


Concentrations of Serum Brain Injury Biomarkers Following SARS-CoV-2 Infection in Individuals with and without Long-COVID—Results from the Prospective Population-Based COVI-GAPP Study

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Blood Sample Collection
2.3. SARS-CoV-2 Antibody Measurement
2.4. Serum GFAP and Serum NFL Measurements
2.5. Questionnaires
2.6. Statistical Analysis
3. Results
3.1. Demographics
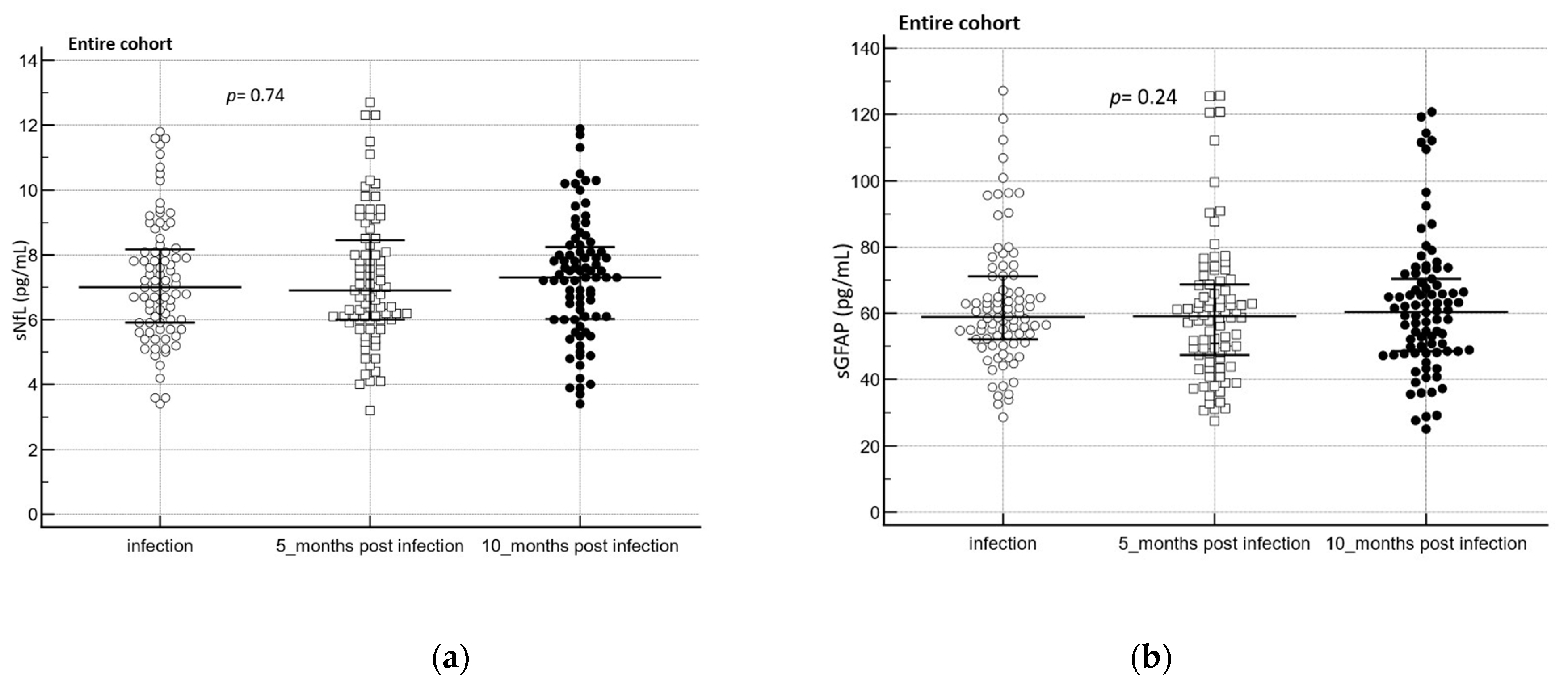
3.2. Biomarkers of Brain Injury after a Mild-to-Moderate SARS-CoV-2 Infection
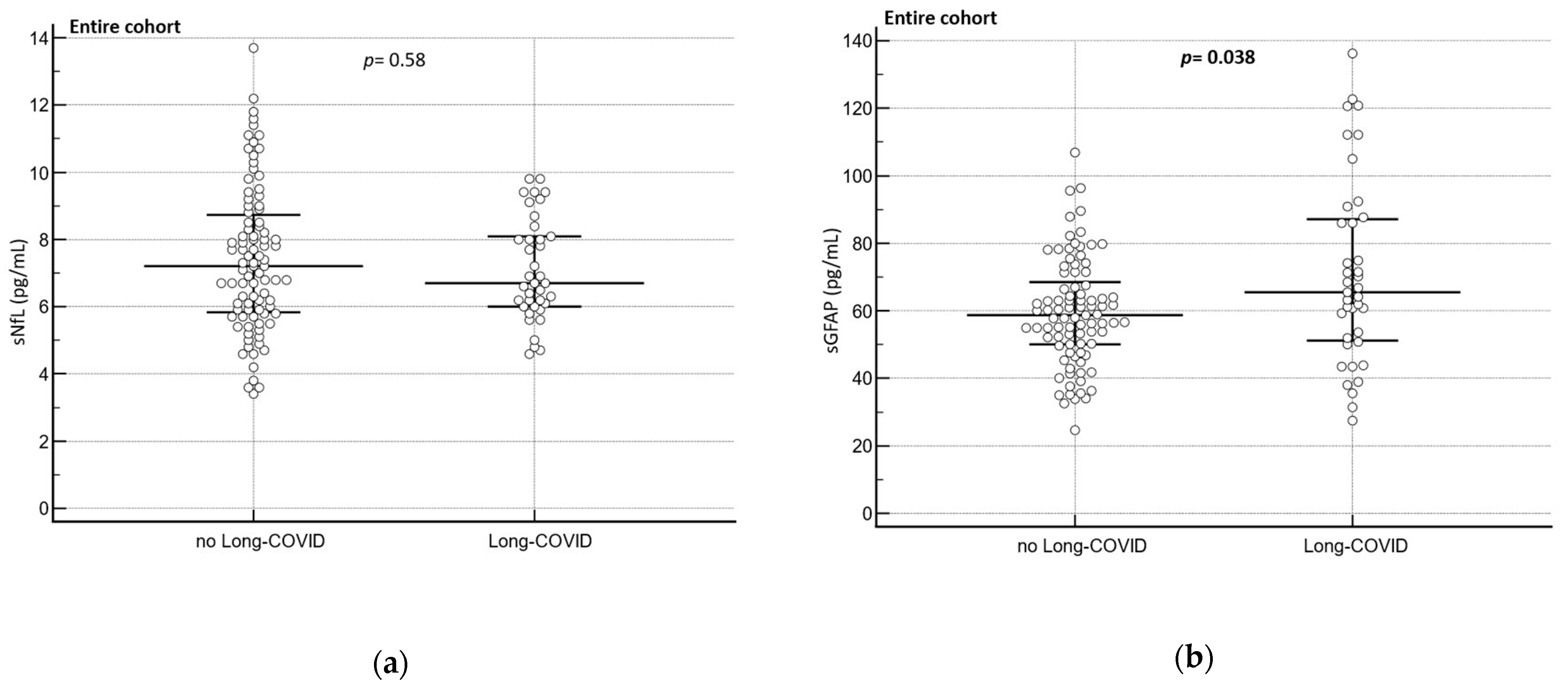
3.3. Biomarkers of Brain Injury in Participants with Long COVID
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Whittaker, A.; Anson, M.; Harky, A. Neurological Manifestations of COVID-19: A systematic review and current update. Acta Neurol. Scand. 2020, 142, 14–22. [Google Scholar] [CrossRef]
- Chou, S.H.-Y.; Beghi, E.; Helbok, R.; Moro, E.; Sampson, J.; Altamirano, V.; Mainali, S.; Bassetti, C.; Suarez, J.I.; McNett, M.; et al. Global Incidence of Neurological Manifestations Among Patients Hospitalized With COVID-19—A Report for the GCS-NeuroCOVID Consortium and the ENERGY Consortium. JAMA Netw. Open 2021, 4, e2112131. [Google Scholar] [CrossRef] [PubMed]
- Helms, J.; Kremer, S.; Merdji, H.; Clere-Jehl, R.; Schenck, M.; Kummerlen, C.; Collange, O.; Boulay, C.; Fafi-Kremer, S.; Ohana, M.; et al. Neurologic Features in Severe SARS-CoV-2 Infection. N. Engl. J. Med. 2020, 382, 2268–2270. [Google Scholar] [CrossRef] [PubMed]
- Rogers, J.P.; Chesney, E.; Oliver, D.; Pollak, T.A.; McGuire, P.; Fusar-Poli, P.; Zandi, M.S.; Lewis, G.; David, A.S. Psychiatric and neuropsychiatric presentations associated with severe coronavirus infections: A systematic review and meta-analysis with comparison to the COVID-19 pandemic. Lancet Psychiatry 2020, 7, 611–627. [Google Scholar] [CrossRef]
- Soriano, J.B.; Murthy, S.; Marshall, J.C.; Relan, P.; Diaz, J. V A clinical case definition of post-COVID-19 condition by a Delphi consensus. Lancet Infect. Dis. 2022, 22, e102–e107. [Google Scholar] [CrossRef]
- Masvekar, R.R.; Kosa, P.; Jin, K.; Dobbs, K.; Stack, M.A.; Castagnoli, R.; Quaresima, V.; Su, H.C.; Imberti, L.; Notarangelo, L.D.; et al. Prognostic value of serum/plasma neurofilament light chain for COVID-19-associated mortality. Ann. Clin. Transl. Neurol. 2022, 9, 622–632. [Google Scholar] [CrossRef]
- Eng, L.F. Glial fibrillary acidic protein (GFAP): The major protein of glial intermediate filaments in differentiated astrocytes. J. Neuroimmunol. 1985, 8, 203–214. [Google Scholar] [CrossRef] [PubMed]
- Chmielewska, N.; Szyndler, J.; Makowska, K.; Wojtyna, D.; Maciejak, P.; Płaźnik, A. Looking for novel, brain-derived, peripheral biomarkers of neurological disorders. Neurol. Neurochir. Pol. 2018, 52, 318–325. [Google Scholar] [CrossRef] [Green Version]
- Amalia, L. Glial Fibrillary Acidic Protein (GFAP): Neuroinflammation Biomarker in Acute Ischemic Stroke. J. Inflamm. Res. 2021, 14, 7501–7506. [Google Scholar] [CrossRef]
- Khalil, M.; Teunissen, C.E.; Otto, M.; Piehl, F.; Sormani, M.P.; Gattringer, T.; Barro, C.; Kappos, L.; Comabella, M.; Fazekas, F.; et al. Neurofilaments as biomarkers in neurological disorders. Nat. Rev. Neurol. 2018, 14, 577–589. [Google Scholar] [CrossRef]
- Yuan, A.; Nixon, R.A. Neurofilament Proteins as Biomarkers to Monitor Neurological Diseases and the Efficacy of Therapies. Front. Neurosci. 2021, 15, 689938. [Google Scholar] [CrossRef] [PubMed]
- Gaetani, L.; Blennow, K.; Calabresi, P.; Di Filippo, M.; Parnetti, L.; Zetterberg, H. Neurofilament light chain as a biomarker in neurological disorders. J. Neurol. Neurosurg. Psychiatry 2019, 90, 870–881. [Google Scholar] [CrossRef]
- Frontera, J.A.; Boutajangout, A.; Masurkar, A.V.; Betensky, R.A.; Ge, Y.; Vedvyas, A.; Debure, L.; Moreira, A.; Lewis, A.; Huang, J.; et al. Comparison of serum neurodegenerative biomarkers among hospitalized COVID-19 patients versus non-COVID subjects with normal cognition, mild cognitive impairment, or Alzheimer’s dementia. Alzheimer’s Dement. 2022, 18, 899–910. [Google Scholar] [CrossRef] [PubMed]
- Aamodt, A.H.; Høgestøl, E.A.; Popperud, T.H.; Holter, J.C.; Dyrhol-Riise, A.M.; Tonby, K.; Stiksrud, B.; Quist-Paulsen, E.; Berge, T.; Barratt-Due, A.; et al. Blood neurofilament light concentration at admittance: A potential prognostic marker in COVID-19. J. Neurol. 2021, 268, 3574–3583. [Google Scholar] [CrossRef] [PubMed]
- Prudencio, M.; Erben, Y.; Marquez, C.P.; Jansen-West, K.R.; Franco-Mesa, C.; Heckman, M.G.; White, L.J.; Dunmore, J.A.; Cook, C.N.; Lilley, M.T.; et al. Serum neurofilament light protein correlates with unfavorable clinical outcomes in hospitalized patients with COVID-19. Sci. Transl. Med. 2021, 13, eabi7643. [Google Scholar] [CrossRef]
- Cooper, J.; Stukas, S.; Hoiland, R.L.; Fergusson, N.A.; Thiara, S.; Foster, D.; Mitra, A.; Stoessl, J.A.; Panenka, W.J.; Sekhon, M.S.; et al. Quantification of Neurological Blood-Based Biomarkers in Critically Ill Patients With Coronavirus Disease 2019. Crit. Care Explor. 2020, 2, e0238. [Google Scholar] [CrossRef]
- De Lorenzo, R.; Loré, N.I.; Finardi, A.; Mandelli, A.; Cirillo, D.M.; Tresoldi, C.; Benedetti, F.; Ciceri, F.; Rovere-Querini, P.; Comi, G.; et al. Blood neurofilament light chain and total tau levels at admission predict death in COVID-19 patients. J. Neurol. 2021, 268, 4436–4442. [Google Scholar] [CrossRef]
- Parasher, A. COVID-19: Current understanding of its Pathophysiology, Clinical presentation and Treatment. Postgrad. Med. J. 2021, 97, 312–320. [Google Scholar] [CrossRef]
- Havdal, L.B.; Berven, L.L.; Selvakumar, J.; Stiansen-Sonerud, T.; Leegaard, T.M.; Tjade, T.; Zetterberg, H.; Blennow, K.; Wyller, V.B.B. Neurological Involvement in COVID-19 Among Non-Hospitalized Adolescents and Young Adults. Front. Neurol. 2022, 13, 915712. [Google Scholar] [CrossRef]
- Ameres, M.; Brandstetter, S.; Toncheva, A.A.; Kabesch, M.; Leppert, D.; Kuhle, J.; Wellmann, S. Association of neuronal injury blood marker neurofilament light chain with mild-to-moderate COVID-19. J. Neurol. 2020, 267, 3476–3478. [Google Scholar] [CrossRef]
- Conen, D.; Schön, T.; Aeschbacher, S.; Paré, G.; Frehner, W.; Risch, M.; Risch, L. Genetic and phenotypic determinants of blood pressure and other cardiovascular risk factors (GAPP). Swiss. Med. Wkly. 2013, 143, w13728. [Google Scholar] [CrossRef]
- Risch, M.; Grossmann, K.; Aeschbacher, S.; Weideli, O.C.; Kovac, M.; Pereira, F.; Wohlwend, N.; Risch, C.; Hillmann, D.; Lung, T.; et al. Investigation of the use of a sensor bracelet for the presymptomatic detection of changes in physiological parameters related to COVID-19: An interim analysis of a prospective cohort study (COVI-GAPP). BMJ Open 2022, 12, e058274. [Google Scholar] [CrossRef]
- Khalil, M.; Pirpamer, L.; Hofer, E.; Voortman, M.M.; Barro, C.; Leppert, D.; Benkert, P.; Ropele, S.; Enzinger, C.; Fazekas, F.; et al. Serum neurofilament light levels in normal aging and their association with morphologic brain changes. Nat. Commun. 2020, 11, 812. [Google Scholar] [CrossRef] [Green Version]
- Thiel, S.L.; Weber, M.C.; Risch, L.; Wohlwend, N.; Lung, T.; Hillmann, D.; Ritzler, M.; Risch, M.; Kohler, P.; Vernazza, P.; et al. Flattening the curve in 52 days: Characterisation of the COVID-19 pandemic in the Principality of Liechtenstein—An observational study. Swiss. Med. Wkly. 2020, 150, w20361. [Google Scholar] [CrossRef]
- Goncalves Cabecinhas, A.R.; Roloff, T.; Stange, M.; Bertelli, C.; Huber, M.; Ramette, A.; Chen, C.; Nadeau, S.; Gerth, Y.; Yerly, S.; et al. SARS-CoV-2 N501Y Introductions and Transmissions in Switzerland from Beginning of October 2020 to February 2021—Implementation of Swiss-Wide Diagnostic Screening and Whole Genome Sequencing. Microorganisms 2021, 9, 677. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Nadeau, S.A.; Topolsky, I.; Manceau, M.; Huisman, J.S.; Jablonski, K.P.; Fuhrmann, L.; Dreifuss, D.; Jahn, K.; Beckmann, C.; et al. Quantification of the spread of SARS-CoV-2 variant B.1.1.7 in Switzerland. Epidemics 2021, 37, 100480. [Google Scholar] [CrossRef] [PubMed]
- Newcombe, V.F.J.; Ashton, N.J.; Posti, J.P.; Glocker, B.; Manktelow, A.; Chatfield, D.A.; Winzeck, S.; Needham, E.; Correia, M.M.; Williams, G.B.; et al. Post-acute blood biomarkers and disease progression in traumatic brain injury. Brain 2022, 145, 2064–2076. [Google Scholar] [CrossRef]
- Zimmermann, P.; Curtis, N. Why Does the Severity of COVID-19 Differ With Age? Pediatr. Infect. Dis. J. 2022, 41, e36–e45. [Google Scholar] [CrossRef] [PubMed]
- van Lierop, Z.Y.G.J.; Verbek, I.M.W.; van Uffelen, K.W.J.; Koel-Simmelink, M.J.A.; In’t Veld, L.; Killestein, J.; Teunissen, C. Pre-analytical stability of serum biomarkers for neurological disease: Neurofilament-light, glial fibrillary acidic protein and contactin-1. Clin. Chem. Lab. Med. 2022, 60, 842–850. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Entire Cohort n = 146 | Mild Infection (No Hospitalization) n = 133 | Moderate Infection (Hospitalization) n = 13 | p-Value |
|---|---|---|---|---|
| Age, years (SD) | 43.2 (5.6) | 43.4 (5.4) | 41.5 (6.1) | p = 0.13 |
| Sex, female (%) | 88 (60%) | 81 (61%) | 7 (54%) | p = 0.62 |
| Duration acute SARS-CoV-2 infection, days (SD) * | 9.6 (6.73) | 8.3 (5.04) | 22 (8) | p < 0.0001 |
| Long COVID-19 (%) | 39 (26%) | 30 (23%) | 9 (69%) | p = 0.01 |
| Symptoms quantity 1–5 | 77 (54%) | 74 (57%) | 3 (23%) | p = 0.02 |
| Symptoms quantity 6–10 | 56 (39%) | 52 (40%) | 4 (31%) | p = 0.51 |
| Symptoms quantity 11–15 | 10 (7%) | 4 (3%) | 6 (46%) | p < 0.0001 |
| Headache (%) | 97 (66%) | 87 (67%) | 10 (78%) | p = 0.46 |
| Fatigue (%) | 83 (57%) | 74 (57%) | 9 (69%) | p = 0.39 |
| Arthralgia (%) | 71 (49%) | 61 (47%) | 10 (78%) | p = 0.04 |
| Anosmia (%) | 66 (45%) | 58 (45%) | 8 (62%) | p = 0.24 |
| Ageusia (%) | 55 (38%) | 48 (37%) | 7 (54%) | p = 0.23 |
| Fever (%) | 51 (35%) | 41 (31.5%) | 10 (77%) | p = 0.001 |
| Chills (%) | 36 (25%) | 28 (22%) | 8 (62%) | p = 0.001 |
| Cough (%) | 65 (45%) | 56 (43%) | 9 (70%) | p = 0.07 |
| Rhinitis (%) | 58 (40%) | 52 (40%) | 6 (46%) | p = 0.67 |
| Dyspnea (%) | 23 (16%) | 18 (14%) | 5 (38%) | p = 0.02 |
| Thoracic tightness (%) | 22 (15%) | 14 (11%) | 8 (62%) | p < 0.0001 |
| Sore throat (%) | 40 (27%) | 34 (26%) | 6 (46%) | p = 0.13 |
| General illness (%) | 65 (45%) | 55 (42%) | 10 (77%) | p = 0.02 |
| Diarrhea (%) | 28 (19%) | 22 (17%) | 6 (46%) | p = 0.01 |
| Sickness (%) | 22 (15%) | 16 (12%) | 6 (46%) | p = 0.001 |
| Vomiting (%) | 8 (5%) | 3 (2%) | 5 (38%) | p < 0.0001 |
| sNfL | sGFAP | |||
|---|---|---|---|---|
| Variables | Coefficient (Sth. Error) | p-Value | Coefficient (Sth. Error) | p-Value |
| Age | b1 = 0.11 (0.03) | p = 0.002 | b1 = 0.54 (0.35) | p = 0.12 |
| Sex | b1 = 0.17 (0.43) | p = 0.78 | b1 = 5.27 (4.26) | p = 0.22 |
| sNfL before Infection vs. after Infection | sGFAP before Infection vs. after Infection | |||||
|---|---|---|---|---|---|---|
| Symptoms | Median | IQR | p-Value | Median | IQR | p-Value |
| headache | 7.1 vs. 7.2 | 5.7 to 8.7 vs. 5.9 to 8.8 | p = 0.25 | 60.5 vs. 60.4 | 47.6 to 72.2 vs. 51.3 to 68.1 | p = 0.51 |
| fatigue | 7.2 vs. 7.2 | 5.9 to 9.2 vs. 5.8 to 8.5 | p = 0.84 | 61.4 vs. 59.4 | 47.6 to 72.2 vs. 51.1 to 67.2 | p = 0.93 |
| anosmia | 12.3 vs. 12.6 | 5.8 to 9.0 vs. 5.7 to 8.8 | p = 0.88 | 60.7 vs. 58.7 | 49.4 to 72.7 vs. 51.3 to 67.4 | p = 0.77 |
| ageusia | 7.2 vs. 7.2 | 5.9 to 8.9 vs. 5.6 to 8.1 | p = 0.73 | 61.1 vs. 56.9 | 47.9 to 75.5 vs. 46.9 to 66.3 | p = 0.47 |
| sNfL | sGFAP | |||||
|---|---|---|---|---|---|---|
| Symptoms | Median | IQR | p-Value | Median | IQR | p-Value |
| headache vs. no headache | 7.2 vs. 7.3 | 5.9 to 8.8 vs. 6.0 to 9.0 | p = 0.89 | 60.4 vs. 58.4 | 50.9 to 68.3 vs. 50.0 to 72.2 | p = 0.99 |
| fatigue vs. no fatigue | 7.2 vs. 7.2 | 5.8 to 8.5 vs. 6.2 to 9.0 | p = 0.69 | 59.7 vs. 60.2 | 50.3 to 67.3 vs. 50.1 to 75.9 | p = 0.38 |
| anosmia vs. no anosmia | 7.4 vs. 7.2 | 5.7 to 8.8 vs. 6.5 to 8.9 | p = 0.99 | 58.5 vs. 60.2 | 49.4 to 67.3 vs. 50.1 to 71.5 | p = 0.41 |
| ageusia vs. no ageusia | 7.2 vs. 7.2 | 5.6 to 8.1 vs. 6.1 to 9.1 | p = 0.25 | 56.2 vs. 61.0 | 44.7 to 65.9 vs. 50.7 to 71.5 | p = 0.09 |
| sNfL before Infection vs. after Infection | sGFAP before Infection vs. after Infection | |||||
|---|---|---|---|---|---|---|
| Symptoms | Median | IQR | p-Value | Median | IQR | p-Value |
| headache | 6.9 to 6.9 | 5.8 to 8.4 vs. 5.5 to 7.8 | p = 0.29 | 67.7 to 66.9 | 52.0 to 79.5 vs. 45.2 to 73.5 | p = 0.71 |
| fatigue | 7.3 vs. 6.9 | 5.8 to 9.3 vs. 5.5 to 8.4 | p = 0.17 | 66.8 to 69.9 | 47.4 to 82.7 vs. 51.8 to 86.0 | p = 0.39 |
| anosmia | 7.3 vs. 6.7 | 5.3 to 8.8 vs. 50.6 to 8.3 | p = 0.35 | 59.0 vs. 60.9 | 47.9 to 74.6 vs. 50.1 to 70.1 | p = 0.35 |
| ageusia | 6.7 vs. 6.6 | 5.3 to 8.6 vs. 5.6 to 7.9 | p = 0.23 | 61.7 vs. 60.7 | 49.5 to 76.8 vs. 45.3 to 71.0 | p = 0.16 |
| sNfL | sGFAP | |||||
|---|---|---|---|---|---|---|
| Symptoms | Median | IQR | p-Value | Median | IQR | p-Value |
| headache vs. no headache | 6.9 vs. 6.7 | 5.5 to 7.8 vs. 6.0 to 7.7 | p = 0.82 | 68.5 vs. 60.7 | 49.0 to 83.6 vs. 51.0 to 65.5 | p = 0.32 |
| fatigue vs. no fatigue | 6.9 vs. 6.2 | 5.5 to 8.4 vs. 5.8 to 6.5 | p = 0.35 | 67.7 vs. 60.7 | 50.1 to 86.0 vs. 53.8 to 66.1 | p = 0.62 |
| anosmia vs. no anosmia | 6.6 vs. 6.6 | 5.8 to 7.9 vs. 6.0 to 8.0 | p = 0.56 | 61.5 vs. 66.8 | 50.0 to 71.4 vs. 48.5 to 91.2 | p = 0.53 |
| ageusia vs. no ageusia | 6.6 vs. 6.6 | 5.8 to 7.9 vs. 6.0 to 8.0 | p = 0.56 | 61.5 vs. 66.8 | 50.0 to 71.4 vs. 48.5 to 91.2 | p = 0.53 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Telser, J.; Grossmann, K.; Weideli, O.C.; Hillmann, D.; Aeschbacher, S.; Wohlwend, N.; Velez, L.; Kuhle, J.; Maleska, A.; Benkert, P.; et al. Concentrations of Serum Brain Injury Biomarkers Following SARS-CoV-2 Infection in Individuals with and without Long-COVID—Results from the Prospective Population-Based COVI-GAPP Study. Diagnostics 2023, 13, 2167. https://doi.org/10.3390/diagnostics13132167
Telser J, Grossmann K, Weideli OC, Hillmann D, Aeschbacher S, Wohlwend N, Velez L, Kuhle J, Maleska A, Benkert P, et al. Concentrations of Serum Brain Injury Biomarkers Following SARS-CoV-2 Infection in Individuals with and without Long-COVID—Results from the Prospective Population-Based COVI-GAPP Study. Diagnostics. 2023; 13(13):2167. https://doi.org/10.3390/diagnostics13132167
Chicago/Turabian StyleTelser, Julia, Kirsten Grossmann, Ornella C. Weideli, Dorothea Hillmann, Stefanie Aeschbacher, Niklas Wohlwend, Laura Velez, Jens Kuhle, Aleksandra Maleska, Pascal Benkert, and et al. 2023. "Concentrations of Serum Brain Injury Biomarkers Following SARS-CoV-2 Infection in Individuals with and without Long-COVID—Results from the Prospective Population-Based COVI-GAPP Study" Diagnostics 13, no. 13: 2167. https://doi.org/10.3390/diagnostics13132167
APA StyleTelser, J., Grossmann, K., Weideli, O. C., Hillmann, D., Aeschbacher, S., Wohlwend, N., Velez, L., Kuhle, J., Maleska, A., Benkert, P., Risch, C., Conen, D., Risch, M., & Risch, L. (2023). Concentrations of Serum Brain Injury Biomarkers Following SARS-CoV-2 Infection in Individuals with and without Long-COVID—Results from the Prospective Population-Based COVI-GAPP Study. Diagnostics, 13(13), 2167. https://doi.org/10.3390/diagnostics13132167