

Endometrioid Carcinomas of the Ovaries and Endometrium Involving Endocervical Polyps: Comprehensive Clinicopathological Analyses


Abstract
:1. Introduction
2. Materials and Methods
2.1. Case Selection
2.2. Clinical Data Collection
2.3. Pathological Data Collection
2.4. Immunohistochemical Staining
2.5. Immunohistochemical Interpretation
3. Results
3.1. The Prevalence and Histological Types of Gynecological Tumors Co-Existing with ECP
3.2. Clinical Presentations of Four Patients with EC Involving ECP
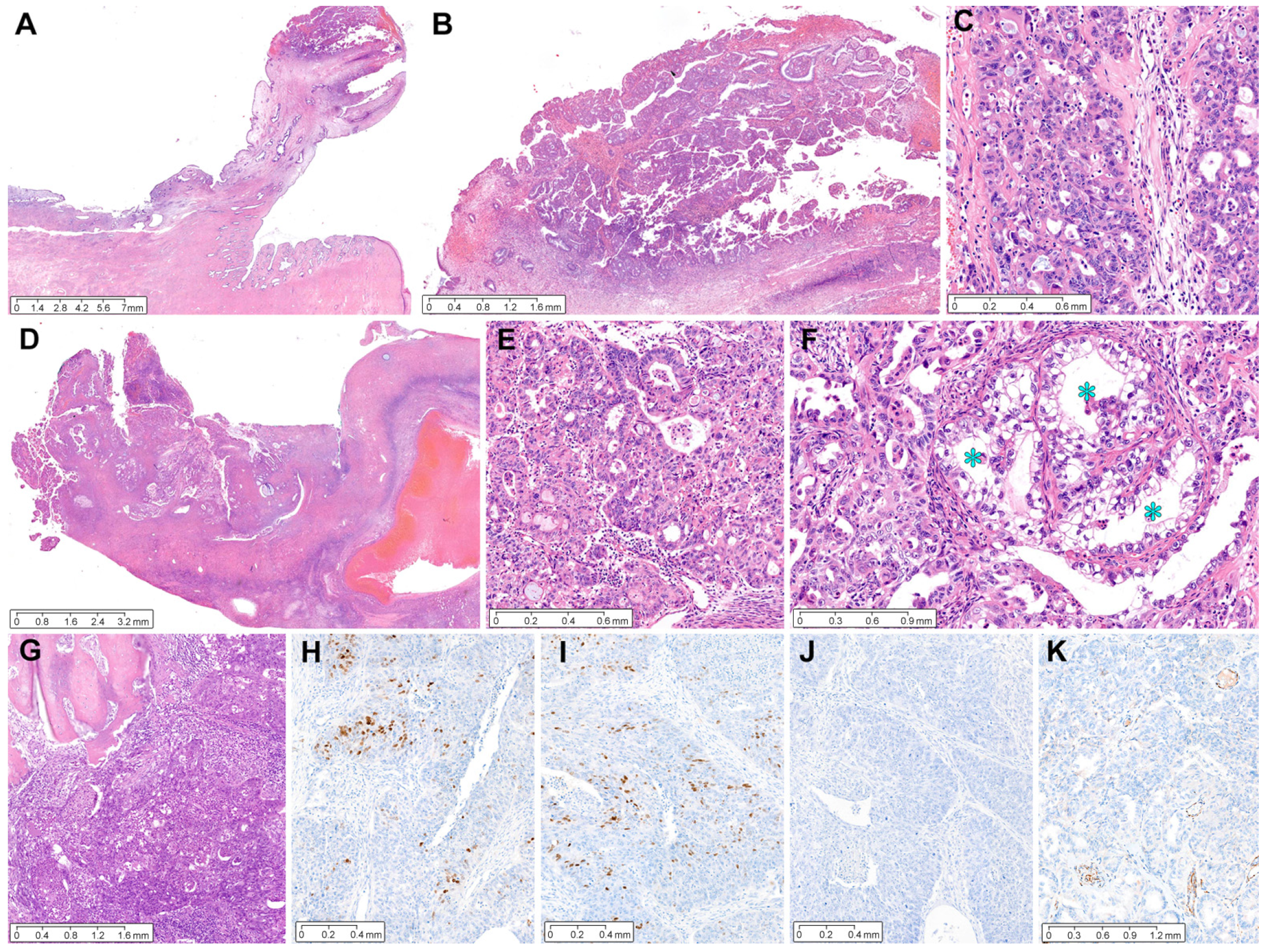
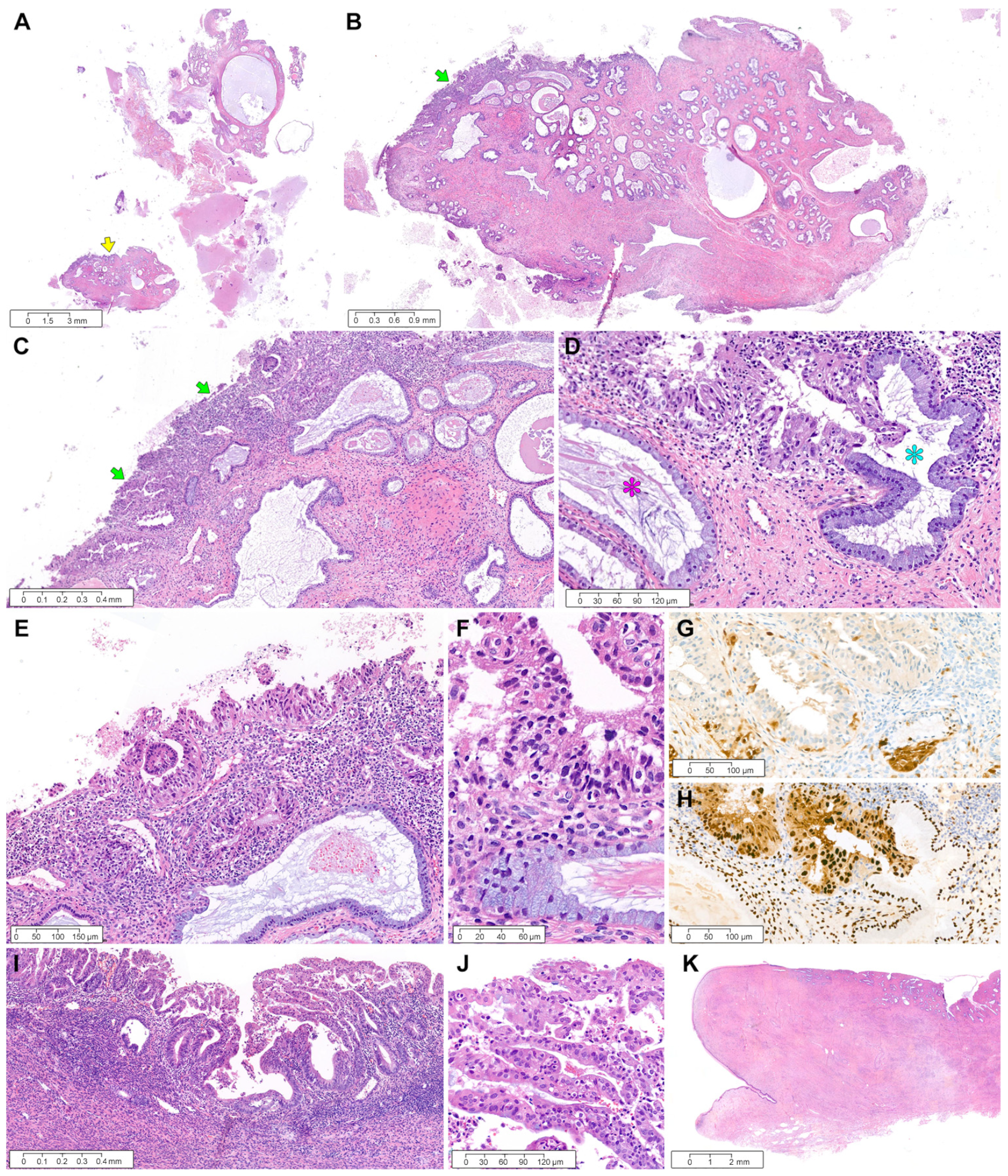
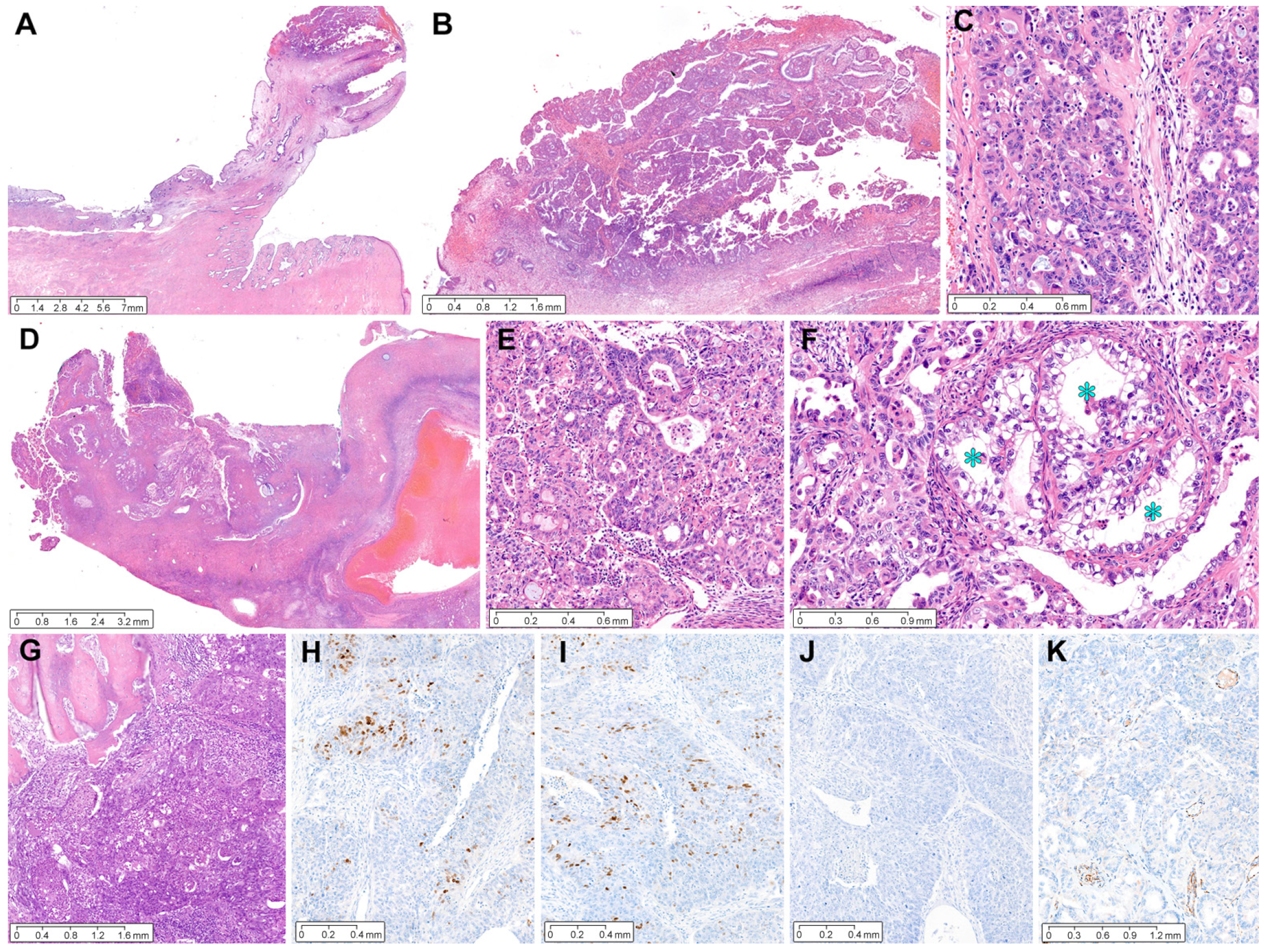
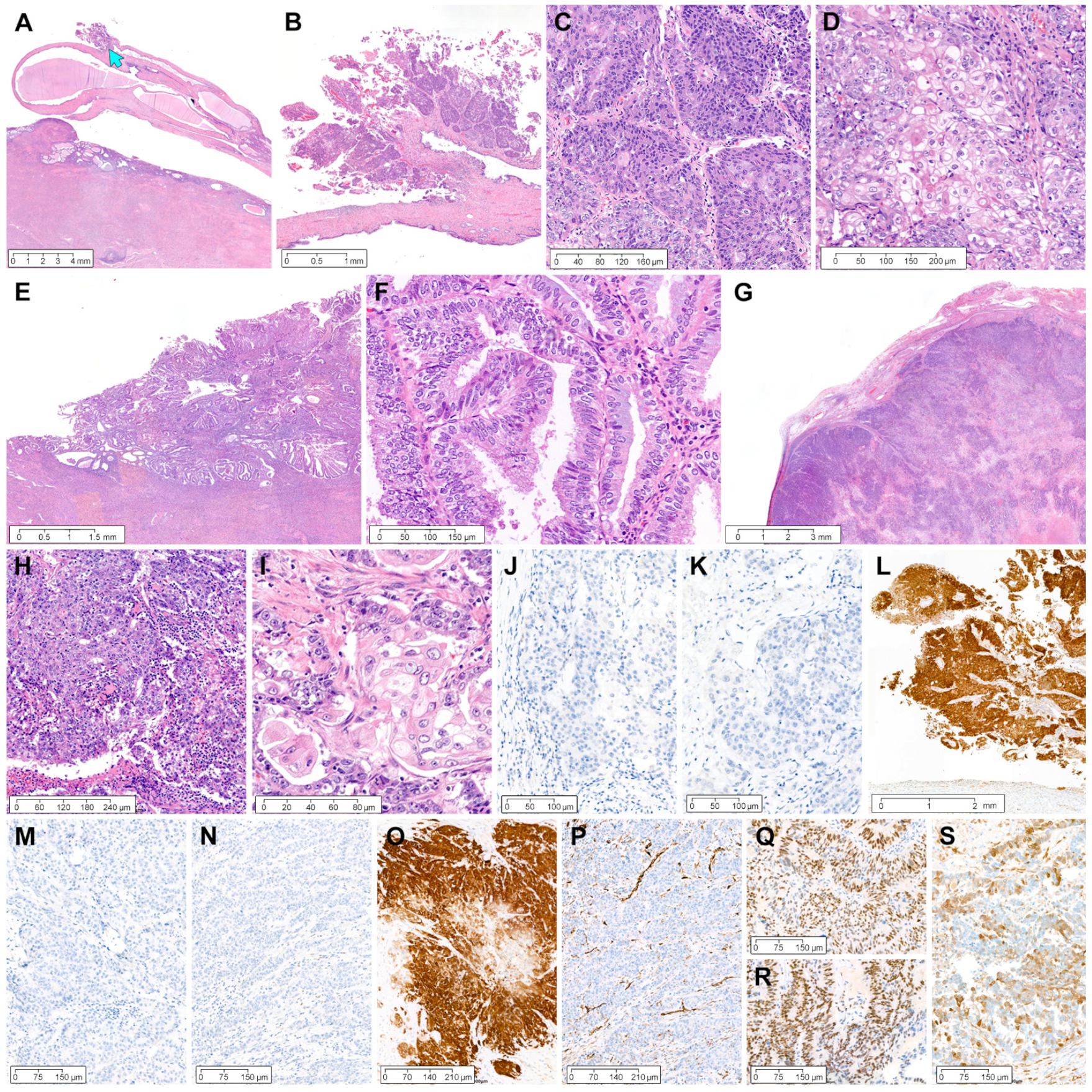
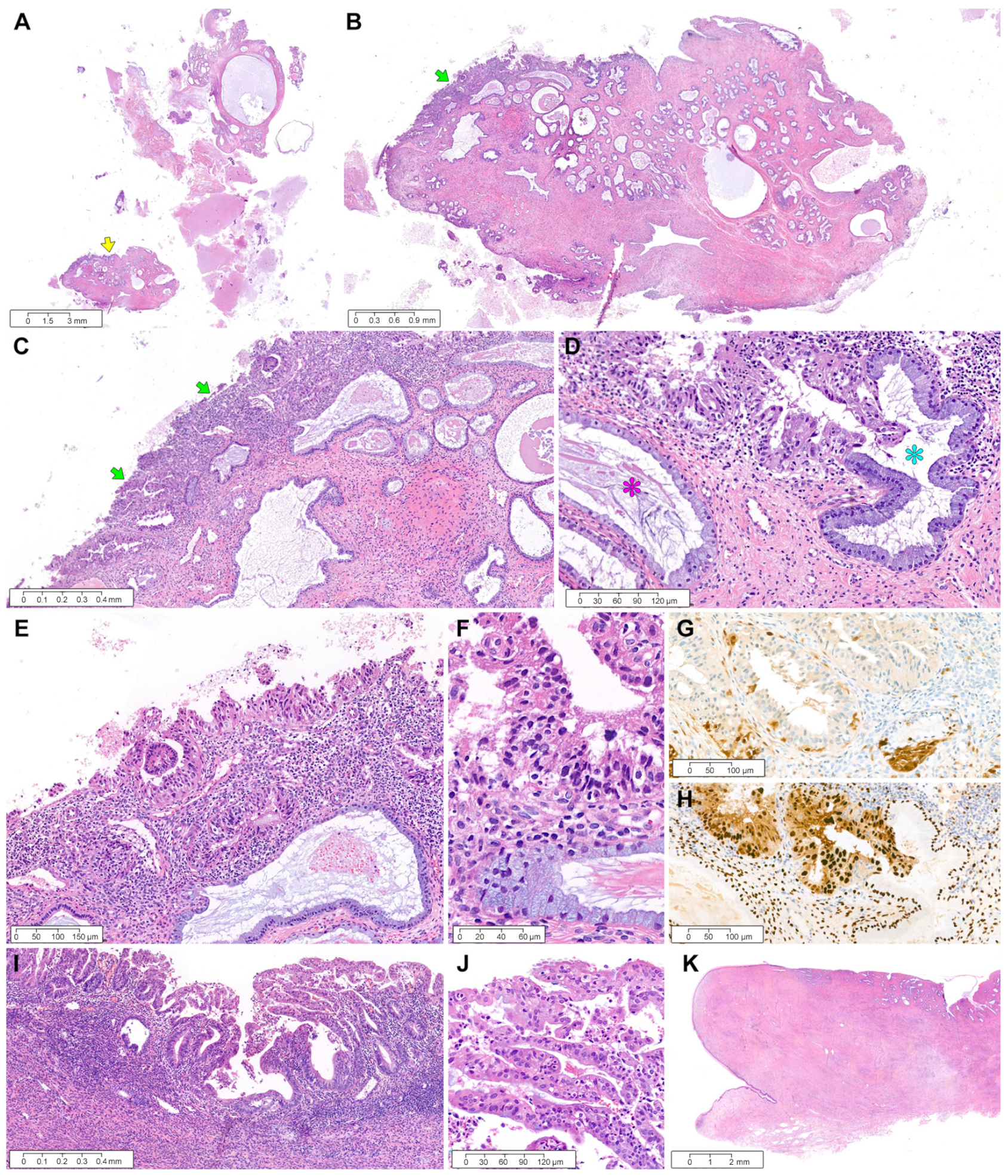
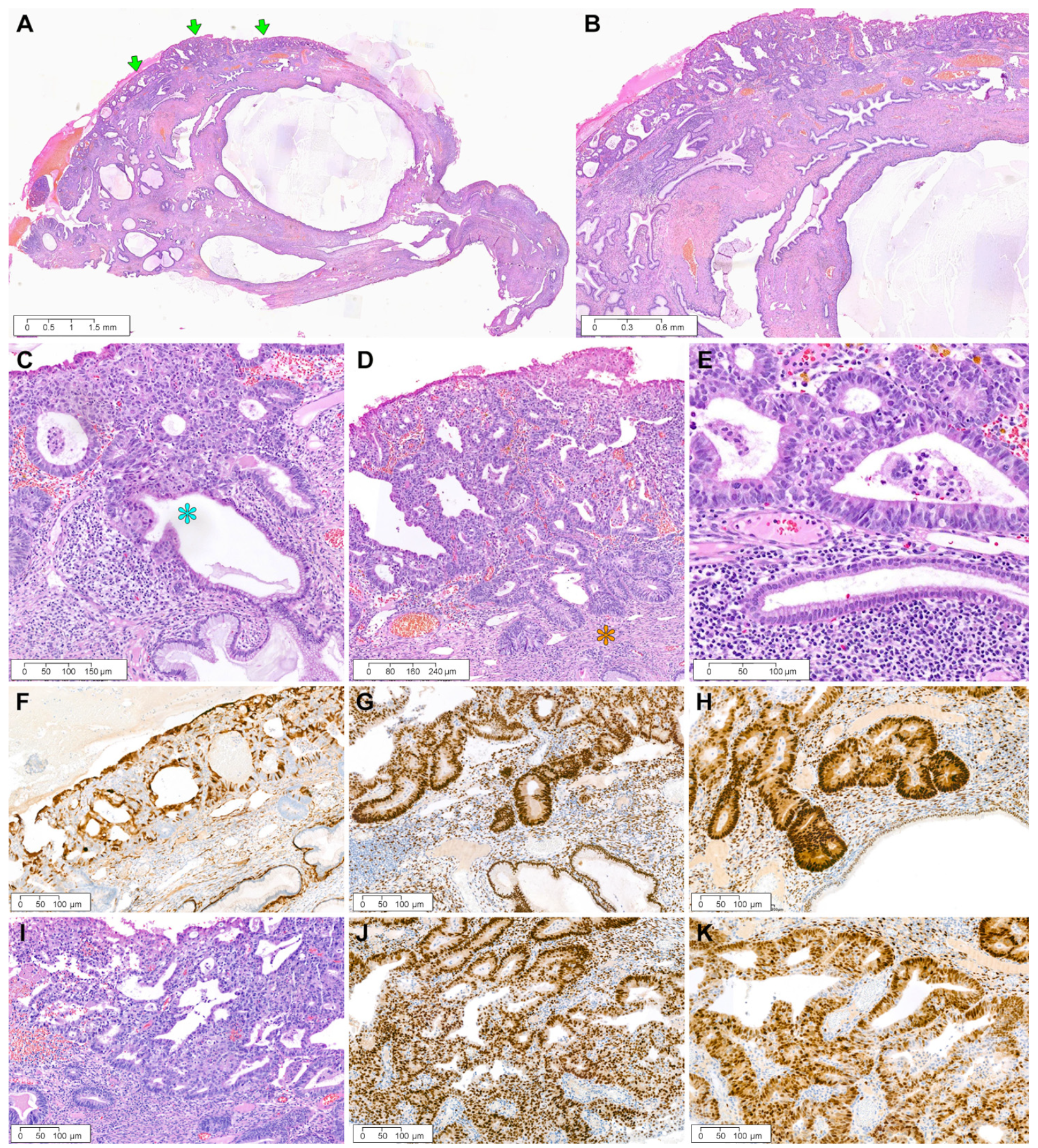
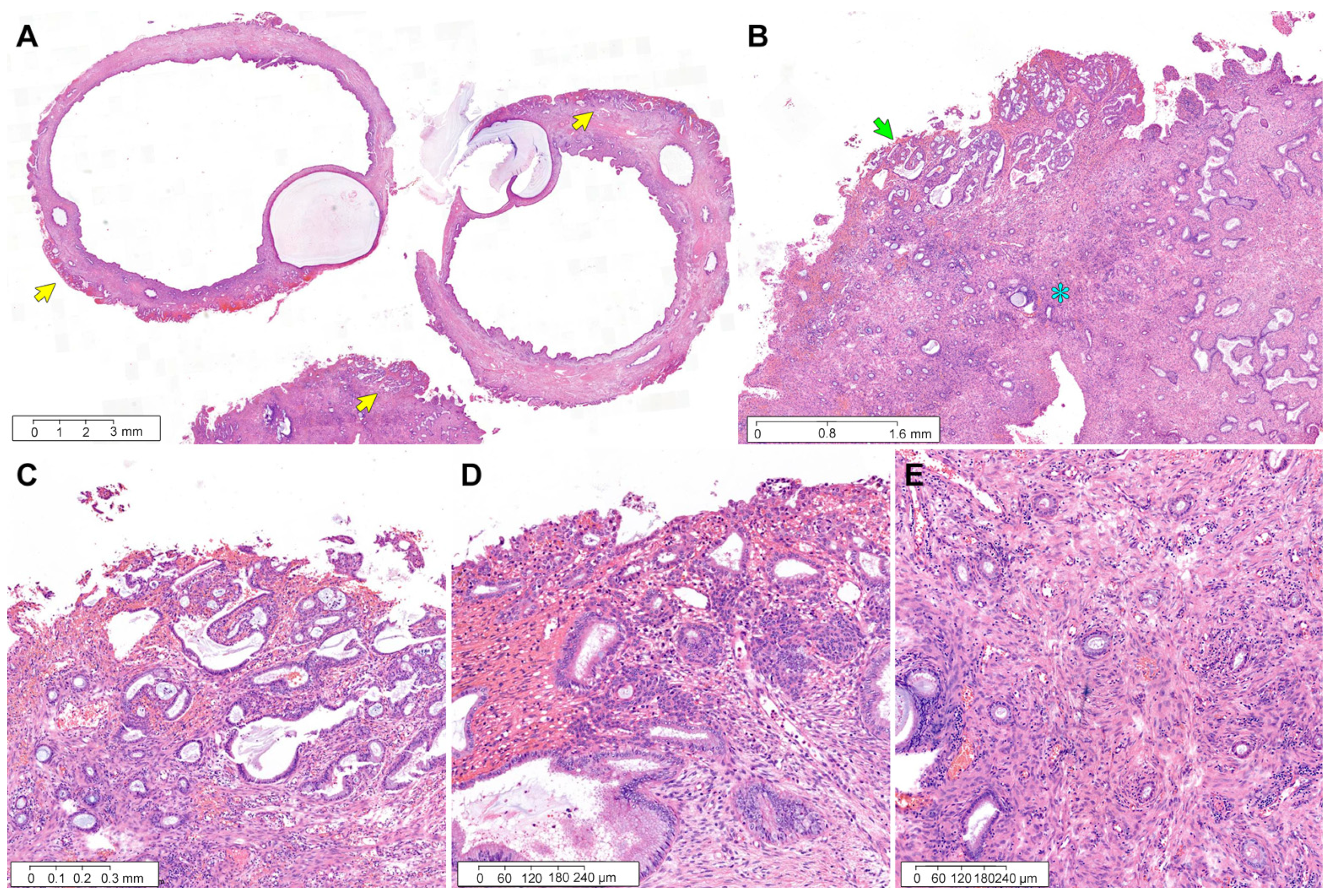
3.3. Pathological Characteristics of Four ECs Involving ECP
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Park, C.K.; Kim, Y.W.; Koh, H.H.; Yoon, N.; Bae, G.E.; Kim, H.S. Clinicopathological characteristics of squamous cell carcinoma and high-grade squamous intraepithelial lesions involving endocervical polyps. In Vivo 2020, 34, 2613–2621. [Google Scholar] [CrossRef] [PubMed]
- Misugi, T.; Kitada, K.; Fudaba, M.; Tanaka, S.; Kurihara, Y.; Tahara, M.; Hamuro, A.; Nakano, A.; Koyama, M.; Tachibana, D. Preliminary outcomes of cervical cerclage for shortened cervix with decidual polyp. Healthcare 2022, 10, 1312. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Bae, G.E.; Kim, J.; Kim, H.S. Mesonephric-like differentiation of endometrial endometrioid carcinoma: Clinicopathological and molecular characteristics distinct from those of uterine mesonephric-like adenocarcinoma. Diagnostics 2021, 11, 1450. [Google Scholar] [CrossRef] [PubMed]
- Alexandrova, E.; Pecoraro, G.; Sellitto, A.; Melone, V.; Ferravante, C.; Rocco, T.; Guacci, A.; Giurato, G.; Nassa, G.; Rizzo, F.; et al. An overview of candidate therapeutic target genes in ovarian cancer. Cancers 2020, 12, 1470. [Google Scholar] [CrossRef]
- Anglesio, M.S.; Yong, P.J. Endometriosis-associated ovarian cancers. Clin. Obs. Gynecol. 2017, 60, 711–727. [Google Scholar] [CrossRef]
- Noe, M.; Ayhan, A.; Wang, T.L.; Shih, I.M. Independent development of endometrial epithelium and stroma within the same endometriosis. J. Pathol. 2018, 245, 265–269. [Google Scholar] [CrossRef]
- Assem, H.; Rambau, P.F.; Lee, S.; Ogilvie, T.; Sienko, A.; Kelemen, L.E.; Kobel, M. High-grade endometrioid carcinoma of the ovary: A clinicopathologic study of 30 cases. Am. J. Surg. Pathol. 2018, 42, 534–544. [Google Scholar] [CrossRef]
- Bennett, J.A.; Pesci, A.; Morales-Oyarvide, V.; Da Silva, A.; Nardi, V.; Oliva, E. Incidence of mismatch repair protein deficiency and associated clinicopathologic features in a cohort of 104 ovarian endometrioid carcinomas. Am. J. Surg. Pathol. 2019, 43, 235–243. [Google Scholar] [CrossRef]
- Choi, K.H.; Kim, H.; Bae, G.E.; Lee, S.H.; Woo, H.Y.; Kim, H.S. Mesonephric-like differentiation of ovarian endometrioid and high-grade serous carcinomas: Clinicopathological and molecular characteristics distinct from those of mesonephric-like adenocarcinoma. Anticancer Res. 2021, 41, 4587–4601. [Google Scholar] [CrossRef]
- Seay, K.; Bustamante, B.; Khutti, S.; Frimer, M. A case of non-HPV related primary endometrioid adenocarcinoma of the cervix. Gynecol. Oncol. Rep. 2020, 32, 100579. [Google Scholar] [CrossRef]
- Ren, H.; Almadani, N.; Pors, J.; Leung, S.; Ho, J.; Chow, C.; Ta, M.; Park, K.J.; Stolnicu, S.; Soslow, R.; et al. International Endocervical Adenocarcinoma Criteria and Classification (IECC): An independent cohort with clinical and molecular findings. Int. J. Gynecol. Pathol. 2021, 40, 533–540. [Google Scholar] [CrossRef]
- Hodgson, A.; Park, K.J.; Djordjevic, B.; Howitt, B.E.; Nucci, M.R.; Oliva, E.; Stolnicu, S.; Xu, B.; Soslow, R.A.; Parra-Herran, C. International Endocervical Adenocarcinoma Criteria and Classification: Validation and interobserver reproducibility. Am. J. Surg. Pathol. 2019, 43, 75–83. [Google Scholar] [CrossRef]
- Stolnicu, S.; Barsan, I.; Hoang, L.; Patel, P.; Terinte, C.; Pesci, A.; Aviel-Ronen, S.; Kiyokawa, T.; Alvarado-Cabrero, I.; Pike, M.C.; et al. International Endocervical Adenocarcinoma Criteria and Classification (IECC): A new pathogenetic classification for invasive adenocarcinomas of the endocervix. Am. J. Surg. Pathol. 2018, 42, 214–226. [Google Scholar] [CrossRef]
- Gilks, C.B.; Kommoss, F. Synchronous tumours of the female reproductive tract. Pathology 2018, 50, 214–221. [Google Scholar] [CrossRef]
- Amant, F.; Mirza, M.R.; Koskas, M.; Creutzberg, C.L. Cancer of the corpus uteri. Int. J. Gynaecol. Obs. 2018, 143 (Suppl. S2), 37–50. [Google Scholar] [CrossRef]
- WHO Classification of Tumors Editorial Board. WHO Classification of Tumours: Female Genital Tumours; IARC: Lyon, France, 2020. [Google Scholar]
- Choi, S.; Na, K.; Kim, S.W.; Kim, H.S. Dedifferentiated mesonephric-like adenocarcinoma of the uterine corpus. Anticancer Res. 2021, 41, 2719–2726. [Google Scholar] [CrossRef]
- Jung, H.; Bae, G.E.; Kim, H.M.; Kim, H.S. Clinicopathological and molecular differences between gastric-type mucinous carcinoma and usual-type endocervical adenocarcinoma of the uterine cervix. Cancer Genom. Proteom. 2020, 17, 627–641. [Google Scholar] [CrossRef]
- Koh, H.H.; Jung, Y.Y.; Kim, H.S. Clinicopathological characteristics of gastric-type endocervical adenocarcinoma misdiagnosed as an endometrial, ovarian or extragenital malignancy, or mistyped as usual-type endocervical adenocarcinoma. In Vivo 2021, 35, 2261–2273. [Google Scholar] [CrossRef]
- Lee, J.; Park, S.; Woo, H.Y.; Kim, H.S. Clinicopathological characteristics of microscopic tubal intraepithelial metastases from adenocarcinoma and small cell neuroendocrine carcinoma of the uterine cervix. In Vivo 2021, 35, 2469–2481. [Google Scholar] [CrossRef]
- Park, S.; Kim, H.S. Primary retroperitoneal mucinous carcinoma with carcinosarcomatous mural nodules: A case report with emphasis on its histological features and immunophenotype. Diagnostics 2020, 10, 580. [Google Scholar] [CrossRef]
- Yoon, N.; Kim, H.S.; Lee, J.W.; Lee, E.J.; Maeng, L.S.; Yoon, W.S. Targeted genomic sequencing reveals different evolutionary patterns between locally and distally recurrent glioblastomas. Cancer Genom. Proteom. 2020, 17, 803–812. [Google Scholar] [CrossRef]
- Choi, S.; Cho, J.; Lee, S.E.; Baek, C.H.; Kim, Y.K.; Kim, H.J.; Ko, Y.H. Adenocarcinoma of the minor salivary gland with concurrent MAML2 and EWSR1 alterations. J. Pathol. Transl. Med. 2021, 55, 132–138. [Google Scholar] [CrossRef]
- Choi, S.; Joo, J.W.; Do, S.I.; Kim, H.S. Endometrium-limited metastasis of extragenital malignancies: A challenge in the diagnosis of endometrial curettage specimens. Diagnostics 2020, 10, 150. [Google Scholar] [CrossRef]
- Choi, S.; Jung, Y.Y.; Kim, H.S. Serous carcinoma of the endometrium with mesonephric-like differentiation initially misdiagnosed as uterine mesonephric-like adenocarcinoma: A case report with emphasis on the immunostaining and the identification of splice site TP53 mutation. Diagnostics 2021, 11, 717. [Google Scholar] [CrossRef]
- Choi, S.; Park, S.; Chung, M.P.; Kim, T.S.; Cho, J.H.; Han, J. A rare case of adenosquamous carcinoma arising in the background of IgG4-related lung disease. J. Pathol. Transl. Med. 2019, 53, 188–191. [Google Scholar] [CrossRef]
- Jang, Y.; Jung, H.; Kim, H.N.; Seo, Y.; Alsharif, E.; Nam, S.J.; Kim, S.W.; Lee, J.E.; Park, Y.H.; Cho, E.Y.; et al. Clinicopathologic characteristics of HER2-positive pure mucinous carcinoma of the breast. J. Pathol. Transl. Med. 2020, 54, 95–102. [Google Scholar] [CrossRef]
- Kim, H.; Kim, J.; Lee, S.K.; Cho, E.Y.; Cho, S.Y. TFE3-expressing perivascular epithelioid cell tumor of the breast. J. Pathol. Transl. Med. 2019, 53, 62–65. [Google Scholar] [CrossRef]
- Kwon, H.J.; Song, S.Y.; Kim, H.S. Prominent papillary growth pattern and severe nuclear pleomorphism induced by neoadjuvant chemotherapy in ovarian mucinous carcinoma: Potential for misdiagnosis as high-grade serous carcinoma. Anticancer Res. 2021, 41, 1579–1586. [Google Scholar] [CrossRef]
- Kobel, M.; Ronnett, B.M.; Singh, N.; Soslow, R.A.; Gilks, C.B.; McCluggage, W.G. Interpretation of p53 immunohistochemistry in endometrial carcinomas: Toward increased reproducibility. Int. J. Gynecol. Pathol. 2019, 38, S123–S131. [Google Scholar] [CrossRef]
- McCluggage, W.G.; Hurrell, D.P.; Kennedy, K. Metastatic carcinomas in the cervix mimicking primary cervical adenocarcinoma and adenocarcinoma in situ: Report of a series of cases. Am. J. Surg. Pathol. 2010, 34, 735–741. [Google Scholar] [CrossRef]
- Stewart, C.J.; Doherty, D.A.; Havlat, M.; Koay, M.H.; Leung, Y.C.; Naran, A.; O’Brien, D.; Ruba, S.; Salfinger, S.; Tan, J. Transtubal spread of endometrial carcinoma: Correlation of intra-luminal tumour cells with tumour grade, peritoneal fluid cytology, and extra-uterine metastasis. Pathology 2013, 45, 382–387. [Google Scholar] [CrossRef] [PubMed]
- Fanning, J.; Alvarez, P.M.; Tsukada, Y.; Piver, M.S. Cervical implantation metastasis by endometrial adenocarcinoma. Cancer 1991, 68, 1335–1339. [Google Scholar] [CrossRef]
- Wang, Y.; Du, J.; Lv, S.; Sui, Y.; Xue, X.; Sun, C.; Zou, J.; Ma, Q.; Fu, G.; Song, Q.; et al. Vaginal implantation metastasis of endometrial carcinoma: A case report. Oncol. Lett. 2016, 12, 513–515. [Google Scholar] [CrossRef] [PubMed]
- Malpica, A.; Deavers, M.T. Ovarian low-grade serous carcinoma involving the cervix mimicking a cervical primary. Int. J. Gynecol. Pathol. 2011, 30, 613–619. [Google Scholar] [CrossRef]
- Stewart, C.J.R.; Crum, C.P.; McCluggage, W.G.; Park, K.J.; Rutgers, J.K.; Oliva, E.; Malpica, A.; Parkash, V.; Matias-Guiu, X.; Ronnett, B.M. Guidelines to aid in the distinction of endometrial and endocervical carcinomas, and the distinction of independent primary carcinomas of the endometrium and adnexa from metastatic spread between these and other sites. Int. J. Gynecol. Pathol. 2019, 38 (Suppl. S1), S75–S92. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Origin | Relationship with ECP | Histological Type | Number of Cases (Prevalence) |
|---|---|---|---|
| Uterine cervix | Involving ECP | HSIL | 11 (2.6%) |
| SCC | 3 (0.7%) | ||
| AIS | 2 (0.5%) | ||
| SMILE and HSIL | 1 (0.2%) | ||
| Separate | SCC | 2 (0.5%) | |
| AIS and HSIL | 1 (0.2%) | ||
| EM | Involving ECP | EC | 2 (0.5%) |
| Separate | EC | 14 (3.3%) | |
| AH/EIN | 6 (1.4%) | ||
| EC and CCC | 1 (0.2%) | ||
| SC | 1 (0.2%) | ||
| Ovary | Involving ECP | EC | 2 (0.5%) |
| Separate | HGSC | 14 (3.3%) | |
| CCC | 3 (0.7%) | ||
| EC | 2 (0.5%) | ||
| MC | 2 (0.5%) | ||
| LGSC | 1 (0.2%) | ||
| Total | 68 (15.9%) | ||
| Case No | 1 | 2 | 3 | 4 |
|---|---|---|---|---|
| Age | 33 years | 57 years | 57 years | 52 years |
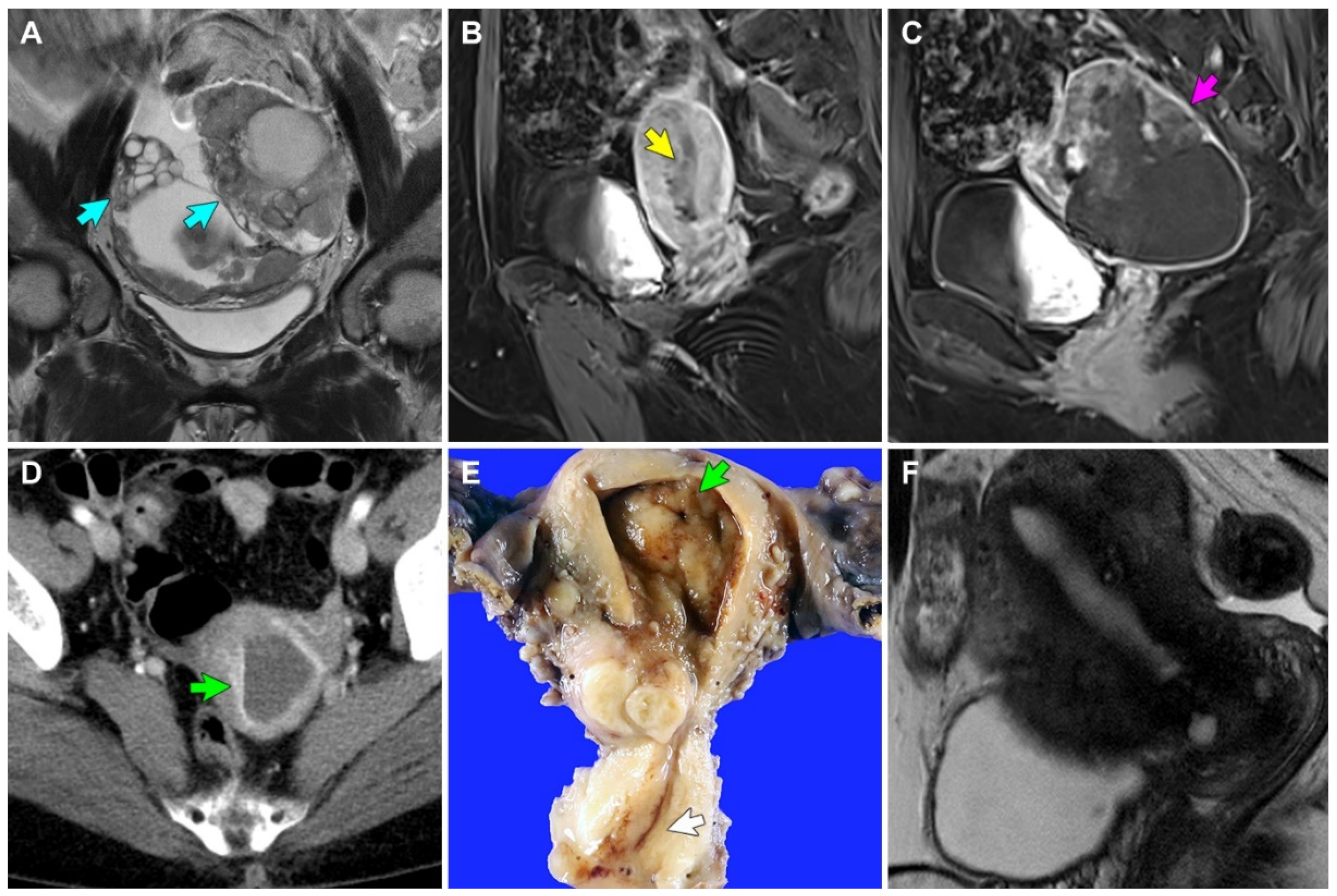
| Imaging finding | 8.6-cm solid and cystic bilateral ovarian masses; borderline-sized pelvic and retroperitoneal lymph nodes; peritoneal carcinomatosis | 8.6-cm solid and cystic left ovarian mass; 3.4-cm EM mass; enlarged retroperitoneal lymph nodes; peritoneal carcinomatosis | 1-cm EM mass; no lymph node enlargement; no peritoneal seeding | No identifiable EM lesion; no lymph node enlargement; no peritoneal seeding |
| Clinical impression | Ovarian cancer | Concurrent ovarian and EM cancers | EM cancer | MRI-invisible EM cancer |
| Neoadjuvant chemotherapy | Paclitaxel-carboplatin (three cycles) | Not received | Not received | Not received |
| Surgical procedure | TH, BSO, PLND, PALND, low anterior resection, omentectomy | TH, BSO, PLND, small bowel resection, appendectomy, omentectomy, peritonectomy | TH, BSO, PLND | TH, BSO |
| Final pathological diagnosis | Stage IIIC grade 3 EC (ovary) | Stage IIIC grade 3 EC (ovary); stage IB grade 1 EC (EM) | Stage IA grade 1 EC (EM) | Stage IA grade 1 EC (EM) |
| Greatest dimension of ECP | 17 mm | 19 mm | 11 mm | 16 mm |
| Greatest dimension of EC | 6 mm | 3 mm | 4 mm | 10 mm |
| Invasion depth into polyp stroma | 1 mm | 0.3 mm | 0.3 mm | 1 mm |
| Polypectomy resection margin involvement (safety distance) | NA | NA | Absent (5 mm) | Absent (<1 mm) |
| Post-operative treatment | Paclitaxel-carboplatin (three cycles) | Paclitaxel-carboplatin (three cycles) | Not received | Not received |
| Post-operative recurrence | Bone (sternum and rib) | Mesentery | Absent | Absent |
| Disease-free survival | 49 months | 3 months | 24 months | 15 months |
| Treatment for recurrence | Complete surgical excision | Pembrolizumab (regimen change) | Not received | Not received |
| Survival status | Alive | Alive | Alive | Alive |
| Overall survival | 67 months | 3 months | 24 months | 15 months |
| Case No | 1 | 2 | 3 | 4 | |||||
|---|---|---|---|---|---|---|---|---|---|
| ECP | Ovary | ECP | Ovary | EM | ECP | EM | ECP | EM | |
| ER | FSP | FSP | Neg | Neg | DSP | DSP | DSP | DSP | DSP |
| PR | FSP | FSP | Neg | Neg | DSP | FSP | FSP | DSP | DSP |
| p16 | PP | PP | DSP | DSP | PP | PP | PP | PP | PP |
| p53 | Mutant (CA) | Mutant (CA) | WT | WT | WT | WT | WT | WT | WT |
| Wilms tumor 1 | Neg | Neg | Neg | Neg | Neg | NA | NA | NA | NA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sohn, J.; Lee, Y.; Kim, H.-S. Endometrioid Carcinomas of the Ovaries and Endometrium Involving Endocervical Polyps: Comprehensive Clinicopathological Analyses. Diagnostics 2022, 12, 2339. https://doi.org/10.3390/diagnostics12102339
Sohn J, Lee Y, Kim H-S. Endometrioid Carcinomas of the Ovaries and Endometrium Involving Endocervical Polyps: Comprehensive Clinicopathological Analyses. Diagnostics. 2022; 12(10):2339. https://doi.org/10.3390/diagnostics12102339
Chicago/Turabian StyleSohn, Jihee, Yurimi Lee, and Hyun-Soo Kim. 2022. "Endometrioid Carcinomas of the Ovaries and Endometrium Involving Endocervical Polyps: Comprehensive Clinicopathological Analyses" Diagnostics 12, no. 10: 2339. https://doi.org/10.3390/diagnostics12102339
APA StyleSohn, J., Lee, Y., & Kim, H.-S. (2022). Endometrioid Carcinomas of the Ovaries and Endometrium Involving Endocervical Polyps: Comprehensive Clinicopathological Analyses. Diagnostics, 12(10), 2339. https://doi.org/10.3390/diagnostics12102339