
Ultrasonographic Measurement of Torsional Side Difference in Proximal Humerus Fractures and Humeral Shaft Fractures: Theoretical Background with Technical Notes for Clinical Implementation
Abstract
1. Introduction
2. Materials and Methods
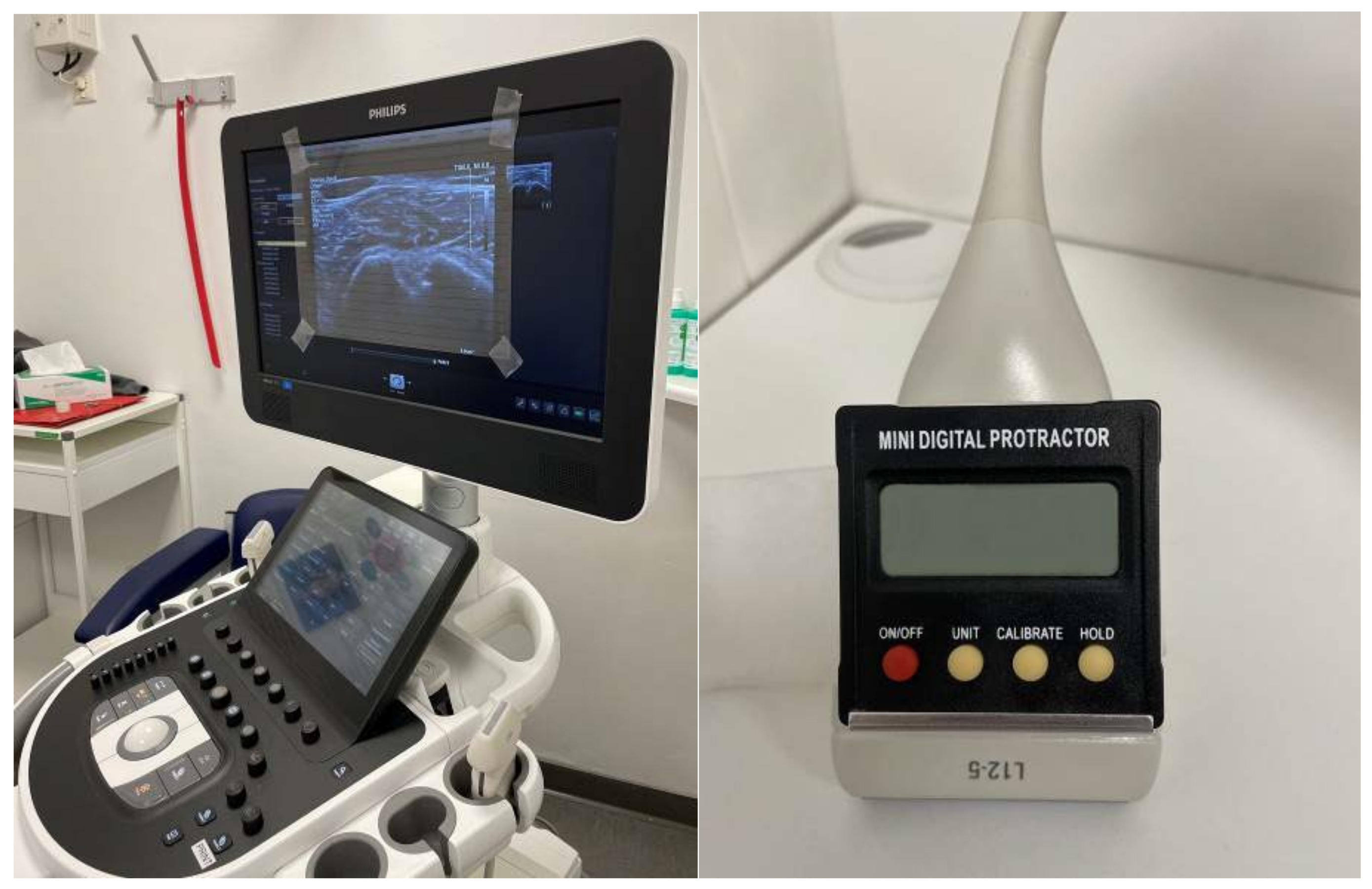
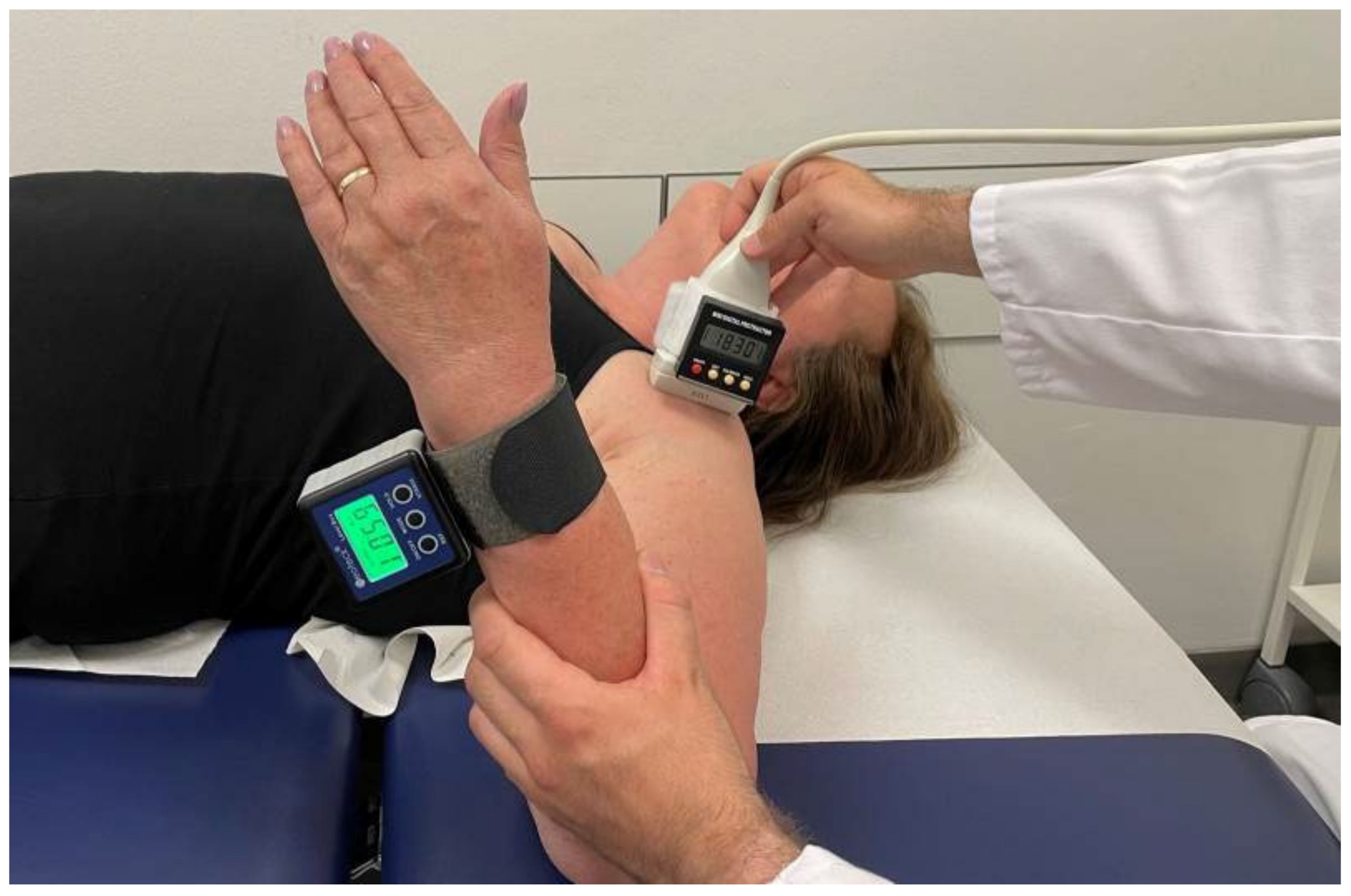
2.1. Clinical Approach and Setup
2.2. Example Case Presentation
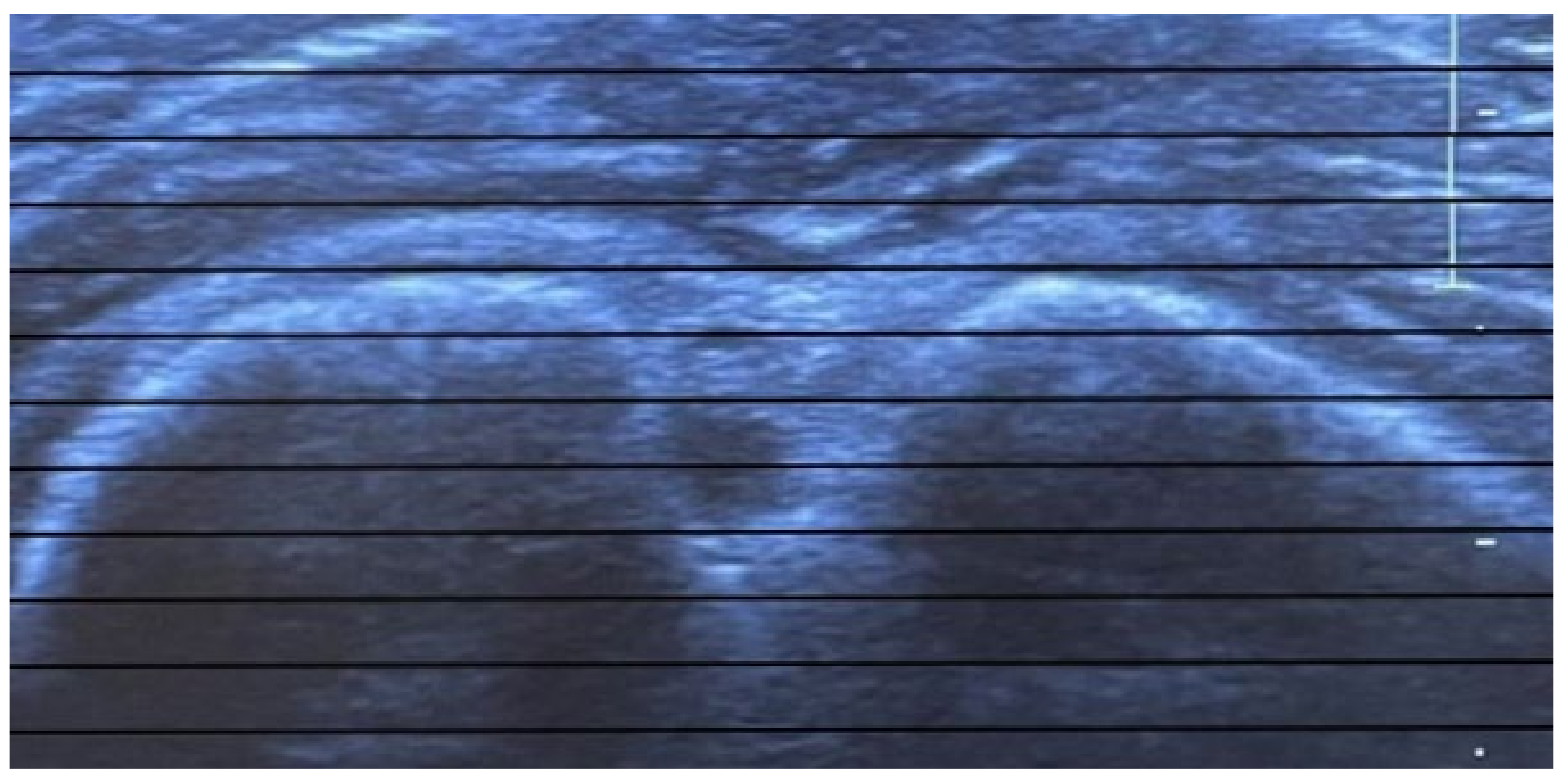
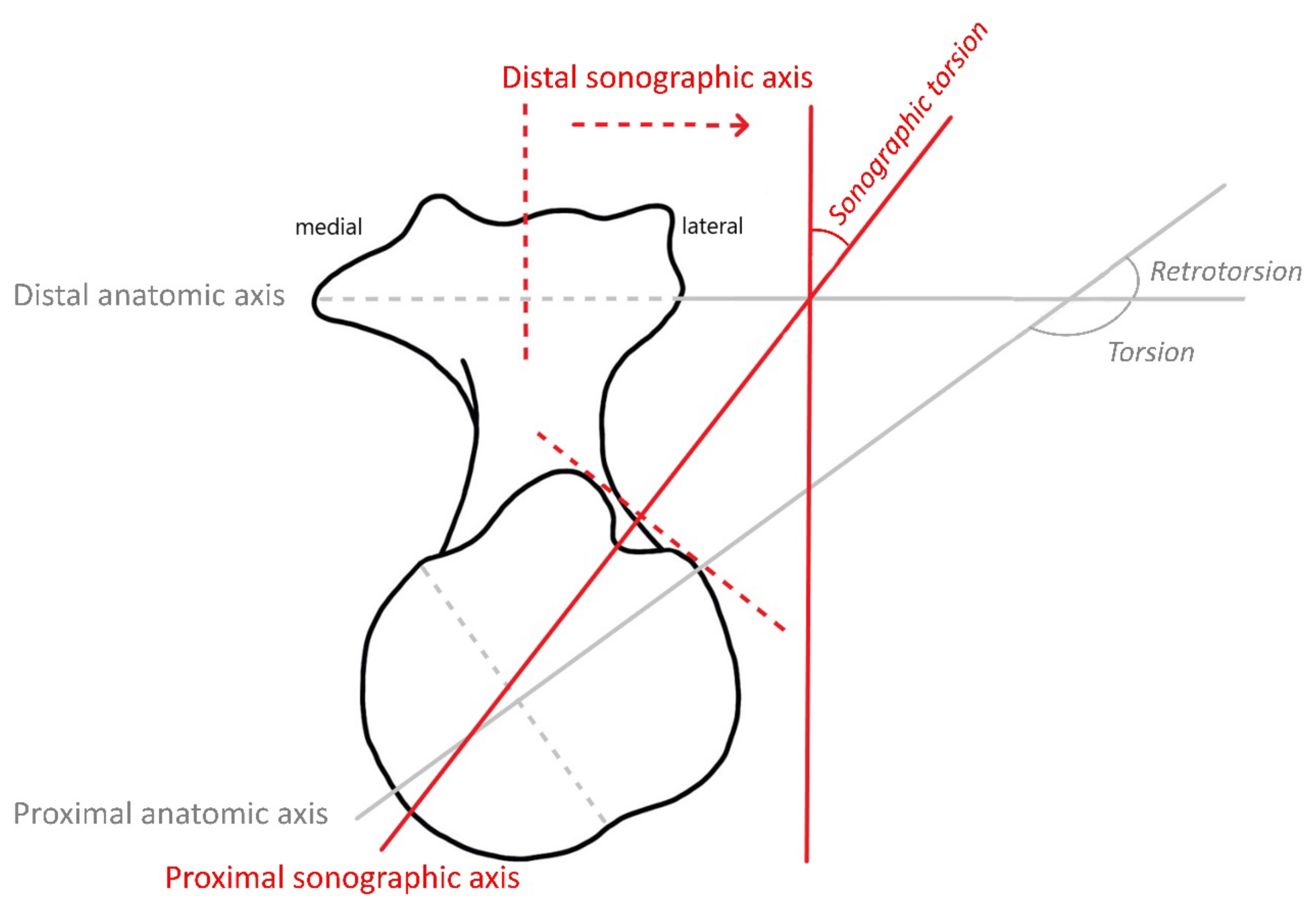
3. Interpretation of Ultrasonographic Measurements
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Doyle, A.J.; Burks, R.T. Comparison of humeral head retroversion with the humeral axis/biceps groove relationship: A study in live subjects and cadavers. J. Shoulder Elb. Surg. 1998, 7, 453–457. [Google Scholar] [CrossRef] [PubMed]
- Martin, R. Lehrbuch der Anthropologie in Systematischer Darstellung mit Besonderer Berücksichtigung der Anthropologischen Methoden; Gustav Fischer Verlag: Jena, Germany, 1914; p. 909. [Google Scholar]
- Dähnert, W.; Bernd, W. Computer tomography determination of the torsion angle of the humerus. Z. Fur. Orthop. Und Ihre Grenzgeb. 1986, 124, 46–49. [Google Scholar] [CrossRef] [PubMed]
- Harland, U.; Diepolder, M.; Gruber, G.; Knöss, H.P. Die sonographische Bestimmung des Humerusretrotorsionswinkels. Z. Fur. Orthop. Und Ihre Grenzgeb. 1991, 129, 36–41. [Google Scholar] [CrossRef] [PubMed]
- Saha, A.K. Dynamic stability of the glenohumeral joint. Acta Orthop. Scand. 1971, 42, 491–505. [Google Scholar] [CrossRef] [PubMed]
- Ito, N.; Eto, M.; Maeda, K.; Rabbi, M.E.; Iwasaki, K. Ultrasonographic measurement of humeral torsion. J. Shoulder Elb. Surg. 1995, 4, 157–161. [Google Scholar] [CrossRef]
- Harland, U. Sonographische Achsenbestimmungen am Skelett. In Ultraschalldiagnostik ’86; Hansmann, M., Koischwitz, D., Lutz, H., Trier, H.G., Eds.; Springer: Berlin/Heidelberg, Germany, 1987; pp. 662–667. [Google Scholar]
- Myers, J.B.; Oyama, S.; Clarke, J.P. Ultrasonographic assessment of humeral retrotorsion in baseball players: A validation study. Am. J. Sports Med. 2012, 40, 1155–1160. [Google Scholar] [CrossRef]
- Saka, M.; Yamauchi, H.; Yoshioka, T.; Hamada, H.; Gamada, K. Conventional Humeral Retroversion Measurements Using Computed Tomography Slices or Ultrasound Images Are Not Correlated With the 3-Dimensional Humeral Retroversion Angle. Orthop. J. Sports Med. 2015, 3, 2325967115573701. [Google Scholar] [CrossRef]
- Hannah, D.C.; Scibek, J.S.; Carcia, C.R.; Phelps, A.L. Reliability and Validity of a 1-Person Technique to Measure Humeral Torsion Using Ultrasound. J. Athl. Train. 2018, 53, 590–596. [Google Scholar] [CrossRef]
- Whiteley, R.; Ginn, K.; Nicholson, L.; Adams, R. Indirect ultrasound measurement of humeral torsion in adolescent baseball players and non-athletic adults: Reliability and significance. J. Sci. Med. Sport 2006, 9, 310–318. [Google Scholar] [CrossRef]
- Achenbach, L.; Clément, A.C.; Hufsky, L.; Greiner, S.; Zeman, F.; Walter, S.S. The throwing shoulder in youth elite handball: Soft-tissue adaptations but not humeral retrotorsion differ between the two sexes. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 3937–3943. [Google Scholar] [CrossRef]
- Yaari, L.S.; Mullaney, M.J.; Fukunaga, T.; Thein, R.; McHugh, M.P.; Nicholas, S.J. Assessment of Humeral Torsion by Palpation in Baseball Pitchers: A Validation Study. Int. J. Sports Phys. 2020, 15, 1073–1079. [Google Scholar] [CrossRef]
- Thomas, S.; Swanik, C.; Kaminski, T.; Higginson, J.; Swanik, K.; Bartolozzi, A.; Nazarian, L. Humeral retroversion and its association with posterior capsule thickness in collegiate baseball players. J. Shoulder Elb. Surg. 2012, 21, 910–916. [Google Scholar] [CrossRef]
- Shanley, E.; Thigpen, C.A.; Clark, J.C.; Wyland, D.J.; Hawkins, R.J.; Noonan, T.J.; Kissenberth, M.J. Changes in passive range of motion and development of glenohumeral internal rotation deficit (GIRD) in the professional pitching shoulder between spring training in two consecutive years. J. Shoulder Elb. Surg. 2012, 21, 1605–1612. [Google Scholar] [CrossRef]
- Noonan, T.J.; Shanley, E.; Bailey, L.B.; Wyland, D.J.; Kissenberth, M.J.; Hawkins, R.J.; Thigpen, C.A. Professional Pitchers With Glenohumeral Internal Rotation Deficit (GIRD) Display Greater Humeral Retrotorsion Than Pitchers Without GIRD. Am. J. Sports Med. 2015, 43, 1448–1454. [Google Scholar] [CrossRef]
- Yamamoto, N.; Itoi, E.; Minagawa, H.; Urayama, M.; Saito, H.; Seki, N.; Iwase, T.; Kashiwaguchi, S.; Matsuura, T. Why is the humeral retroversion of throwing athletes greater in dominant shoulders than in nondominant shoulders? J. Shoulder Elb. Surg. 2006, 15, 571–575. [Google Scholar] [CrossRef]
- Martin, C.P. The Cause of Torsion of the Humerus and of the Notch on the Anterior Edge of the Glenoid Cavity of the Scapula. J. Anat. 1933, 67, 573–582. [Google Scholar]
- Evans, F.G.; Krahl, V.E. The torsion of the humerus: A phylogenetic survey from fish to man. Am. J. Anat. 1945, 76, 303–337. [Google Scholar] [CrossRef]
- Roach, N.T.; Lieberman, D.E.; Gill, T.J.T.; Palmer, W.E.; Gill, T.J., 3rd. The effect of humeral torsion on rotational range of motion in the shoulder and throwing performance. J. Anat. 2012, 220, 293–301. [Google Scholar] [CrossRef]
- Edelson, G. Variations in the retroversion of the humeral head. J. Shoulder Elb. Surg. 1999, 8, 142–145. [Google Scholar] [CrossRef]
- Boileau, P.; Bicknell, R.T.; Mazzoleni, N.; Walch, G.; Urien, J.P. CT scan method accurately assesses humeral head retroversion. Clin. Orthop. Relat. Res. 2008, 466, 661–669. [Google Scholar] [CrossRef]
- Cassagnaud, X.; Maynou, C.; Petroff, E.; Dujardin, C.; Mestdagh, H. A study of reproducibility of an original method of CT measurement of the lateralization of the intertubercular groove and humeral retroversion. Surg. Radiol. Anat. 2003, 25, 145–151. [Google Scholar] [CrossRef] [PubMed]
- Kronberg, M.; Broström, L.A.; Söderlund, V. Retroversion of the humeral head in the normal shoulder and its relationship to the normal range of motion. Clin. Orthop. Relat. Res. 1990, 253, 113–117. [Google Scholar] [CrossRef]
- Yoshida, M.; Saho, Y.; Katayose, M. Reliability of measuring humeral retroversion using ultrasound imaging in a healthy nonthrowing population. J. Sport Rehabil. 2010, 19, 149–160. [Google Scholar] [CrossRef] [PubMed]
- Dare, S.S.; Masilili, G.; Mugagga, K.; Ekanem, P.E. Evaluation of Bilateral Asymmetry in the Humerus of Human Skeletal Specimen. BioMed Res. Int. 2019, 2019, 3194912. [Google Scholar] [CrossRef] [PubMed]
- Matsumura, N.; Ogawa, K.; Kobayashi, S.; Oki, S.; Watanabe, A.; Ikegami, H.; Toyama, Y. Morphologic features of humeral head and glenoid version in the normal glenohumeral joint. J. Shoulder Elb. Surg. 2014, 23, 1724–1730. [Google Scholar] [CrossRef]
- Hernigou, P.; Duparc, F.; Hernigou, A. Determining humeral retroversion with computed tomography. J. Bone Jt. Surg. Am. Vol. 2002, 84, 1753–1762. [Google Scholar] [CrossRef]
- Pieper, H.G. Humeral torsion in the throwing arm of handball players. Am. J. Sports Med. 1998, 26, 247–253. [Google Scholar] [CrossRef]
- Debevoise, N.T.; Hyatt, G.W.; Townsend, G.B. Humeral torsion in recurrent shoulder dislocations. A technic of determination by X-ray. Clin. Orthop. Relat. Res. 1971, 76, 87–93. [Google Scholar] [CrossRef]
- Fuchs, C.C.; Schmid, P.; Engelhardt, P. Computerized tomography measurement of humerus torsion. Z. Fur. Orthop. Und Ihre Grenzgeb. 1991, 129, 423–425. [Google Scholar] [CrossRef]
- Öztuna, V.; Öztürk, H.; Eskandari, M.M.; Kuyurtar, F. Measurement of the humeral head retroversion angle. Arch. Orthop. Trauma Surg. 2002, 122, 406–409. [Google Scholar] [CrossRef]
- Pan, Z.; Chen, J.; Qu, L.; Cui, Y.; Sun, C.; Zhang, H.; Yang, X.; Guan, Q. Correlation between anatomical parameters of intertubercular sulcus and retroversion angle of humeral head. Int. J. Clin. Exp. Med. 2015, 8, 4837–4845. [Google Scholar]
- Kunz, C.; Rieder, T.; Viehweger, R. Can ultrasonography be used to measure torsion angle of the humerus? Comparison of ultrasonographic, computerized tomographic and anthropometric methods. Z. Fur. Orthop. Und Ihre Grenzgeb. 1993, 131, 307–312. [Google Scholar] [CrossRef]
- Chu, Y.-L.; Chen, C.-K.; Liu, Y.-C.; Lu, T.-W.; Liaw, C.-K. Geometrical analysis for assessing torsional alignment of humerus. BMC Musculoskelet. Disord. 2020, 21, 92. [Google Scholar] [CrossRef]
- Oh, J.H.; Kim, W.; Cayetano, A.A., Jr. Measurement Methods for Humeral Retroversion Using Two-Dimensional Computed Tomography Scans: Which Is Most Concordant with the Standard Method? Clin. Orthop. Surg. 2017, 9, 223–231. [Google Scholar] [CrossRef]
- Jerosch, J.; Sons, H.U.; Sterken, W.; Winkelmann, W. Ultrasound determination of the humerus retrotorsion angle. An experimental and clinical study. Ultraschall Der Med. 1989, 10, 270–274. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case Study: Passive Range of Rotational Motion in 90° Abduction | ||
|---|---|---|
| Internal rotation (in degrees [°]) | External rotation (in degrees [°]) | |
| Left arm (unaffected) | 65° | 100° |
| Right arm (affected) | 0° | 140° |
| Different Sonographic Torsion Measurements in Previous Literature | ||||
|---|---|---|---|---|
| Author | Year | n | Torsion Angle (in degrees [°]) Mean ± Standard Deviation (Range) | Journal |
| Determining the torsion angle using the forearm and measuring the angles in relation to a vertical reference axis | ||||
| Ito et al. [6] | 1995 | 30 | 15.1 ± 3.9 (right) ± 2.9 (left) | J. Shoulder Elbow Surg. |
| Whiteley et al. [11] | 2006 | 32 | 18.2 ± 9.6 (4 to 40) (dominant) 19.8 ± 10.8 (5 to 45) (nondominant) | J. Sci. Med. Sport |
| Whiteley et al. [11] | 2006 | 70 | 13.8 ± 8.6 (−3 to 36) (dominant) 25 ± 9.2 (8 to 50) (nondominant) | J. Sci. Med. Sport |
| Thomas et al. [14] | 2012 | 48 | 0.53 ± 12.53 (dominant) 16.13 ± 11.53 (nondominant) | J. Shoulder Elbow Surg. |
| Shanley et al. [15] | 2012 | 66 | 10 ± 11 (dominant) 23 ± 11 (nondominant) | J. Shoulder Elbow Surg. |
| Noonan et al. [16] | 2015 | 324 | 10.4 ± 11.7 (dominant) 22.7 ± 11.7 (nondominant) | Am. J. Sports Med. |
| Achenbach et al. [12] | 2019 | 276 | 16.5 ± 9.6 (dominant) 13.5 ± 9.4 (nondominant) | Knee Surg. Sports Traumatol. Arthrosc. |
| Yaari et al. [13] | 2020 | 40 | 20 ± 10 (dominant) 29 ± 12 (nondominant) | Int. J. Sports Phys. Ther. |
| Determining the torsion angle using the forearm and measuring the angles in relation to a horizontal reference axis | ||||
| Myers et al. [8] | 2012 | 24 | 74.2 ± 14.5 (dominant) 61.2 ± 14.4 (nondominant) | Am. J. Sports Med. |
| Saka et al. [9] | 2015 | 28 | 78.5 ± 7.9 (dominant) 70.1 ± 7.8 (nondominant) | Orthop. J. Sports Med. |
| Hannah et al. [10] | 2018 | 30 | 64.4 ± 9.5 | J. Athl. Train. |
| Sonographic measurement of retroversion according to Harland | ||||
| Jerosch et al. [37] | 1989 | 20 | 67.85 ± 7.1 (52 to 80) | Ultraschall Med. |
| Harland et al. [4] | 1991 | 20 | 70.65 ± 8.4 (52 to 86) | Z. Orthop. |
| Harland et al. [4] | 1991 | 111 | 60.9 | Z. Orthop. |
| Kunz et al. [34] | 1993 | 40 | 52.0 ± 13.1 (24 to 75) | Z. Orthop. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Menzel, J.-N.; Zhang, D.; Krettek, C.; Hawi, N.; Razaeian, S. Ultrasonographic Measurement of Torsional Side Difference in Proximal Humerus Fractures and Humeral Shaft Fractures: Theoretical Background with Technical Notes for Clinical Implementation. Diagnostics 2022, 12, 3110. https://doi.org/10.3390/diagnostics12123110
Menzel J-N, Zhang D, Krettek C, Hawi N, Razaeian S. Ultrasonographic Measurement of Torsional Side Difference in Proximal Humerus Fractures and Humeral Shaft Fractures: Theoretical Background with Technical Notes for Clinical Implementation. Diagnostics. 2022; 12(12):3110. https://doi.org/10.3390/diagnostics12123110
Chicago/Turabian StyleMenzel, Jan-Niklas, Dafang Zhang, Christian Krettek, Nael Hawi, and Sam Razaeian. 2022. "Ultrasonographic Measurement of Torsional Side Difference in Proximal Humerus Fractures and Humeral Shaft Fractures: Theoretical Background with Technical Notes for Clinical Implementation" Diagnostics 12, no. 12: 3110. https://doi.org/10.3390/diagnostics12123110
APA StyleMenzel, J.-N., Zhang, D., Krettek, C., Hawi, N., & Razaeian, S. (2022). Ultrasonographic Measurement of Torsional Side Difference in Proximal Humerus Fractures and Humeral Shaft Fractures: Theoretical Background with Technical Notes for Clinical Implementation. Diagnostics, 12(12), 3110. https://doi.org/10.3390/diagnostics12123110