
Postpartum Assessment of the Correlation between Serum Hormone Levels of Estradiol, Progesterone, Prolactin and ß-HCG and Blood Pressure Measurements in Pre-Eclampsia Patients

 , , , ,
, , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Cases and Performed Measurements
2.2. Statistical Analysis
3. Results
3.1. Clinical and Laboratory Parameters of Study Cases
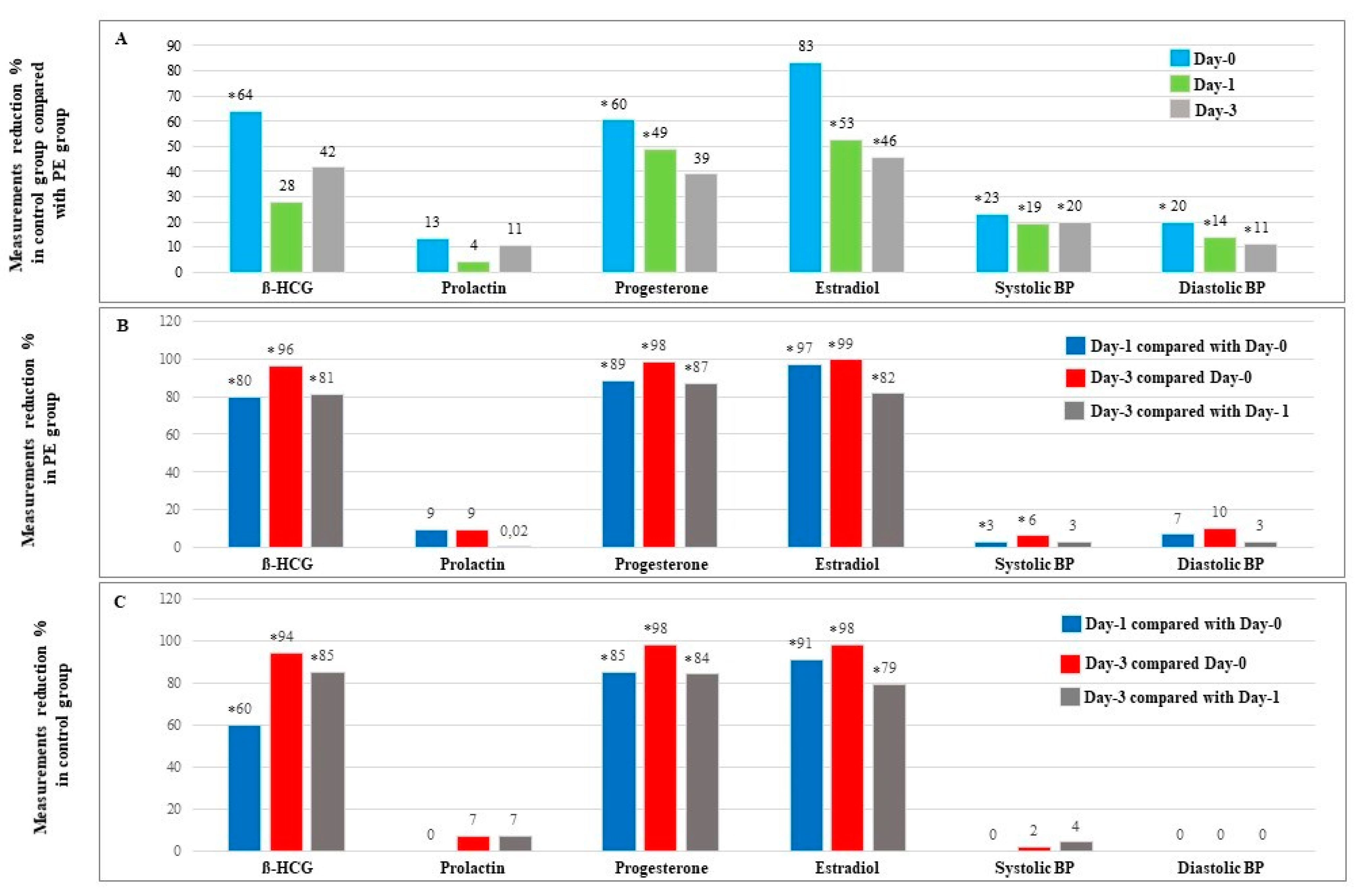
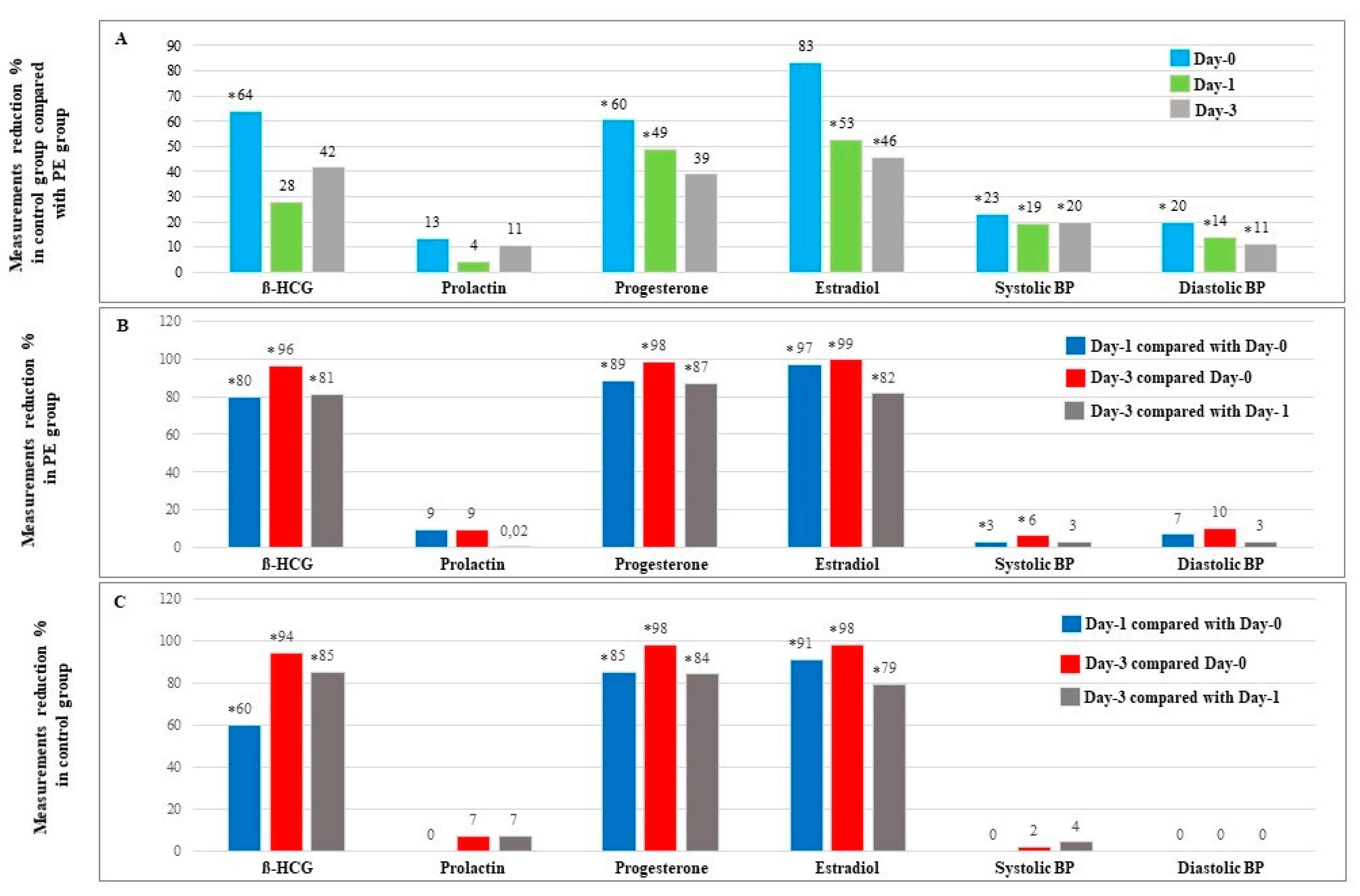
3.2. Postpartum Serum Hormone Levels and BP Measurements in Normal and PE Cases
3.3. Association between Serum Hormone Levels with PE and BP Measurements
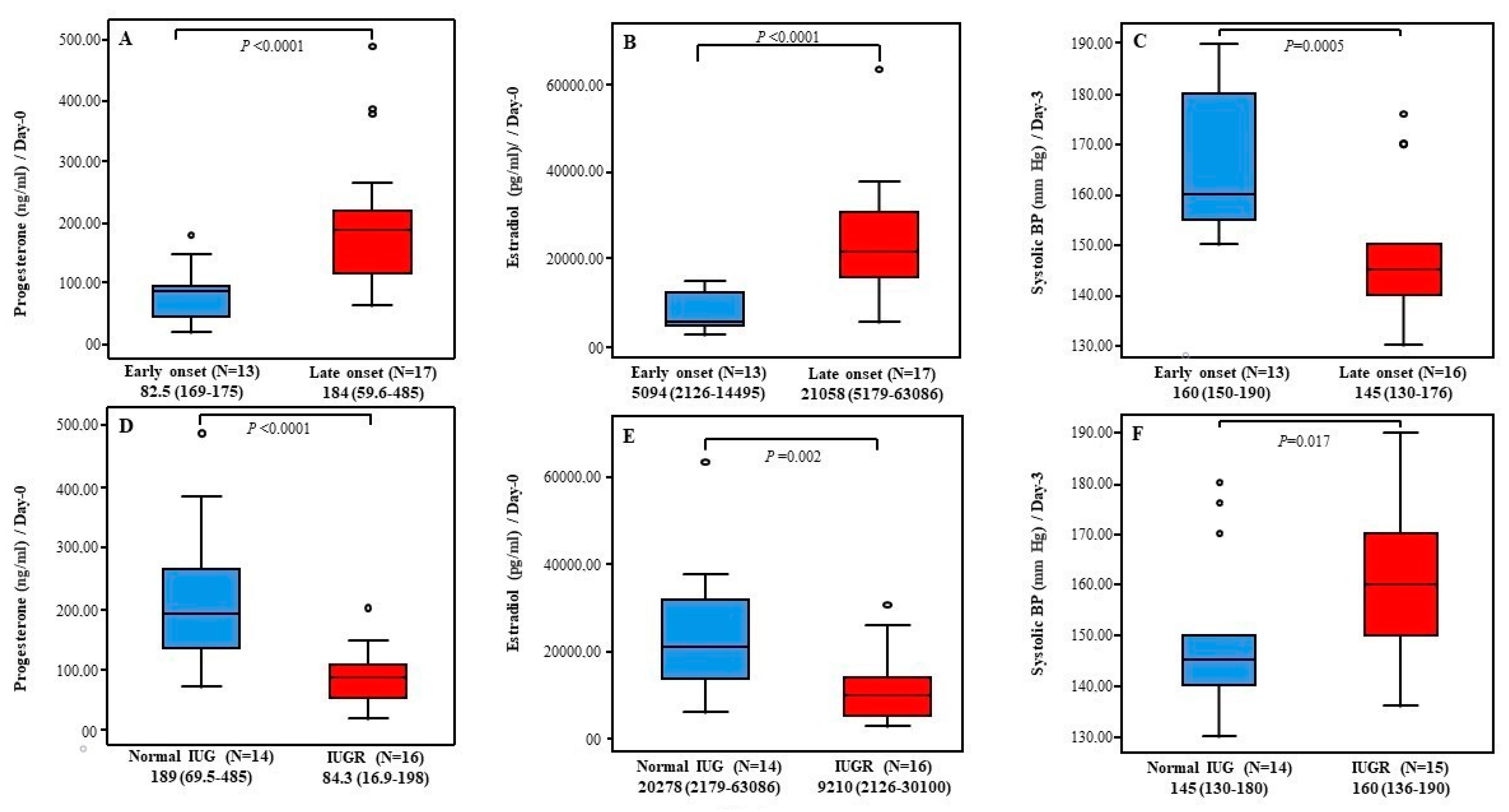
3.4. Relevant Diagnosis and Characteristics within the PE Group
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Stepan, H.; Kuse-Fohl, S.; Klockenbusch, W.; Rath, W.; Schauf, B.; Walther, T.; Schlembach, D. Diagnosis and Treatment of Hypertensive Pregnancy Disorders. Guideline of DGGG (S1-Level, AWMF Registry No. 015/018, December 2013). Geburtshilfe Frauenheilkunde 2015, 75, 900–914. [Google Scholar] [CrossRef] [Green Version]
- Peres, G.M.; Mariana, M.; Cairrão, E. Pre-Eclampsia and Eclampsia: An Update on the Pharmacological Treatment Applied in Portugal. J. Cardiovasc. Dev. Dis. 2018, 17, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmed, A.; Rezai, H.; Broadway-Stringer, S. Evidence-Based Revised View of the Pathophysiology of Preeclampsia. Adv. Exp. Med. Biol. 2017, 956, 355–374. [Google Scholar] [CrossRef] [PubMed]
- Phipps, E.; Prasanna, D.; Brima, W.; Jim, B. Preeclampsia: Updates in pathogenesis, definitions, and guidelines. Clin. J. Am. Soc. Nephrol. 2016, 11, 1102–1113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, P.; Haththotuwa, R.; Kwok, C.S.; Babu, A.; Kotronias, R.A.; Rushton, C.; Mamas, M.A. Preeclampsia and Future Cardiovascular Health: A Systematic Review and Meta-Analysis. Circ. Cardiovasc. Qual. Outcomes 2017, 10, 003497. [Google Scholar] [CrossRef] [PubMed]
- Napso, T.; Yong, H.E.; Lopez-Tello, J.; Sferruzzi-Perri, A.N. The Role of Placental Hormones in Mediating Maternal Adaptations to Support Pregnancy and Lactation. Front. Physiol. 2018, 17, 1091. [Google Scholar] [CrossRef]
- Maliqueo, M.; Echiburu, B.; Crisosto, N. Sex steroids modulate uterine-placental vasculature: Implications for obstetrics and neonatal outcomes. Front. Physiol. 2016, 7, 152. [Google Scholar] [CrossRef] [Green Version]
- Shen, Z.; Wu, Y.; Chen, X.; Chang, X.; Zhou, Q.; Zhou, J.; Wang, K. Decreased maternal serum 2-methoxyestradiol levels are associated with the development of preeclampsia. Cell Physiol. Biochem. 2014, 34, 2189–2199. [Google Scholar] [CrossRef]
- Lan, K.C.; Lai, Y.J.; Cheng, H.H.; Tsai, N.C.; Su, Y.T.; Tsai, C.C.; Hsu, T.Y. Levels of sex steroid hormones and their receptors in women with preeclampsia. Reprod. Biol. Endocrinol. 2020, 18, 12. [Google Scholar] [CrossRef] [Green Version]
- Babic, G.M.; Markovic, S.D.; Varjacic, M.; Djordjevic, N.Z.; Nikolic, T.; Stojic, I.; Jakovljevic, V. Estradiol decreases blood pressure in association with redox regulation in preeclampsia. Clin. Exp. Hypertens. 2018, 40, 281–286. [Google Scholar] [CrossRef]
- Djordjević, N.Z.; Babić, G.M.; Marković, S.D.; Ognjanović, B.I.; Štajn, A.Š.; Saičić, Z.S. The antioxidative effect of estradiol therapy on erythrocytes in women with preeclampsia. Reprod. Toxicol. 2010, 29, 231–236. [Google Scholar] [CrossRef] [PubMed]
- Kiprono, L.V.; Wallace, K.; Moseley, J.; Martin, J., Jr.; LaMarca, B. Progesterone blunts vascular endothelial cell secretion of endothelin-1 in response to placental ischemia. Am. J. Obstet. Gynecol. 2013, 209, 44.e1–44.e6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, G.; Xu, W.; Chen, Y.; Liu, X.; Xi, M. Abnormal apoptosis of trophoblastic cells is related to the up-regulation of CYP11A gene in placenta of preeclampsia patients. PLoS ONE 2013, 8, e59609. [Google Scholar] [CrossRef] [Green Version]
- Bernard, V.; Young, J.; Binart, N. Prolactin-a pleiotropic factor in health and disease. Nat. Rev. Endocrinol. 2019, 15, 356–365. [Google Scholar] [CrossRef]
- Maslar, I.A.; Ansbacher, R. Effects of progesterone on decidual prolactin production by organ cultures of human endometrium. Endocrinology 1986, 118, 2102–2108. [Google Scholar] [CrossRef] [PubMed]
- Toft, D.J.; Linzer, D.I. Prolactin (PRL)-Like Protein J, a Novel Member of the PRL/Growth Hormone Family, Is Exclusively Expressed in Maternal Decidua. Endocrinology 1999, 140, 5095–5101. [Google Scholar] [CrossRef] [PubMed]
- Freeman, M.E.; Kanyicska, B.; Lerant, A.; Nagy, G. Prolactin: Structure, function, and regulation of secretion. Physiol. Rev. 2000, 80, 1523–1631. [Google Scholar] [CrossRef]
- Ekinci, E.I.; Torkamani, N.; Ramchand, S.K.; Churilov, L.; Sikaris, K.A.; Lu, Z.X.; Houlihan, C.A. Higher maternal serum prolactin levels are associated with reduced glucose tolerance during pregnancy. J. Diabetes Investig. 2017, 8, 697–700. [Google Scholar] [CrossRef] [Green Version]
- Marlettini, M.G.; Cassani, A.; Morselli-Labate, A.M.; Crippa, S.; Contarini, A.; Miniero, R.; Orlandi, C. Maternal and fetal prolactin in pregnancy-induced hypertension. Arch. Gynecol. Obstet. 1990, 247, 73–81. [Google Scholar] [CrossRef]
- Chen, B.L.; Zhang, Z.H.; Liu, N.B.; Huang, K.S. Prolactin in normal pregnancy and severe pregnancy-induced hypertension. Hunan Yi Ke Da Xue Xue Bao 2001, 28, 67–69. [Google Scholar]
- Evans, J. Hyperglycosylated hCG: A Unique Human Implantation and Invasion Factor. Am. J. Reprod. Immunol. 2016, 75, 333–340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, H.Q.; Wang, Y.H.; Wang, L.L.; Hao, M. Predictive Value of Free β-Hcg Multiple of the Median for Women With Preeclampsia. Gynecol. Obstet. Investig. 2015, 81, 137–147. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Q.; Deng, Y.; Zhong, S.; Shi, Y. Human Chorionic Gonadotropin, Fetal Sex and Risk of Hypertensive Disorders of Pregnancy: A Nested Case-Control Study. Pregnancy Hypertens. 2016, 6, 17–21. [Google Scholar] [CrossRef] [PubMed]
- Long, W.; Zhou, Q.; Wang, H.; Lu, B.; Chen, Y.; Zhang, B.; Yu, B. Second-Trimester Maternal Serum Screening Biomarkers in the Risk Assessment for Preeclampsia. Ann. Clin. Lab. Sci. 2018, 48, 308–313. [Google Scholar]
- Poon, L.C.; Sahota, D. Screening and Prevention of Preeclampsia. Matern.-Fetal Med. 2019, 1, 25–30. [Google Scholar] [CrossRef]
- Hamza, A.; Gerlinger, C.; Radosa, J.; Solomayer, E.F.; Hagmann, J.; Sester, U.; Kasoha, M. Pilot study: Placental biomarker predictive capability (sFlt-1, PlGF and their ratio) of postpartum maternal outcome. Arch. Gynecol. Obstet. 2019, 299, 1557–1566. [Google Scholar] [CrossRef]
- Kasoha, M.; Takacs, Z.; Fackiner, L.; Gerlinger, C.; Sklavounos, P.; Radosa, J.; Hamza, A. Comparison of maternal serum levels and placental mRNA levels of dickkopf-1 in preeclamptic and normal pregnant women at delivery. Geburtshilfe Frauenheilkunde 2021, 81, 1247–1255. [Google Scholar] [CrossRef]
- Phipps, E.A.; Thadhani, R.; Benzing, T.; Karumanchi, S.A. Pre-eclampsia: Pathogenesis, novel diagnostics and therapies. Nat. Rev. Nephrol. 2019, 15, 275–289. [Google Scholar] [CrossRef]
- Austdal, M.; Tangerås, L.H.; Skråstad, R.B.; Salvesen, K.Å.; Austgulen, R.; Iversen, A.C.; Bathen, T.F. First Trimester Urine and Serum Metabolomics for Prediction of Preeclampsia and Gestational Hypertension: A Prospective Screening Study. Int. J. Mol. Sci. 2015, 16, 21520–21538. [Google Scholar] [CrossRef] [Green Version]
- Sibai, B.M. Diagnosis, controversies, and management of the syndrome of hemolysis, elevated liver enzymes, and low platelet count. Obs. Gynecol. 2004, 103, 981–991. [Google Scholar] [CrossRef] [Green Version]
- Berger, R.; Rath, W.; Abele, H.; Garnier, Y.; Kuon, R.J.; Maul, H. Reducing the Risk of Preterm Birth by Ambulatory Risk Factor Management. Dtsch. Arztebl. Int. 2019, 116, 858–864. [Google Scholar] [CrossRef] [PubMed]
- Tomimatsu, T.; Mimura, K.; Matsuzaki, S.; Endo, M.; Kumasawa, K.; Kimura, T. Preeclampsia: Maternal Systemic Vascular Disorder Caused by Generalized Endothelial Dysfunction Due to Placental Antiangiogenic Factors. Int. J. Mol. Sci. 2019, 20, 4246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Granger, J.P.; Alexander, B.T.; Bennett, W.A.; Khalil, R.A. Pathophysiology of pregnancy-induced hypertension. Am. J. Hypertens. 2001, 53, 178S–185S. [Google Scholar] [CrossRef]
- Sibai, B.M. Etiology and management of postpartum hypertension-preeclampsia. Am. J. Obs. Gynecol. 2012, 206, 470–475. [Google Scholar] [CrossRef] [PubMed]
- Brown, M.A.; Magee, L.A.; Kenny, L.C.; Karumanchi, S.A.; McCarthy, F.P.; Saito, S.; Ishaku, S. The hypertensive disorders of pregnancy: ISSHP classification, diagnosis & management recommendations for international practice. Pregnancy Hypertens. 2018, 13, 291–310. [Google Scholar] [CrossRef]
- Cantonwine, D.E.; McElrath, T.F.; Trabert, B.; Xu, X.; Sampson, J.; Roberts, J.M.; Troisi, R. Estrogen metabolism pathways in preeclampsia and normal pregnancy. Steroids 2019, 144, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Di Renzo, G.C.; Giardina, I.; Clerici, G.; Brillo, E.; Gerli, S. Progesterone in normal and pathological pregnancy. Horm. Mol. Biol. Clin. Investig. 2016, 27, 35–48. [Google Scholar] [CrossRef]
- Panwar, M.; Kumari, A.; Arora, R.; Singh, V.; Bansiwal, R. Raised neutrophil lymphocyte ratio and serum beta hCG level in early second trimester of pregnancy as predictors for development and severity of preeclampsia. Drug Discov. Ther. 2019, 13, 34–37. [Google Scholar] [CrossRef] [Green Version]
- Lenke LMartínez de la Escalera, G.; Clapp, C.; Bertsch, T.; Triebel, J.A. Dysregulation of the Prolactin/Vasoinhibin Axis Appears to Contribute to Preeclampsia. Front. Endocrinol 2020, 10, 893. [Google Scholar] [CrossRef]
- Chen, Y.; Xie, Z.; Wang, X.; Xiao, Q.; Lu, X.; Lu, S.; Lv, S. A risk model of prenatal screening markers in first trimester for predicting hypertensive disorders of pregnancy. EPMA J. 2020, 11, 343–353. [Google Scholar] [CrossRef]
- Shu, C.; Han, S.; Xu, P.; Wang, Y.; Cheng, T.; Hu, C.E. strogen and Preeclampsia: Potential of Estrogens as Therapeutic Agents in Preeclampsia. Drug Des. Devel. Ther. 2021, 15, 2543–2550. [Google Scholar] [CrossRef] [PubMed]
- Chang, A.S.; Grant, R.; Tomita, H.; Kim, H.S.; Smithies, O.; Kakoki, M. Prolactin alters blood pressure by modulating the activity of endothelial nitric oxide synthase. Proc. Natl. Acad. Sci. USA 2016, 113, 12538–12543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alawad, Z.M.; Al-Omary, H.L. Maternal and cord blood prolactin level and pregnancy complications. Pak. J. Med. Sci. 2019, 35, 1122–1127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leaños-Miranda, A.; Campos-Galicia, I.; Ramírez-Valenzuela, K.L.; Chinolla-Arellano, Z.L.; Isordia-Salas, I. Circulating angiogenic factors and urinary prolactin as predictors of adverse outcomes in women with preeclampsia. Hypertension 2013, 61, 1118–1125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mendelson, C.R. Minireview: Fetal-maternal hormonal signaling in pregnancy and labor. Mol. Endocrinol. 2009, 23, 947–954. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
{kind=link}
| Characteristic | Control Cases (N = 20) | PE Cases (N = 30) | p |
|---|---|---|---|
| * Age (Years) | 31 ± 7 | 32 ± 5 | NS |
| * BMI (Kg/m2) | 32.3 ± 5.7 | 36.9 ± 8.7 | 0.030 |
| ⁑ Gestation age at the time of delivery (Weak) | 38.7 (34.3–41.9) | 34.4 (26.6–40.1) | <0.0001 |
| * Creatinin (mg/dL) | 0.6 ± 0.12 | 0.7 ± 0.16 | <0.0001 |
| ⁑ Alanine aminotransferase (ALT) (U/L) | 11.50 (8–28) φ | 20.5 (8–392) | 0.003 |
| ⁑ Aspartate aminotransferase (AST) (U/L) | 20 (15–34) φ | 31.5 (7–242) | 0.018 |
| ⁋ Gravida [N (%)] | |||
| One Gravida ≥2 Gravida | 3 (15) 17 (75) | 31 (70) 9 (30) | <0.0001 |
| ⁋ Para [N (%)] | |||
| 0 Para ≥1 Para | 5 (25) 15 (75) | 25 (83) 6 (17) | <0.0001 |
| ⁋,‽ Symptoms [N (%)] | |||
| No Yes | 20 (100) 0 (0) | 24 (80) 6 (20) | NS |
| Parameter | Control Cases (N = 20) | PE Cases ℷ | p |
|---|---|---|---|
| Systolic blood pressure (mm Hg) | |||
| Day-0 | 123 (105–170) | 160 (130–200) | <0.0001 |
| Day-1 | 125 (100–145) | 157 (130–194) | <0.0001 |
| Day-3 | 120 (80–150) | 150 (130–190) | <0.0001 |
| Φ p | NS * | Day-1 vs. Day-0: 0.032 Day-3 vs. Day-0: 0.029 Day-3 vs. Day-1: NS | |
| Diastolic blood pressure (mm Hg) | |||
| Day-0 | 80 (60–90) | 100 (60–140) | <0.0001 |
| Day-1 | 80 (50–90) | 92 (70–120) | <0.0001 |
| Day-3 | 80 (65–90) | 90 (70–110) | <0.0001 |
| Φ p | NS * | NS * | |
| ß-HCG (mIU/mL) | |||
| Day-0 | 8357 (1786–95,328) | 26,623 (2675–172,281) | 0.005 |
| Day-1 | 3379 (948–17,942) | 4685 (487–43,860) | NS |
| Day-3 | 519 (6–2103) | 916 (138–6975) | NS |
| Φ p | <0.0001 * | <0.0001 * | |
| Prolactin (µIU/mL) | |||
| Day-0 | 5682 (1868–9277) | 6327 (2489–17,660) | NS |
| Day-1 | 5687 (369–14,576) | 5766 (314–10,661) | NS |
| Day-3 | 5310 (193–11,383) | 5570 (149–12,275) | NS |
| Φ p | NS | NS | |
| Progesterone (ng/mL) | |||
| Day-0 | 55.8 (8.16–250) | 115.5 (16.9–485) | 0.046 |
| Day-1 | 8.3 (3.1–24.3) | 14.8 (3.8–103) | 0.002 |
| Day-3 | 1.3 (0.2–3.7) | 1.8 (0.8–11.7) | NS |
| Φ p | <0.0001 * | <0.0001 * | |
| Estradiol (pg/mL) | |||
| Day-0 | 2544 (215–55,080) | 12,675 (2126–63,086) | NS |
| Day-1 | 227 (75–817) | 425 (85–10,665) | 0.020 |
| Day-3 | 48 (12–278) | 89 (12–681) | 0.008 |
| Φ p | <0.0001 * | <0.0001 * |
| Predictor Variable * | B | p | Exp(B) | 95% CI for Exp(B) | |
|---|---|---|---|---|---|
| Lower | Upper | ||||
| BMI Δ | 0.085 | 0.053 | 1.089 | 0.999 | 1.188 |
| Gestation age (Week) | -0.324 | 0.004 | 0.723 | 0.581 | 0.900 |
| Creatinin (mg/dL) | 8.895 | 0.002 | 7294.2 | 25.7 | 20,741,143.8 |
| ALT (U/L) | 0.117 | 0.038 | 1.124 | 1.006 | 1.256 |
| AST (U/L) | 0.067 | 0.081 | 1.069 | 0.992 | 1.153 |
| ß-HCG-Day-0 (mIU/mL) | 0.031 | 0.030 | 1.03 | 1.003 | 1.061 |
| Progesterone-Day-0 (ng/mL) | 0.007 | 0.074 | 1.007 | 0.999 | 1.014 |
| Progesterone-Day-1 (ng/mL) | 0.145 | 0.018 | 1.156 | 1.025 | 1.304 |
| Estradiol-Day-1 (pg/mL) | 0.246 | 0.061 | 1.278 | 0.989 | 1.635 |
| Estradiol-Day-3 (pg/mL) | 0.100 | 0.109 | 1.100 | 0.978 | 1.250 |
| Systolic BP Measurements (mm Hg) | Diastolic BP Measurements (mm Hg) | |||||
|---|---|---|---|---|---|---|
| Predictor Variable | Day-0 | Day-1 | Day-3 | Day-0 | Day-1 | Day-3 |
| PE diagnosis | ||||||
| P | <0.0001 | <0.0001 | <0.0001 | <0.0001 | <0.0001 | <0.0001 |
| β | 37.800 | 29.7 | 36.4 | 21.8 | 13.4 | 13.6 |
| BMI | ||||||
| P | 0.017 | NS | NS | 0.017 | NS | NS |
| β | 1.071 | --- | --- | 0.710 | --- | --- |
| Gestation age (Weeks) | ||||||
| P | <0.0001 | <0.0001 | <0.0001 | 0.005 | 0.024 | 0.002 |
| β | −2.471 | −2.467 | −2.841 | −1.475 | −0.966 | −1.060 |
| Creatinin (mg/dL) | ||||||
| P | 0.001 | 0.003 | 0.003 | 0.003 | 0.018 | NS |
| β | 66.9 | 53.2 | 61.2 | 41.6 | 27.3 | 17.1 |
| ALT (U/L) | ||||||
| P | 0.023 | NS | 0.040 | NS | NS | NS |
| β | 0.134 | --- | 0.122 | --- | --- | --- |
| AST (U/L) | ||||||
| P | NS | NS | 0.042 | NS | NS | NS |
| β | --- | --- | 0.192 | --- | --- | --- |
| ß-HCG (mIU/mL) * | ||||||
| Day-0 P | NS | NS | 0.013 | 0.028 | NS | NS |
| β | --- | --- | 4.928 | 0.136 | --- | --- |
| Day-1 P | NT | NS | 0.004 | NT | NS | NS |
| β | --- | --- | 4.846 | --- | --- | --- |
| Day-3 P | NT | NT | 0.014 | NT | NT | NS |
| β | --- | --- | 4.769 | --- | --- | --- |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kasoha, M.; Takacs, Z.; Dumé, J.; Findeklee, S.; Gerlinger, C.; Sima, R.-M.; Ples, L.; Solomayer, E.-F.; Haj Hamoud, B. Postpartum Assessment of the Correlation between Serum Hormone Levels of Estradiol, Progesterone, Prolactin and ß-HCG and Blood Pressure Measurements in Pre-Eclampsia Patients. Diagnostics 2022, 12, 1700. https://doi.org/10.3390/diagnostics12071700
Kasoha M, Takacs Z, Dumé J, Findeklee S, Gerlinger C, Sima R-M, Ples L, Solomayer E-F, Haj Hamoud B. Postpartum Assessment of the Correlation between Serum Hormone Levels of Estradiol, Progesterone, Prolactin and ß-HCG and Blood Pressure Measurements in Pre-Eclampsia Patients. Diagnostics. 2022; 12(7):1700. https://doi.org/10.3390/diagnostics12071700
Chicago/Turabian StyleKasoha, Mariz, Zoltan Takacs, Jacob Dumé, Sebastian Findeklee, Christoph Gerlinger, Romina-Marina Sima, Liana Ples, Erich-Franz Solomayer, and Bashar Haj Hamoud. 2022. "Postpartum Assessment of the Correlation between Serum Hormone Levels of Estradiol, Progesterone, Prolactin and ß-HCG and Blood Pressure Measurements in Pre-Eclampsia Patients" Diagnostics 12, no. 7: 1700. https://doi.org/10.3390/diagnostics12071700
APA StyleKasoha, M., Takacs, Z., Dumé, J., Findeklee, S., Gerlinger, C., Sima, R.-M., Ples, L., Solomayer, E.-F., & Haj Hamoud, B. (2022). Postpartum Assessment of the Correlation between Serum Hormone Levels of Estradiol, Progesterone, Prolactin and ß-HCG and Blood Pressure Measurements in Pre-Eclampsia Patients. Diagnostics, 12(7), 1700. https://doi.org/10.3390/diagnostics12071700