
Gender Differences and Amputation Risk in Peripheral Artery Disease—A Single-Center Experience

 , , , , ,
, , , , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
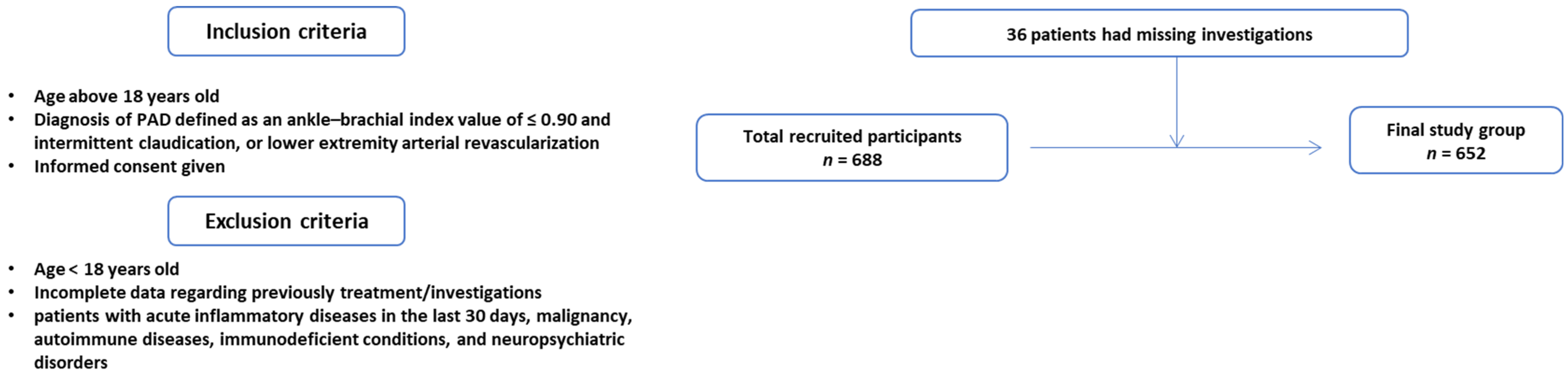
2.1. Study Design
2.2. Measurements
2.2.1. Comorbidities and Laboratory Data
2.2.2. Transthoracic Echocardiography
2.2.3. Angiography
2.3. Risk Scores
2.4. Statistical Analysis
2.5. Ethics
3. Results
- PREVENT III risk score: Of the patients undergoing surgical revascularization, 42 women (87.5%) and 297 men (92.81%) were treated in an intervention via infra-inguinal bypass. The mean value of the score was approximately equal in the two statistically analyzed groups (2.89 ± 0.18 vs. 2.63 ± 0.09, p = 0.882), discretely higher in the patients of the first group taking into account older age and the presence of a higher percentage of coronary artery disease.
- Finnvasc Score: A small percentage of the patients included in the study were treated with an intervention, and of these, 60% of women (3 cases) and 65.11% of men (28 cases) had associated critical injuries requiring emergency treatment. The mean score calculated in this subgroup of patients was higher among men but was not statistically significant (p = 0.788).
- GermanVasc risk score: Analyzing the subgroup of patients with critical injuries, we found approximately equal scores in both subgroups, without statistical significance (13.18 ± 1.59 vs. 12.89 ± 1.44. p = 0.182).
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Criqui, M.H.; Matsushita, K.; Aboyans, V.; Hess, C.N.; Hicks, C.W.; Kwan, T.W.; McDermott, M.M.; Misra, S.; Ujueta, F. Lower Extremity Peripheral Artery Disease: Contemporary Epidemiology, Management Gaps, and Future Directions: A Scientific Statement from the American Heart Association. Circulation 2021, 144, e171–e191. [Google Scholar] [CrossRef]
- Leeper, N.J.; Hamburg, N.M. Peripheral Vascular Disease in 2021. Circ. Res. 2021, 128, 1803–1804. [Google Scholar] [CrossRef]
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990–2019. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef]
- Ankle Brachial Index Collaboration. Ankle Brachial Index Combined with Framingham Risk Score to Predict Cardiovascular Events and Mortality: A Meta-Analysis. JAMA 2008, 300, 197. [Google Scholar] [CrossRef]
- Colantonio, L.D.; Hubbard, D.; Monda, K.L.; Mues, K.E.; Huang, L.; Dai, Y.; Jackson, E.A.; Brown, T.M.; Rosenson, R.S.; Woodward, M.; et al. Atherosclerotic Risk and Statin Use among Patients with Peripheral Artery Disease. J. Am. Coll. Cardiol. 2020, 76, 251–264. [Google Scholar] [CrossRef]
- Kavurma, M.M.; Boccanfuso, L.; Cutmore, C.; Passam, F.; Patel, S.; Hennessy, A.; Loa, J.; Figtree, G.A.; Golledge, J.; Robinson, D.A.; et al. A hidden problem: Peripheral artery disease in women. Eur. Heart J.–Qual. Care Clin. Outcomes 2023, 9, 342–350. [Google Scholar] [CrossRef]
- Collins, T.C.; Suarez-Almazor, M.; Bush, R.L.; Petersen, N.J. Gender and Peripheral Arterial Disease. J. Am. Board Fam. Med. 2006, 19, 132–140. [Google Scholar] [CrossRef][Green Version]
- McDermott, M.M.; Ferrucci, L.; Liu, K.; Guralnik, J.M.; Tian, L.; Kibbe, M.; Liao, Y.; Tao, H.; Criqui, M.H. Women with Peripheral Arterial Disease Experience Faster Functional Decline Than Men with Peripheral Arterial Disease. J. Am. Coll. Cardiol. 2011, 57, 707–714. [Google Scholar] [CrossRef] [PubMed]
- McDermott, M.M.; Greenland, P.; Liu, K.; Criqui, M.H.; Guralnik, J.M.; Celic, L.; Chan, C. Sex Differences in Peripheral Arterial Disease: Leg Symptoms and Physical Functioning. J. Am. Geriatr. Soc. 2003, 51, 222–228. [Google Scholar] [CrossRef] [PubMed]
- Coman, A.E.; Ceasovschih, A.; Petroaie, A.D.; Popa, E.; Lionte, C.; Bologa, C.; Haliga, R.E.; Cosmescu, A.; Slănină, A.M.; Bacușcă, A.I.; et al. The Significance of Low Magnesium Levels in COVID-19 Patients. Medicina 2023, 59, 279. [Google Scholar] [CrossRef] [PubMed]
- Swaminathan, A.; Vemulapalli, S.; Patel, M.; Jones, W.S. Lower extremity amputation in peripheral artery disease: Improving patient outcomes. Vasc Health Risk Manag. 2014, 10, 417–424. [Google Scholar] [CrossRef] [PubMed]
- Arvela, E.; Söderström, M.; Korhonen, M.; Halmesmäki, K.; Albäck, A.; Lepäntalo, M.; Venermo, M.; Biancari, F. Finnvasc Score and Modified Prevent III Score Predict Long-Term Outcome after Infrainguinal Surgical and Endovascular Revascularization for Critical Limb Ischemia. J. Vasc. Surg. 2010, 52, 1218–1225. [Google Scholar] [CrossRef] [PubMed]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the Management of Arterial Hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef] [PubMed]
- Cosentino, F.; Grant, P.J.; Aboyans, V.; Bailey, C.J.; Ceriello, A.; Delgado, V.; Federici, M.; Filippatos, G.; Grobbee, D.E.; Hansen, T.B.; et al. 2019 ESC Guidelines on Diabetes, Pre-Diabetes, and Cardiovascular Diseases Developed in Collaboration with the EASD. Eur. Heart J. 2020, 41, 255–323. [Google Scholar] [CrossRef]
- Aboyans, V.; Ricco, J.-B.; Bartelink, M.-L.E.L.; Björck, M.; Brodmann, M.; Cohnert, T.; Collet, J.-P.; Czerny, M.; De Carlo, M.; Debus, S.; et al. 2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in Collaboration with the European Society for Vascular Surgery (ESVS). Eur. Heart J. 2018, 39, 763–816. [Google Scholar] [CrossRef]
- Wood, D.M. “Pack Year” Smoking Histories: What about Patients Who Use Loose Tobacco? Tob. Control 2005, 14, 141–142. [Google Scholar] [CrossRef]
- Cheung, A.K.; Chang, T.I.; Cushman, W.C.; Furth, S.L.; Hou, F.F.; Ix, J.H.; Knoll, G.A.; Muntner, P.; Pecoits-Filho, R.; Sarnak, M.J.; et al. KDIGO 2021 Clinical Practice Guideline for the Management of Blood Pressure in Chronic Kidney Disease. Kidney Int. 2021, 99, S1–S87. [Google Scholar] [CrossRef]
- Lancellotti, P.; Zamorano, J.L.; Habib, G.; Badano, L. The EACVI Textbook of Echocardiography; Oxford University Press: Oxford, UK, 2016; ISBN 978-0-19-103889-1. [Google Scholar]
- Omeh, D.J.; Shlofmitz, E. Angiography. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Erikson, U. Technique of Coronary Angiography. Acta Radiol. Diagn. 1976, 17, 781–785. [Google Scholar] [CrossRef]
- Wijnand, J.G.J.; Zarkowsky, D.; Wu, B.; van Haelst, S.T.W.; Vonken, E.-J.P.A.; Sorrentino, T.A.; Pallister, Z.; Chung, J.; Mills, J.L.; Teraa, M.; et al. The Global Limb Anatomic Staging System (GLASS) for CLTI: Improving Inter-Observer Agreement. J. Clin. Med. 2021, 10, 3454. [Google Scholar] [CrossRef]
- Cerqueira, L.d.O.; Duarte Júnior, E.G.; Barros, A.L.d.S.; Cerqueira, J.R.; Araújo, W.J.B.d. Classificação WifI: O Novo Sistema de Classificação Da Society for Vascular Surgery Para Membros Inferiores Ameaçados, Uma Revisão de Literatura. J. Vasc. Bras. 2020, 19, e20190070. [Google Scholar] [CrossRef]
- Schanzer, A.; Goodney, P.P.; Li, Y.; Eslami, M.; Cronenwett, J.; Messina, L.; Conte, M.S. Validation of the PIII CLI Risk Score for the Prediction of Amputation-Free Survival in Patients Undergoing Infrainguinal Autogenous Vein Bypass for Critical Limb Ischemia. J. Vasc. Surg. 2009, 50, 769–775. [Google Scholar] [CrossRef] [PubMed]
- Kechagias, A.; Perälä, J.; Ylönen, K.; Asim Mahar, M.A.; Biancari, F. Validation of the Finnvasc Score in Infrainguinal Percutaneous Transluminal Angioplasty for Critical Lower Limb Ischemia. Ann. Vasc. Surg. 2008, 22, 547–551. [Google Scholar] [CrossRef] [PubMed]
- Varu, V.N.; Hogg, M.E.; Kibbe, M.R. Critical Limb Ischemia. J. Vasc. Surg. 2010, 51, 230–241. [Google Scholar] [CrossRef]
- Schwaneberg, T.; Peters, F.; Kuchenbecker, J.; Marschall, U.; Lee, R.; Kriston, L.; Debus, E.; Behrendt, C.-A. The GermanVasc Score: A Pragmatic Risk Score Predicts Five Year Amputation Free Survival in Patients with Peripheral Arterial Occlusive Disease. Eur. J. Vasc. Endovasc. Surg. 2020, 61, 248–256. [Google Scholar] [CrossRef]
- Schramm, K.; Rochon, P.J. Gender Differences in Peripheral Vascular Disease. Semin. Interv. Radiol. 2018, 35, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Yoon, S.H.; Kim, G.Y.; Choi, G.T.; Do, J.T. Organ Abnormalities Caused by Turner Syndrome. Cells 2023, 12, 1365. [Google Scholar] [CrossRef]
- Alsiraj, Y.; Thatcher, S.E.; Blalock, E.; Fleenor, B.; Daugherty, A.; Cassis, L.A. Sex Chromosome Complement Defines Diffuse Versus Focal Angiotensin II–Induced Aortic Pathology. Arterioscler. Thromb. Vasc. Biol. 2018, 38, 143–153. [Google Scholar] [CrossRef]
- Davignon, J.; Ganz, P. Role of Endothelial Dysfunction in Atherosclerosis. Circulation 2004, 109 (Suppl. S1), III-27–III-32. [Google Scholar] [CrossRef]
- Ryczkowska, K.; Adach, W.; Janikowski, K.; Banach, M.; Bielecka-Dabrowa, A. Menopause and Women’s Cardiovascular Health: Is It Really an Obvious Relationship? Arch. Med. Sci. AMS 2022, 19, 458–466. [Google Scholar] [CrossRef]
- Taddei, S.; Virdis, A.; Ghiadoni, L.; Salvetti, G.; Bernini, G.; Magagna, A.; Salvetti, A. Age-Related Reduction of NO Availability and Oxidative Stress in Humans. Hypertension 2001, 38, 274–279. [Google Scholar] [CrossRef]
- Ding, N.; Sang, Y.; Chen, J.; Ballew, S.H.; Kalbaugh, C.A.; Salameh, M.J.; Blaha, M.J.; Allison, M.; Heiss, G.; Selvin, E.; et al. Cigarette Smoking, Smoking Cessation, and Long-Term Risk of 3 Major Atherosclerotic Diseases. J. Am. Coll. Cardiol. 2019, 74, 498–507. [Google Scholar] [CrossRef] [PubMed]
- Huxley, R.R.; Yatsuya, H.; Lutsey, P.L.; Woodward, M.; Alonso, A.; Folsom, A.R. Impact of Age at Smoking Initiation, Dosage, and Time Since Quitting on Cardiovascular Disease in African Americans and Whites: The Atherosclerosis Risk in Communities Study. Am. J. Epidemiol. 2012, 175, 816–826. [Google Scholar] [CrossRef] [PubMed]
- Hiramoto, J.S.; Katz, R.; Weisman, S.; Conte, M. Gender-Specific Risk Factors for Peripheral Artery Disease in a Voluntary Screening Population. J. Am. Heart Assoc. 2014, 3, e000651. [Google Scholar] [CrossRef] [PubMed]
- Tunstall-Pedoe, H.; Peters, S.A.E.; Woodward, M.; Struthers, A.D.; Belch, J.J.F. Twenty-Year Predictors of Peripheral Arterial Disease Compared with Coronary Heart Disease in the Scottish Heart Health Extended Cohort (SHHEC). J. Am. Heart Assoc. 2017, 6, e005967. [Google Scholar] [CrossRef]
- Fowkes, F.G.R.; Rudan, D.; Rudan, I.; Aboyans, V.; Denenberg, J.O.; McDermott, M.M.; Norman, P.E.; Sampson, U.K.A.; Williams, L.J.; Mensah, G.A.; et al. Comparison of Global Estimates of Prevalence and Risk Factors for Peripheral Artery Disease in 2000 and 2010: A Systematic Review and Analysis. Lancet Lond. Engl. 2013, 382, 1329–1340. [Google Scholar] [CrossRef]
- Grigorescu, E.-D.; Sorodoc, V.; Floria, M.; Anisie, E.; Popa, A.D.; Onofriescu, A.; Ceasovschih, A.; Sorodoc, L. The Inflammatory Marker HSCRP as a Predictor of Increased Insulin Resistance in Type 2 Diabetics without Atherosclerotic Manifestations. Rev. Chim. 2019, 70, 1791–1794. [Google Scholar] [CrossRef]
- Grigorescu, E.-D.; Lăcătușu, C.-M.; Floria, M.; Cazac, G.-D.; Onofriescu, A.; Ceasovschih, A.; Crețu, I.; Mihai, B.-M.; Șorodoc, L. Association of Inflammatory and Metabolic Biomarkers with Mitral Annular Calcification in Type 2 Diabetes Patients. J. Pers. Med. 2022, 12, 1484. [Google Scholar] [CrossRef]
- Bavry, A.A.; Anderson, R.D.; Gong, Y.; Denardo, S.J.; Cooper-DeHoff, R.M.; Handberg, E.M.; Pepine, C.J. Outcomes among Hypertensive Patients with Concomitant Peripheral and Coronary Artery Disease. Hypertension 2010, 55, 48–53. [Google Scholar] [CrossRef]
- Kannel, W.B.; McGee, D.L. Update on Some Epidemiologic Features of Intermittent Claudication: The Framingham Study. J. Am. Geriatr. Soc. 1985, 33, 13–18. [Google Scholar] [CrossRef]
- Haine, A.; Kavanagh, S.; Berger, J.S.; Hess, C.N.; Norgren, L.; Fowkes, F.G.R.; Katona, B.G.; Mahaffey, K.W.; Blomster, J.I.; Patel, M.R.; et al. Sex-Specific Risks of Major Cardiovascular and Limb Events in Patients with Symptomatic Peripheral Artery Disease. J. Am. Coll. Cardiol. 2020, 75, 608–617. [Google Scholar] [CrossRef]
- Aday, A.W.; Matsushita, K. Epidemiology of Peripheral Artery Disease and Polyvascular Disease. Circ. Res. 2021, 128, 1818–1832. [Google Scholar] [CrossRef] [PubMed]
- Aday, A.W.; Lawler, P.R.; Cook, N.R.; Ridker, P.M.; Mora, S.; Pradhan, A.D. Lipoprotein Particle Profiles, Standard Lipids, and Peripheral Artery Disease Incidence: Prospective Data from the Women’s Health Study. Circulation 2018, 138, 2330–2341. [Google Scholar] [CrossRef]
- Liang, K.P.; Liang, K.V.; Matteson, E.L.; McClelland, R.L.; Christianson, T.J.H.; Turesson, C. Incidence of Noncardiac Vascular Disease in Rheumatoid Arthritis and Relationship to Extraarticular Disease Manifestations. Arthritis Rheum. 2006, 54, 642–648. [Google Scholar] [CrossRef] [PubMed]
- Wang, G.J.; Shaw, P.A.; Townsend, R.R.; Anderson, A.H.; Xie, D.; Wang, X.; Nessel, L.C.; Mohler, E.R.; Sozio, S.M.; Jaar, B.G.; et al. Sex Differences in the Incidence of Peripheral Artery Disease in the Chronic Renal Insufficiency Cohort. Circ. Cardiovasc. Qual. Outcomes 2016, 9, S86–S93. [Google Scholar] [CrossRef] [PubMed]
- Eraso, L.H.; Fukaya, E.; Mohler, E.R., III; Xie, D.; Sha, D.; Berger, J.S. Peripheral Arterial Disease, Prevalence and Cumulative Risk Factor Profile Analysis. Eur. J. Prev. Cardiol. 2014, 21, 704–711. [Google Scholar] [CrossRef] [PubMed]
- Lionte, C.; Bologa, C.; Sorodoc, V.; Petris, O.R.; Puha, G.; Stoica, A.; Ceasovschih, A.; Jaba, E.; Sorodoc, L. Biomarkers of Inflammation and Inflammation-Related Indexes upon Emergency Department Admission Are Predictive for the Risk of Intensive Care Unit Hospitalization and Mortality in Acute Poisoning: A 6-Year Prospective Observational Study. Dis. Markers 2021, 2021, e4696156. [Google Scholar] [CrossRef]
- Wilson, A.M.; Ryan, M.C.; Boyle, A.J. The Novel Role of C-Reactive Protein in Cardiovascular Disease: Risk Marker or Pathogen. Int. J. Cardiol. 2006, 106, 291–297. [Google Scholar] [CrossRef]
- Pabon, M.; Cheng, S.; Altin, S.E.; Sethi, S.S.; Nelson, M.D.; Moreau, K.L.; Hamburg, N.; Hess, C.N. Sex Differences in Peripheral Artery Disease. Circ. Res. 2022, 130, 496–511. [Google Scholar] [CrossRef]
- Morrell, J.; Zeymer, U.; Baumgartner, I.; Limbourg, T.; Röther, J.; Bhatt, D.L.; Steg, P.G.; the REACH Registry Investigators. Differences in Management and Outcomes between Male and Female Patients with Atherothrombotic Disease: Results from the REACH Registry in Europe. Eur. J. Cardiovasc. Prev. Rehabil. 2011, 18, 270–277. [Google Scholar] [CrossRef]
- Sigvant, B.; Lundin, F.; Wahlberg, E. The Risk of Disease Progression in Peripheral Arterial Disease Is Higher than Expected: A Meta-Analysis of Mortality and Disease Progression in Peripheral Arterial Disease. Eur. J. Vasc. Endovasc. Surg. 2016, 51, 395–403. [Google Scholar] [CrossRef]
- Farber, A.; Eberhardt, R.T. The Current State of Critical Limb Ischemia: A Systematic Review. JAMA Surg. 2016, 151, 1070–1077. [Google Scholar] [CrossRef] [PubMed]
- Mentias, A.; Vaughan-Sarrazin, M.; Saad, M.; Girotra, S. Sex Differences in Management and Outcomes of Critical Limb Ischemia in the Medicare Population. Circ. Cardiovasc. Interv. 2020, 13, e009459. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Total Group (n = 652) | Women (n = 100) | Men (n = 552) | p |
|---|---|---|---|---|
| Demographics | ||||
| Age | 66.46 ± 10.47 | 70.27 ± 10 | 65.79 ± 10.63 | <0.001 # |
| Area of residence (urban) | 273 (41.9%) | 49 (49%) | 224 (40.58%) | 0.124 † |
| Anthropometric data | ||||
| Height, m | 1.92 ± 6.4 | 1.67 ± 0.05 | 1.95 ± 6.75 | 0.325 # |
| Weight, kg | 75.94 ± 9.15 | 78.69 ± 10.64 | 91.38 ± 8.92 | 0.044 # |
| BMI, kg/m2 | 26.21 ± 3.01 | 25.09 ± 3.3 | 27.14 ± 3.05 | 0.049 # |
| Abdominal circumference, cm | 98.85 ± 10.16 | 95.14 ± 8.79 | 103.58 ± 11.05 | 0.031 # |
| Vitals | ||||
| HR, bpm | 74.12 ± 13.96 | 77.07 ± 15.46 | 76.22 ± 13.88 | 0.825 # |
| Systolic BP, mmHg | 141.93 ± 14.89 | 151.30 ± 14.92 | 141.91 ± 14.62 | 0.704 # |
| Diastolic BP, mmHg | 80.15 ± 7.66 | 88.40 ± 7.74 | 80.13 ± 7.56 | 0.750 # |
| Mean BP, mmHg | 100.74 ± 8.93 | 109.70 ± 9.15 | 100.72 ± 8.75 | 0.981 # |
| Pulse pressure, mmHg | 73.56 ± 12.99 | 83.75 ± 15.44 | 74.19 ± 13.62 | 0.772 # |
| Cardiovascular risk factors and comorbidities | ||||
| Smoking | 435 (66.72%) | 35 (35.0%) | 400 (72.46%) | 0.008 |
| Smoking (pack-years) | 23.69 ± 18.43 | 10.69 ± 15.99 | 25.89 ± 19.10 | 0.017 # |
| Dyslipidemia | 350 (53.68%) | 62 (62.0%) | 288 (52.17%) | 0.070 † |
| Diabetes mellitus | 213 (32.67%) | 29 (29.0%) | 184 (33.33%) | 0.630 † |
| Hypercholesterolemia (>200 mg/dL) | 267 (40.95%) | 51 (51.0%) | 216 (36.13%) | 0.026 † |
| Hypercholesterolemia (>250 mg/dL) | 67 (10.28%) | 13 (13.0%) | 54 (9.78%) | 0.330 † |
| HDL-cholesterol < 40 mg/dL | 244 (37.42%) | 16 (16.0%) | 116 (21.01%) | 0.101 † |
| LDL-cholesterol > 130 mg/dL | 276 (42.33%) | 48 (48.0%) | 228 (41.30%) | 0.212 † |
| Hypertriglyceridemia | 35 (5.37%) | 11 (11.0%) | 24 (4.34%) | 0.137 † |
| Overweight | 51 (70.8%) | 24 (24.0%) | 26 (4.71%) | 0.009 * |
| Obesity class I | 18 (25.0%) | 10 (10.0%) | 8 (1.44%) | |
| Obesity class II | 3 (4.2%) | 2 (2.0%) | 1 (0.18%) | |
| Hypertension | 315 (48.31%) | 45 (45.0%) | 270 (48.91%) | 0.696 † |
| Number of risk factors | ||||
| 0 | 16 (2.5%) | 1 (1.0%) | 15 (2.72%) | 0.478 † |
| 1 | 180 (27.6%) | 28 (28.0%) | 152 (27.59%) | |
| 2 | 238 (36.6%) | 40 (40.0%) | 198 (35.93%) | |
| 3 | 156 (24.0%) | 25 (25.0%) | 131 (23.77%) | |
| 4 | 45 (6.9%) | 6 (6.0%) | 39 (7.08%) | |
| 5 | 16 (2.5%) | - | 16 (2.90%) | |
| Cerebrovascular disease | 51 (7.82%) | 11 (11.0%) | 40 (7.24%) | 0.005 † |
| Coronary artery disease | 294 (45.09%) | 38 (38.0%) | 256 (46.37%) | 0.033 † |
| Chronic kidney disease | 70 (10.73%) | 21 (21.0%) | 49 (8.87%) | 0.046 † |
| Rutherford classification | ||||
| Class 3 | 106 (16.3%) | 22 (22.0%) | 84 (15.25%) | |
| Class 4 | 213 (32.7%) | 24 (24.0%) | 188 (34.12%) | |
| Class 5 | 205 (31.4%) | 32 (32.0%) | 173 (31.40%) | |
| Class 6 | 128 (19.6%) | 22 (22.0%) | 82 (14.86%) | |
| Biological data | ||||
| Total cholesterol. mg/dL | 198.47 ± 46.57 | 207.69 ± 46.70 | 193.14 ± 45.74 | 0.004 # |
| LDL-cholesterol. mg/dL | 126.82 ± 40.30 | 142.44 ± 40.80 | 125.74 ± 40.03 | 0.018 # |
| HDL-cholesterol. mg/dL | 41.65 ± 10.60 | 44.74 ± 13.05 | 40.87 ± 9.87 | 0.001 # |
| Triglycerides. mg/dL | 135.45 ±71.79 | 152.57 ± 78.23 | 132.61 ± 70.29 | 0.019 # |
| Serum creatinine. mg/dL | 0.96 ± 0.36 | 1.09 ± 0.44 | 1.05 ± 0.35 | 0.369 # |
| Serum urea. mg/dL | 44.71 ± 18.92 | 46.53 ± 21.77 | 44.43 ± 18.88 | 0.320 # |
| Creatinine clearance. mL/min/1.73 m2 | 62.49 ± 22.01 | 61.71 ± 24.25 | 62.56 ± 21.51 | 0.721 # |
| Fasting glucose. mg/dL | 118.49 ± 48.90 | 117.90 ± 49.66 | 119.36 ± 49.22 | 0.787 # |
| Serum fibrinogen. mg/dL | 395.59 ± 132.22 | 393.21 ± 131.01 | 436.89 ± 133.11 | 0.049 # |
| hs-CRP. mg/dL | 6.34 ± 2.78 | 7.99 ± 2.91 | 5.03 ± 1.86 | 0.041 # |
| Hematocrit. % | 41.74 ± 5.16 | 40.95 ± 6.65 | 41.82 ± 5 | 0.132 # |
| Platelets (×103/mL) | 297.44 ± 11.17 | 309.09 ± 99.95 | 296 ± 112.49 | 0.240 # |
| Clinical parameters | ||||
| Pain at rest | 541 (81.44%) | 77 (77.0%) | 464 (84.06%) | 0.190 † |
| Erythema | 77 (11.81%) | 12 (12.0%) | 487 (88.22%) | 0.949 † |
| Ulcerations | 93 (14.26%) | 16 (16.0%) | 77 (13.95%) | 0.589 † |
| Necrosis | 27 (4.14%) | 5 (5.0%) | 22 (3.99%) | 0.845 † |
| Gangrene | 121 (18.51%) | 17 (17.0%) | 103 (18.66%) | 0.780 † |
| Bilateral clinical involvement | 231 (35.43%) | 33 (33.0%) | 198 (35.87%) | 0.552 † |
| Cardiac murmurs | 119 (18.25%) | 27 (27.0%) | 92 (16.67%) | 0.042 † |
| Femoral artery murmur | 149 (22.85%) | 25 (25.0%) | 124 (22.46%) | 0.786 † |
| Carotid artery murmur | 77 (11.81%) | 20 (20.0%) | 57 (10.33%) | 0.021 † |
| Renal artery murmur | 24 (3.68%) | 8 (8.0%) | 16 (2.90%) | 0.041 † |
| Ankle brachial index | 0.81 ± 0.08 | 0.73 ± 0.11 | 0.82 ± 0.15 | 0.053 † |
| Paraclinical data | ||||
| Arterial Doppler US | 110 (16.95%) | 21 (21.0%) | 89 (16.12%) | |
| Angio MRI | 32 (4.9%) | 4 (4.0%) | 28 (5.07%) | |
| Arteriography | 635 (97.4%) | 98 (98.0%) | 536 (97.10%) | |
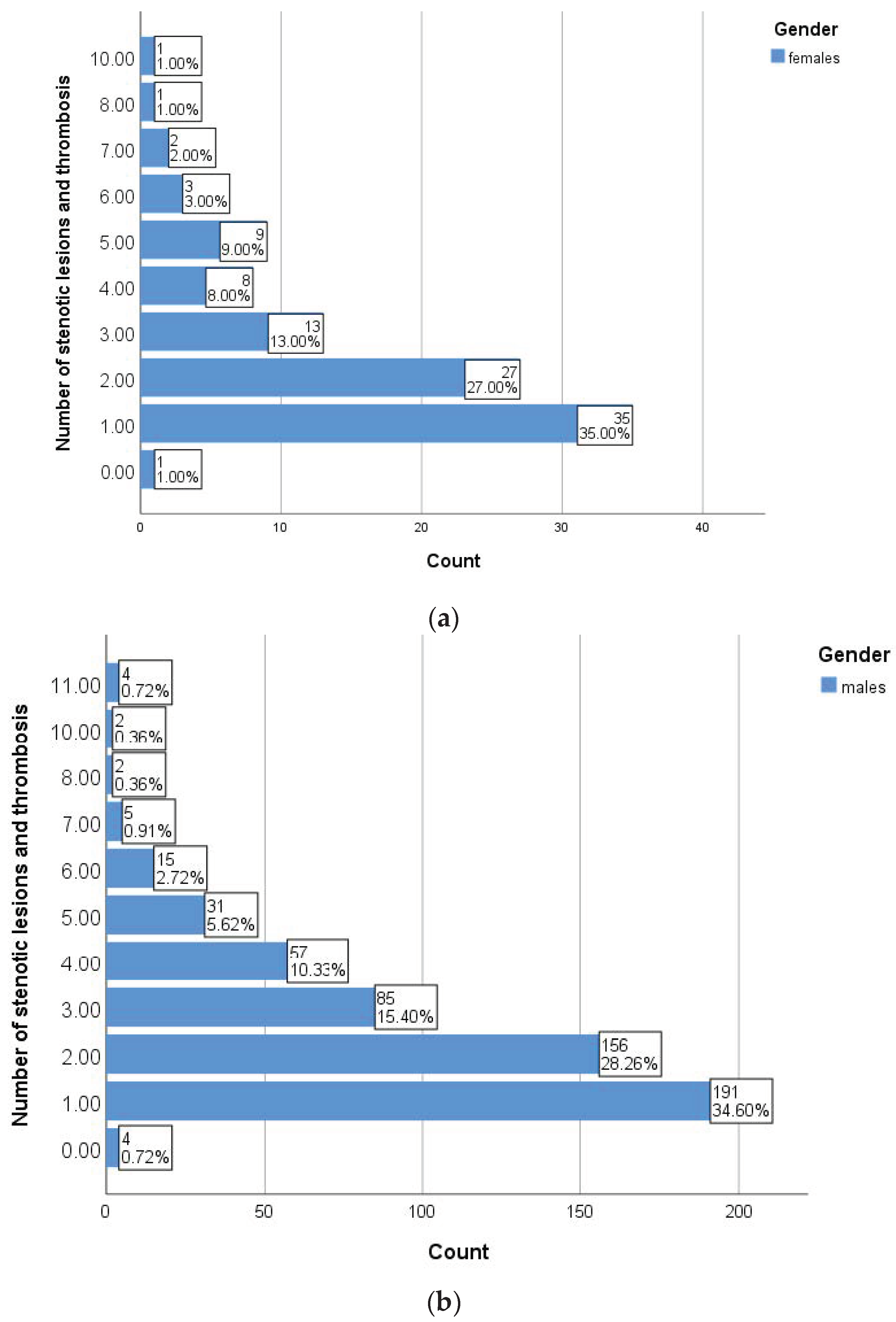
| Number of lesions (stenosis and thrombosis) | 0.037 † | |||
| 0 | 5 (0.8%) | 1 (1.0%) | 4 (0.72%) | |
| 1 | 226 (34.7%) | 35 (35.0%) | 191 (34.60%) | |
| 2 | 183 (28.1%) | 27 (27.0%) | 156 (28.26%) | |
| 3 | 98 (15.0%) | 13 (13.0%) | 85 (15.40%) | |
| 4 | 65 (10.0%) | 8 (8.0%) | 57 (10.33%) | |
| 5 | 40 (6.1%) | 9 (9.0%) | 31 (5.62%) | |
| ≥6 | 35 (4.6%) | 7 (7.0%) | 28 (5.07%) | |
| LVEF, % | 57.36 ± 10.08 | 57.30 ± 10.48 | 57.26 ± 10.05 | 0.973 # |
| Therapeutic management | ||||
| Medical | 650 (99.8%) | 99 (99.0%) | 551 (99.82%) | 0.129 † |
| Interventional revascularization | 48 (7.36%) | 5 (5.0%) | 43 (7.79%) | 0.326 † |
| Surgical revascularization | 369 (56.6%) | 48 (48.0%) | 320 (57.97%) | 0.149 † |
| Risk of amputation | 210 (32.1%) | 33 (33.0%) | 177 (32.07%) | 0.854 † |
| Women | Men | |||||||
|---|---|---|---|---|---|---|---|---|
| Number of Stenotic Lesions and Thromboses | ABI | Number of Stenotic Lesions and Thromboses | ABI | |||||
| r | p * | r | p * | r | p | r | p * | |
| Age | −0.061 | 0.546 | −0.059 | 0.566 | −0.058 | 0.117 | 0.049 | 0.258 |
| Smoking (packs/year) | 0.651 | 0.005 | −0.400 | <0.001 | 0.599 | 0.008 | 0.418 | 0.042 |
| Total cholesterol | 0.048 | 0.638 | 0.046 | 0.656 | 0.072 | 0.092 | 0.009 | 0.828 |
| HDL-cholesterol | 0.136 | 0.176 | −0.058 | 0.570 | −0.11 | 0.791 | 0.060 | 0.167 |
| LDL-cholesterol | 0.042 | 0.677 | 0.039 | 0.705 | 0.050 | 0.244 | −0.007 | 0.880 |
| Triglycerides | −0.082 | 0.420 | 0.083 | 0.417 | 0.100 | 0.019 | 0.007 | 0.870 |
| Systolic BP | −0.004 | 0.967 | 0.002 | 0.981 | 0.031 | 0.461 | 0.018 | 0.686 |
| Uric acid | 0.351 | <0.001 | 0.097 | 0.345 | 0.019 | 0.650 | −0.066 | 0.130 |
| hs-CRP | 0.408 | 0.018 | 0.511 | 0.009 | 0.703 | 0.025 | 0.560 | 0.019 |
| Serum fibrinogen | 0.478 | 0.029 | 0.478 | 0.017 | 0.551 | 0.037 | 0.603 | 0.039 |
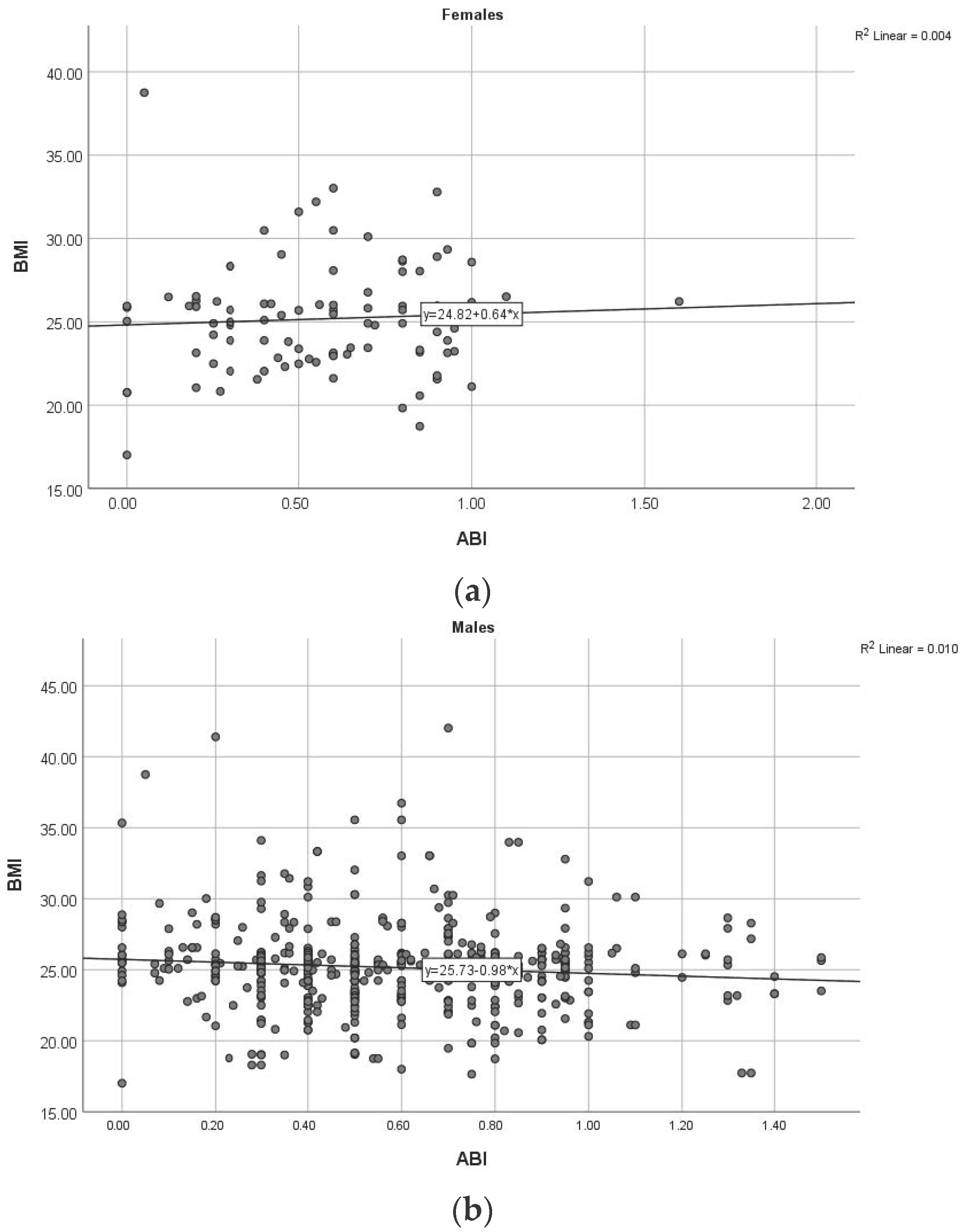
| BMI | 0.010 | 0.923 | 0.060 | 0.562 | −0.065 | 0.129 | −0.098 | 0.025 |
| More than 3 CVD risk factors | 0.047 | 0.644 | −0.087 | 0.398 | −0.146 | 0.001 | 0.056 | 0.200 |
| Area Under the Curve | |||||
|---|---|---|---|---|---|
| Test Result Variable(s) | Area | Std. Error | Asymptotic Sig. | Asymptotic 95% Confidence Interval | |
| Lower Bound | Upper Bound | ||||
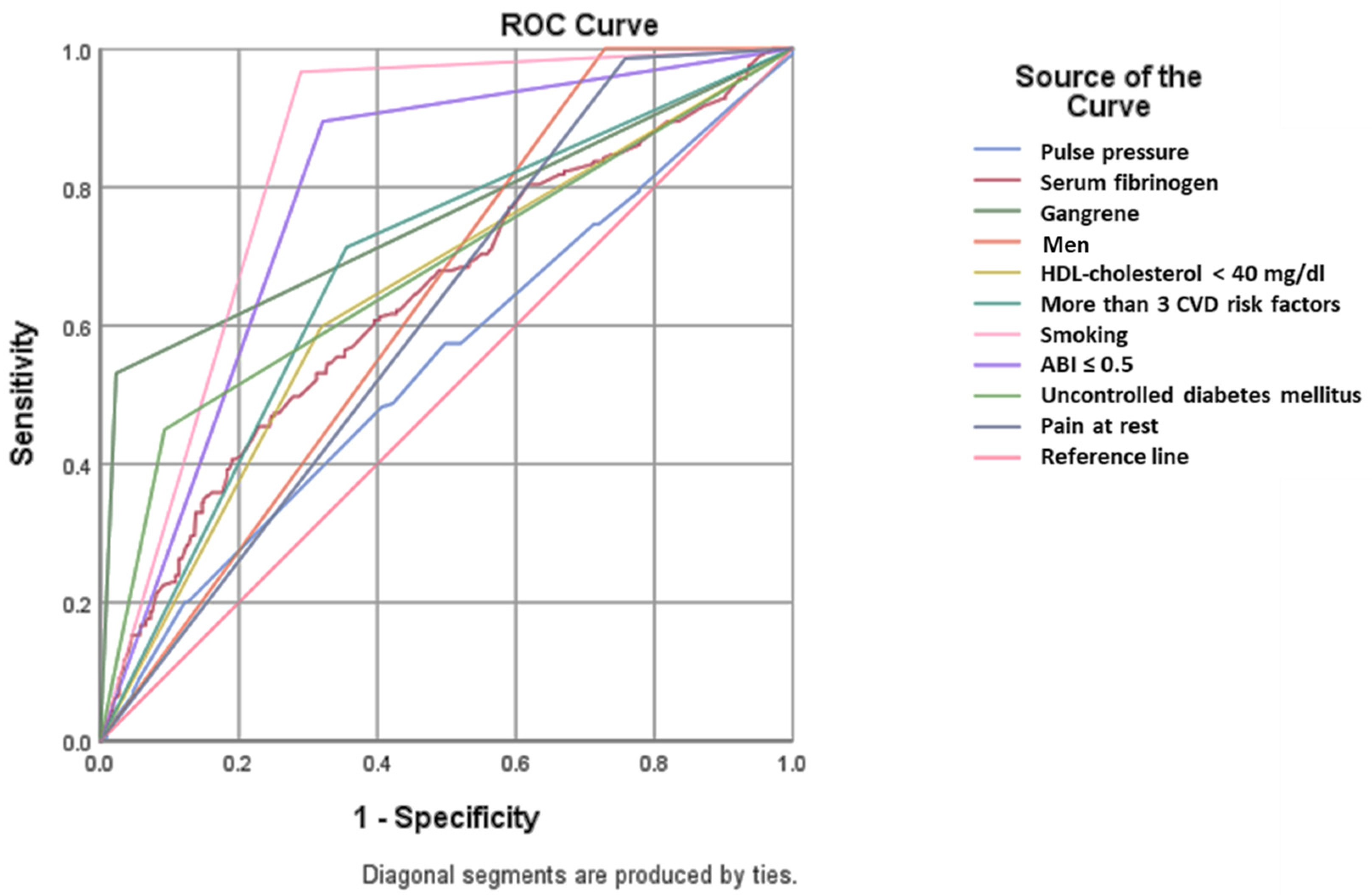
| Pulse pressure | 0.545 | 0.025 | 0.062 | 0.497 | 0.594 |
| Serum fibrinogen | 0.639 | 0.024 | <0.001 | 0.592 | 0.685 |
| Gangrene | 0.754 | 0.023 | <0.001 | 0.709 | 0.799 |
| Men | 0.636 | 0.021 | <0.001 | 0.594 | 0.678 |
| HDL-cholesterol < 40 mg/dL | 0.640 | 0.023 | <0.001 | 0.593 | 0.686 |
| More than 3 CVD risk factors | 0.679 | 0.022 | <0.001 | 0.635 | 0.723 |
| Smoking | 0.838 | 0.016 | <0.001 | 0.808 | 0.869 |
| ABI ≤ 0.5 | 0.787 | 0.019 | <0.001 | 0.750 | 0.823 |
| Uncontrolled diabetes mellitus | 0.679 | 0.024 | <0.001 | 0.631 | 0.726 |
| Pain at rest | 0.614 | 0.022 | <0.001 | 0.571 | 0.657 |
| Parameter | Univariate Regression | Multivariate Regression | ||||
|---|---|---|---|---|---|---|
| β | p | Odds Ratio (95% CI) | β | p | Odds Ratio (95% CI) | |
| Serum fibrinogen | 0.004 | <0.001 | 1.004 (1.003–1.005) | −0.003 | 0.045 | 0.997 (0.969–1.024) |
| Gangrene | 3.880 | <0.001 | 8.436 (1.466–25.892) | 3.752 | <0.001 | 8.206 (2.687–17.105) |
| Men | 3.009 | <0.001 | 6.559 (3.761–9.367) | 2.789 | <0.001 | 6.313 (3.115–8.006) |
| HDL-cholesterol less than 40 mg/dL | 1.164 | <0.001 | 3.202 (2.277–4.503) | 1.393 | <0.001 | 2.948 (1.194–4.882) |
| More than 3 CVD risk factors | 1.489 | <0.001 | 4.434 (3.106–6.330) | 2.364 | <0.001 | 4.138 (3.040–7.225) |
| Smoking | 4.265 | <0.001 | 11.141 (5.579–15.345) | 4.679 | <0.001 | 10.660 (5.874–27.956) |
| ABI ≤ 0.5 | 2.893 | <0.001 | 18.054 (11.119–29.313) | 3.666 | <0.001 | 16.282 (9.182–30.821) |
| Uncontrolled diabetes mellitus | 2.089 | <0.001 | 4.080 (5.304–12.307) | 1.342 | 0.161 | 3.826 (0.586–25.004) |
| Pain at rest | 3.093 | <0.001 | 12.039 (2.906–17.327) | 3.489 | 0.006 | 12.168 (2.711–16.085) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Onofrei, V.; Adam, C.A.; Marcu, D.T.M.; Leon, M.-M.; Cumpăt, C.; Mitu, F.; Cojocaru, D.-C. Gender Differences and Amputation Risk in Peripheral Artery Disease—A Single-Center Experience. Diagnostics 2023, 13, 3145. https://doi.org/10.3390/diagnostics13193145
Onofrei V, Adam CA, Marcu DTM, Leon M-M, Cumpăt C, Mitu F, Cojocaru D-C. Gender Differences and Amputation Risk in Peripheral Artery Disease—A Single-Center Experience. Diagnostics. 2023; 13(19):3145. https://doi.org/10.3390/diagnostics13193145
Chicago/Turabian StyleOnofrei, Viviana, Cristina Andreea Adam, Dragos Traian Marius Marcu, Maria-Magdalena Leon, Carmen Cumpăt, Florin Mitu, and Doina-Clementina Cojocaru. 2023. "Gender Differences and Amputation Risk in Peripheral Artery Disease—A Single-Center Experience" Diagnostics 13, no. 19: 3145. https://doi.org/10.3390/diagnostics13193145
APA StyleOnofrei, V., Adam, C. A., Marcu, D. T. M., Leon, M.-M., Cumpăt, C., Mitu, F., & Cojocaru, D.-C. (2023). Gender Differences and Amputation Risk in Peripheral Artery Disease—A Single-Center Experience. Diagnostics, 13(19), 3145. https://doi.org/10.3390/diagnostics13193145