossRef]
- Latvala, S.; Jacobsen, B.; Otteneder, M.B.; Herrmann, A.; Kronenberg, S. Distribution of FcRn Across Species and Tissues. J. Histochem. Cytochem. 2017, 65, 321–333. [Google Scholar] [CrossRef] [PubMed]
- Lozano, N.A.; Lozano, A.; Marini, V.; Saranz, R.J.; Blumberg, R.S.; Baker, K.; Agresta, M.F.; Ponzio, M.F. Expression of FcRn receptor in placental tissue and its relationship with IgG levels in term and preterm newborns. Am. J. Reprod. Immunol. 2018, 80, e12972. [Google Scholar] [CrossRef]
- Tenten, V.; Menzel, S.; Kunter, U.; Sicking, E.-M.; van Roeyen, C.R.C.; Sanden, S.K.; Kaldenbach, M.; Boor, P.; Fuss, A.; Uhlig, S.; et al. Albumin is recycled from the primary urine by tubular transcytosis. J. Am. Soc. Nephrol. 2013, 24, 1966–1980. [Google Scholar] [CrossRef]
- Pyzik, M.; Rath, T.; Kuo, T.T.; Win, S.; Baker, K.; Hubbard, J.J.; Grenha, R.; Gandhi, A.; Krämer, T.D.; Mezo, A.R.; et al. Hepatic FcRn regulates albumin homeostasis and susceptibility to liver injury. Proc. Natl. Acad. Sci. USA 2017, 114, E2862–E2871. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, M.; Claypool, S.M.; Wagner, J.S.; Mizoguchi, E.; Mizoguchi, A.; Roopenian, D.C.; Lencer, W.; Blumberg, R.S. Human neonatal Fc receptor mediates transport of IgG into luminal secretions for delivery of antigens to mucosal dendritic cells. Immunity 2004, 20, 769–783. [Google Scholar] [CrossRef] [PubMed]
- Kazemi, T.; Younesi, V.; Jadidi-Niaragh, F.; Yousefi, M. Immunotherapeutic approaches for cancer therapy: An updated review. Artif. Cells Nanomed. Biotechnol. 2016, 44, 769–779. [Google Scholar] [CrossRef]
- Toh, W.H.; Louber, J.; Mahmoud, I.S.; Chia, J.; Bass, G.T.; Dower, S.K.; Verhagen, A.M.; Gleeson, P.A. FcRn mediates fast recycling of endocytosed albumin and IgG from early macropinosomes in primary macrophages. J. Cell Sci. 2019, 133, 235416. [Google Scholar] [CrossRef]
- Cadena Castaneda, D.; Brachet, G.; Goupille, C.; Ouldamer, L.; Gouilleux-Gruart, V. The neonatal Fc receptor in cancer FcRn in cancer. Cancer Med. 2020, 9, 4736–4742. [Google Scholar] [CrossRef]
- Dalloneau, E.; Baroukh, N.; Mavridis, K.; Maillet, A.; Gueugnon, F.; Courty, Y.; Petit, A.; Kryza, T.; Del Rio, M.; Guyetant, S.; et al. Downregulation of the neonatal Fc receptor expression in non-small cell lung cancer tissue is associated with a poor prognosis. Oncotarget 2016, 7, 54415–54429. [Google Scholar] [CrossRef]
- Baker, K.; Rath, T.; Flak, M.B.; Arthur, J.C.; Chen, Z.; Glickman, J.N.; Zlobec, I.; Karamitopoulou, E.; Stachler, M.D.; Odze, R.D.; et al. Neonatal Fc receptor expression in dendritic cells mediates protective immunity against colorectal cancer. Immunity 2013, 39, 1095–1107. [Google Scholar] [CrossRef]
- Edge, S.B.; Compton, C.C. The American Joint Committee on Cancer: The 7th edition of the AJCC cancer staging manual and the future of TNM. Ann. Surg. Oncol. 2010, 17, 1471–1474. [Google Scholar] [CrossRef]
- McCluggage, W.G.; Singh, N.; Gilks, C.B. Key changes to the World Health Organization (WHO) classification of female genital tumours introduced in the 5th edition (2020). Histopathology 2022, 80, 762–778. [Google Scholar] [CrossRef] [PubMed]
- Burmeister, W.P.; Gastinel, L.N.; Simister, N.E.; Blum, M.L.; Bjorkman, P.J. Crystal structure at 2.2 A resolution of the MHC-related neonatal Fc receptor. Nature 1994, 372, 336–343. [Google Scholar] [CrossRef] [PubMed]
- Kandil, E.; Egashira, M.; Miyoshi, O.; Niikawa, N.; Ishibashi, T.; Kasahara, M. The human gene encoding the heavy chain of the major histocompatibility complex class I-like Fc receptor (FCGRT) maps to 19q13.3. Cytogenet. Cell Genet. 1996, 73, 97–98. [Google Scholar] [CrossRef] [PubMed]
- Simister, N.E.; Mostov, K.E. An Fc receptor structurally related to MHC class I antigens. Nature 1989, 337, 184–187. [Google Scholar] [CrossRef] [PubMed]
- Fan, Y.Y.; Farrokhi, V.; Caiazzo, T.; Wang, M.; O’Hara, D.M.; Neubert, H. Human FcRn Tissue Expression Profile and Half-Life in PBMCs. Biomolecules 2019, 9, 373. [Google Scholar] [CrossRef]
- Raghavan, M.; Gastinel, L.N.; Bjorkman, P.J. The class I major histocompatibility complex related Fc receptor shows pH-dependent stability differences correlating with immunoglobulin binding and release. Biochemistry 1993, 32, 8654–8660. [Google Scholar] [CrossRef]
- Chaudhury, C.; Mehnaz, S.; Robinson, J.M.; Hayton, W.L.; Pearl, D.K.; Roopenian, D.C.; Anderson, C.L. The major histocompatibility complex-related Fc receptor for IgG (FcRn) binds albumin and prolongs its lifespan. J. Exp. Med. 2003, 197, 315–322. [Google Scholar] [CrossRef]
- Schmidt, E.G.W.; Hvam, M.L.; Antunes, F.; Cameron, J.; Viuff, D.; Andersen, B.; Kristensen, N.N.; Howard, K.A. Direct demonstration of a neonatal Fc receptor (FcRn)-driven endosomal sorting pathway for cellular recycling of albumin. J. Biol. Chem. 2017, 292, 13312–13322. [Google Scholar] [CrossRef]
- Morell, A.; Terry, W.D.; Waldmann, T.A. Metabolic properties of IgG subclasses in man. J. Clin. Investig. 1970, 49, 673–680. [Google Scholar] [CrossRef]
- Rudnik-Jansen, I.; Howard, K.A. FcRn expression in cancer: Mechanistic basis and therapeutic opportunities. J. Control. Release 2021, 337, 248–257. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.H.; Lee, J.H.; Lee, J.S.; Kim, D.C.; Yang, J.W.; An, H.J.; Na, J.M.; Shin, M.C.; Song, D.H. Fc Receptor Expression as a Prognostic Factor in Patients With Non-small-cell Lung Cancer. Vivo 2022, 36, 2708–2713. [Google Scholar] [CrossRef] [PubMed]
- Jansen, M.P.; Foekens, J.A.; van Staveren, I.L.; Dirkzwager-Kiel, M.M.; Ritstier, K.; Look, M.P.; Gelder, M.E.M.-V.; Sieuwerts, A.M.; Portengen, H.; Dorssers, L.C.; et al. Molecular classification of tamoxifen-resistant breast carcinomas by gene expression profiling. J. Clin. Oncol. 2005, 23, 732–740. [Google Scholar] [CrossRef] [PubMed]
- Mahant, A.M.; Trejo, F.E.; Aguilan, J.T.; Sidoli, S.; Permar, S.R.; Herold, B.C. Antibody attributes, Fc receptor expression, gestation and maternal SARS-CoV-2 infection modulate HSV IgG placental transfer. iScience 2023, 26, 107648. [Google Scholar] [CrossRef] [PubMed]
- Sherer, M.L.; Lei, J.; Creisher, P.; Jang, M.; Reddy, R.; Voegtline, K.; Olson, S.; Littlefield, K.; Park, H.S.; Ursin, R.L.; et al. Dysregulated immunity in SARS-CoV-2 infected pregnant women. medRxiv 2020. [Google Scholar] [CrossRef]
- Mandal, G.; Biswas, S.; Anadon, C.M.; Yu, X.; Gatenbee, C.D.; Prabhakaran, S.; Payne, K.K.; Chaurio, R.A.; Martin, A.; Innamarato, P.; et al. IgA-Dominated Humoral Immune Responses Govern Patients’ Outcome in Endometrial Cancer. Cancer Res. 2022, 82, 859–871. [Google Scholar] [CrossRef]
- Moise, K.J., Jr.; Oepkes, D.; Lopriore, E.; Bredius, R.G.M. Targeting neonatal Fc receptor: Potential clinical applications in pregnancy. Ultrasound Obstet. Gynecol. 2022, 60, 167–175. [Google Scholar] [CrossRef]
- Mamat Yusof, M.N.; Chew, K.T.; Kampan, N.C.; Shafiee, M.N. Expression of PD-1 and PD-L1 in Endometrial Cancer: Molecular and Clinical Significance. Int. J. Mol. Sci. 2023, 24, 15233. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Value | |
|---|---|---|
| Age, years (mean [range]) | 51 (35–78) | |
| Menopause, n (%) | No | 20 (48.8%) |
| Yes | 21 (51.2%) | |
| FIGO stage, n (%) | IA | 26 (63.4%) |
| IB | 8 (19.5%) | |
| IIA | 2 (4.9%) | |
| 3A | 2 (4.9%) | |
| 3C | 3 (7.3%) | |
| Tumor grade, n (%) | Low | 38 (92.7%) |
| High | 3 (7.3%) | |
| Tumor size, n (%) | <2 cm | 8 (19.5%) |
| 2≥, <4 cm | 13 (31.7%) | |
| ≥4 cm | 20 (48.8%) | |
| LVSI, n (%) | Absent | 36 (87.8%) |
| Present | 5 (12.2%) | |
| Myometrial invasion, n (%) | <1/2 | 23 (56.1%) |
| ≥1/2 | 18 (43.9%) | |
| FcRn expression, n (%) | Negative | 24 (58.5%) |
| Positive | 17 (41.5%) |
| Variables | FcRn Expression | p Value | |
|---|---|---|---|
| Negative | Positive | ||
| Age, years | 0.105 | ||
| ≤60 | 22 | 12 | |
| >60 | 2 | 5 | |
| FIGO stage | 0.021 | ||
| IA | 19 | 7 | |
| Higher than IA | 5 | 10 | |
| Tumor grade | 0.064 | ||
| Low (G1,G2) | 24 | 14 | |
| High (G3) | 0 | 3 | |
| LVSI | 0.084 | ||
| Absent | 23 | 13 | |
| Present | 1 | 4 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Song, D.H.; Yang, J.; Kim, C.H.; Kim, M.H.; Jo, J.Y.; Baek, J.C. FcRn Expression in Endometrial Cancer and Its Association with Clinicopathologic Features. Diagnostics 2023, 13, 3660. https://doi.org/10.3390/diagnostics13243660
Song DH, Yang J, Kim CH, Kim MH, Jo JY, Baek JC. FcRn Expression in Endometrial Cancer and Its Association with Clinicopathologic Features. Diagnostics. 2023; 13(24):3660. https://doi.org/10.3390/diagnostics13243660
Chicago/Turabian StyleSong, Dae Hyun, Juseok Yang, Cho Hee Kim, Min Hye Kim, Jae Yoon Jo, and Jong Chul Baek. 2023. "FcRn Expression in Endometrial Cancer and Its Association with Clinicopathologic Features" Diagnostics 13, no. 24: 3660. https://doi.org/10.3390/diagnostics13243660
APA StyleSong, D. H., Yang, J., Kim, C. H., Kim, M. H., Jo, J. Y., & Baek, J. C. (2023). FcRn Expression in Endometrial Cancer and Its Association with Clinicopathologic Features. Diagnostics, 13(24), 3660. https://doi.org/10.3390/diagnostics13243660