
Diagnostic Role of Native T1 Mapping Compared to Conventional Magnetic Resonance Techniques in Cardiac Disease in a Real-Life Cohort

 , , ,
, , ,  ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. CMR Protocol
2.2. CMR Post-Processing
2.3. Statistical Analysis
3. Results
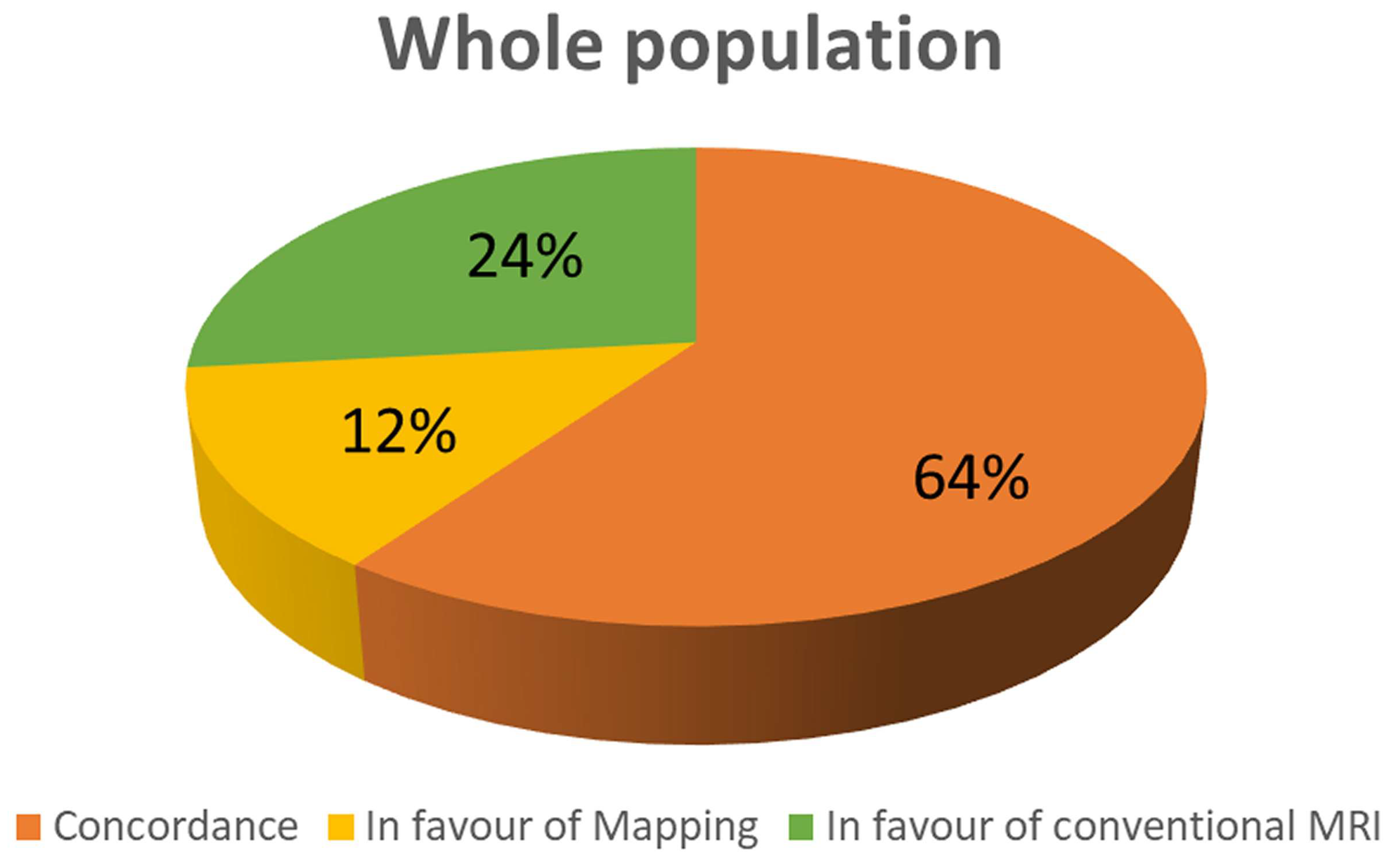
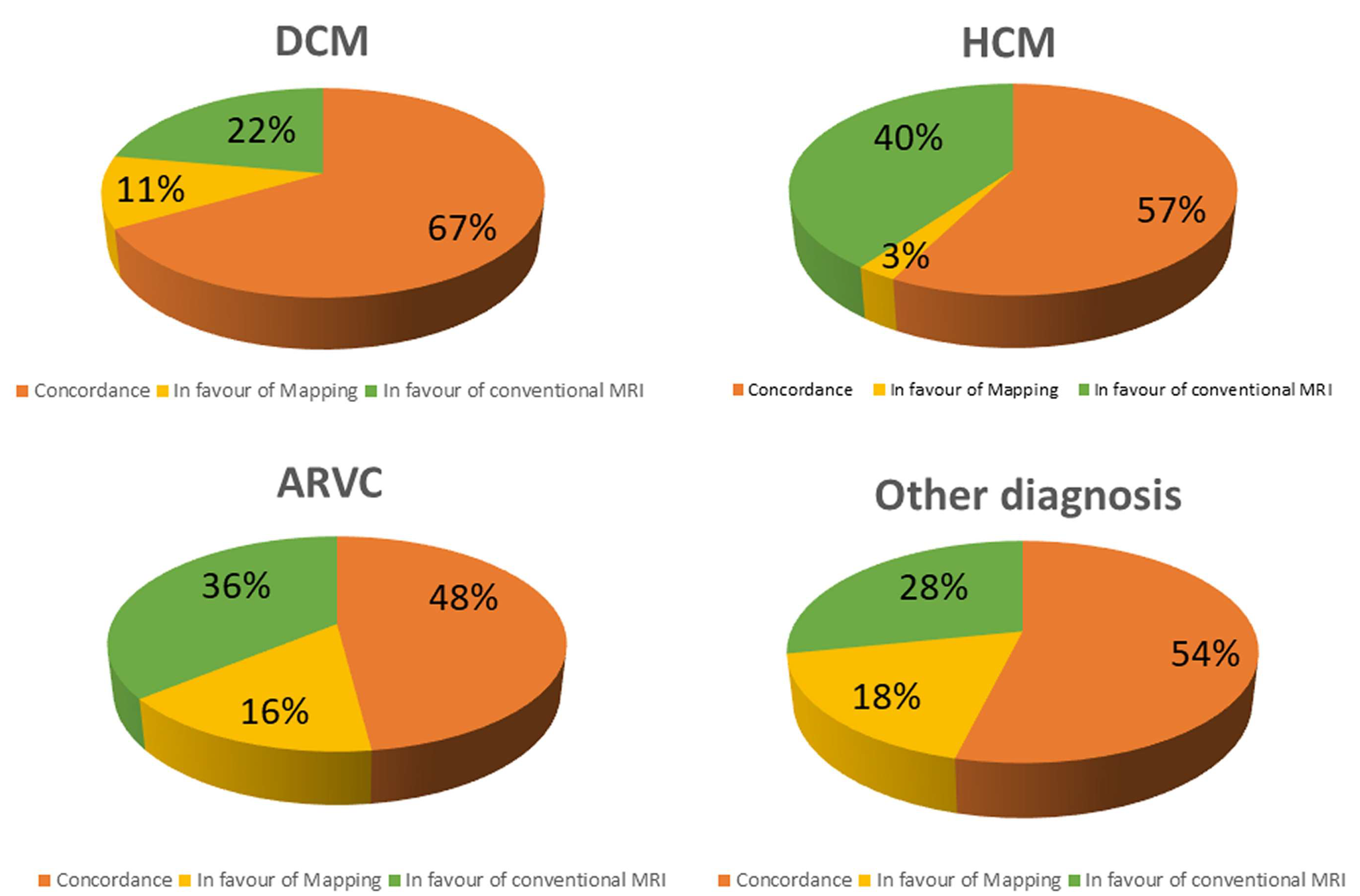
3.1. Conventional CMR vs. T1 Mapping
3.2. Diagnostic Role of T1 Mapping
3.3. Diffuse vs. Regional Myocardial Damage
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Haaf, P.; Garg, P.; Messroghli, D.R.; Broadbent, D.A.; Greenwood, J.P.; Plein, S. Cardiac T1 Mapping and Extracellular Volume (ECV) in clinical practice: A comprehensive review. J. Cardiovasc. Magn. Reson. 2017, 18, 89. [Google Scholar] [CrossRef] [PubMed]
- Aquaro, G.D.; De Gori, C.; Faggioni, L.; Parisella, M.L.; Cioni, D.; Lencioni, R.; Neri, E. Diagnostic and prognostic role of late gadolinium enhancement in cardiomyopathies. Eur. Heart J. Suppl. 2023, 25 (Suppl. C), C130–C136. [Google Scholar] [CrossRef] [PubMed]
- Taylor, A.J.; Salerno, M.; Dharmakumar, R.; Jerosch-Herold, M. T1 Mapping: Basic Techniques and Clinical Applications. JACC Cardiovasc. Imaging 2016, 9, 67–81. [Google Scholar] [CrossRef]
- Burt, J.R.; Zimmerman, S.L.; Kamel, I.R.; Halushka, M.; Bluemke, D.A. Myocardial T1 mapping: Techniques and potential applications. Radiographics 2014, 34, 377–395. [Google Scholar] [CrossRef] [PubMed]
- Kellman, P.; Hansen, M.S. T1-mapping in the heart: Accuracy and precision. J. Cardiovasc. Magn. Reson. 2014, 16, 2. [Google Scholar] [CrossRef]
- Radenkovic, D.; Weingärtner, S.; Ricketts, L.; Moon, J.C.; Captur, G. T1 mapping in cardiac MRI. Heart Fail. Rev. 2017, 22, 415–430. [Google Scholar] [CrossRef]
- Barison, A.; Del Torto, A.; Chiappino, S.; Aquaro, G.D.; Todiere, G.; Vergaro, G.; Passino, C.; Lombardi, M.; Emdin, M.; Masci, P.G. Prognostic significance of myocardial extracellular volume fraction in nonischaemic dilated cardiomyopathy. J. Cardiovasc. Med. (Hagerstown) 2015, 16, 681–687. [Google Scholar] [CrossRef]
- Messroghli, D.R.; Moon, J.C.; Ferreira, V.M.; Grosse-Wortmann, L.; He, T.; Kellman, P.; Mascherbauer, J.; Nezafat, R.; Salerno, M.; Schelbert, E.B.; et al. Clinical recommendations for cardiovascular magnetic resonance mapping of T1, T2, T2* and extracellular volume: A consensus statement by the Society for Cardiovascular Magnetic Resonance (SCMR) endorsed by the European Association for Cardiovascular Imaging (EACVI). J. Cardiovasc. Magn. Reson. 2017, 19, 75. [Google Scholar] [CrossRef]
- Ferreira, V.M.; Piechnik, S.K.; Dall’Armellina, E.; Karamitsos, T.D.; Francis, J.M.; Ntusi, N.; Holloway, C.; Choudhury, R.P.; Kardos, A.; Robson, M.D.; et al. T(1) mapping for the diagnosis of acute myocarditis using CMR: Comparison to T2-weighted and late gadolinium enhanced imaging. JACC Cardiovasc. Imaging 2013, 6, 1048–1058. [Google Scholar] [CrossRef]
- Garg, P.; Saunders, L.C.; Swift, A.J.; Wild, J.M.; Plein, S. Role of cardiac T1 mapping and extracellular volume in the assessment of myocardial infarction. Anatol. J. Cardiol. 2018, 19, 404–411. [Google Scholar] [CrossRef]
- Xu, J.; Zhuang, B.; Sirajuddin, A.; Li, S.; Huang, J.; Yin, G.; Song, L.; Jiang, Y.; Zhao, S.; Lu, M. MRI T1 Mapping in Hypertrophic Cardiomyopathy: Evaluation in Patients Without Late Gadolinium Enhancement and Hemodynamic Obstruction. Radiology 2020, 294, 275–286. [Google Scholar] [CrossRef] [PubMed]
- Quarta, G.; Aquaro, G.D.; Pedrotti, P.; Pontone, G.; Dellegrottaglie, S.; Iacovoni, A.; Brambilla, P.; Pradella, S.; Todiere, G.; Rigo, F.; et al. Cardiovascular magnetic resonance imaging in hypertrophic cardiomyopathy: The importance of clinical context. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 601–610. [Google Scholar] [CrossRef]
- Todiere, G.; Pisciella, L.; Barison, A.; Del Franco, A.; Zachara, E.; Piaggi, P.; Re, F.; Pingitore, A.; Emdin, M.; Lombardi, M.; et al. Abnormal T2-STIR magnetic resonance in hypertrophic cardiomyopathy: A marker of advanced disease and electrical myocardial instability. PLoS ONE 2014, 9, e111366. [Google Scholar] [CrossRef]
- Aquaro, G.D.; Masci, P.; Formisano, F.; Barison, A.; Strata, E.; Pingitore, A.; Positano, V.; Spirito, P.; Lombardi, M. Usefulness of delayed enhancement by magnetic resonance imaging in hypertrophic cardiomyopathy as a marker of disease and its severity. Am. J. Cardiol. 2010, 105, 392–397. [Google Scholar] [CrossRef] [PubMed]
- Florian, A.; Masci, P.G.; De Buck, S.; Aquaro, G.D.; Claus, P.; Todiere, G.; Van Cleemput, J.; Lombardi, M.; Bogaert, J. Geometric assessment of asymmetric septal hypertrophic cardiomyopathy by CMR. JACC Cardiovasc. Imaging 2012, 5, 702–711. [Google Scholar] [CrossRef] [PubMed]
- Karamitsos, T.D.; Piechnik, S.K.; Banypersad, S.M.; Fontana, M.; Ntusi, N.B.; Ferreira, V.M.; Whelan, C.J.; Myerson, S.G.; Robson, M.D.; Hawkins, P.N.; et al. Noncontrast T1 mapping for the diagnosis of cardiac amyloidosis. JACC Cardiovasc. Imaging 2013, 6, 488–497. [Google Scholar] [CrossRef] [PubMed]
- Aquaro, G.D.; Pugliese, N.R.; Perfetto, F.; Cappelli, F.; Barison, A.; Masci, P.G.; Passino, C.; Emdin, M. Myocardial signal intensity decay after gadolinium injection: A fast and effective method for the diagnosis of cardiac amyloidosis. Int. J. Cardiovasc. Imaging 2014, 30, 1105–1115. [Google Scholar] [CrossRef]
- Roller, F.C.; Fuest, S.; Meyer, M.; Harth, S.; Gündüz, D.; Bauer, P.; Schneider, C.; Rolfs, A.; Krombach, G.A.; Tanislav, C. Assessment of Cardiac Involvement in Fabry Disease (FD) with Native T1 Mapping. Rofo 2019, 191, 932–939. [Google Scholar] [CrossRef]
- Aquaro, G.D.; De Gori, C.; Faggioni, L.; Parisella, M.L.; Aringhieri, G.; Cioni, D.; Lencioni, R.; Neri, E. Cardiac Magnetic Resonance in Fabry Disease: Morphological, Functional, and Tissue Features. Diagnostics 2022, 12, 2652. [Google Scholar] [CrossRef]
- Pica, S.; Sado, D.M.; Maestrini, V.; Fontana, M.; White, S.K.; Treibel, T.; Captur, G.; Anderson, S.; Piechnik, S.K.; Robson, M.D.; et al. Reproducibility of native myocardial T1 mapping in the assessment of Fabry disease and its role in early detection of cardiac involvement by cardiovascular magnetic resonance. J. Cardiovasc. Magn. Reson. 2014, 16, 99. [Google Scholar] [CrossRef]
- Aus dem Siepen, F.; Buss, S.J.; Messroghli, D.; Andre, F.; Lossnitzer, D.; Seitz, S.; Keller, M.; Schnabel, P.A.; Giannitsis, E.; Korosoglou, G.; et al. T1 mapping in dilated cardiomyopathy with cardiac magnetic resonance: Quantification of diffuse myocardial fibrosis and comparison with endomyocardial biopsy. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 210–216. [Google Scholar] [CrossRef] [PubMed]
- Minegishi, S.; Kato, S.; Takase-Minegishi, K.; Horita, N.; Azushima, K.; Wakui, H.; Ishigami, T.; Kosuge, M.; Kimura, K.; Tamura, K. Native T1 time and extracellular volume fraction in differentiation of normal myocardium from non-ischemic dilated and hypertrophic cardiomyopathy myocardium: A systematic review and meta-analysis. Int. J. Cardiol. Heart Vasc. 2019, 25, 100422. [Google Scholar] [CrossRef] [PubMed]
- Chaosuwannakit, N.; Makarawate, P. Value of cardiac magnetic resonance imaging in systemic sclerosis. Reumatologia. 2018, 56, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, V.M.; Schulz-Menger, J.; Holmvang, G.; Kramer, C.M.; Carbone, I.; Sechtem, U.; Kindermann, I.; Gutberlet, M.; Cooper, L.T.; Liu, P.; et al. Cardiovascular Magnetic Resonance in Nonischemic Myocardial Inflammation: Expert Recommendations. J. Am. Coll. Cardiol. 2018, 72, 3158–3176. [Google Scholar] [CrossRef] [PubMed]
- Meloni, A.; Martini, N.; Positano, V.; D’Angelo, G.; Barison, A.; Todiere, G.; Grigoratos, C.; Barra, V.; Pistoia, L.; Gargani, L.; et al. Myocardial T1 Values at 1.5 T: Normal Values for General Electric Scanners and Sex-Related Differences. J. Magn. Reson. Imaging 2021, 54, 1486–1500. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Indication | Morphologic Features (Cine-SSFP) | Edema/Fat | LGE | Native T1 |
|---|---|---|---|---|
| DCM | LV dilation and dysfunction | Non-specific pattern |
| Slight diffuse increase |
| HCM |
| Mid-wall edema in hypertrophied segments associated with LGE (40%) | Mid-wall distribution in hypertrophied segments (55–95%) | Focal increase on T1 only in scar region (55–95%) |
| ARC |
| Fat infiltration/metaplasia |
|
|
| Myocarditis |
| Non-ischemic pattern (85–100%) | Non-ischemic pattern (85–100%) | Increased |
| MINOCA |
| Ischemic-like pattern (100% in acute phase) | Ischemic presentation with potential no-reflow (hypointensity within hyperintense regions) (100%) |
|
| Tako-tsubo | Regional wall motion abnormalities in apical segments (apical ballooning) | Transmural in apical regions (100% in acute phase) | Absent | Increased in apical regions |
| Clinical Indication | Morphologic Features (Cine SSFP) | Edema | LGE | Native T1 |
|---|---|---|---|---|
| Scleroderma | Non-specific | Diffuse/focal edema in active inflammation (possible) |
| Diffuse/focal increase |
| Amyloidosis |
| Non-specific pattern | Specific pattern:
| Diffuse increase |
| Myocardial infarction |
|
| Ischemic presentation
|
|
| Fabry disease |
| Non-specific pattern |
|
|
| Dystrophy |
| Non-specific pattern | Non-ischemic pattern (10–20%) |
|
| Pericarditis |
| Hyperintensity of pericardial layers in pericarditis (80%) |
| Unknown |
| Indication | n | Males | Age | LV EF | LV EDVi | RV EF | RV EDVi |
|---|---|---|---|---|---|---|---|
| DCM | 61 (18.9) | 47 (77) | 59 ± 14 | 43.15 ± 14.58 | 112.56 ± 35.31 | 56.16 ± 11.54 | 78.21 ± 21.39 |
| HCM | 51 (15.8) | 35 (69) | 60 ± 13 | 67.43 ± 11.31 | 73.80 ± 21.64 | 65.29 ± 7.94 | 69.59 ± 21.74 |
| ARC | 63 (19.5) | 43 (68) | 40 ± 17 | 65.08 ± 7.64 | 87.79 ± 16.22 | 60.74 ± 7.38 | 91.79 ± 19.85 |
| Myocarditis | 44 (13.6) | 29 (66) | 50 ± 20 | 61.34 ± 9.04 | 77.86 ± 18.39 | 61.61 ± 5.93 | 76.09 ± 17.55 |
| Scleroderma | 21 (6.5) | 2 (10) | 56 ± 15 | 61.29 ± 16.71 | 76.81 ± 16.97 | 62.38 ± 7.51 | 75.19 ± 16.48 |
| Amyloidosis | 17 (5.3) | 9 (53) | 76 ± 8 | 63.06 ± 14.25 | 70.94 ± 20.64 | 66.76 ± 9.48 | 59.94 ± 12.43 |
| Myocardial infarction (acute/chronic) | 15 (4.6) | 11 (73) | 62 ± 15 | 49.73 ± 16.42 | 89.60 ± 27.13 | 63.80 ± 8.17 | 61.47 ± 14.73 |
| Dystrophy/mitochondrial | 8 (2.8) | 7 (85) | 41 ± 17 | 62.00 ± 9.51 | 70.67 ± 20.56 | 62.78 ± 9.68 | 65.44 ± 15.62 |
| Pericarditis–pericardial effusion | 6 (1.9) | 2 (33) | 46 ± 13 | 66.50 ± 10.21 | 80.50 ± 15.14 | 66.67 ± 6.95 | 71.83 ± 13.06 |
| LV non-compaction | 4 (1.2) | 2 (50) | 39 ± 21 | 65.50 ± 10.63 | 83.25 ± 11.21 | 58.75 ± 7.41 | 87.75 ± 16.32 |
| Systemic sarcoidosis | 3 (0.9) | 1 (33) | 56 ± 9 | 46.67 ± 21.01 | 74.00 ± 3.61 | 38.00 ± 22.61 | 97.00 ± 32.51 |
| Fabry | 1 (0.3) | 1 (100) | 45 | 65 | 70 | 63 | 72 |
| Pulmonary hypertension | 1 (0.3) | 1 (100) | 58 | 57 | 83 | 49 | 81 |
| Valvular disease | 1 (0.3) | 1 (100) | 77 | 58 | 88 | 70 | 78 |
| Healthy controls | 27 (8.4) | 16 (59) | 51 ± 18 | 67.15 ± 6.73 | 78.44 ± 18.25 | 63.59 ± 7.00 | 78.07 ± 19.48 |
| Indication | T2-STIR+ | LGE+ | T1 Regional Abnormality | Mean T1 |
|---|---|---|---|---|
| DCM | 1 (1.6) | 44 (73.3) | 37 (60.7%) | 1050 ± 44 |
| HCM | 2 (3.9) | 37 (74) | 19 (37.3%) | 1029 ± 48 |
| ARVC | 2 (3.2) | 31 (50.8) | 19 (30.2%) | 1012 ± 54 |
| Myocarditis | 27 (61.4) | 33 (75.0) | 25 (56.8%) | 1053 ± 65 |
| Scleroderma | 4 (19.0) | 10 (50.0) | 18 (85.7%) | 1092 ± 41 |
| Amyloidosis | 0 | 12 (70.6) | 11 (64.7%) | 1063 ± 78 |
| Myocardial infarction (acute/chronic) | 3 (20.0) | 15 (100) | 11 (73.3%) | 1063 ± 87 |
| Dystrophy/mitochondrial disease | 0 (0.0) | 6 (66.7) | 6 (66.7%) | 1058 ± 65 |
| Pericarditis–pericardial effusion | 1 (16.7) | 1 (16.7) | 3 (50.0%) | 1105 ± 102 |
| LV non-compaction | 0 (0.0) | 4 (100) | 2 (50.0%) | 1059 ± 76 |
| Systemic sarcoidosis | 1 (33.3) | 2 (66.7) | 2 (66.7%) | 1049 ± 33 |
| Fabry | 0 | 1 (100) | 1 (100) | 827 |
| Pulmonary hypertension | 0 | 1 (100) | 0 (0.0%) | 1026 |
| Valvular disease | 0 | 1 (100) | 0 (0.0%) | 1018 |
| Healthy controls | 0 (0.0) | 0 (0.0 | 0(0.0%) | 1034 ± 29 |
| Initial Suspicion | Specific Findings N (%) | Alternative Diagnosis N (%) | Non-Specific Findings N (%) | Negative CMR N (%) |
|---|---|---|---|---|
| DCM | 34 (55.7) | 7 (11.5) | 17 (27.9) | 3 (4.9) |
| HCM | 33 (64.7) | 2 (3.9) | 16 (31,4) | 0 |
| ARVC | 12 (19.0) | 11 (17.5) | 22 (34.9) | 18 (28.6) |
| Myocarditis | 22 (50) | 14 (31.8) | 6 (13.6) | 2 (4.6) |
| Scleroderma | 17 (80.9) | 0 | 3 (14.3) | 1 (4.8) |
| Amyloidosis | 5 (29.4) | 4 (23.5) | 6 (35.3) | 2 (11.8) |
| Myocardial infarction (acute/chronic) | 10 (66.7) | 1 (6.6) | 4 (26.7) | 0 |
| Dystrophy/mitochondrial disease | 8 (88.9) | 0 | 0 | 1 (11.1) |
| Pericarditis–pericardial effusion | 4 (66.6) | 1 (16.7) | 1 (16,7) | 0 |
| LV non-compaction | 1 (25) | 1 (25) | 2 (50) | 0 |
| Systemic sarcoidosis | 1 (33.3) | 0 | 1 (33.3) | 1 (33.3) |
| Fabry | 1(100) | 0 | 0 | 0 |
| Pulmonary hypertension | 1 (100) | 0 | 0 | 0 |
| Valvular disease | 1 (100) | 0 | 0 | 0 |
| Total | 149 (50.3) | 41 (13.8) | 78 (26.4) | 28 (9.5) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aquaro, G.D.; Monastero, S.; Todiere, G.; Barison, A.; De Gori, C.; Grigoratos, C.; Parisella, M.L.; Faggioni, L.; Cioni, D.; Lencioni, R.; et al. Diagnostic Role of Native T1 Mapping Compared to Conventional Magnetic Resonance Techniques in Cardiac Disease in a Real-Life Cohort. Diagnostics 2023, 13, 2461. https://doi.org/10.3390/diagnostics13142461
Aquaro GD, Monastero S, Todiere G, Barison A, De Gori C, Grigoratos C, Parisella ML, Faggioni L, Cioni D, Lencioni R, et al. Diagnostic Role of Native T1 Mapping Compared to Conventional Magnetic Resonance Techniques in Cardiac Disease in a Real-Life Cohort. Diagnostics. 2023; 13(14):2461. https://doi.org/10.3390/diagnostics13142461
Chicago/Turabian StyleAquaro, Giovanni Donato, Silvia Monastero, Giancarlo Todiere, Andrea Barison, Carmelo De Gori, Crysanthos Grigoratos, Maria Luisa Parisella, Lorenzo Faggioni, Dania Cioni, Riccardo Lencioni, and et al. 2023. "Diagnostic Role of Native T1 Mapping Compared to Conventional Magnetic Resonance Techniques in Cardiac Disease in a Real-Life Cohort" Diagnostics 13, no. 14: 2461. https://doi.org/10.3390/diagnostics13142461
APA StyleAquaro, G. D., Monastero, S., Todiere, G., Barison, A., De Gori, C., Grigoratos, C., Parisella, M. L., Faggioni, L., Cioni, D., Lencioni, R., & Neri, E. (2023). Diagnostic Role of Native T1 Mapping Compared to Conventional Magnetic Resonance Techniques in Cardiac Disease in a Real-Life Cohort. Diagnostics, 13(14), 2461. https://doi.org/10.3390/diagnostics13142461