
Cancer Stem Cell Markers in Rhabdomyosarcoma in Children


 , , ,
, , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Analyzed Clinical Parameters
2.3. Immunohistochemistry
2.4. Statistical Analysis
3. Results
3.1. Study Population
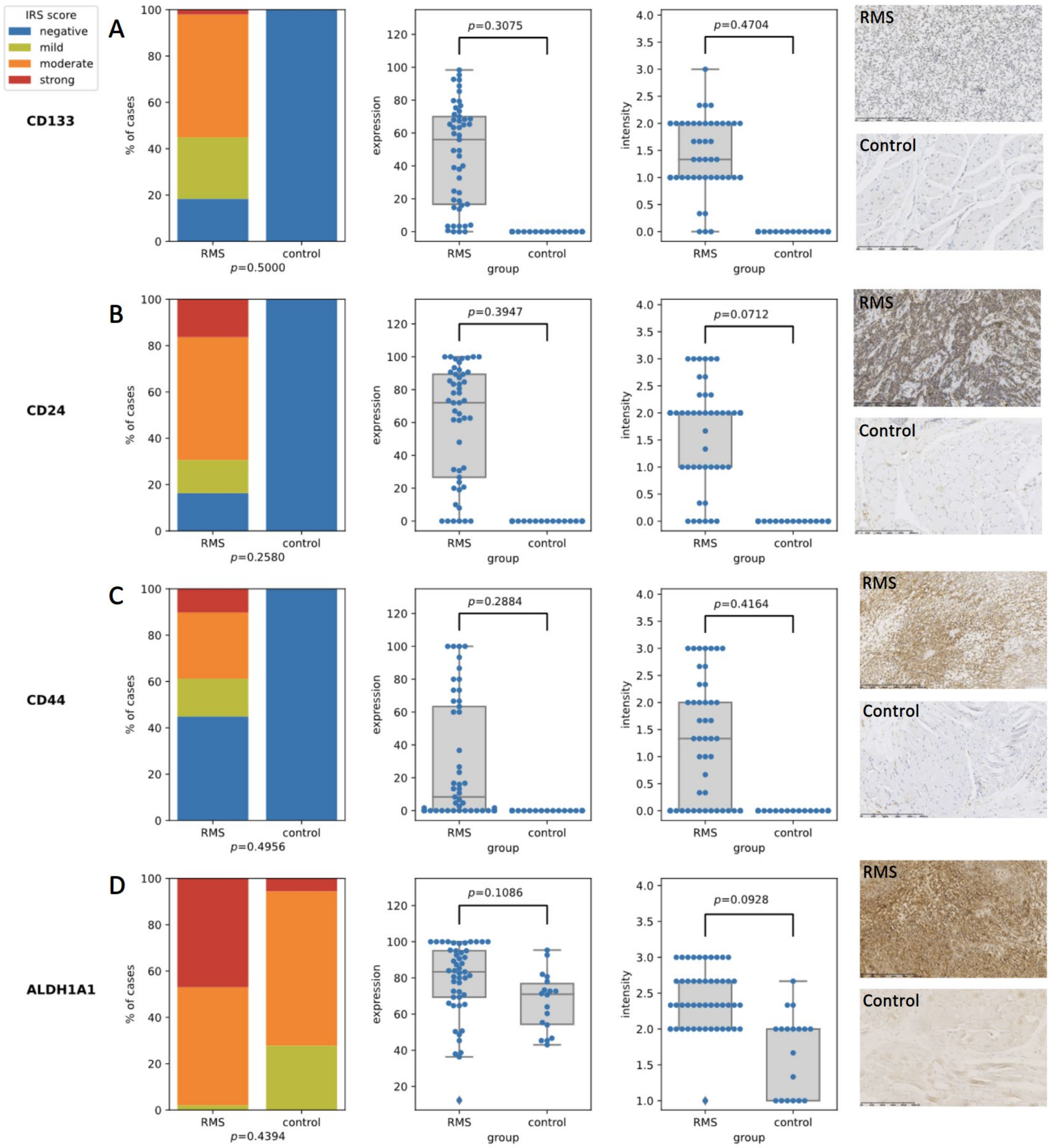
3.2. CD24, CD44, CD133, and ALDH1A1 Expression in RMS
3.3. Expression of Stem Cell Markers in Different Disease Stages
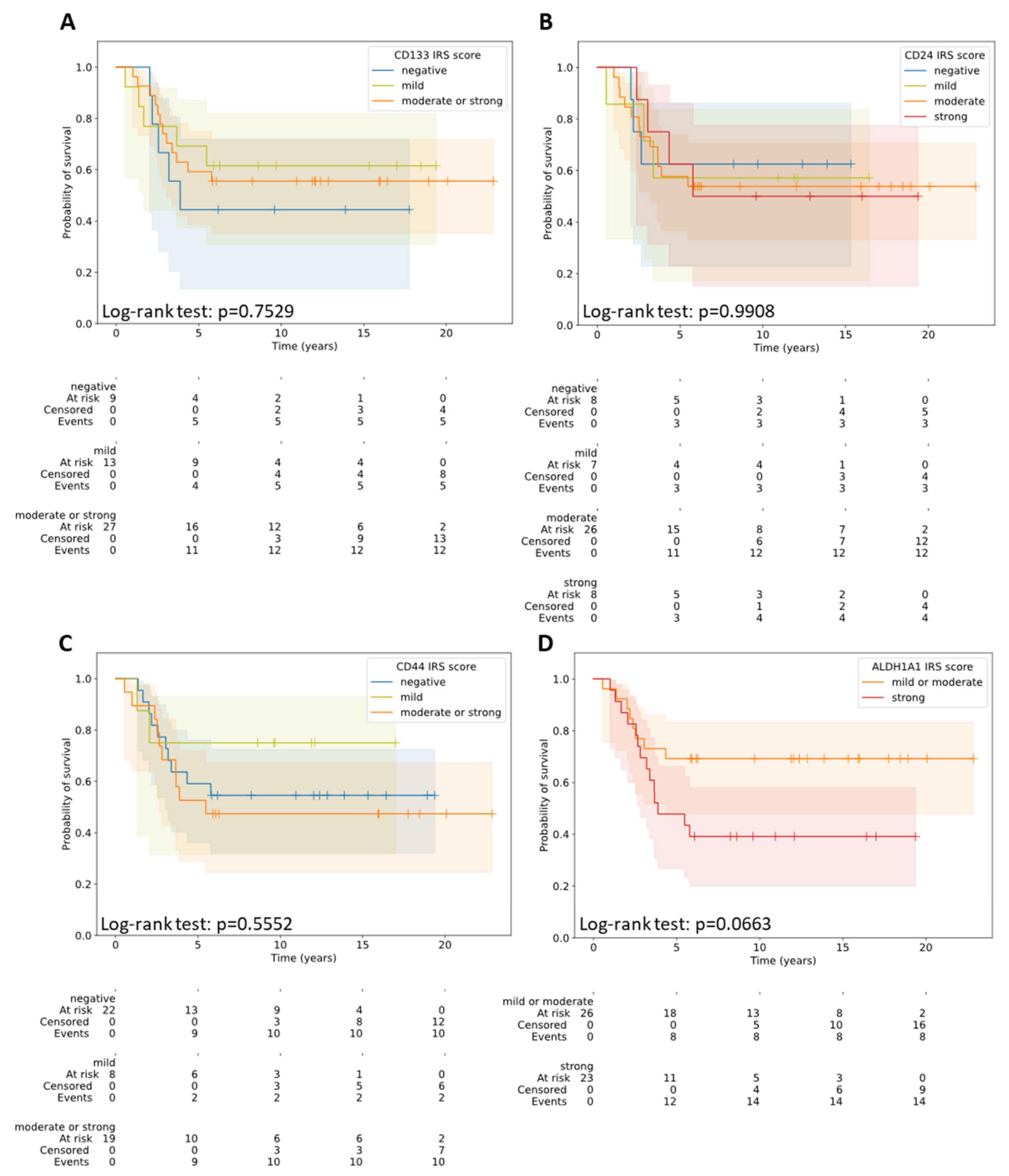
3.4. Overall Survival Prognostic Factors
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dasgupta, R.; Fuchs, J.; Rodeberg, D. Rhabdomyosarcoma. Semin. Pediatr. Surg. 2016, 25, 276–283. [Google Scholar] [CrossRef]
- Shern, J.F.; Yohe, M.E.; Khan, J. Pediatric Rhabdomyosarcoma. Crit. Rev. Oncog. 2015, 20, 227–243. [Google Scholar] [CrossRef] [PubMed]
- Ognjanovic, S.; Linabery, A.M.; Charbonneau, B.; Ross, J.A. Trends in childhood rhabdomyosarcoma incidence and survival in the United States, 1975–2005. Cancer 2009, 115, 4218–4226. [Google Scholar] [CrossRef] [PubMed]
- Parham, D.M.; Barr, F.G. Classification of rhabdomyosarcoma and its molecular basis. Adv. Anat. Pathol. 2013, 20, 387–397. [Google Scholar] [CrossRef] [PubMed]
- Radzikowska, J.; Kukwa, W.; Kukwa, A. Rhabdomyosarcoma of the head and neck in children. Contemp. Oncol. 2015, 19, 98–107. [Google Scholar]
- Fiedorowicz, M.; Bartnik, E.; Sobczuk, P.; Teterycz, P.; Czarnecka, A.M. Molecular biology of sarcoma. Oncol. Clin. Pract. 2018, 14, 307–330. [Google Scholar] [CrossRef]
- Crane, J.N.W.X.; Qumseya, A.; Zhengya, G.; Arndt, C.A.S.; Donaldson, S.S. Clinical group and modified TNM stage for rhabdomyosarcoma: A review from the Children’s Oncology Group. Pediatr. Blood Cancer 2022, 69, e29644. [Google Scholar] [CrossRef]
- Skapek, S.X.; Anderson, J.; Barr, F.G.; Bridge, J.A.; Gastier-Foster, J.M.; Parham, D.M.; Rudzinski, E.R.; Triche, T.; Hawkins, D.S. PAX-FOXO1 fusion status drives unfavorable outcome for children with rhabdomyosarcoma: A children's oncology group report. Pediatr. Blood Cancer 2013, 60, 1411–1417. [Google Scholar] [CrossRef]
- Genadry, K.C.; Pietrobono, S.; Rota, R.; Linardic, C.M. Soft Tissue Sarcoma Cancer Stem Cells: An Overview. Front. Oncol. 2018, 8, 475. [Google Scholar] [CrossRef]
- Visvader, J.E.; Lindeman, G.J. Cancer stem cells in solid tumours, accumulating evidence and unresolved questions. Nat. Rev. Cancer 2008, 8, 755–768. [Google Scholar] [CrossRef]
- Lawrence, W., Jr.; Anderson, J.R.; Gehan, E.A.; Maurer, H. Pretreatment TNM staging of childhood rhabdomyosarcoma, a report of the Intergroup Rhabdomyosarcoma Study Group. Children's Cancer Study Group. Pediatric Oncology Group. Cancer 1997, 80, 1165–1170. [Google Scholar] [CrossRef]
- Remmele, W.; Stegner, H.E. Recommendation for uniform definition of an immunoreactive score (IRS) for immunohistochemical estrogen receptor detection (ER-ICA) in breast cancer tissue. Pathologe 1987, 8, 138–140. [Google Scholar]
- Sana, J.; Zambo, I.; Skoda, J.; Neradil, J.; Chlapek, P.; Hermanova, M.; Mudry, P.; Vasikova, A.; Zitterbart, K.; Hampl, A.; et al. CD133 expression and identification of CD133/nestin positive cells in rhabdomyosarcomas and rhabdomyosarcoma cell lines. Anal. Cell Pathol. 2011, 34, 303–318. [Google Scholar] [CrossRef][Green Version]
- Walter, D.; Satheesha, S.; Albrecht, P.; Bornhauser, B.; D'Alessandro, V.; Oesch, S.M.; Rehrauer, H.; Leuschner, I.; Koscielniak, E.; Gengler, C.; et al. CD133 positive embryonal rhabdomyosarcoma stem-like cell population is enriched in rhabdospheres. PLoS ONE 2011, 6, e19506. [Google Scholar] [CrossRef]
- Pressey, J.G.; Haas, M.C.; Pressey, C.S.; Kelly, V.M.; Parker, J.N.; Gillespie, G.Y.; Friedman, G.K. CD133 marks a myogenically primitive subpopulation in rhabdomyosarcoma cell lines that are relatively chemoresistant but sensitive to mutant HSV. Pediatr. Blood Cancer 2013, 60, 45–52. [Google Scholar] [CrossRef]
- Zambo, I.; Hermanova, M.; Zapletalova, D.; Skoda, J.; Mudry, P.; Kyr, M.; Zitterbart, K.; Sterba, J.; Veselska, R. Expression of nestin, CD133 and ABCG2 in relation to the clinical outcome in pediatric sarcomas. Cancer Biomark. 2016, 17, 107–116. [Google Scholar] [CrossRef]
- Yin, A.H.; Miraglia, S.; Zanjani, E.D.; Almeida-Porada, G.; Ogawa, M.; Leary, A.G.; Olweus, J.; Kearney, J.; Buck, D.W. AC133, a novel marker for human hematopoietic stem and progenitor cells. Blood 1997, 90, 5002–5012. [Google Scholar] [CrossRef]
- Miraglia, S.; Godfrey, W.; Yin, A.H.; Atkins, K.; Warnke, R.; Holden, J.T.; Bray, R.A.; Waller, E.K.; Buck, D.W. A novel five-transmembrane hematopoietic stem cell antigen: Isolation, characterization, and molecular cloning. Blood 1997, 90, 5013–5021. [Google Scholar] [CrossRef]
- Fargeas, C.A.; Florek, M.; Huttner, W.B.; Corbeil, D. Characterization of prominin-2, a new member of the prominin family of pentaspan membrane glycoproteins. J. Biol. Chem. 2003, 278, 8586–8596. [Google Scholar] [CrossRef]
- Weigmann, A.; Corbeil, D.; Hellwig, A.; Huttner, W.B. Prominin, a novel microvilli-specific polytopic membrane protein of the apical surface of epithelial cells, is targeted to plasmalemmal protrusions of non-epithelial cells. Proc. Natl. Acad. Sci. USA 1997, 94, 12425–12430. [Google Scholar] [CrossRef]
- Corbeil, D.; Roper, K.; Fargeas, C.A.; Joester, A.; Huttner, W.B. Prominin: A story of cholesterol, plasma membrane protrusions and human pathology. Traffic 2001, 2, 82–91. [Google Scholar] [CrossRef]
- Corbeil, D.; Marzesco, A.M.; Wilsch-Brauninger, M.; Huttner, W.B. The intriguing links between prominin-1 (CD133), cholesterol-based membrane microdomains, remodeling of apical plasma membrane protrusions, extracellular membrane particles, and (neuro)epithelial cell differentiation. FEBS Lett. 2010, 584, 1659–1664. [Google Scholar] [CrossRef]
- Marzesco, A.M.; Janich, P.; Wilsch-Brauninger, M.; Dubreuil, V.; Langenfeld, K.; Corbeil, D.; Huttner, W.B. Release of extracellular membrane particles carrying the stem cell marker prominin-1 (CD133) from neural progenitors and other epithelial cells. J. Cell Sci. 2005, 118, 2849–2858. [Google Scholar] [CrossRef]
- Humphrey, G.; Hazel, D.L.; MacLennan, K.; Lewis, I. Expression of CD44 by rhabdomyosarcoma, a new prognostic marker? Br. J. Cancer 1999, 80, 918–921. [Google Scholar] [CrossRef][Green Version]
- Saxon, B.R.; Byard, R.W.; Han, P. Cellular expression of adhesion factors in childhood rhabdomyosarcoma. Pediatr. Pathol. Lab. Med. 1997, 17, 259–266. [Google Scholar] [CrossRef]
- Heerema-McKenney, A.; Wijnaendts, L.C.; Pulliam, J.F.; Lopez-Terrada, D.; McKenney, J.K.; Zhu, S.; Montgomery, K.; Mitchell, J.; Marinelli, R.J.; Hart, A.A.M.; et al. Diffuse myogenin expression by immunohistochemistry is an independent marker of poor survival in pediatric rhabdomyosarcoma: A tissue microarray study of 71 primary tumors including correlation with molecular phenotype. Am. J. Surg. Pathol. 2008, 32, 1513–1522. [Google Scholar] [CrossRef]
- Goodison, S.; Urquidi, V.; Tarin, D. CD44 cell adhesion molecules. Mol. Pathol. 1999, 52, 189–196. [Google Scholar] [CrossRef]
- Yan, Y.; Zuo, X.; Wei, D. Concise Review: Emerging Role of CD44 in Cancer Stem Cells: A Promising Biomarker and Therapeutic Target. Stem Cells Transl. Med. 2015, 4, 1033–1043. [Google Scholar] [CrossRef]
- Heyse, T.J.; Malcherczyk, D.; Moll, R.; Timmesfeld, N.; Wapelhorst, J.; Fuchs-Winkelmann, S.; Paletta, J.; Schofer, M. CD44: Survival and metastasis in chondrosarcoma. Osteoarthr. Cartil. 2010, 18, 849–856. [Google Scholar] [CrossRef]
- Karbownik, M.S.; Nowak, J.Z. Hyaluronan in cancer—Pathophysiology and pharmacotherapy perspectives. Nowotwory 2011, 61, 380–395. [Google Scholar]
- Sagiv, E.; Arber, N. The novel oncogene CD24 and its arising role in the carcinogenesis of the GI tract: From research to therapy. Expert Rev. Gastroenterol. Hepatol. 2008, 2, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.M.; Ju, J.H.; Jang, K.; Yang, W.; Yi, J.Y.; Noh, D.Y.; Shin, I. CD24 regulates cell proliferation and transforming growth factor beta-induced epithelial to mesenchymal transition through modulation of integrin beta1 stability. Cell Signal. 2012, 24, 2132–2142. [Google Scholar] [CrossRef] [PubMed]
- Aigner, S.; Sthoeger, Z.M.; Fogel, M.; Weber, E.; Zarn, J.; Ruppert, M.; Zeller, Y.; Vestweber, D.; Stahel, R.; Sammar, M.; et al. CD24, a mucin-type glycoprotein, is a ligand for P-selectin on human tumor cells. Blood 1997, 89, 3385–3395. [Google Scholar] [CrossRef] [PubMed]
- Aigner, S.; Ramos, C.L.; Hafezi-Moghadam, A.; Lawrence, M.B.; Friederichs, J.; Altevogt, P.; Ley, K. CD24 mediates rolling of breast carcinoma cells on P-selectin. FASEB J. 1998, 12, 1241–1251. [Google Scholar] [CrossRef] [PubMed]
- Baumann, P.; Cremers, N.; Kroese, F.; Orend, G.; Chiquet-Ehrismann, R.; Uede, T.; Yagita, H.; Sleeman, J.P. CD24 expression causes the acquisition of multiple cellular properties associated with tumor growth and metastasis. Cancer Res. 2005, 65, 10783–10793. [Google Scholar] [CrossRef] [PubMed]
- Pors, K.; Moreb, J.S. Aldehyde dehydrogenases in cancer: An opportunity for biomarker and drug development? Drug Discov. Today 2014, 19, 1953–1963. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Torres, M.; Allan, A.L. Aldehyde dehydrogenase as a marker and functional mediator of metastasis in solid tumors. Clin. Exp. Metastasis 2016, 33, 97–113. [Google Scholar] [CrossRef]
- Greco, N.; Schott, T.; Mu, X.; Rothenberg, A.; Voigt, C.; McGough, R.L., III; Goodman, M.; Huard, J.; Weiss, K.R. ALDH Activity Correlates with Metastatic Potential in Primary Sarcomas of Bone. J. Cancer Ther. 2014, 5, 331–338. [Google Scholar] [CrossRef]
- Martinez-Cruzado, L.; Tornin, J.; Santos, L.; Rodriguez, A.; García-Castro, J.; Morís, F.; Rodriguez, R. Aldh1 Expression and Activity Increase During Tumor Evolution in Sarcoma Cancer Stem Cell Populations. Sci. Rep. 2016, 6, 27878. [Google Scholar] [CrossRef]
- Lohberger, B.; Rinner, B.; Stuendl, N.; Absenger, M.; Liegl-Atzwanger, B.; Walzer, S.M.; Windhager, R.; Leithner, A. Aldehyde dehydrogenase 1, a potential marker for cancer stem cells in human sarcoma. PLoS ONE 2012, 7, e43664. [Google Scholar] [CrossRef]
- Nakahata, K.; Uehara, S.; Nishikawa, S.; Kawatsu, M.; Zenitani, M.; Oue, T.; Okuyama, H. Aldehyde Dehydrogenase 1 (ALDH1) Is a Potential Marker for Cancer Stem Cells in Embryonal Rhabdomyosarcoma. PLoS ONE 2015, 10, e0125454. [Google Scholar] [CrossRef]
- Jackson, B.; Brocker, C.; Thompson, D.C.; Black, W.; Vasiliou, K.; Nebert, D.W.; Vasiliou, V. Update on the aldehyde dehydrogenase gene (ALDH) superfamily. Hum. Genom. 2011, 5, 283–303. [Google Scholar] [CrossRef]
- Ma, I.; Allan, A.L. The role of human aldehyde dehydrogenase in normal and cancer stem cells. Stem Cell Rev. 2011, 7, 292–306. [Google Scholar] [CrossRef]
- Clay, M.R.; Tabor, M.; Owen, J.H.; Carey, T.; Bradford, C.R.; Wolf, G.T.; Wicha, M.S.; Prince, M.E. Single-marker identification of head and neck squamous cell carcinoma cancer stem cells with aldehyde dehydrogenase. Head Neck 2010, 32, 1195–1201. [Google Scholar] [CrossRef]
- Ucar, D.; Cogle, C.R.; Zucali, J.R.; Ostmark, B.; Scott, E.W.; Zori, R.; Gray, B.A.; Moreb, J.S. Aldehyde dehydrogenase activity as a functional marker for lung cancer. Chem. Biol. Interact. 2009, 178, 48–55. [Google Scholar] [CrossRef]
- Rasheed, Z.A.; Yang, J.; Wang, Q.; Kowalski, J.; Freed, I.; Murter, C.; Hong, S.-M.; Koorstra, J.-B.; Rajeshkumar, N.V.; He, X.; et al. Prognostic significance of tumorigenic cells with mesenchymal features in pancreatic adenocarcinoma. J. Natl. Cancer Inst. 2010, 102, 340–351. [Google Scholar] [CrossRef]
- Bortolomai, I.; Canevari, S.; Facetti, I.; De Cecco, L.; Castellano, G.; Zacchetti, A.; Alison, M.R.; Miotti, S. Tumor initiating cells: Development and critical characterization of a model derived from the A431 carcinoma cell line forming spheres in suspension. Cell Cycle 2010, 9, 1194–1206. [Google Scholar] [CrossRef]
- Ginestier, C.; Hur, M.H.; Charafe-Jauffret, E.; Monville, F.; Dutcher, J.; Brown, M.; Jacquemier, J.; Viens, P.; Kleer, C.G.; Liu, S.; et al. ALDH1 is a marker of normal and malignant human mammary stem cells and a predictor of poor clinical outcome. Cell Stem Cell 2007, 1, 555–567. [Google Scholar] [CrossRef]
- Van den Hoogen, C.; van der Horst, G.; Cheung, H.; Buijs, J.T.; Lippitt, J.M.; Guzmán-Ramírez, N.; Hamdy, F.C.; Eaton, C.L.; Thalmann, G.N.; Cecchini, M.G.; et al. High aldehyde dehydrogenase activity identifies tumor-initiating and metastasis-initiating cells in human prostate cancer. Cancer Res. 2010, 70, 5163–5173. [Google Scholar] [CrossRef]
- Su, Y.; Qiu, Q.; Zhang, X.; Jiang, Z.; Leng, Q.; Liu, Z.; Stass, S.A.; Jiang, F. Aldehyde dehydrogenase 1 A1-positive cell population is enriched in tumor-initiating cells and associated with progression of bladder cancer. Cancer Epidemiol. Biomark. Prev. 2010, 19, 327–337. [Google Scholar] [CrossRef]
- Huang, E.H.; Hynes, M.J.; Zhang, T.; Ginestier, C.; Dontu, G.; Appelman, H.; Fields, J.Z.; Wicha, M.S.; Boman, B.M. Aldehyde dehydrogenase 1 is a marker for normal and malignant human colonic stem cells (SC) and tracks SC overpopulation during colon tumorigenesis. Cancer Res. 2009, 69, 3382–3389. [Google Scholar] [CrossRef]
- Dylla, S.J.; Beviglia, L.; Park, I.K.; Chartier, C.; Raval, J.; Ngan, L.; Pickell, K.; Aguilar, J.; Lazetic, S.; Smith-Berdan, S.; et al. Colorectal cancer stem cells are enriched in xenogeneic tumors following chemotherapy. PLoS ONE 2008, 3, e2428. [Google Scholar] [CrossRef]
- Croker, A.K.; Allan, A.L. Inhibition of aldehyde dehydrogenase (ALDH) activity reduces chemotherapy and radiation resistance of stem-like ALDHhiCD44(+) human breast cancer cells. Breast Cancer Res. Treat. 2012, 133, 75–87. [Google Scholar] [CrossRef]
- Brennan, S.K.; Meade, B.; Wang, Q.; Merchant, A.A.; Kowalski, J.; Matsui, W. Mantle cell lymphoma activation enhances bortezomib sensitivity. Blood 2010, 116, 4185–4191. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Chai, S.; Wang, P.; Zhang, C.; Yang, Y.; Wang, K. Aldehyde dehydrogenases and cancer stem cells. Cancer Lett. 2015, 369, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Sladek, N.E. Human aldehyde dehydrogenases: Potential pathological, pharmacological, and toxicological impact. J. Biochem. Mol. Toxicol. 2003, 17, 7–23. [Google Scholar] [CrossRef] [PubMed]
- Jean, E.; Laoudj-Chenivesse, D.; Notarnicola, C.; Rouger, K.; Serratrice, N.; Bonnieu, A.; Gay, S.; Bacou, F.; Duret, C.; Carnac, G. Aldehyde dehydrogenase activity promotes survival of human muscle precursor cells. J. Cell Mol. Med. 2011, 15, 119–133. [Google Scholar] [CrossRef] [PubMed]
- Kozakowska, M.; Dulak, J.; Jozkowicz, A. Mięśniowe komórki progenitorowe—Charakterystyka i funkcja. Post Biol. Kom. 2015, 42, 465–490. [Google Scholar]
- Tomita, H.; Tanaka, K.; Tanaka, T.; Hara, A. Aldehyde dehydrogenase 1A1 in stem cells and cancer. Oncotarget 2016, 7, 11018–11032. [Google Scholar] [CrossRef]
- Fedchenko, N.; Reifenrath, J. Different approaches for interpretation and reporting of immunohistochemistry analysis results in the bone tissue—A review. Diagn. Pathol. 2014, 9, 221. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Cancer (n = 49) | Control (n = 18) | p | |
|---|---|---|---|---|
| Gender | female | 19 | 12 | 0.0554 a |
| male | 30 | 6 | ||
| Age (years) | median (IQR) | 4.8 (2.3, 8.7) | 14.0 (8.5, 15.5) | 0.0001 b |
| Histologic subtype | ARMS | 19 (39%) | - | - |
| ERMS | 30 (61%) | - | - | |
| Tumor localization | favorable | 17 (35%) | - | - |
| unfavorable | 32 (65%) | - | - | |
| Tumor size | ≤5 cm | 16 (33%) | - | - |
| >5 cm | 33 (67%) | - | - | |
| T | T1 | 15 (31%) | - | - |
| T2 | 34 (69%) | - | - | |
| N | N0 | 39 (80%) | - | - |
| N1 | 10 (20%) | - | - | |
| M | M0 | 32 (65%) | - | - |
| M1 | 17 (35%) | - | - | |
| TNM stage | 1 | 15 (31%) | - | - |
| 2 | 2 (4%) | - | - | |
| 3 | 15 (31%) | - | - | |
| 4 | 17 (34%) | - | - |
| T1 | T2 | p | |||
|---|---|---|---|---|---|
| CD133 | Expression | median (IQR) | 58.7 (17.7, 68.3) | 52.7 (17.2, 71.0) | 0.4611 a |
| Intensity | median (IQR) | 1.0 (1.0, 1.8) | 1.3 (1.0, 2.0) | 0.2062 a | |
| IRS score | negative | 3 | 6 | 1.000 b | |
| mild | 4 | 9 | |||
| moderate | 8 | 18 | |||
| strong | 0 | 1 | |||
| CD24 | Expression | median (IQR) | 83.3 (64.0, 90.0) | 64.8 (21.4, 88.2) | 0.0822 a |
| Intensity | median (IQR) | 2.0 (1.5, 2.0) | 2.0 (1.0, 2.2) | 0.3596 a | |
| IRS score | negative | 1 | 7 | 0.3224 b | |
| mild | 1 | 6 | |||
| moderate | 11 | 15 | |||
| strong | 2 | 6 | |||
| CD44 | Expression | median (IQR) | 1.7 (0.0, 76.7) | 10.8 (0.0, 60.0) | 0.4119 a |
| Intensity | median (IQR) | 0.7 (0.0, 2.2) | 1.3 (0.0, 2.0) | 0.3077 a | |
| IRS score | negative | 8 | 14 | 0.6649 b | |
| mild | 1 | 7 | |||
| moderate | 4 | 10 | |||
| strong | 2 | 3 | |||
| ALDH1A1 | Expression | median (IQR) | 81.3 (71.0, 92.0) | 83.7 (66.8, 95.2) | 0.4524 a |
| Intensity | median (IQR) | 2.3 (2.0, 2.7) | 2.3 (2.1, 2.7) | 0.2544 a | |
| IRS score | mild | 1 | 0 | 0.3148 b | |
| moderate | 8 | 17 | |||
| strong | 6 | 17 |
| TNM Stage 1 + 2 + 3 | TNM Stage 4 | p | |||
|---|---|---|---|---|---|
| CD133 | expression | median (IQR) | 57.3 (16.5, 68.4) | 49.3 (23.7, 71.3) | 0.722 a |
| intensity | median (IQR) | 1.5 (1.0, 2.0) | 1.3 (1.0, 1.7) | 0.565 a | |
| IRS score | negative | 6 | 3 | reference | |
| mild | 8 | 5 | 0.515 b | ||
| moderate or strong | 18 | 9 | 0.757 b | ||
| CD24 | expression | median (IQR) | 62.7 (22.9, 87.8) | 78.0 (67.0, 93.3) | 0.363 a |
| intensity | median (IQR) | 2.0 (1.0, 2.0) | 2.0 (2.0, 2.3) | 0.632 a | |
| IRS score | negative | 5 | 3 | reference | |
| mild | 6 | 1 | 0.168 b | ||
| moderate | 17 | 9 | 0.578 b | ||
| strong | 4 | 4 | 0.939 b | ||
| CD44 | expression | median (IQR) | 12.0 (0.0, 73.3) | 4.7 (0.0, 60.0) | 0.634 a |
| intensity | median (IQR) | 1.2 (0.0, 2.1) | 1.3 (0.0, 2.0) | 0.953 a | |
| IRS score | negative | 15 | 7 | reference | |
| mild | 4 | 4 | 0.191 b | ||
| moderate or strong | 13 | 6 | 0.906 b | ||
| ALDH1A1 | expression | median (IQR) | 83.0 (68.3, 99.1) | 85.3 (72.3, 94.0) | 0.715 a |
| intensity | median (IQR) | 2.3 (2.0, 2.7) | 2.3 (2.3, 2.7) | 0.988 a | |
| IRS score | mild or moderate | 18 | 8 | reference | |
| strong | 14 | 9 | 0.697 b |
| Variable | Group | Median Survival (Years) | p (Log-Rank Test) |
|---|---|---|---|
| Gender | female | NA | 0.7533 |
| male | NA | ||
| Histologic subtype | ARMS | 3.4 | 0.0279 |
| ERMS | NA | ||
| Tumor localization | favorable | NA | 0.0977 |
| unfavorable | 5.5 | ||
| Tumor size | ≤5 cm | NA | 0.0134 |
| >5 cm | 4.3 | ||
| T | T1 | NA | 0.0241 |
| T2 | 4.3 | ||
| N | N0 | NA | 0.0168 |
| N1 | 2.7 | ||
| M | M0 | NA | 0.0006 |
| M1 | 3.2 | ||
| TNM stage | 1 | NA | 0.0045 |
| 2 | NA | ||
| 3 | NA | ||
| 4 | 3.2 | ||
| CD133 IRS score | negative | 3.9 | 0.7529 |
| mild | NA | ||
| moderate or strong | NA | ||
| CD24 IRS score | negative | NA | 0.9908 |
| mild | NA | ||
| moderate | NA | ||
| strong | NA | ||
| CD44 IRS score | negative | NA | 0.5552 |
| mild | NA | ||
| moderate or strong | 5.5 | ||
| ALDH1A1 IRS score | mild or moderate | NA | 0.0663 |
| strong | 3.9 |
| Variable | HR (95% CI) | p (Cox Regression) |
|---|---|---|
| Age | 1.11 (1.03, 1.21) | 0.0095 |
| CD133 expression * | 0.94 (0.82, 1.07) | 0.3256 |
| CD133 intensity | 0.71 (0.38, 1.35) | 0.3026 |
| CD24 expression * | 1.03 (0.91, 1.16) | 0.6487 |
| CD24 intensity | 1.31 (0.80, 2.14) | 0.2771 |
| CD44 expression * | 1.03 (0.92, 1.15) | 0.6391 |
| CD44 intensity | 1.07 (0.73, 1.56) | 0.7257 |
| ALDH1A1 expression * | 1.06 (0.85, 1.31) | 0.6272 |
| ALDH1A1 intensity | 2.44 (0.84, 7.13) | 0.1018 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Radzikowska, J.; Czarnecka, A.M.; Klepacka, T.; Rychłowska-Pruszyńska, M.; Raciborska, A.; Dembowska-Bagińska, B.; Pronicki, M.; Kukwa, A.; Fendler, W.; Smyczyńska, U.; et al. Cancer Stem Cell Markers in Rhabdomyosarcoma in Children. Diagnostics 2022, 12, 1895. https://doi.org/10.3390/diagnostics12081895
Radzikowska J, Czarnecka AM, Klepacka T, Rychłowska-Pruszyńska M, Raciborska A, Dembowska-Bagińska B, Pronicki M, Kukwa A, Fendler W, Smyczyńska U, et al. Cancer Stem Cell Markers in Rhabdomyosarcoma in Children. Diagnostics. 2022; 12(8):1895. https://doi.org/10.3390/diagnostics12081895
Chicago/Turabian StyleRadzikowska, Joanna, Anna M. Czarnecka, Teresa Klepacka, Magdalena Rychłowska-Pruszyńska, Anna Raciborska, Bożenna Dembowska-Bagińska, Maciej Pronicki, Andrzej Kukwa, Wojciech Fendler, Urszula Smyczyńska, and et al. 2022. "Cancer Stem Cell Markers in Rhabdomyosarcoma in Children" Diagnostics 12, no. 8: 1895. https://doi.org/10.3390/diagnostics12081895
APA StyleRadzikowska, J., Czarnecka, A. M., Klepacka, T., Rychłowska-Pruszyńska, M., Raciborska, A., Dembowska-Bagińska, B., Pronicki, M., Kukwa, A., Fendler, W., Smyczyńska, U., Kukwa, W., & Krzeski, A. (2022). Cancer Stem Cell Markers in Rhabdomyosarcoma in Children. Diagnostics, 12(8), 1895. https://doi.org/10.3390/diagnostics12081895