
Development of a Deep Learning Model for Malignant Small Bowel Tumors Survival: A SEER-Based Study

 , ,
, , 
Abstract
:1. Background
2. Materials and Methods
2.1. Cohorts Dataset
2.2. Data Preprocessing
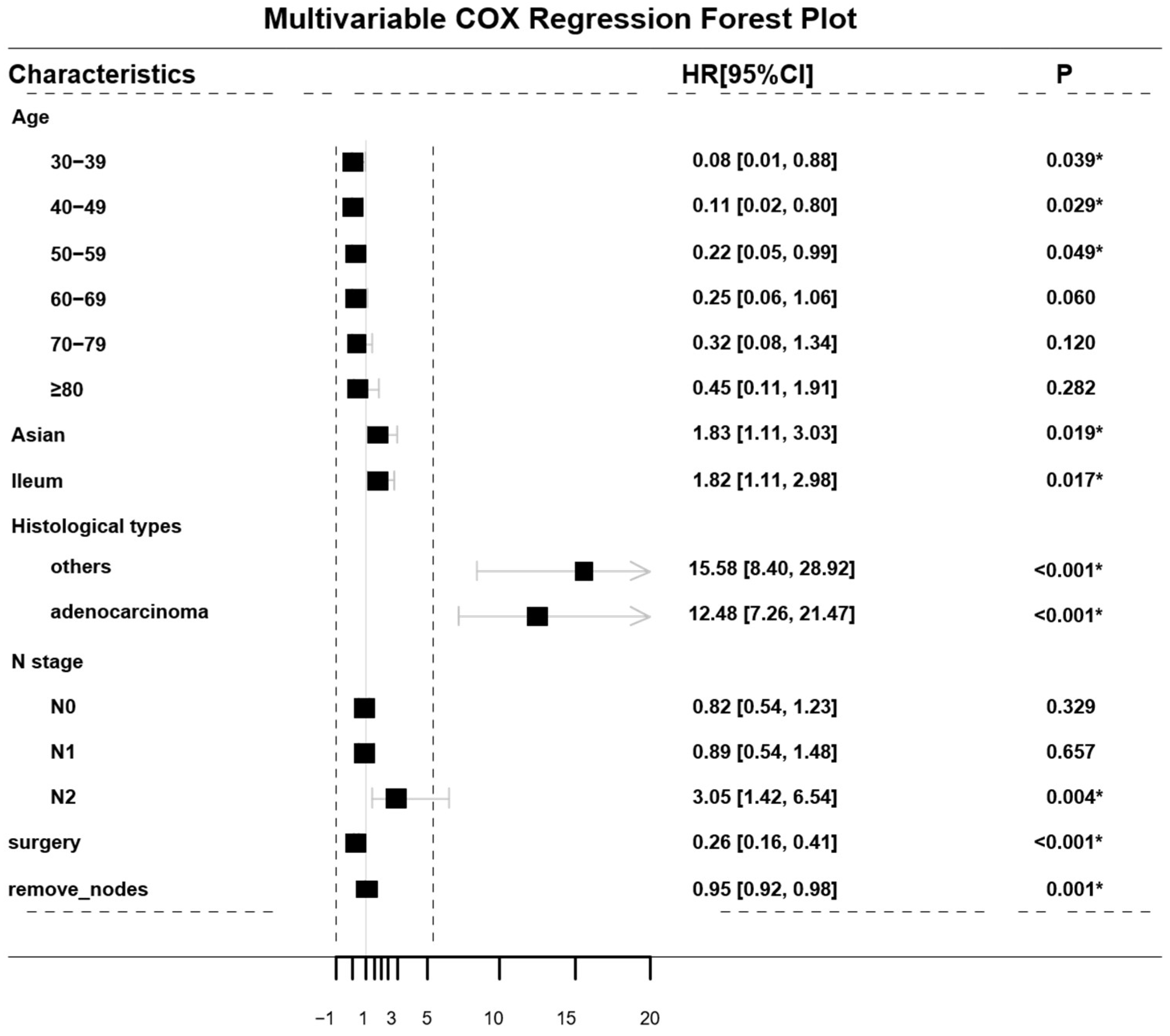
2.3. Development of the Cox-PH Model
2.4. Development of the DeepSurv Model
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
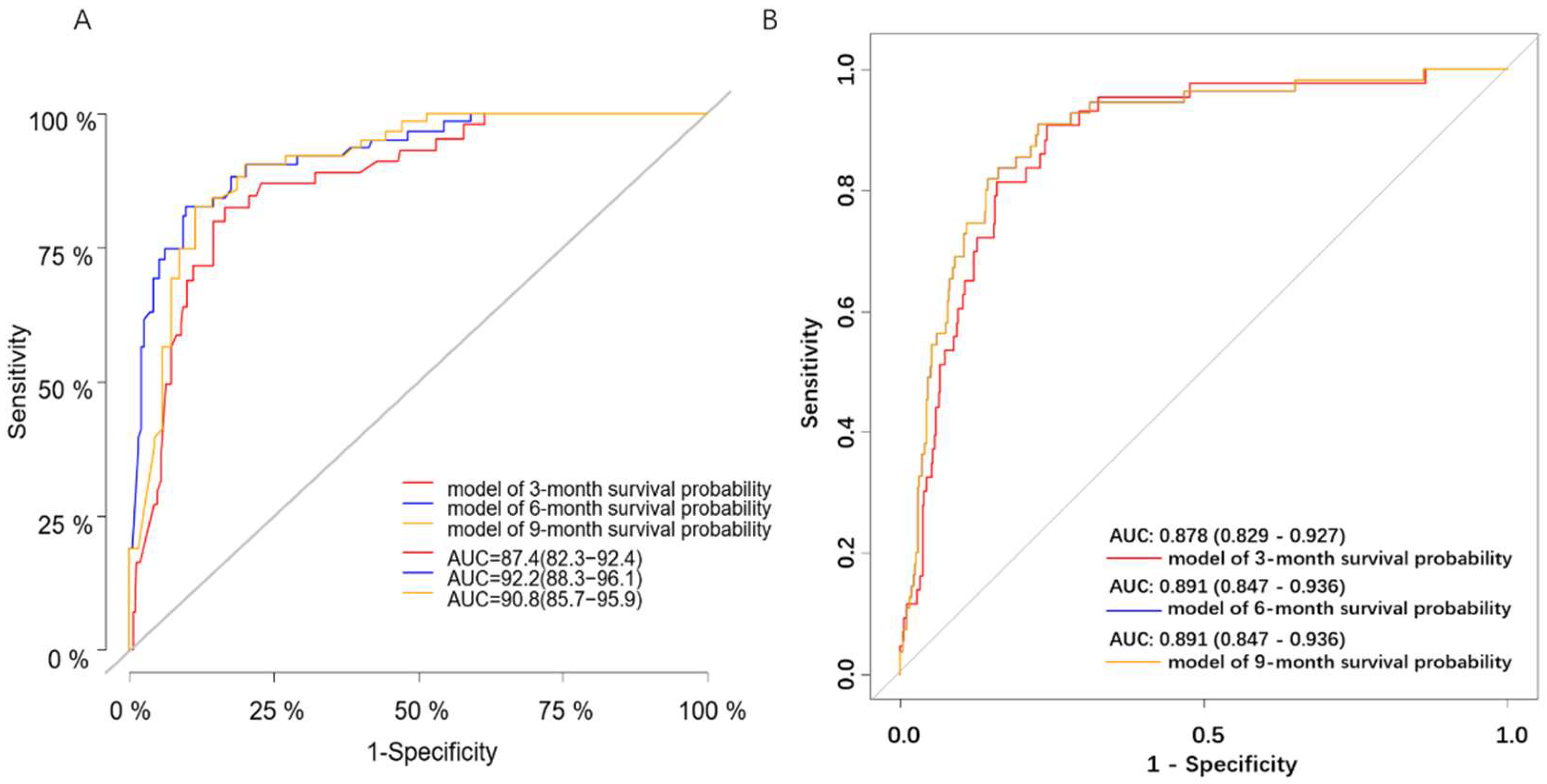
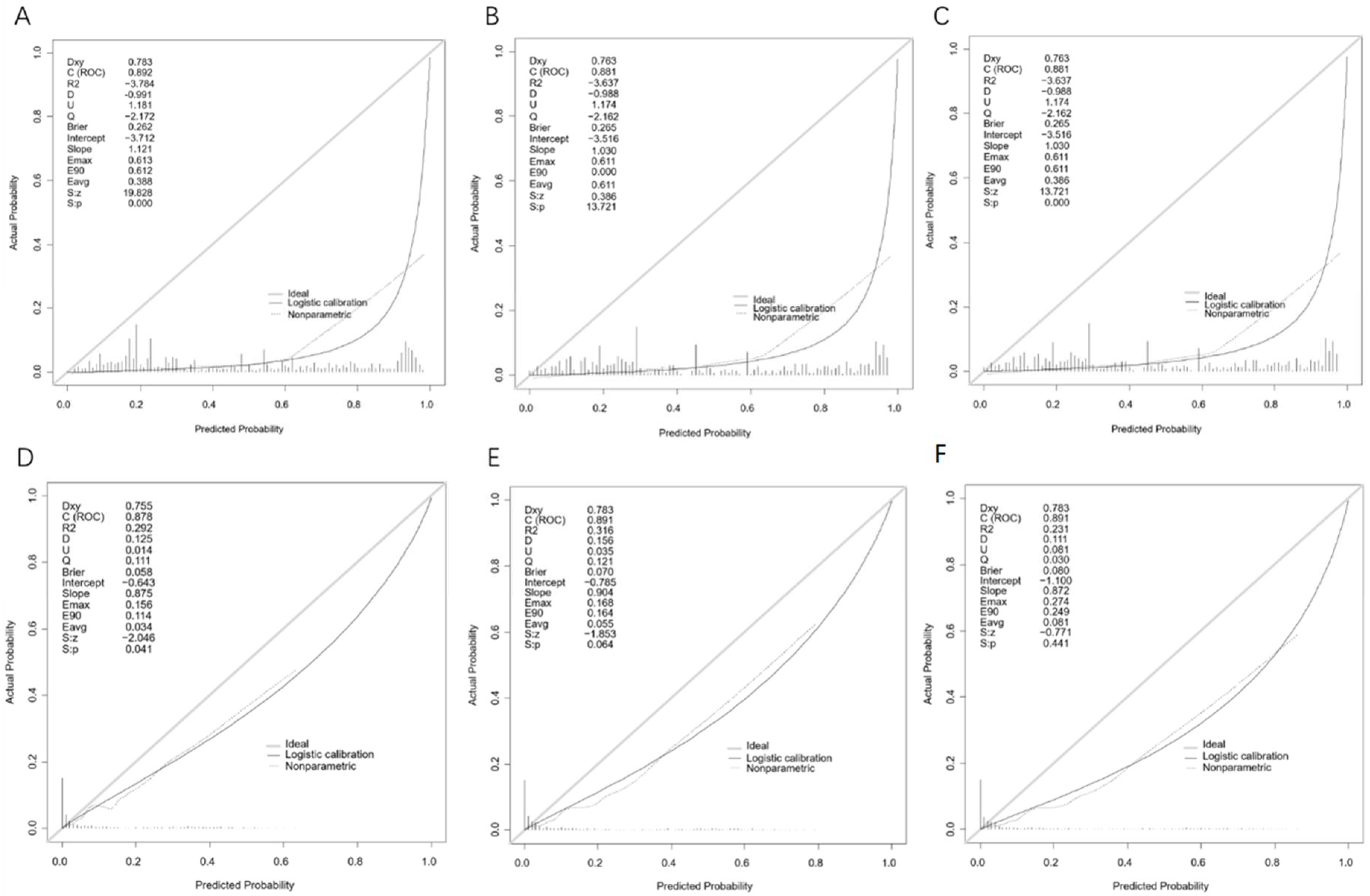
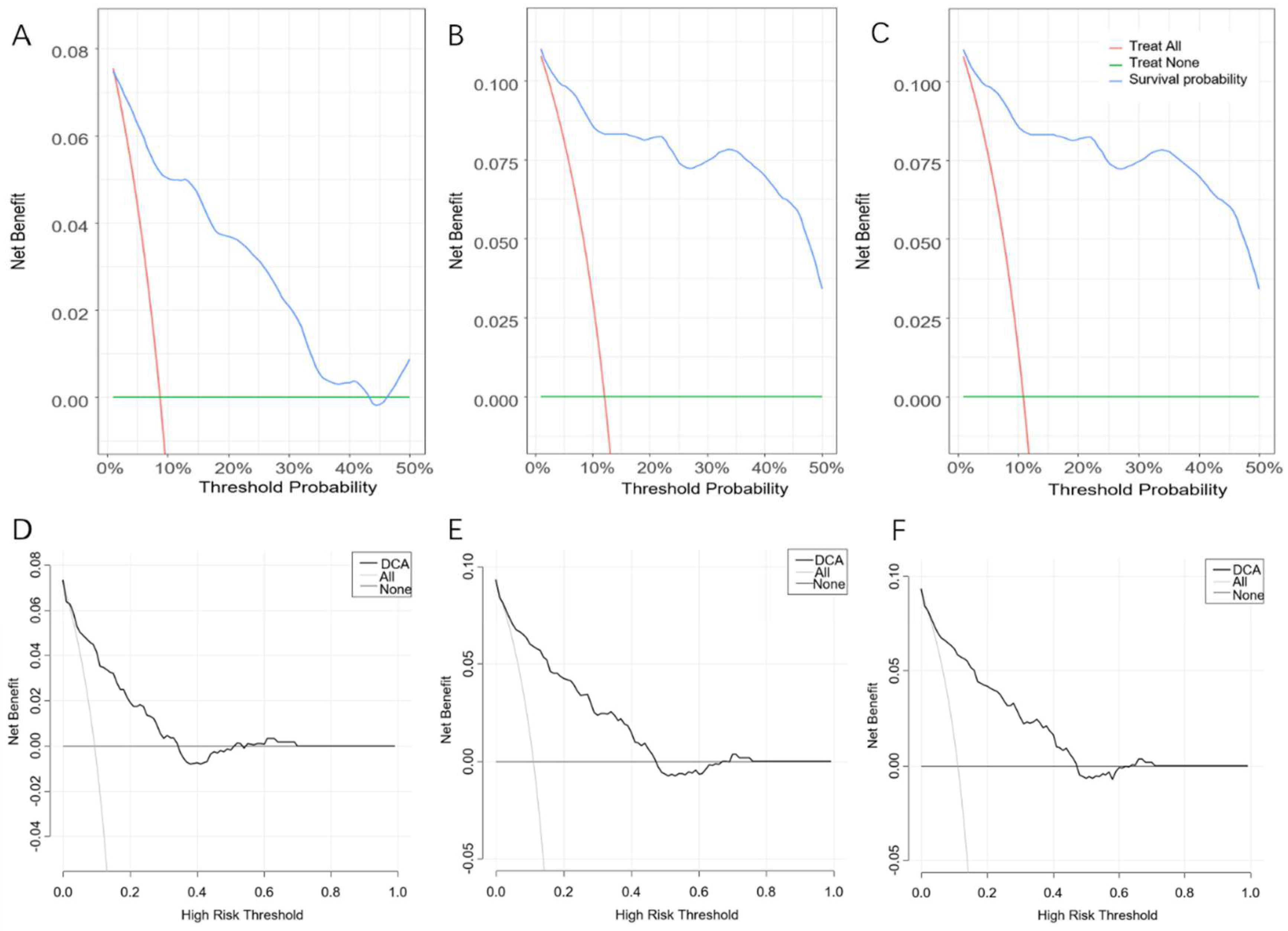
3.2. Performance of the Cox-PH Model
3.3. Performance of the DeepSurv Model
3.4. K–M Survival Analysis Based on the COX-PH Model
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Benson, A.B.; Venook, A.P.; Al-Hawary, M.M.; Arain, M.A.; Chen, Y.J.; Ciombor, K.K.; Cohen, S.A.; Cooper, H.S.; Deming, D.A.; Garrido-Laguna, I.; et al. Small Bowel Adenocarcinoma, Version 1.2020, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2019, 17, 1109–1133. [Google Scholar] [CrossRef] [PubMed]
- Kang, B.; Zhang, Q.; Shang, D.; Ni, Q.; Muhammad, F.; Hou, L.; Cui, W. Resolution of intussusception after spontaneous expulsion of an ileal lipoma per rectum: A case report and literature review. World J. Surg. Oncol. 2014, 12, 143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, N.; Yang, J.; Lyu, J.; Liu, Q.; He, H.; Liu, J.; Li, L.; Ren, X.; Li, Z. A convenient clinical nomogram for predicting the cancer-specific survival of individual patients with small-intestine adenocarcinoma. BMC Cancer 2020, 20, 505. [Google Scholar] [CrossRef]
- Min, M.; Noujaim, M.G.; Green, J.; Schlieve, C.R.; Vaze, A.; Cahan, M.A.; Cave, D.R. Role of Mucosal Protrusion Angle in Discriminating between True and False Masses of the Small Bowel on Video Capsule Endoscopy. J. Clin. Med. 2019, 8, 418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skrede, O.-J.; De Raedt, S.; Kleppe, A.; Hveem, T.S.; Liestøl, K.; Maddison, J.; A Askautrud, H.; Pradhan, M.; Nesheim, J.A.; Albregtsen, F.; et al. Deep learning for prediction of colorectal cancer outcome: A discovery and validation study. Lancet 2020, 395, 350–360. [Google Scholar] [CrossRef]
- Foersch, S.; Eckstein, M.; Wagner, D.-C.; Gach, F.; Woerl, A.-C.; Geiger, J.; Glasner, C.; Schelbert, S.; Schulz, S.; Porubsky, S.; et al. Deep learning for diagnosis and survival prediction in soft tissue sarcoma. Ann. Oncol. 2021, 32, 1178–1187. [Google Scholar] [CrossRef]
- Adeoye, J.; Koohi-Moghadam, M.; Lo, A.W.I.; Tsang, R.K.-Y.; Chow, V.L.Y.; Zheng, L.-W.; Choi, S.-W.; Thomson, P.; Su, Y.-X. Deep Learning Predicts the Malignant-Transformation-Free Survival of Oral Potentially Malignant Disorders. Cancers 2021, 13, 6054. [Google Scholar] [CrossRef]
- Levi, R.; Carli, F.; Arévalo, A.R.; Altinel, Y.; Stein, D.J.; Naldini, M.M.; Grassi, F.; Zanoni, A.; Finkelstein, S.; Vieira, S.M.; et al. Artificial intelligence-based prediction of transfusion in the intensive care unit in patients with gastrointestinal bleeding. BMJ Health Care Inform. 2021, 28, e100245. [Google Scholar] [CrossRef]
- Huang, L.; Lu, X.; Huang, X.; Zou, X.; Wu, L.; Zhou, Z.; Wu, D.; Tang, D.; Chen, D.; Wan, X.; et al. Intelligent difficulty scoring and assistance system for endoscopic extraction of common bile duct stones based on deep learning: Multicenter study. Laryngo-Rhino-Otologie 2020, 53, 491–498. [Google Scholar] [CrossRef]
- Itoh, T.; Kawahira, H.; Nakashima, H.; Yata, N. Deep learning analyzes Helicobacter pylori infection by upper gastrointestinal endoscopy images. Endosc. Int. Open 2018, 6, E139–E144. [Google Scholar] [CrossRef] [Green Version]
- Hirasawa, T.; Aoyama, K.; Tanimoto, T.; Ishihara, S.; Shichijo, S.; Ozawa, T.; Ohnishi, T.; Fujishiro, M.; Matsuo, K.; Fujisaki, J.; et al. Application of artificial intelligence using a convolutional neural network for detecting gastric cancer in endoscopic images. Gastric Cancer 2018, 21, 653–660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chuang, W.-Y.; Chen, C.-C.; Yu, W.-H.; Yeh, C.-J.; Chang, S.-H.; Ueng, S.-H.; Wang, T.-H.; Hsueh, C.; Kuo, C.-F.; Yeh, C.-Y. Identification of nodal micrometastasis in colorectal cancer using deep learning on annotation-free whole-slide images. Mod. Pathol. 2021, 34, 1901–1911. [Google Scholar] [CrossRef] [PubMed]
- Katzman, J.L.; Shaham, U.; Cloninger, A.; Bates, J.; Jiang, T.; Kluger, Y. DeepSurv: Personalized treatment recommender system using a Cox proportional hazards deep neural network. BMC Med. Res. Methodol. 2018, 18, 24. [Google Scholar] [CrossRef]
- Kather, J.N.; Pearson, A.T.; Halama, N.; Jäger, D.; Krause, J.; Loosen, S.H.; Marx, A.; Boor, P.; Tacke, F.; Neumann, U.P.; et al. Deep learning can predict microsatellite instability directly from histology in gastrointestinal cancer. Nat. Med. 2019, 25, 1054–1056. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Liu, Y.; Zhang, W.; Hong, Y.; Meng, J.; Wang, J.; Zheng, S.; Xu, X. Deep learning for prediction of hepatocellular carcinoma recurrence after resection or liver transplantation: A discovery and validation study. Hepatol. Int. 2022, 1–13. [Google Scholar] [CrossRef]
- Hosny, A.; Parmar, C.; Coroller, T.P.; Grossmann, P.; Zeleznik, R.; Kumar, A.; Bussink, J.; Gillies, R.J.; Mak, R.H.; Aerts, H.J.W.L. Deep learning for lung cancer prognostication: A retrospective multi-cohort radiomics study. PLoS Med. 2018, 15, e1002711. [Google Scholar] [CrossRef] [Green Version]
- She, Y.; Jin, Z.; Wu, J.; Deng, J.; Zhang, L.; Su, H.; Jiang, G.; Liu, H.; Xie, D.; Cao, N.; et al. Development and Validation of a Deep Learning Model for Non–Small Cell Lung Cancer Survival. JAMA Netw. Open 2020, 3, e205842. [Google Scholar] [CrossRef] [PubMed]
- Howard, F.M.; Kochanny, S.; Koshy, M.; Spiotto, M.; Pearson, A.T. Machine Learning–Guided Adjuvant Treatment of Head and Neck Cancer. JAMA Netw. Open 2020, 3, e2025881. [Google Scholar] [CrossRef]
- Wang, L.; Laurentiev, J.; Yang, J.; Lo, Y.-C.; Amariglio, R.E.; Blacker, D.; Sperling, R.A.; Marshall, G.A.; Zhou, L. Development and Validation of a Deep Learning Model for Earlier Detection of Cognitive Decline From Clinical Notes in Electronic Health Records. JAMA Netw. Open 2021, 4, e2135174. [Google Scholar] [CrossRef]
- Wang, D.; Li, C.; Li, Y.; Liu, W.; Zhao, L.; Güngör, C.; Tan, F.; Zhou, Y. Specific survival nomograms based on SEER database for small intestine adenocarcinoma. Ann. Palliat. Med. 2021, 10, 7440–7457. [Google Scholar] [CrossRef]
- Zheng, Z.; Zhou, X.; Zhang, J.; Zhao, B.; Chen, C.; Liu, X.; Cao, H.; Li, T.; Geng, R.; Wang, W.; et al. Nomograms predict survival of patients with small bowel adenocarcinoma: A SEER-based study. Int. J. Clin. Oncol. 2020, 26, 387–398. [Google Scholar] [CrossRef]
- Jiang, S.; Zhao, L.; Xie, C.; Su, H.; Yan, Y. Prognostic Performance of Different Lymph Node Staging Systems in Patients with Small Bowel Neuroendocrine Tumors. Front. Endocrinol. 2020, 11, 402. [Google Scholar] [CrossRef] [PubMed]
- Dong, D.; Fang, M.-J.; Tang, L.; Shan, X.-H.; Gao, J.-B.; Giganti, F.; Wang, R.-P.; Chen, X.; Wang, X.-X.; Palumbo, D.; et al. Deep learning radiomic nomogram can predict the number of lymph node metastasis in locally advanced gastric cancer: An international multicenter study. Ann. Oncol. 2020, 31, 912–920. [Google Scholar] [CrossRef] [PubMed]
- Gu, Y.; Deng, H.; Wang, D.; Li, Y. Metastasis Pattern and Survival Analysis in Primary Small Bowel Adenocarcinoma: A SEER-Based Study. Front. Surg. 2021, 8, 759162. [Google Scholar] [CrossRef] [PubMed]
- Blazek, K.; van Zwieten, A.; Saglimbene, V.; Teixeira-Pinto, A. A practical guide to multiple imputation of missing data in nephrology. Kidney Int. 2020, 99, 68–74. [Google Scholar] [CrossRef]
- Xie, J.-B.; Pang, Y.-S.; Li, X.; Wu, X.-T. Role of Removed Lymph Nodes on the Prognosis of M0 Small-Bowel Neuroendocrine Tumors: A Propensity Score Matching Analysis from SEER Database. J. Gastrointest. Surg. 2021, 25, 3188–3197. [Google Scholar] [CrossRef]
- Shaffie, A.; Soliman, A.; Fraiwan, L.; Ghazal, M.; Taher, F.; Dunlap, N.; Wang, B.; Van Berkel, V.; Keynton, R.; Elmaghraby, A.; et al. A Generalized Deep Learning-Based Diagnostic System for Early Diagnosis of Various Types of Pulmonary Nodules. Technol. Cancer Res. Treat. 2018, 17, 1533033818798800. [Google Scholar] [CrossRef]
- Hathaway, Q.A.; Yanamala, N.; Budoff, M.J.; Sengupta, P.P.; Zeb, I. Deep neural survival networks for cardiovascular risk prediction: The Multi-Ethnic Study of Atherosclerosis (MESA). Comput. Biol. Med. 2021, 139, 104983. [Google Scholar] [CrossRef]
- Nicholl, M.B.; Ahuja, V.; Conway, W.C.; Vu, V.D.; Sim, M.-S.; Singh, G. Small Bowel Adenocarcinoma: Understaged and Undertreated? Ann. Surg. Oncol. 2010, 17, 2728–2732. [Google Scholar] [CrossRef]
- Liu, T.; Wu, Y.; Jiang, T. Efficacy of surgery and chemotherapy for stage IV small bowel adenocarcinoma: A population-based analysis using Surveillance, Epidemiology, and End Result Program database. Cancer Med. 2020, 9, 6638–6645. [Google Scholar] [CrossRef]
- Aparicio, T.; Henriques, J.; Manfredi, S.; Tougeron, D.; Bouché, O.; Pezet, D.; Piessen, G.; Coriat, R.; Zaanan, A.; Legoux, J.-L.; et al. Small bowel adenocarcinoma: Results from a nationwide prospective ARCAD-NADEGE cohort study of 347 patients. Int. J. Cancer 2020, 147, 967–977. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| The Training Set (n = 1398) | The Validation Set (n = 589) | |||||
|---|---|---|---|---|---|---|
| Characteristics | Non-CSD (n = 1238) | CSD (n = 160) | p | Non-CSD (n = 534) | CSD (n = 55) | p |
| Sex (%) | 0.404 | 0.320 | ||||
| Female | 566 (45.7) | 67 (41.9) | 258 (48.3) | 31 (56.4) | ||
| Male | 672 (54.3) | 93 (58.1) | 276 (51.7) | 24 (43.6) | ||
| Age (years, %) | <0.001 | <0.001 | ||||
| <30 | 7 (0.6) | 2 (1.2) | 4 (0.7) | 0 (0.0) | ||
| 30–39 | 40 (3.2) | 1 (0.6) | 20 (3.7) | 1 (1.8) | ||
| 40–49 | 100 (8.1) | 2 (1.2) | 42 (7.9) | 1 (1.8) | ||
| 50–59 | 249 (20.1) | 16 (10.0) | 119 (22.3) | 10 (18.2) | ||
| 60–69 | 382 (30.9) | 39 (24.4) | 142 (26.6) | 8 (14.5) | ||
| 70–79 | 308 (24.9) | 53 (33.1) | 143 (26.8) | 14 (25.5) | ||
| ≥80 | 152 (12.3) | 47 (29.4) | 64 (12.0) | 21 (38.2) | ||
| Race (%) | 0.056 | 0.199 | ||||
| Black | 246 (19.9) | 29 (18.1) | 89 (16.7) | 11 (20.0) | ||
| White | 914 (73.8) | 112 (70.0) | 408 (76.4) | 39 (70.9) | ||
| Asian | 70 (5.7) | 18 (11.2) | 33 (6.2) | 3 (5.5) | ||
| Indian | 8 (0.6) | 1 (0.6) | 4 (0.7) | 2 (3.6) | ||
| Median household Income ($, %) | 0.732 | 0.984 | ||||
| (−∞, 35,000) | 19 (1.5) | 1 (0.6) | 10 (1.9) | 1 (1.8) | ||
| [35,000, 55,000) | 271 (21.9) | 38 (23.8) | 106 (19.9) | 12 (21.8) | ||
| [55,000, 75,000) | 539 (43.5) | 66 (41.2) | 222 (41.6) | 23 (41.8) | ||
| [75,000, +∞) | 409 (33.0) | 55 (34.4) | 196 (36.7) | 19 (34.5) | ||
| Region | 0.386 | 0.743 | ||||
| non-metropolis | 141 (11.4) | 14 (8.8) | 55 (10.3) | 7 (12.7) | ||
| metropolis | 1097 (88.6) | 146 (91.2) | 479 (89.7) | 48 (87.3) | ||
| Primary tumor site (%) | <0.001 | <0.001 | ||||
| NOS | 131 (10.6) | 18 (11.2) | 51 (9.6) | 5 (9.1) | ||
| Duodenum | 537 (43.4) | 102 (63.7) | 210 (39.3) | 38 (69.1) | ||
| Jejunum | 145 (11.7) | 15 (9.4) | 57 (10.7) | 2 (3.6) | ||
| Ileum | 419 (33.8) | 23 (14.4) | 210 (39.3) | 9 (16.4) | ||
| Overlapping | 6 (0.5) | 2 (1.2) | 6 (1.1) | 1 (1.8) | ||
| Histological type (%) | <0.001 | <0.001 | ||||
| others | 72 (5.8) | 31 (19.4) | 40 (7.5) | 10 (18.2) | ||
| Adenocarcinoma | 320 (25.8) | 111 (69.4) | 143 (26.8) | 39 (70.9) | ||
| Carcinoid | 685 (55.3) | 16 (10.0) | 295 (55.2) | 6 (10.9) | ||
| Stromal sarcoma | 161 (13.0) | 2 (1.2) | 56 (10.5) | 0 (0.0) | ||
| T stage (%) | <0.001 | 0.001 | ||||
| Tx | 164 (13.2) | 68 (42.5) | 77 (14.4) | 23 (41.8) | ||
| T0 | 3 (0.2) | 2 (1.2) | 0 | 0 | ||
| Tis | 0 (0.0) | 1 (0.6) | 0 | 0 | ||
| T1 | 298 (24.1) | 22 (13.8) | 112 (21.0) | 9 (16.4) | ||
| T2 | 176 (14.2) | 5 (3.1) | 84 (15.7) | 1 (1.8) | ||
| T3 | 340 (27.5) | 17 (10.6) | 146 (27.3) | 5 (9.1) | ||
| T4 | 257 (20.8) | 45 (28.1) | 115 (21.5) | 17 (30.9) | ||
| N stage (%) | 0.731 | 0.556 | ||||
| Nx | 109 (8.8) | 37 (23.1) | 53 (9.9) | 12 (21.8) | ||
| N0 | 687 (55.5) | 79 (49.4) | 260 (48.7) | 27 (49.1) | ||
| N1 | 303 (24.5) | 29 (18.1) | 150 (28.1) | 11 (20.0) | ||
| N2 | 139 (11.2) | 15 (9.4) | 71 (13.3) | 5 (9.1) | ||
| M stage (%) | <0.001 | <0.001 | ||||
| M1 | 983 (79.4) | 78 (48.8) | 408 (76.4) | 27 (49.1) | ||
| M2 | 255 (20.6) | 82 (51.2) | 126 (23.6) | 28 (50.9) | ||
| Stage (%) | <0.001 | <0.001 | ||||
| NA | 117 (9.5) | 27 (16.9) | 42 (7.9) | 9 (16.4) | ||
| I | 342 (27.6) | 16 (10.0) | 132 (24.7) | 3 (5.5) | ||
| II | 207 (16.7) | 17 (10.6) | 77 (14.4) | 6 (10.9) | ||
| III | 317 (25.6) | 18 (11.2) | 157 (29.4) | 9 (16.4) | ||
| IV | 255 (20.6) | 82 (51.2) | 126 (23.6) | 28 (50.9) | ||
| Surgery (%) | <0.001 | <0.001 | ||||
| No | 288 (23.3) | 114 (71.2) | 123 (23.0) | 40 (72.7) | ||
| Yes | 950 (76.7) | 46 (28.7) | 411 (77.0) | 15 (27.3) | ||
| Tumor size (mm, median [IQR]) | 21.00 [12.00, 42.00] | 32.00 [20.00, 55.00] | <0.001 | 22.00 [12.00, 41.00] | 40.00 [25.50, 53.00] | <0.001 |
| Removed nodes (median [IQR]) | 3.00 [0.00, 15.00] | 0.00 [0.00, 1.00] | <0.001 | 3.00 [0.00, 15.00] | 0.00 [0.00, 0.00] | <0.001 |
| Lymph node examine (%) | <0.001 | <0.001 | ||||
| No | 522 (42.2) | 115 (71.9) | 222 (41.6) | 41 (74.5) | ||
| Yes | 716 (57.8) | 45 (28.1) | 312 (58.4) | 14 (25.5) | ||
| Model | Group | C-index | AUCs | Brier Scores | ||||
|---|---|---|---|---|---|---|---|---|
| 3-Month | 6-Month | 9-Month | 3-Month | 6-Month | 9-Month | |||
| Cox-PH | The training set (n = 1398) | 0.878 | 0.898 | 0.897 | 0.894 | 0.262 | 0.252 | 0.246 |
| The validation set (n = 589) | 0.866 | 0.874 | 0.922 | 0.908 | 0.282 | 0.265 | 0.265 | |
| DeepSurv | The internal validation set (n = 269) | 0.869 | 0.874 | 0.871 | 0.871 | 0.068 | 0.079 | 0.085 |
| The validation set (n = 589) | 0.871 | 0.878 | 0.891 | 0.891 | 0.058 | 0.070 | 0.080 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yin, M.; Lin, J.; Liu, L.; Gao, J.; Xu, W.; Yu, C.; Qu, S.; Liu, X.; Qian, L.; Xu, C.; et al. Development of a Deep Learning Model for Malignant Small Bowel Tumors Survival: A SEER-Based Study. Diagnostics 2022, 12, 1247. https://doi.org/10.3390/diagnostics12051247
Yin M, Lin J, Liu L, Gao J, Xu W, Yu C, Qu S, Liu X, Qian L, Xu C, et al. Development of a Deep Learning Model for Malignant Small Bowel Tumors Survival: A SEER-Based Study. Diagnostics. 2022; 12(5):1247. https://doi.org/10.3390/diagnostics12051247
Chicago/Turabian StyleYin, Minyue, Jiaxi Lin, Lu Liu, Jingwen Gao, Wei Xu, Chenyan Yu, Shuting Qu, Xiaolin Liu, Lijuan Qian, Chunfang Xu, and et al. 2022. "Development of a Deep Learning Model for Malignant Small Bowel Tumors Survival: A SEER-Based Study" Diagnostics 12, no. 5: 1247. https://doi.org/10.3390/diagnostics12051247
APA StyleYin, M., Lin, J., Liu, L., Gao, J., Xu, W., Yu, C., Qu, S., Liu, X., Qian, L., Xu, C., & Zhu, J. (2022). Development of a Deep Learning Model for Malignant Small Bowel Tumors Survival: A SEER-Based Study. Diagnostics, 12(5), 1247. https://doi.org/10.3390/diagnostics12051247