

Gross Cystic Disease Fluid Protein-15 (GCDFP-15) Expression Characterizes Breast Mucinous Carcinomas in Older Women

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
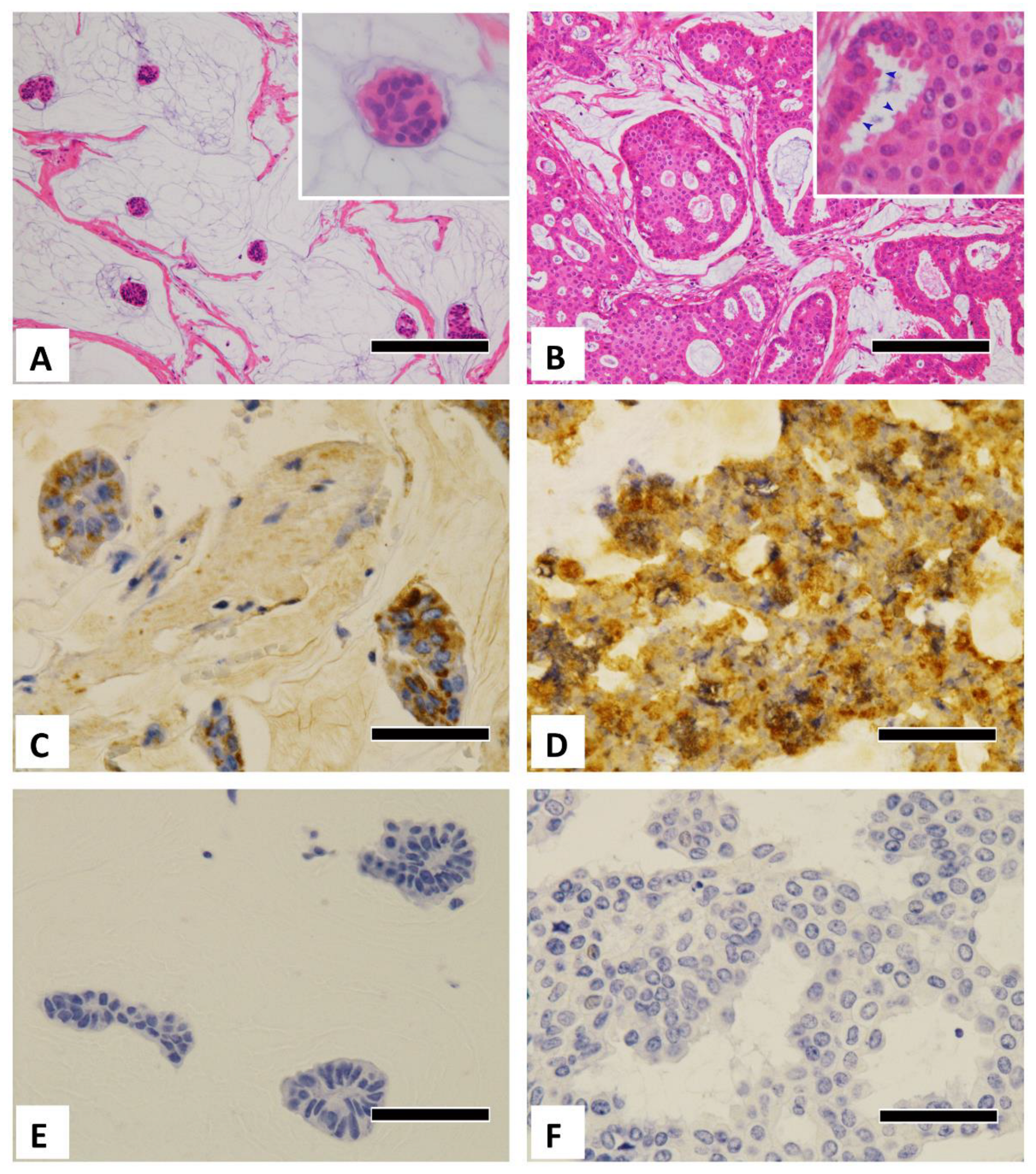
2.1. Subjects and Classification of Mucinous Carcinoma
2.2. Clinicopathological Analysis
2.3. Immunohistochemical Procedures and Evaluations
2.4. Statistical Analyses
3. Results
3.1. Clinicopathological Features
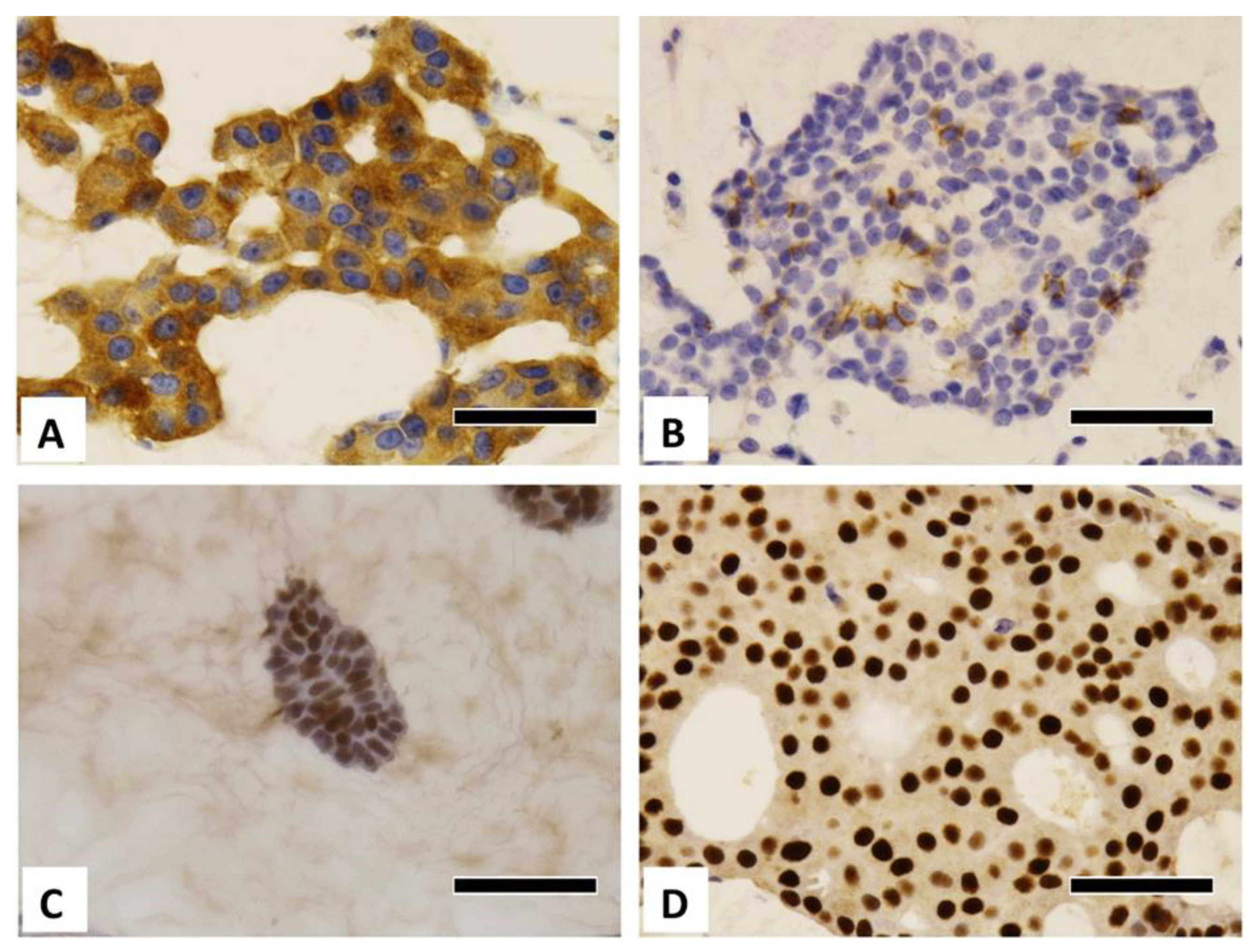
3.2. Immunohistochemical Study
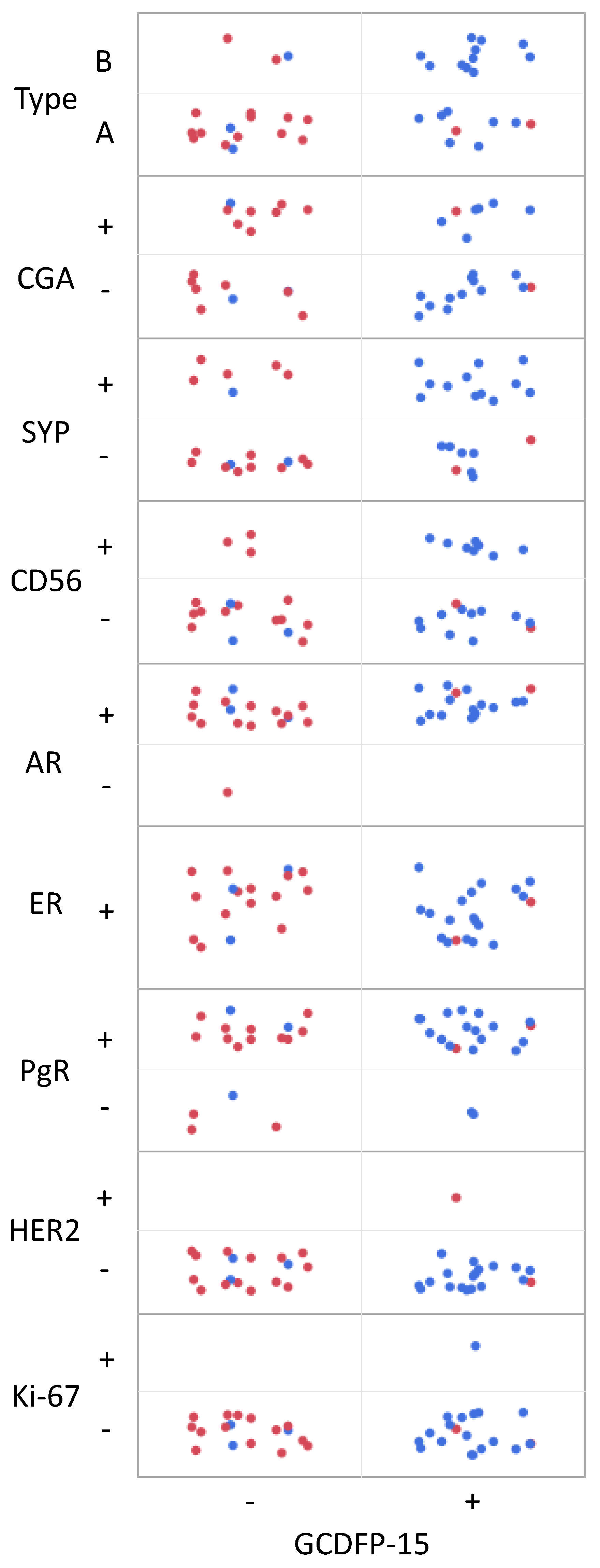
3.2.1. GCDFP-15
3.2.2. Neuroendocrine Markers
3.2.3. Steroid Hormone Receptors
3.2.4. HER2 and Ki-67 Immunostaining
3.2.5. Comparison between GCDFP-15 Expression and Other Factors
4. Discussion
4.1. Apocrine Markers (GCDFP-15/AR)
4.2. GCDFP-15 and AR/PgR Expression
4.3. Expression of Other Immunohistochemical Markers
4.4. Limitations of This Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Li, C.I.; Uribe, D.J.; Daling, J.R. Clinical Characteristics of Different Histologic Types of Breast Cancer. Br. J. Cancer 2005, 93, 1046–1052. [Google Scholar] [CrossRef] [Green Version]
- Komaki, K.; Sakamoto, G.; Sugano, H.; Morimoto, T.; Monden, Y. Mucinous Carcinoma of the Breast in Japan. A Prognostic Analysis Based on Morphologic Features. Cancer 1988, 61, 989–996. [Google Scholar] [CrossRef] [PubMed]
- Honma, N.; Sakamoto, G.; Akiyama, F.; Esaki, Y.; Sawabe, M.; Arai, T.; Hosoi, T.; Harada, N.; Younes, M.; Takubo, K. Breast Carcinoma in Women Over the Age of 85: Distinct Histological Pattern and Androgen, Oestrogen, and Progesterone Receptor Status. Histopathology 2003, 42, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Wen, H.Y.; Desmedt, C.; Reis-Filho, J.S.; Schmitt, F. Mucinous carcinoma. In Breast Tumours (WHO Classification of Tumours), 5th ed.; International Agency for Research on Cancer: Lyon, France, 2019; pp. 123–125. [Google Scholar]
- Capella, C.; Eusebi, V.; Mann, B.; Azzopardi, J.G. Endocrine Differentiation in Mucoid Carcinoma of the Breast. Histopathology 1980, 4, 613–630. [Google Scholar] [CrossRef] [PubMed]
- de Andrade Natal, R.; Derchain, S.F.; Pavanello, M.; Paiva, G.R.; Sarian, L.O.; Vassallo, J. Expression of Unusual Immunohistochemical Markers in Mucinous Breast Carcinoma. Acta Histochem. 2017, 119, 327–336. [Google Scholar] [CrossRef]
- Shirahata, H.; Honma, N.; Kotani, T.; Imaizumi, M.; Hamashima, Y.; Esaki, Y.; Kinoshita, M.; Suzuki, A.; Sakurai, U.; Arai, T. Cytological Characteristics of Mucinous Carcinoma of the Breast in the Elderly with Bibliographical Considerations (in Japanese with English Abstract). J. Jpn. Soc. Clin. Cytol. 2017, 56, 75–84. [Google Scholar] [CrossRef] [Green Version]
- Kryvenko, O.N.; Chitale, D.A.; Yoon, J.; Arias-Stella, J.; Meier, F.A.; Lee, M.W. Precursor Lesions of Mucinous Carcinoma of the Breast: Analysis of 130 Cases. Am. J. Surg. Pathol. 2013, 37, 1076–1084. [Google Scholar] [CrossRef]
- Corben, A.D.; Brogi, E. Mucinous carcinoma. In Rosen’s Breast Pathology, 4th ed.; Hoda, S.A., Brogi, E., Koemer, F.C., Rosen, P.P., Eds.; Lippincott Willams & Wilkins: Philadelphia, PA, USA, 2014; pp. 611–644. [Google Scholar]
- Budzik, M.P.; Fudalej, M.M.; Badowska-Kozakiewicz, A.M. Histopathological Analysis of Mucinous Breast Cancer Subtypes and Comparison with Invasive Carcinoma of no Special Type. Sci. Rep. 2021, 11, 5770. [Google Scholar] [CrossRef]
- Weigelt, B.; Geyer, F.C.; Horlings, H.M.; Kreike, B.; Halfwerk, H.; Reis-Filho, J.S. Mucinous and Neuroendocrine Breast Carcinomas are Transcriptionally Distinct from Invasive Ductal Carcinomas of no Special Type. Mod. Pathol. 2009, 22, 1401–1414. [Google Scholar] [CrossRef] [Green Version]
- Brierley, J.D.; Gospodarowicz, M.K.; Wittekind, C. Breast Tumours. In TNM Classification of Malignant Tumours, 8th ed.; Brierley, J.D., Gospodarowicz, M.K., Wittekind, C., Eds.; Wiley-Blackwell: Hoboken, NJ, USA, 2017; pp. 151–158. [Google Scholar]
- Tsuda, H.; Akiyama, F.; Kurosumi, M.; Sakamoto, G.; Watanabe, T. Establishment of Histological Criteria for High-Risk Node-Negative Breast Carcinoma for a Multi-Institutional Randomized Clinical Trial of Adjuvant Therapy. Japan National Surgical Adjuvant Study of Breast Cancer (NSAS-BC) Pathology Section. Jpn. J. Clin. Oncol. 1998, 28, 486–491. [Google Scholar] [CrossRef]
- Otsuki, Y.; Shimizu, S.; Suwa, K.; Yoshida, M.; Kanzaki, M.; Kobayashi, H. Which is the Better Pathological Prognostic Factor, the Nottingham Histological Grade Or the Japanese Nuclear Grade? A Large Scale Study with a Long-Term Follow-Up. Jpn. J. Clin. Oncol. 2007, 37, 266–274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fitzgibbons, P.L.; Dillon, D.A.; Alsabeh, R.; Berman, M.A.; Hayes, D.F.; Hicks, D.G.; Hughes, K.S.; Nofech-Mozes, S. Template for Reporting Results of Biomarker Testing of Specimens from Patients with Carcinoma of the Breast. Arch. Pathol. Lab. Med. 2014, 138, 595–601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soares, M.; Madeira, S.; Correia, J.; Peleteiro, M.; Cardoso, F.; Ferreira, F. Molecular Based Subtyping of Feline Mammary Carcinomas and Clinicopathological Characterization. Breast 2016, 27, 44–51. [Google Scholar] [CrossRef]
- Tsuda, H.; Akiyama, F.; Terasaki, H.; Hasegawa, T.; Kurosumi, M.; Shimadzu, M.; Yamamori, S.; Sakamoto, G. Detection of HER-2/Neu (C-Erb B-2) DNA Amplification in Primary Breast Carcinoma. Interobserver Reproducibility and Correlation with Immunohistochemical HER-2 Overexpression. Cancer 2001, 92, 2965–2974. [Google Scholar] [CrossRef] [PubMed]
- Provenzano, E.; Gatalica, Z.; Vranic, S. Carcinoma with apocrine differentiation. In Breast Tumours (WHO Classification of Tumours), 5th ed.; International Agency for Research on Cancer: Lyon, France, 2019; pp. 131–133. [Google Scholar]
- Kasashima, S.; Kawashima, A.; Zen, Y.; Ozaki, S.; Kobayashi, M.; Tsujibata, A.; Minato, H. Expression of Aberrant Mucins in Lobular Carcinoma with Histiocytoid Feature of the Breast. Virchows Arch. 2007, 450, 397–403. [Google Scholar] [CrossRef]
- Shimizu, S.; Kitamura, H.; Ito, T.; Nakamura, T.; Fujisawa, J.; Matsukawa, H. Histiocytoid Breast Carcinoma: Histological, Immunohistochemical, Ultrastructural, Cytological and Clinicopathological Studies. Pathol. Int. 1998, 48, 549–556. [Google Scholar] [CrossRef]
- Tan, P.H.; Harada, O.; Thike, A.A.; Tse, G.M. Histiocytoid Breast Carcinoma: An Enigmatic Lobular Entity. J. Clin. Pathol. 2011, 64, 654–659. [Google Scholar] [CrossRef] [Green Version]
- Striebel, J.M.; Dacic, S.; Yousem, S.A. Gross Cystic Disease Fluid Protein-(GCDFP-15): Expression in Primary Lung Adenocarcinoma. Am. J. Surg. Pathol. 2008, 32, 426–432. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.J.; Greaves, W.O.; Sabo, E.; Noble, L.; Tavares, R.; Ng, T.; DeLellis, R.A.; Resnick, M.B. GCDFP-15 Positive and TTF-1 Negative Primary Lung Neoplasms: A Tissue Microarray Study of 381 Primary Lung Tumors. Appl. Immunohistochem. Mol. Morphol. 2009, 17, 505–511. [Google Scholar] [CrossRef]
- Simpson, R.H.W.; Prasad, A.R.; Lewis, J.E.; Skálová, A.; David, L. Mucin-Rich Variant of Salivary Duct Carcinoma: A Clinicopathologic and Immunohistochemical Study of Four Cases. Am. J. Surg. Pathol. 2003, 27, 1070–1079. [Google Scholar] [CrossRef]
- Ravi, P.Y.; Walsh, N.M.; Archibald, C.; Pasternak, S. Endocrine Mucin-Producing Sweat Gland Carcinoma: Emerging Evidence of Multicentric Cutaneous Origin and Occasional Concurrence with Analogous Breast Tumors. Am. J. Dermatopathol. 2022, 44, 321–326. [Google Scholar] [CrossRef] [PubMed]
- Brogi, E. Apocrine carcinoma. In Rosen’s Breast Pathology, 4th ed.; Hoda, S., Brogi, E., Koerner, F.C., Rosen, P.P., Eds.; Wolters Kluwer Health, Inc.: Philadelphia, PA, USA, 2014; pp. 645–666. [Google Scholar]
- Loos, S.; Schulz, K.D.; Hackenberg, R. Regulation of GCDFP-15 Expression in Human Mammary Cancer Cells. Int. J. Mol. Med. 1999, 4, 135–140. [Google Scholar] [CrossRef]
- Cho, L.; Hsu, Y. Expression of Androgen, Estrogen and Progesterone Receptors in Mucinous Carcinoma of the Breast. Kaohsiung J. Med. Sci. 2008, 24, 227–232. [Google Scholar] [CrossRef] [Green Version]
- Raudrant, D.; Rabe, T. Progestogens with Antiandrogenic Properties. Drugs 2003, 63, 463–492. [Google Scholar] [CrossRef] [PubMed]
- Bardin, C.W.; Brown, T.; Isomaa, V.V.; Jänne, O.A. Progestins can Mimic, Inhibit and Potentiate the Actions of Androgens. Pharmacol. Ther. 1983, 23, 443–459. [Google Scholar] [CrossRef]
- Hankinson, S.E.; Eliassen, A.H. Endogenous Estrogen, Testosterone and Progesterone Levels in Relation to Breast Cancer Risk. J. Steroid Biochem. Mol. Biol. 2007, 106, 24–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manjer, J.; Johansson, R.; Berglund, G.; Janzon, L.; Kaaks, R.; Agren, A.; Lenner, P. Postmenopausal Breast Cancer Risk in Relation to Sex Steroid Hormones, Prolactin and SHBG (Sweden). Cancer Causes Control 2003, 14, 599–607. [Google Scholar] [CrossRef] [PubMed]
- Missmer, S.A.; Eliassen, A.H.; Barbieri, R.L.; Hankinson, S.E. Endogenous Estrogen, Androgen, and Progesterone Concentrations and Breast Cancer Risk among Postmenopausal Women. J. Natl. Cancer Inst. 2004, 96, 1856–1865. [Google Scholar] [CrossRef]
- Sieri, S.; Krogh, V.; Bolelli, G.; Abagnato, C.A.; Grioni, S.; Pala, V.; Evangelista, A.; Allemani, C.; Micheli, A.; Tagliabue, G.; et al. Sex Hormone Levels, Breast Cancer Risk, and Cancer Receptor Status in Postmenopausal Women: The ORDET Cohort. Cancer Epidemiol. Biomark. Prev. 2009, 18, 169–176. [Google Scholar] [CrossRef] [Green Version]
- Scopsi, L.; Andreola, S.; Pilotti, S.; Bufalino, R.; Baldini, M.T.; Testori, A.; Rilke, F. Mucinous Carcinoma of the Breast. A Clinicopathologic, Histochemical, and Immunocytochemical Study with Special Reference to Neuroendocrine Differentiation. Am. J. Surg. Pathol. 1994, 18, 702–711. [Google Scholar] [CrossRef]
- Dickersin, G.R.; Maluf, H.M.; Koerner, F.C. Solid Papillary Carcinoma of Breast: An Ultrastructural Study. Ultrastruct. Pathol. 1997, 21, 153–161. [Google Scholar] [CrossRef] [PubMed]
- Ng, W. Mammary Mucinous Carcinoma with Marked Cytoplasmic Hyalinization. A Report of 2 Cases with Emphasis on Fine Needle Aspiration Cytologic Findings. Acta Cytol. 2003, 47, 1045–1049. [Google Scholar] [CrossRef] [PubMed]
- Di Saverio, S.; Gutierrez, J.; Avisar, E. A Retrospective Review with Long Term Follow Up of 11.400 Cases of Pure Mucinous Breast Carcinoma. Breast Cancer Res. Treat. 2008, 111, 541–547. [Google Scholar] [CrossRef] [PubMed]
- Lacroix-Triki, M.; Suarez, P.H.; MacKay, A.; Lambros, M.B.; Natrajan, R.; Savage, K.; Geyer, F.C.; Weigelt, B.; Ashworth, A.; Reis-Filho, J.S. Mucinous Carcinoma of the Breast is Genomically Distinct from Invasive Ductal Carcinomas of no Special Type. J. Pathol. 2010, 222, 282–298. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Primary Antibody | Primary Ab (Clone Name) | Dilution | Antigen Retrieval Method | Intracellular Localization | Positive Thresholds | Supplier |
|---|---|---|---|---|---|---|
| GCDFP-15 | M (D6) | 1:700 | None | Cp | AS ≥ 4 | SIGNET |
| CGA | P | RtoU | None | Cp | AS ≥ 3 | Nichirei |
| SYP | M (27G12) | RtoU | None | Cp | AS ≥ 4 | Nichirei |
| CD56 | M (MRQ-42) | RtoU | 40 min, pH 9 | Cm | AS ≥ 3 | Nichirei |
| AR | M (AR27) | 1:25 | 40 min, pH 9 | N | AS ≥ 3 | Novocastra |
| ER | M (SPI) | RtoU | 40 min, pH 9 | N | AS ≥ 3 | Nichirei |
| PgR | M (A9621A) | RtoU | 40 min, pH 9 | N | AS ≥ 3 | Nichirei |
| HER2 | M (SV2-61γ) | Kit | None | Cm | HS ≥ 3+ | Nichirei |
| Ki-67 | M (MIB-1) | 1:200 | 40 min, pH 6 | N | LI ≥ 5% | Dako |
| Older Group (≥65 y/o) | Younger Group (<55 y/o) | Fisher’s Exact Test (p-Value) | |
|---|---|---|---|
| Number of cases | 21 | 16 | |
| Age, mean ± SD (range) | 81.7 ± 6.81 (67–92) | 44.6 ± 8.63 (28–55) | |
| T category (%) | 0.733 | ||
| T0 | 0 (0%) | 0 (0%) | |
| T1 | 7 (33.3%) | 8 (50.0%) | |
| T2 | 11 (52.4%) | 6 (37.5%) | |
| T3 | 3 (14.3%) | 2 (12.5%) | |
| T4 | 0 (0%) | 0 (0%) | |
| N stage | 1.000 | ||
| N0 | 18 (85.7%) | 14 (87.5%) | |
| N1 | 3 (14.3%) | 2 (12.5%) | |
| N2, N3 | 0 (0%) | 0 (0%) | |
| M category | |||
| M0 | 21 (100%) | 16 (100%) | |
| M1 | 0 (0%) | 0 (0%) | |
| TNM stage | 0.364 | ||
| Stage 0 | 0 (0%) | 0 (0%) | |
| Stage I | 7 (33.3%) | 8 (50%) | |
| Stage II | 13 (61.9%) | 6 (37.5%) | |
| Stage III | 1(4.8%) | 2 (12.5%) | |
| Stage IV | 0 (0%) | 0 (0%) | |
| Nuclear grade | 0.832 | ||
| Grade I | 4 (19.0%) | 4 (25.0%) | |
| Grade II | 10 (47.6%) | 8 (50.0%) | |
| Grade III | 7 (33.3%) | 4 (25.0%) |
| Median Score (Range) | Median Score (Range) | |||||
|---|---|---|---|---|---|---|
| Antibodies | Older | Younger | p-Value (Older vs. Younger) | Type A | Type B | p-Value (Type A vs. B) |
| Number of cases | 21 | 16 | 23 | 14 | ||
| GCDFP-15 | 5 (0–8) | 0 (0–5) | <0.001 | 3 (0–8) | 5.5 (0–8) | 0.014 |
| CGA | 0 (0–6) | 2.5 (0–7) | 0.046 | 2 (0–6) | 0 (2–8) | 0.394 |
| SYP | 4 (0–8) | 2 (0–8) | 0.059 | 3 (0–8) | 6 (0–8) | 0.186 |
| CD56 | 0 (0–7) | 0 (0–3) | 0.201 | 0 (0–6) | 1 (0–7) | 0.237 |
| AR | 6 (3–8) | 6 (2–7) | 0.250 | 6 (4–8) | 6 (2–8) | 0.652 |
| ER | 8 (6–8) | 7.5 (4–8) | 0.906 | 7 (4–8) | 8 (7–8) | 0.032 |
| PgR | 6 (2–8) | 7 (0–8) | 0.376 | 6 (2–8) | 5.5 (0–8) | 0.525 |
| HER2 | 0 (0–2) | 0 (0–3) | 1.000 | 0 (0–3) | 0 (0–2) | 0.904 |
| Ki-67 | 1.5 (1–30) | 1.5 (0–15) | 0.874 | 1.5 (0–10) | 1.75 (1–30) | 0.190 |
| Median Score (Range) | ||||||
|---|---|---|---|---|---|---|
| Antibodies | Older Type A (1) | Older Type B (2) | Younger Type A (3) | Younger Type B | p-Value (1) (2) (3) (KW Test) | p-Value (1) vs. (2)/(1) vs. (3) (Dunn Test) |
| Number of cases | 9 | 12 | 14 | 2 | ||
| GCDFP-15 | 5 (0–8) | 6 (3–8) | 0 (0–5) | 0, 0 | <0.001 | 1.000/0.042 |
| CGA | 0 (0–6) | 0 (0–6) | 2 (0–6) | 3, 7 | 0.124 | n.a. |
| SYP | 4 (0–8) | 5 (0–8) | 2 (0–5) | 6, 8 | 0.024 | 1.000/0.093 |
| CD56 | 0 (0–6) | 1 (0–7) | 0 (0–6) | 0, 3 | 0.545 | n.a. |
| AR | 7 (4–8) | 6 (3–8) | 6 (4–7) | 7, 2 | 0.447 | n.a. |
| ER | 7 (6–8) | 8 (7–8) | 7.5 (4–8) | 7, 8 | 0.077 | n.a. |
| PgR | 6 (2–8) | 5.5 (2–8) | 7 (2–8) | 0, 8 | 0.793 | n.a. |
| HER2 | 0 (0–1) | 0 (0–2) | 0 (0–3) | 0, 0 | 0.738 | n.a. |
| Ki-67 | 1.5 (1–5) | 1.5 (1–30) | 1.25 (0–10) | 5, 15 | 0.248 | n.a. |
| Antibodies | Older Type A (1) | Older Type B (2) | Younger Type A (3) | Younger Type B | p-Value (1) vs. (2)/(1) vs. (3) |
|---|---|---|---|---|---|
| n = 9 +/− | n = 12 +/− | n = 14 +/− | n = 2 +/− | ||
| GCDFP-15 | 7/2 | 11/1 | 2/12 | 0/2 | 0.553/0.007 |
| CGA | 4/5 | 3/9 | 6/8 | 2/0 | 0.397/1.000 |
| SYP | 6/3 | 7/5 | 3/11 | 2/0 | 1.000/0.077 |
| CD56 | 3/6 | 5/7 | 2/12 | 1/1 | 1.000/0.343 |
| AR | 8/0 | 10/0 | 14/0 | 1/1 | 1.000/1.000 |
| ER | 9/0 | 12/0 | 14/0 | 2/0 | 1.000/1.000 |
| PgR | 8/1 | 10/2 | 12/2 | 1/1 | 1.000/1.000 |
| HER2 | 0/9 | 0/12 | 1/13 | 0/2 | 1.000/1.000 |
| Ki-67 | 1/8 | 3/9 | 4/10 | 2/0 | 0.603/0.611 |
| Study | Group | Number of Cases | Mean Age | ER | PgR | HER2 | Ki-67 | Ki-67 Threshold |
|---|---|---|---|---|---|---|---|---|
| Our study | Older (67–92 y/o) | 21 | 81.7 | 100% | 85.7% | 0% | 19% | 5% |
| Younger (28–55 y/o) | 16 | 44.6 | 100% | 81.3% | 6.3% | 37.5% | 5% | |
| Li et al. [1] | 50–89 y/o | 2730 | n.a. | 96% | 83% | n.a. | n.a. | n.a. |
| 30–49 y/o | 516 | n.a. | 91% | 81% | n.a. | n.a. | n.a. | |
| Di Saverio et al. [38] | 25–85 y/o | 11422 | 68.3 | 94.1% | 81.5% | n.a. | n.a. | n.a. |
| de Andrade Natal et al. [6] | Type A | 17 | 57.0 | 100% | 52.9% | 5.9% | 0% | 14% |
| Type B | 23 | 66.0 | 95.7% | 73.9% | 4.3% | 21.7% | 14% | |
| Lacroix-Triki et al. [39] | 35 | n.a. | 100% | 85.7% | 2.9% | 8.6% | 10% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kinoshita, M.; Sawabe, M.; Soejima, Y.; Mieno, M.N.; Arai, T.; Honma, N. Gross Cystic Disease Fluid Protein-15 (GCDFP-15) Expression Characterizes Breast Mucinous Carcinomas in Older Women. Diagnostics 2022, 12, 3129. https://doi.org/10.3390/diagnostics12123129
Kinoshita M, Sawabe M, Soejima Y, Mieno MN, Arai T, Honma N. Gross Cystic Disease Fluid Protein-15 (GCDFP-15) Expression Characterizes Breast Mucinous Carcinomas in Older Women. Diagnostics. 2022; 12(12):3129. https://doi.org/10.3390/diagnostics12123129
Chicago/Turabian StyleKinoshita, Mayumi, Motoji Sawabe, Yurie Soejima, Makiko Naka Mieno, Tomio Arai, and Naoko Honma. 2022. "Gross Cystic Disease Fluid Protein-15 (GCDFP-15) Expression Characterizes Breast Mucinous Carcinomas in Older Women" Diagnostics 12, no. 12: 3129. https://doi.org/10.3390/diagnostics12123129
APA StyleKinoshita, M., Sawabe, M., Soejima, Y., Mieno, M. N., Arai, T., & Honma, N. (2022). Gross Cystic Disease Fluid Protein-15 (GCDFP-15) Expression Characterizes Breast Mucinous Carcinomas in Older Women. Diagnostics, 12(12), 3129. https://doi.org/10.3390/diagnostics12123129