
Comparative Evaluation of Breast Ductal Carcinoma Grading: A Deep-Learning Model and General Pathologists’ Assessment Approach

 , , , , ,
, , , , , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Dataset
2.2. Nottingham Grading by Pathologists
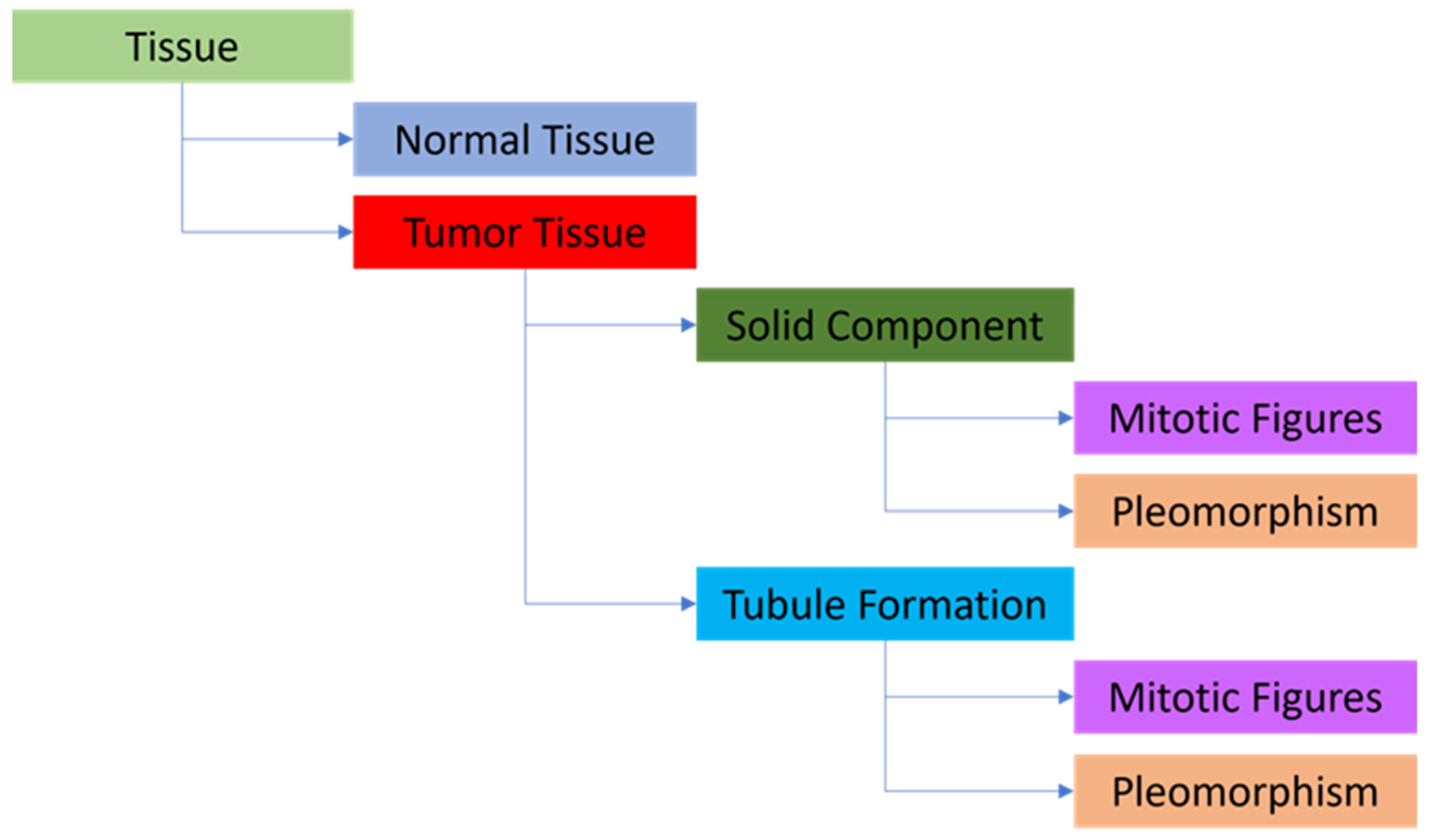
2.3. Machine Learning Approach
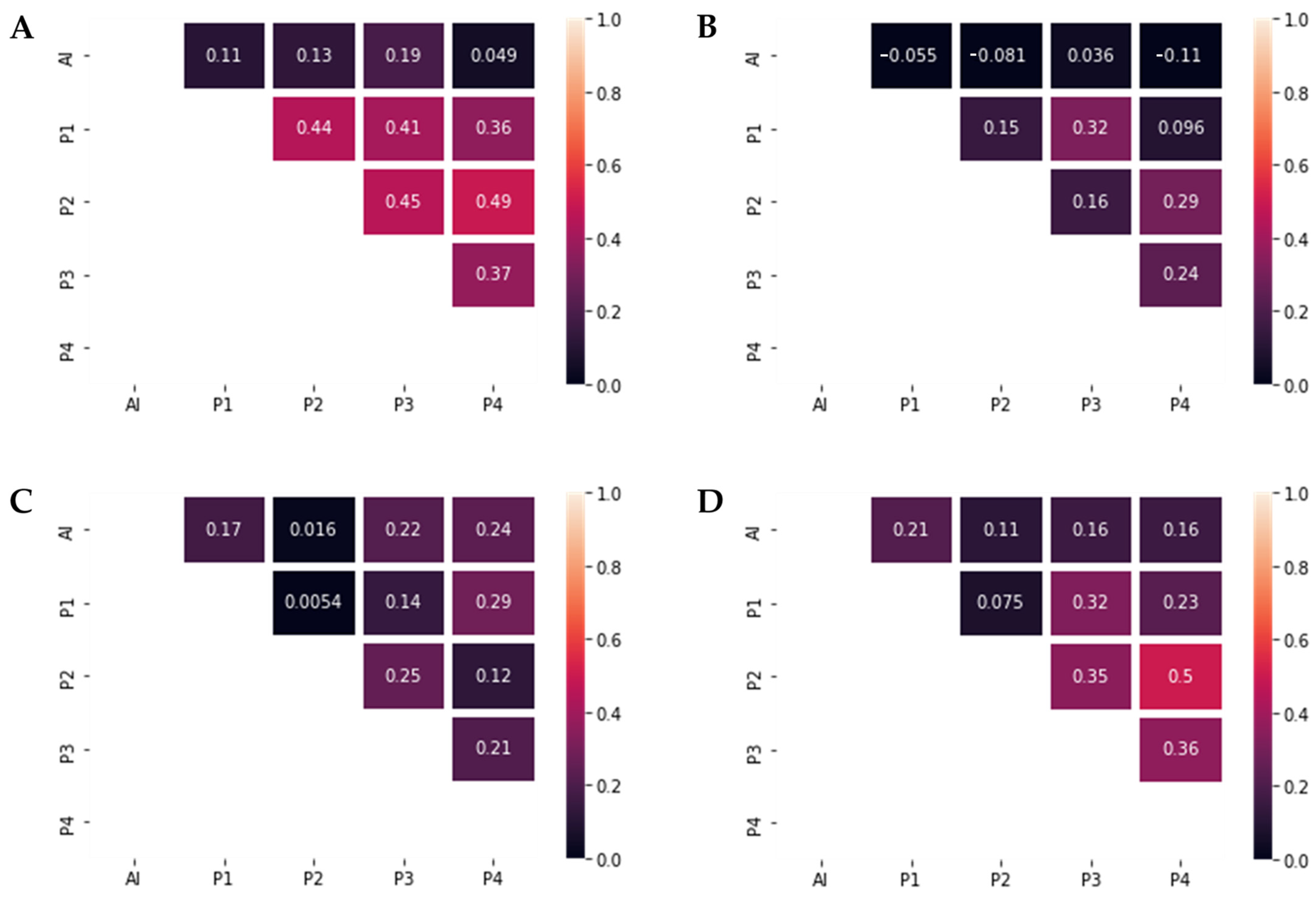
2.4. Statistical Analysis
3. Results
3.1. Pathological Description of the Data Set Used for HA and AI Evaluation
3.2. Pathological Description of the Data Set Used for AI Model/Deep Learning-Based Model Training
3.3. Performance and Comparison of the HA and DL
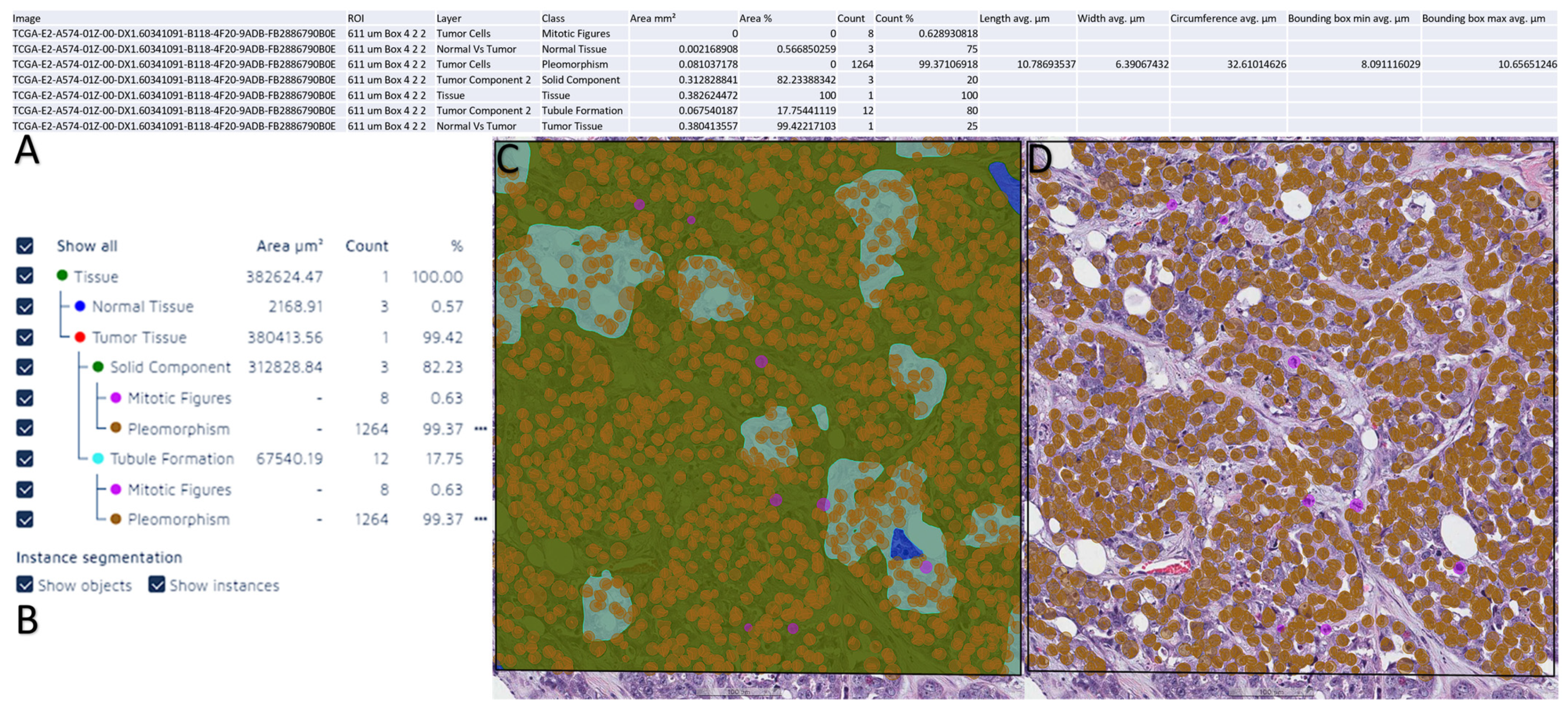
3.4. Performance of the DL Model
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Harbeck, N.; Penault-Llorca, F.; Cortes, J.; Gnant, M.; Houssami, N.; Poortmans, P.; Ruddy, K.; Tsang, J.; Cardoso, F. Breast cancer. Nat. Rev. Dis. Primers 2019, 5, 66. [Google Scholar] [CrossRef] [PubMed]
- Rakha, E.A.; El-Sayed, M.E.; Lee, A.H.S.; Elston, C.W.; Grainge, M.J.; Hodi, Z.; Blamey, R.W.; Ellis, I.O. Prognostic Significance of Nottingham Histologic Grade in Invasive Breast Carcinoma. J. Clin. Oncol. 2008, 26, 3153–3158. [Google Scholar] [CrossRef]
- Couture, H.D.; Williams, L.A.; Geradts, J.; Nyante, S.J.; Butler, E.N.; Marron, J.S.; Perou, C.M.; Troester, M.A.; Niethammer, M. Image analysis with deep learning to predict breast cancer grade, ER status, histologic subtype, and intrinsic subtype. npj Breast Cancer 2018, 4, 30. [Google Scholar] [CrossRef] [PubMed]
- Elston, C.; Ellis, I. pathological prognostic factors in breast cancer. I. The value of histological grade in breast cancer: Experience from a large study with long-term follow-up. Histopathology 1991, 19, 403–410. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, H.; Oshi, M.; Asaoka, M.; Yan, L.; Endo, I.; Takabe, K. Molecular Biological Features of Nottingham Histological Grade 3 Breast Cancers. Ann. Surg. Oncol. 2020, 27, 4475–4485. [Google Scholar] [CrossRef]
- Bera, K.; Schalper, K.A.; Rimm, D.L.; Velcheti, V.; Madabhushi, A. Artificial intelligence in digital pathology—New tools for diagnosis and precision oncology. Nat. Rev. Clin. Oncol. 2019, 16, 703–715. [Google Scholar] [CrossRef]
- Komura, D.; Ishikawa, S. Machine learning approaches for pathologic diagnosis. Virchows Arch. 2019, 475, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Wetstein, S.C.; Stathonikos, N.; Pluim, J.P.W.; Heng, Y.J.; ter Hoeve, N.D.; Vreuls, C.P.H.; van Diest, P.J.; Veta, M. Deep learning-based grading of ductal carcinoma in situ in breast histopathology images. Lab. Investig. 2021, 101, 525–533. [Google Scholar] [CrossRef]
- Rabe, K.; Snir, O.L.; Bossuyt, V.; Harigopal, M.; Celli, R.; Reisenbichler, E.S. Interobserver variability in breast carcinoma grading results in prognostic stage differences. Hum. Pathol. 2019, 94, 51–57. [Google Scholar] [CrossRef]
- Melo, R.C.N.; Raas, M.W.D.; Palazzi, C.; Neves, V.H.; Malta, K.K.; Silva, T.P. Whole Slide Imaging and Its Applications to Histopathological Studies of Liver Disorders. Front. Med. 2020, 6, 310. [Google Scholar] [CrossRef]
- Cui, M.; Zhang, D.Y. Artificial intelligence and computational pathology. Lab. Investig. 2021, 101, 412–422. [Google Scholar] [CrossRef] [PubMed]
- Ginter, P.S.; Idress, R.; D’Alfonso, T.M.; Fineberg, S.; Jaffer, S.; Sattar, A.K.; Chagpar, A.; Wilson, P.; Harigopal, M. Histologic grading of breast carcinoma: A multi-institution study of interobserver variation using virtual microscopy. Mod. Pathol. 2021, 34, 701–709. [Google Scholar] [CrossRef] [PubMed]
- Mantrala, S.; Ginter, P.S.; Mitkari, A.; Joshi, S.; Prabhala, H.; Ramachandra, V.; Kini, L.; Idress, M.R.; D’Alfonso, T.M.; Fineberg, S.; et al. Concordance in Breast Cancer Grading by Artificial Intelligence on Whole Slide Images Compares With a Multi-Institutional Cohort of Breast Pathologists. Arch. Pathol. Lab. Med. 2022, 146, 1369–1377. [Google Scholar] [CrossRef]
- Kumar, Y.; Gupta, S.; Singla, R.; Hu, Y.-C. A Systematic Review of Artificial Intelligence Techniques in Cancer Prediction and Diagnosis. Arch. Comput. Methods Eng. 2021, 29, 2043–2070. [Google Scholar] [CrossRef]
- Kiani, A.; Uyumazturk, B.; Rajpurkar, P.; Wang, A.; Gao, R.; Jones, E.; Yu, Y.; Langlotz, C.P.; Ball, R.L.; Montine, T.J.; et al. Impact of a deep learning assistant on the histopathologic classification of liver cancer. npj Digit. Med. 2020, 3, 23. [Google Scholar] [CrossRef] [PubMed]
- Balkenhol, M.C.A.; Tellez, D.; Vreuls, W.; Clahsen, P.C.; Pinckaers, H.; Ciompi, F.; Bult, P.; van der Laak, J.A.W.M. Deep learning assisted mitotic counting for breast cancer. Lab. Investig. 2019, 99, 1596–1606. [Google Scholar] [CrossRef]
- Jaroensri, R.; Wulczyn, E.; Hegde, N.; Brown, T.; Flament-Auvigne, I.; Tan, F.; Cai, Y.; Nagpal, K.; Rakha, E.A.; Dabbs, D.J.; et al. Deep learning models for histologic grading of breast cancer and association with disease prognosis. npj Breast Cancer 2022, 8, 113. [Google Scholar] [CrossRef] [PubMed]
- Elsharawy, K.A.; Gerds, T.A.; Rakha, E.A.; Dalton, L.W. Artificial intelligence grading of breast cancer: A promising method to refine prognostic classification for management precision. Histopathology 2021, 79, 187–199. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Cruz-Roa, A.; Basavanhally, A.; Gilmore, H.; Shih, N.; Feldman, M.; Tomaszewski, J.; Gonzalez, F.; Madabhushi, A. Mitosis detection in breast cancer pathology images by combining handcrafted and convolutional neural network features. J. Med. Imaging 2014, 1, 034003. [Google Scholar] [CrossRef]
- Mahmood, T.; Arsalan, M.; Owais, M.; Lee, M.B.; Park, K.R. Artificial Intelligence-Based Mitosis Detection in Breast Cancer Histopathology Images Using Faster R-CNN and Deep CNNs. J. Clin. Med. 2020, 9, 749. [Google Scholar] [CrossRef]
- Bankhead, P.; Loughrey, M.B.; Fernández, J.A.; Dombrowski, Y.; McArt, D.G.; Dunne, P.D.; McQuaid, S.; Gray, R.T.; Murray, L.J.; Coleman, H.G.; et al. QuPath: Open source software for digital pathology image analysis. Sci. Rep. 2017, 7, 16878. [Google Scholar] [CrossRef]
- Rakha, E.A.; Sasano, H.; Wu, Y. WHO Classification of Tumors Editorial Board: Breast Tumors; WHO Classification of Tumors Series; IARC Publications: Lyon, France, 2019. [Google Scholar]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- van Dooijeweert, C.; van Diest, P.J.; Ellis, I.O. Grading of invasive breast carcinoma: The way forward. Virchows Arch. 2022, 480, 33–43. [Google Scholar] [CrossRef] [PubMed]
- Van Dooijeweert, C.; Van Diest, P.J.; Willems, S.M.; Kuijpers, C.C.H.J.; Van Der Wall, E.; Overbeek, L.I.H.; Deckers, I.A.G. Significant inter- and intra-laboratory variation in grading of invasive breast cancer: A nationwide study of 33,043 patients in the Netherlands. Int. J. Cancer 2020, 146, 769–780. [Google Scholar] [CrossRef]
- Davidson, T.M.; Rendi, M.H.; Frederick, P.D.; Onega, T.; Allison, K.H.; Mercan, E.; Brunyé, T.T.; Shapiro, L.G.; Weaver, D.L.; Elmore, J.G. Breast Cancer Prognostic Factors in the Digital Era: Comparison of Nottingham Grade using Whole Slide Images and Glass Slides. J. Pathol. Inform. 2019, 10, 11. [Google Scholar] [CrossRef]
- Longacre, T.A.; Ennis, M.; Quenneville, L.A.; Bane, A.L.; Bleiweiss, I.J.; Carter, B.A.; Catelano, E.; Hendrickson, M.R.; Hibshoosh, H.; Layfield, L.J.; et al. Interobserver agreement and reproducibility in classification of invasive breast carcinoma: An NCI breast cancer family registry study. Mod. Pathol. 2006, 19, 195–207. [Google Scholar] [CrossRef]
- Wang, Y.; Acs, B.; Robertson, S.; Liu, B.; Solorzano, L.; Wählby, C.; Hartman, J.; Rantalainen, M. Improved breast cancer histological grading using deep learning. Ann. Oncol. 2022, 33, 89–98. [Google Scholar] [CrossRef]
- Yousif, M.; van Diest, P.J.; Laurinavicius, A.; Rimm, D.; van der Laak, J.; Madabhushi, A.; Schnitt, S.; Pantanowitz, L. Artificial intelligence applied to breast pathology. Virchows Arch. 2022, 480, 191–209. [Google Scholar] [CrossRef] [PubMed]
- Dunne, B.; Going, J.J. Scoring nuclear pleomorphism in breast cancer. Histopathology 2001, 39, 259–265. [Google Scholar] [CrossRef] [PubMed]
- Delides, G.S.; Garas, G.; Georgouli, G.; Jiortziotis, D.; Lecca, J.; Liva, T.; Elemenoglou, J. Intralaboratory variations in the grading of breast carcinoma. Arch. Pathol. Lab. Med. 1982, 106, 126–128. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Grade | 1 (N = 10) | 2 (N = 25) | 3 (N = 47) |
|---|---|---|---|
| Tumor Stage | |||
| I | 1 (10%) | 4 (17%) | 4 (8.9%) |
| IA | 1 (10%) | 1 (4.2%) | 3 (6.7%) |
| IIA | 0 (0%) | 0 (0%) | 2 (4.4%) |
| IIB | 2 (20%) | 8 (33%) | 8 (18%) |
| IIIA | 1 (10%) | 3 (12%) | 4 (8.9%) |
| IIIB | 0 (0%) | 0 (0%) | 2 (4.4%) |
| IIIC | 0 (0%) | 0 (0%) | 5 (11%) |
| Grade | 1 (N = 10) | 2 (N = 25) | 3 (N = 47) |
|---|---|---|---|
| Tubule formation | |||
| 1 | 2 (20%) | 0 (0%) | 0 (0%) |
| 2 | 8 (80%) | 15 (65%) | 1 (2.3%) |
| 3 | 0 (0%) | 8 (35%) | 42 (98%) |
| Nuclear pleomorphism | |||
| 1 | 0 (0%) | 1 (4.3%) | 0 (0%) |
| 2 | 10 (100%) | 13 (57%) | 7 (16%) |
| 3 | 0 (0%) | 9 (39%) | 36 (84%) |
| Mitotic activity | |||
| 1 | 9 (90%) | 12 (52%) | 0 (0%) |
| 2 | 1 (10%) | 7 (30%) | 10 (23%) |
| 3 | 0 (0%) | 4 (17%) | 33 (77%) |
| Case ID | Tumor Stage | Tubule Formation | Nuclear Pleomorphism | Mitotic Activity | Nottingham Grade |
|---|---|---|---|---|---|
| TCGA-D8-A1JU | IA | 2 | 2 | 1 | 1 |
| TCGA-D8-A1XW | IIA | 3 | 3 | 2 | 3 |
| TCGA-BH-A0B7 | IIB | 2 | 3 | 3 | 3 |
| TCGA-D8-A27L | IIIA | 2 | 2 | 1 | 1 |
| TCGA-D8-A1X9 | IIB | 2 | 2 | 3 | 2 |
| TCGA-BH-A0H3 | I | 1 | 2 | 1 | 1 |
| TCGA-EW-A2FS | IIB | 3 | 3 | 3 | 3 |
| All Values in Percentages | Total Area Error | False-Positive | False-Negative | Precision | Sensitivity | F1 Score | Training Loss Value |
|---|---|---|---|---|---|---|---|
| Tissue | 0.46 | 0.13 | 0.33 | 99.85 | 99.63 | 99.74 | 0.0085 |
| Normal Tissue | 2.02 | 0.47 | 2.40 | 99.53 | 97.50 | 98.55 | |
| Tumor Tissue | 0.54 | 0.97 | 1.68 | 99.02 | 98.32 | 98.67 | |
| Solid Component | 5.06 | 0.97 | 6.73 | 98.97 | 93.27 | 96.04 | |
| Tubule Formation | 2.37 | 5.03 | 5.51 | 94.95 | 94.49 | 94.73 | |
| Mitotic Figures | 4.07 | 2.77 | 1.29 | 97.27 | 98.71 | 97.98 | |
| Pleomorphism | 3.51 | 1.50 | 2.00 | 98.49 | 98.00 | 98.24 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Köteles, M.M.; Vigdorovits, A.; Kumar, D.; Mihai, I.-M.; Jurescu, A.; Gheju, A.; Bucur, A.; Harich, O.O.; Olteanu, G.-E. Comparative Evaluation of Breast Ductal Carcinoma Grading: A Deep-Learning Model and General Pathologists’ Assessment Approach. Diagnostics 2023, 13, 2326. https://doi.org/10.3390/diagnostics13142326
Köteles MM, Vigdorovits A, Kumar D, Mihai I-M, Jurescu A, Gheju A, Bucur A, Harich OO, Olteanu G-E. Comparative Evaluation of Breast Ductal Carcinoma Grading: A Deep-Learning Model and General Pathologists’ Assessment Approach. Diagnostics. 2023; 13(14):2326. https://doi.org/10.3390/diagnostics13142326
Chicago/Turabian StyleKöteles, Maria Magdalena, Alon Vigdorovits, Darshan Kumar, Ioana-Maria Mihai, Aura Jurescu, Adelina Gheju, Adeline Bucur, Octavia Oana Harich, and Gheorghe-Emilian Olteanu. 2023. "Comparative Evaluation of Breast Ductal Carcinoma Grading: A Deep-Learning Model and General Pathologists’ Assessment Approach" Diagnostics 13, no. 14: 2326. https://doi.org/10.3390/diagnostics13142326
APA StyleKöteles, M. M., Vigdorovits, A., Kumar, D., Mihai, I.-M., Jurescu, A., Gheju, A., Bucur, A., Harich, O. O., & Olteanu, G.-E. (2023). Comparative Evaluation of Breast Ductal Carcinoma Grading: A Deep-Learning Model and General Pathologists’ Assessment Approach. Diagnostics, 13(14), 2326. https://doi.org/10.3390/diagnostics13142326