
Perls’ Stain Guidelines from the French-Speaking Cellular Hematology Group (GFHC)

 , , and add
Show full author list
, , and add
Show full author list
Abstract
1. Introduction
2. Methods
3. Guidelines
3.1. Indications
3.2. Procedure
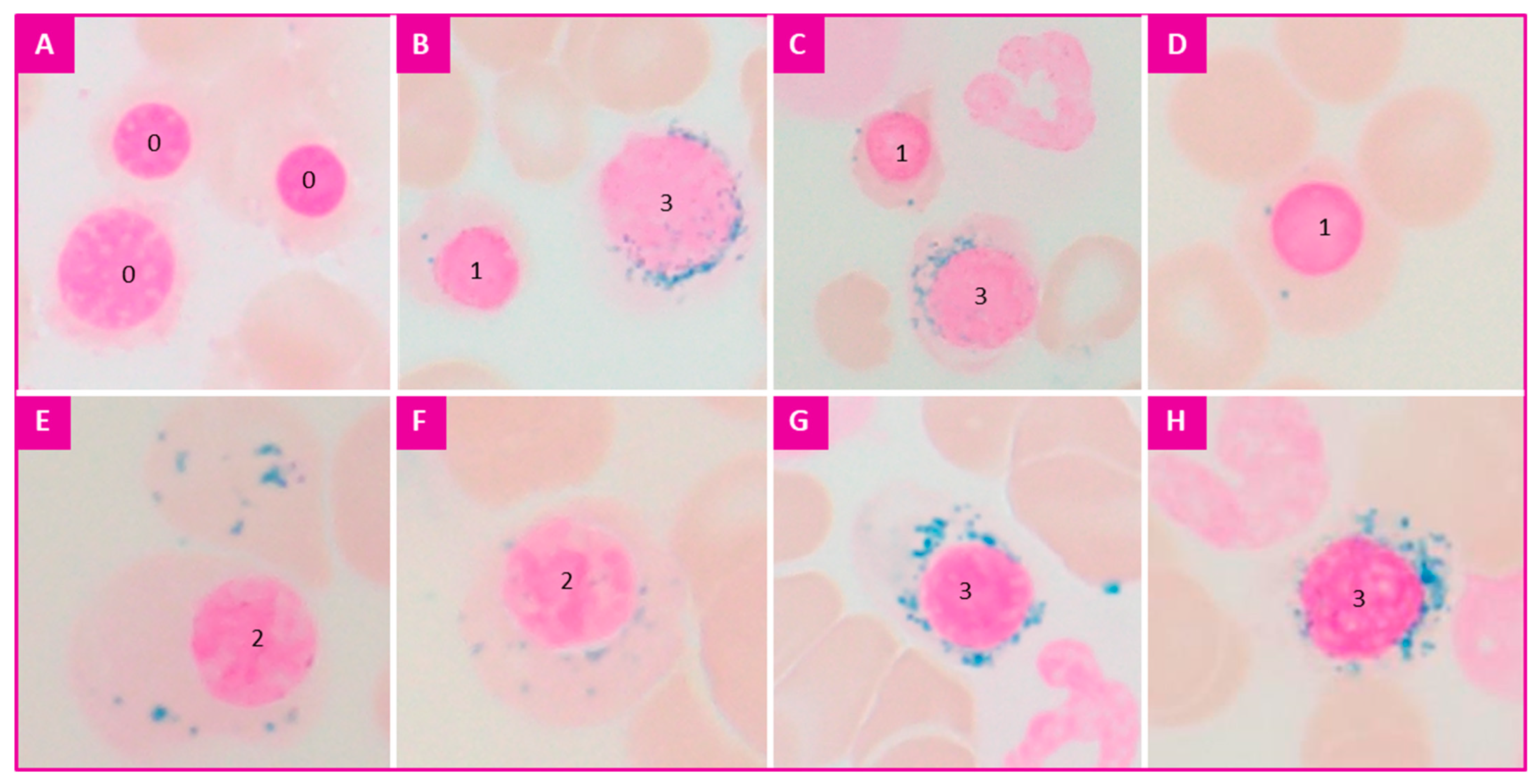
3.3. Interpretation
- -
- Type 0: no visible granules;
- -
- Type 1: less than five granules in the cytoplasm;
- -
- Type 2: five or more granules but not peri-nuclear;
- -
- Ring sideroblasts (or type 3): five or more granules in a peri-nuclear position, encircling one-third or more of the circumference of the nucleus.
- Siderocytes are normally absent;
- In the case of sideroblastic anemia, several sideroblasts can be observed per field (obvious, and most often at least five per field at ×100 magnification);
- In the absence of iron deficiency, a few iron-containing macrophages are always observed (at least one macrophage out of five is stained);
- Reference values have been proposed for sideroblasts:
- -
- type 0: 60–90%,
- -
- type 1: 10–40%,
- -
- type 2: <1% (a count of less than one type 2 sideroblast among 100 erythroblasts is considered insignificant).
- -
- type 3: <1% (a count of less than one ring sideroblast among 100 erythroblasts is considered insignificant).
- -
- Absence of pathological sideroblastosis;
- -
- Numerous sideroblasts with some ring sideroblasts between 5 and 14%. To be completed by a SF3B1 gene mutation research;
- -
- Presence of pathological sideroblasts, with ring sideroblasts ≥ 15%. In favor of MDS with ring sideroblasts (in the absence of excess blasts and Auer rods, and diagnostic criteria for myelodysplastic/myeloproliferative neoplasm with ring sideroblasts and thrombocytosis).
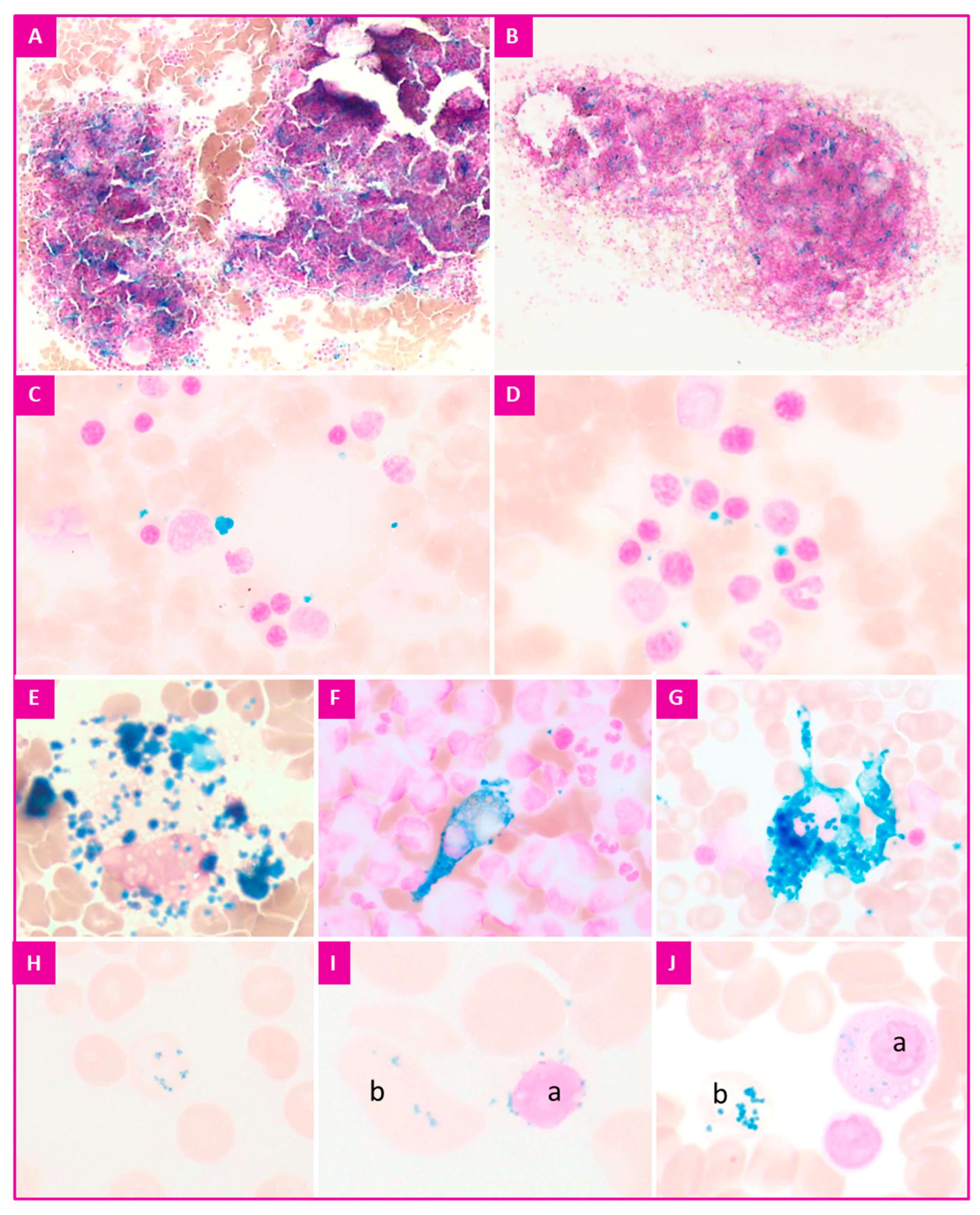
- The macrophagic iron content;
- The presence of red blood cells containing precipitates of iron complexed with proteins (Pappenheimer bodies in MGG staining, siderocytes in Perls’ stain);
- The presence or absence of extracellular iron [9].
- -
- Overall iron content of macrophages and iron distribution in erythroblasts are normal. In favor of undisturbed iron utilization in erythroblasts for hemoglobin synthesis;
- -
- Decreased overall iron content of macrophages. Normal/decreased sideroblastosis. In favor of a deficit of iron in erythroblasts for hemoglobin synthesis. To be explored;
- -
- Increased global iron content of macrophages. Sideroblastosis in the levels normally observed. In favor of an inflammatory process, the cause of the inflammation should be investigated.
- -
- Benzene, chemotherapy (Melphalan), antibiotics (Chloramphenicol, Linezolid), anti-tuberculosis drugs (Isoniazid, Pyrazinamide, Cycloserine);
- -
- Thalassemias, inflammatory syndromes, copper deficiency (possibly secondary to excessive ingestion of zinc), liver diseases (Wilson’s Disease), chronic alcoholism, lead poisoning, arsenic poisoning, severe undernutrition, deficiency of vitamins B1, B6, B9, B12, poly-transfusion, thiamine-sensitive megaloblastic anemias with mutation of the SLC19 gene, Wolfram syndrome (DIDMOAD: ‘diabetes insipidus, diabetes mellitus, optic atrophy and deafness’);
- -
- Constitutional sideroblastic anemias, mitochondrial cytopathies (Pearson syndrome).
3.4. Reporting Arrangements
3.5. Conservation
3.6. Quality Controls
4. Technical Protocol
- -
- Non-specific laboratory equipment: glass dishes, test tubes, pipettes, staining trays, smear racks, timer;
- -
- Adjustable water bath at 50 °C.
- -
- Hydrochloric acid 1 N stored at room temperature (secure cabinet);
- -
- Hematoxylin of Harris, of Mayer or Nuclear test Red;
- -
- Absolute methanol stored at room temperature (secure cabinet);
- -
- Potassium ferrocyanide (potassium hexacyanoferrate or ferrocyanide trihydrate) stored at room temperature (secure cabinet);
- -
- Aluminum sulfate 98% (optionally);
- -
- Nuclear red or safranin (optionally).
- -
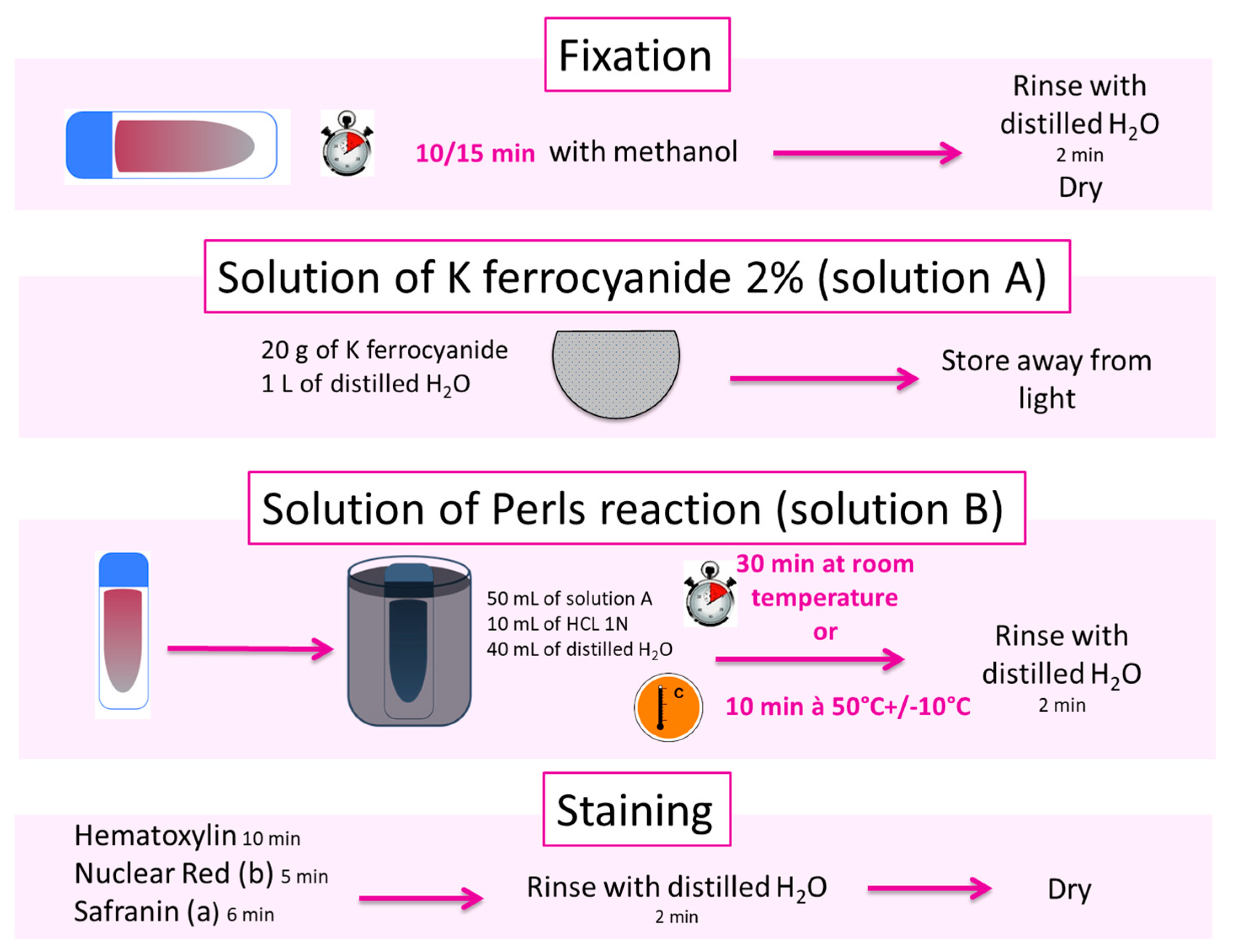
- Fix patient’s BM or blood smears and the control smear for 10 min by covering them with methanol;
- -
- Rinse with distilled water and then dry;
- -
- Put the smears in a tank equipped with a smear holder;
- -
- Put solution B in the tank containing the smears and place it in a water bath at 50 °C for 10 min;
- -
- Rinse with distilled water and then dry;
- -
- Counterstain by covering with hematoxylin for 10 min or with nuclear red for 5 min or with safranin (6 min);
- -
- Rinse with distilled water and then dry.
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Swerdlow, S.H.; Campo, E. WHO Classification of Tumors of Haematopoietic and Lymphoid Tissues, IARC revised 4th ed.; IARC: Lyon, France, 2017. [Google Scholar]
- Bain, B.J.; Bates, I. Dacie and Lewis Practical Haematology, 12th ed.; Elsevier: London, UK, 2017. [Google Scholar]
- Patnaik, M.M.; Tefferi, A. Myelodysplastic syndromes with ring sideroblasts (MDS-RS) and MDS/myeloproliferative neoplasm with RS and thrombocytosis (MDS/MPN-RS-T)—«2021 update on diagnosis, risk-stratification, and management». Am. J. Hematol. 2021, 96, 379–394. [Google Scholar] [CrossRef] [PubMed]
- Malcovati, L.; Hellström-Lindberg, E. Diagnosis and treatment of primary myelodysplastic syndromes in adults: Recommendations from the European LeukemiaNet. Blood 2013, 122, 2943–2964. [Google Scholar] [CrossRef] [PubMed]
- Guillosson, J.J.; Nafziger, J. Fiche technique: Recherche des sidéroblastes et sidérocytes dans la moelle osseuse par la réaction de Perls. Feuill. de Biol. Clin. 1987, 28, 41–42. [Google Scholar]
- Lesesve, J.F.; Chatelain, B. Myélogramme: Recommandations du GFHC. Feuill. Biol. 2018, 342, 17–32. [Google Scholar]
- Lesesve, J.F.; Clerc-Urmes, I. Évaluation de l’intervalle de confiance des pourcentages seuils (1%, 5%, 10%, 20%) utilisés pour la définition des hémopathies. Feuill. de Biol. 2018, 342, 41–46. [Google Scholar]
- Mufti, G.J.; Bennett, J.M. Diagnosis and Classification of Myelodysplastic Syndrome: International Working Group on Morphology of Myelodysplastic Syndrome (IWGM-MDS) Consensus Proposals for the Definition and Enumeration of Myeloblasts and Ring Sideroblasts. Haematologica 2008, 93, 1712–1717. [Google Scholar] [CrossRef] [PubMed]
- Sollis, M.; Perrin, J. RBCs inclusions after splenectomy: Not only Howell-Jolly bodies! Ann. Biol. Clin. 2013, 71, 185–189. [Google Scholar] [CrossRef] [PubMed]
- Rault, E.; Fenneteau, O. Présence de sidéroblastes en couronne en dehors du contexte de syndrome myélodysplasique: Que faut-il évoquer? Rev. de Biol. Médicale 2020, 352, 31–36. [Google Scholar]
- Bain, B.J. Hemosiderin-containing plasma cells. Am. J. Hematol. 2012, 87, 815. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | MDS-RS | MDS/MPN-RS-T |
|---|---|---|
| Blood and bone marrow findings | Presence of cytopenia, morphological dysplasia and BM RS ≥ 15%, or RS ≥ 5% in the presence of SF3B1 mutations.Can have single lineage or multi-lineage dysplasia (MDS-RS-SLD and MDS-RS-MLD). <1% PB blasts, <5% BM blasts and no Auer rods. | Anemia with erythroid lineage dysplasia, with or without multi-lineage dysplasia, ≥15%BM RS. <1% PB Blasts, <5% BM blasts and no Auer rods. Megakaryocytic hyperplasia with morphological features similar to those seen in BCR-ABL1 negative MPN. |
| Platelet counts | Normal to decreased | Persistent thrombocytosis ≥ 450 G/L |
| BM RS (%) | BM RS ≥ 15% or BM RS≥5% in the presence of SF3B1 mutations. | BM RS ≥ 15% regardless of the presence or absence of SF3B1 mutations. |
| Cytogenetic/Molecular categories that exclude a diagnosis | Del(5q)-MDS | BCR-ABL1 PDGFRA, PDGFRB, FGFR1 PCM1-JAK2 Del(5q) t(3;3)(q21;q26), inv(3)(q21;q26) |
| Frequency of cytogenetic abnormalities | 20% MDS-RS-SLD 50% MDS-RS-MLD | 20% |
| Molecular signature | SF3B1—80% TET2—30% DNMT3A—20% ASXL1—15% RUNX1—10% TP53—5% | SF3B1—80% JAK2 V617F—50% TET2—20% DNMT3A—15% ASXL—15% SETBP1—10% MPL—5% SH2B3—5% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lours, C.; Cottin, L.; Wiber, M.; Andrieu, V.; Baccini, V.; Baseggio, L.; Brouzes, C.; Chatelain, B.; Daliphard, S.; Fenneteau, O.; et al. Perls’ Stain Guidelines from the French-Speaking Cellular Hematology Group (GFHC). Diagnostics 2022, 12, 1698. https://doi.org/10.3390/diagnostics12071698
Lours C, Cottin L, Wiber M, Andrieu V, Baccini V, Baseggio L, Brouzes C, Chatelain B, Daliphard S, Fenneteau O, et al. Perls’ Stain Guidelines from the French-Speaking Cellular Hematology Group (GFHC). Diagnostics. 2022; 12(7):1698. https://doi.org/10.3390/diagnostics12071698
Chicago/Turabian StyleLours, Camille, Laurane Cottin, Margaux Wiber, Valérie Andrieu, Véronique Baccini, Lucile Baseggio, Chantal Brouzes, Bernard Chatelain, Sylvie Daliphard, Odile Fenneteau, and et al. 2022. "Perls’ Stain Guidelines from the French-Speaking Cellular Hematology Group (GFHC)" Diagnostics 12, no. 7: 1698. https://doi.org/10.3390/diagnostics12071698
APA StyleLours, C., Cottin, L., Wiber, M., Andrieu, V., Baccini, V., Baseggio, L., Brouzes, C., Chatelain, B., Daliphard, S., Fenneteau, O., Geneviève, F., Girard, S., Leymarie, V., Maloum, K., Rieu, J.-B., Sebahoun, G., Sudaka, I., Troussard, X., Wagner-Ballon, O., ... Lesesve, J.-F. (2022). Perls’ Stain Guidelines from the French-Speaking Cellular Hematology Group (GFHC). Diagnostics, 12(7), 1698. https://doi.org/10.3390/diagnostics12071698