
Application of the Interaction between Tissue Immunohistochemistry Staining and Clinicopathological Factors for Evaluating the Risk of Oral Cancer Progression by Hierarchical Clustering Analysis: A Case-Control Study in a Taiwanese Population

 , , ,
, , , 
Abstract
1. Introduction
2. Materials and Methods
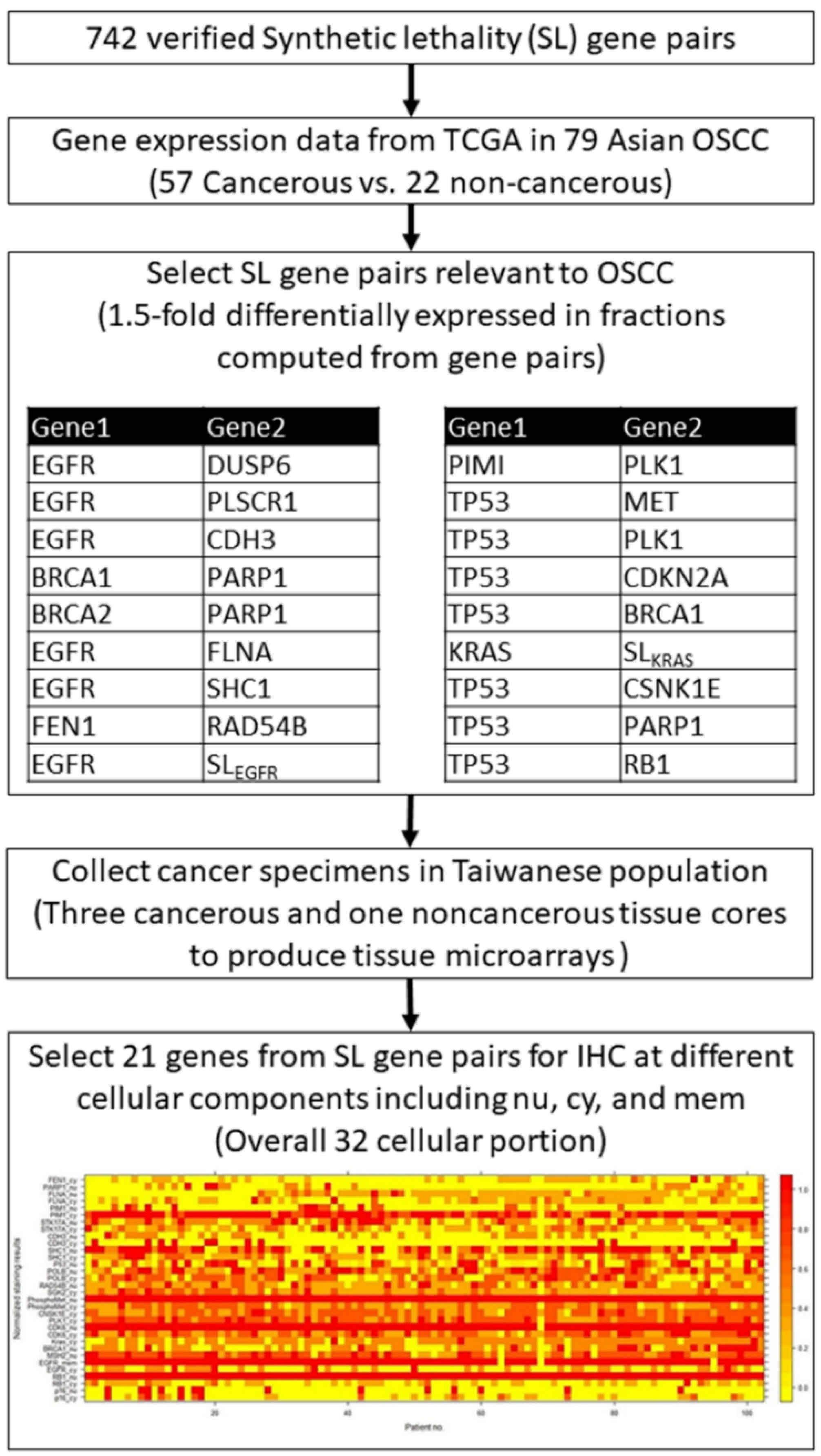
2.1. Data Set
2.2. Computation of Gene Expression Profiles for Oral Cavity Cancer versus Non-Cancerous Tissues
2.3. Protein Staining
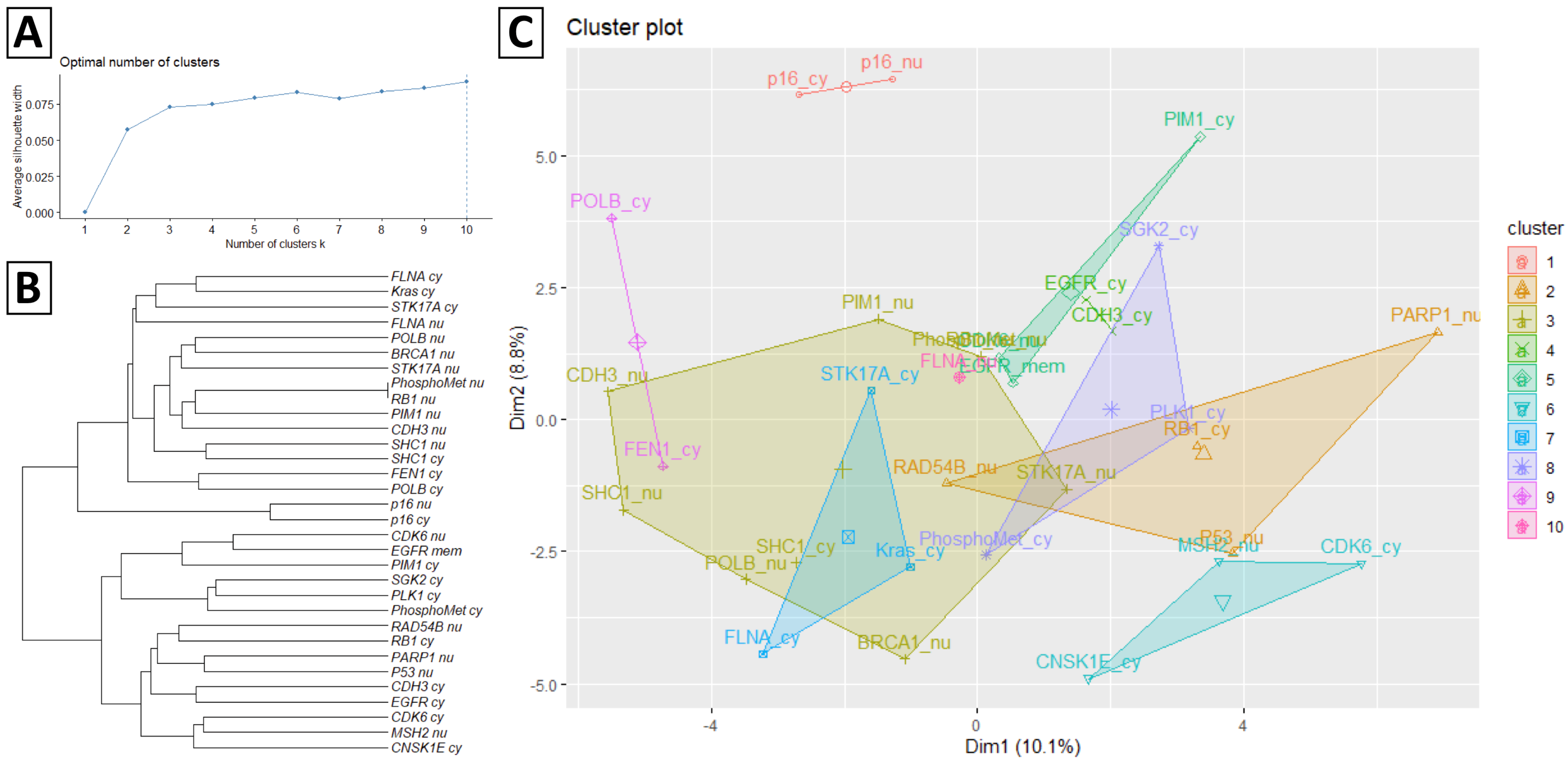
2.4. Ward’s Agglomerative Hierarchical Clustering
2.5. OCPRS
2.6. Statistical Analyses
3. Results
3.1. Clinicopathological Characteristics and Progression of Oral Cancer
3.2. Hierarchical Clustering Analysis of the Optimal Combination of Protein Staining
3.3. Hierarchical Clustering Results of Protein Staining
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Parkin, D.M.; Bray, F.; Ferlay, J.; Pisani, P. Global cancer statistics, 2002. CA Cancer J. Clin. 2005, 55, 74–108. [Google Scholar] [CrossRef]
- Jadhav, K.B.; Gupta, N. Clinicopathological prognostic implicators of oral squamous cell carcinoma: Need to understand and revise. N. Am. J. Med. Sci. 2013, 5, 671. [Google Scholar] [CrossRef] [PubMed]
- Irani, S. Distant metastasis from oral cancer: A review and molecular biologic aspects. J. Int. Soc. Prev. Community Dent. 2016, 6, 265. [Google Scholar] [CrossRef] [PubMed]
- Takes, R.P.; Rinaldo, A.; Silver, C.E.; Haigentz, M., Jr.; Woolgar, J.A.; Triantafyllou, A.; Mondin, V.; Paccagnella, D.; De Bree, R.; Shaha, A.R. Distant metastases from head and neck squamous cell carcinoma. Part I. Basic aspects. Oral Oncol. 2012, 48, 775–779. [Google Scholar] [CrossRef] [PubMed]
- Ko, Y.C.; Huang, Y.L.; Lee, C.H.; Chen, M.J.; Lin, L.M.; Tsai, C.C. Betel quid chewing, cigarette smoking and alcohol consumption related to oral cancer in Taiwan. J. Oral Pathol. Med. 1995, 24, 450–453. [Google Scholar] [CrossRef]
- Chen, P.-H.; Lee, K.-W.; Hsu, C.-C.; Chen, J.Y.-F.; Wang, Y.-H.; Chen, K.-K.; Wang, H.-M.D.; Huang, H.-W.; Huang, B. Expression of a splice variant of CYP26B1 in betel quid-related oral cancer. Sci. World J. 2014, 2014. [Google Scholar] [CrossRef]
- Hsieh, L.-L.; Chien, H.-T.; Chen, I.-H.; Liao, C.-T.; Wang, H.-M.; Jung, S.-M.; Wang, P.-F.; Chang, J.T.-C.; Chen, M.-C.; Cheng, A.-J. The XRCC1 399Gln polymorphism and the frequency of p53 mutations in Taiwanese oral squamous cell carcinomas. Cancer Epidemiol. Prev. Biomark. 2003, 12, 439–443. [Google Scholar]
- Choi, K.Y.; Rho, Y.S.; Kwon, K.H.; Chung, E.J.; Kim, J.H.; Park, I.S.; Lee, D.J. ECRG1 and FGFR4 single nucleotide polymorphism as predictive factors for nodal metastasis in oral squamous cell carcinoma. Cancer Biomark. 2013, 12, 115–124. [Google Scholar] [CrossRef]
- Chen, T.-W.; Lee, C.-C.; Liu, H.; Wu, C.-S.; Pickering, C.R.; Huang, P.-J.; Wang, J.; Chang, I.Y.-F.; Yeh, Y.-M.; Chen, C.-D. APOBEC3A is an oral cancer prognostic biomarker in Taiwanese carriers of an APOBEC deletion polymorphism. Nat. Commun. 2017, 8, 465. [Google Scholar] [CrossRef]
- Ohshima, M.; Sugahara, K.; Kasahara, K.; Katakura, A. Metabolomic analysis of the saliva of Japanese patients with oral squamous cell carcinoma. Oncol. Rep. 2017, 37, 2727–2734. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.J.; Chang, K.W.; Chao, S.Y.; Kwan, P.C.; Chang, S.M.; Yen, R.Y.; Wang, C.Y.; Wong, Y.K. The molecular markers for prognostic evaluation of areca-associated buccal squamous cell carcinoma. J. Oral Pathol. Med. 2004, 33, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Arora, S.; Kaur, J.; Sharma, C.; Mathur, M.; Bahadur, S.; Shukla, N.K.; Deo, S.V.; Ralhan, R. Stromelysin 3, Ets-1, and vascular endothelial growth factor expression in oral precancerous and cancerous lesions: Correlation with microvessel density, progression, and prognosis. Clin. Cancer Res. 2005, 11, 2272–2284. [Google Scholar] [CrossRef]
- Shah, N.; Trivedi, T.; Tankshali, R.; Goswami, J.; Shah, J.; Jetly, D.; Kobawala, T.; Patel, K.; Shukla, S.; Shah, P. Molecular alterations in oral carcinogenesis: Significant risk predictors in malignant transformation and tumor progression. Int. J. Biol. Markers 2007, 22, 132–143. [Google Scholar] [CrossRef] [PubMed]
- Wicker, C.A.; Takiar, V.; Suganya, R.; Arnold, S.M.; Brill, Y.M.; Chen, L.; Horbinski, C.M.; Napier, D.; Valentino, J.; Kudrimoti, M.R. Evaluation of antioxidant network proteins as novel prognostic biomarkers for head and neck cancer patients. Oral Oncol. 2020, 111, 104949. [Google Scholar] [CrossRef]
- Sá, M.C.; Conceição, T.S.; de Moura Santos, E.; De Morais, E.F.; Galvão, H.C.; de Almeida Freitas, R. Immunohistochemical expression of TFIIH and XPF in oral tongue squamous cell carcinoma. Eur. Arch. OtoRhinoLaryngol. 2020, 277, 893–902. [Google Scholar] [CrossRef]
- Vasan, K.; Satgunaseelan, L.; Anand, S.; Asher, R.; Selinger, C.; Low, T.-H.H.; Palme, C.E.; Clark, J.R.; Gupta, R. Tumour mismatch repair protein loss is associated with advanced stage in oral cavity squamous cell carcinoma. Pathology 2019, 51, 688–695. [Google Scholar] [CrossRef]
- Kimes, P.K.; Liu, Y.; Neil Hayes, D.; Marron, J.S. Statistical significance for hierarchical clustering. Biometrics 2017, 73, 811–821. [Google Scholar] [CrossRef]
- Eisen, M.B.; Spellman, P.T.; Brown, P.O.; Botstein, D. Cluster analysis and display of genome-wide expression patterns. Proc. Natl. Acad. Sci. 1998, 95, 14863–14868. [Google Scholar] [CrossRef]
- Cho, Y.R.; Hwang, W.C.; Ramanathan, M.; Zhang, A.D. Semantic integration to identify overlapping functional modules in protein interaction networks. BMC Bioinform. 2007, 8, 1–13. [Google Scholar] [CrossRef]
- Kaisers, W.; Schwender, H.; Schaal, H. Hierarchical Clustering of DNA k-mer Counts in RNAseq Fastq Files Identifies Sample Heterogeneities. Int. J. Mol. Sci. 2018, 19, 3687. [Google Scholar] [CrossRef]
- Wang, J.X.; Li, M.; Chen, J.E.; Pan, Y. A Fast Hierarchical Clustering Algorithm for Functional Modules Discovery in Protein Interaction Networks. IEEE ACM Trans. Comput. Biol. Bioinform. 2011, 8, 607–620. [Google Scholar] [CrossRef] [PubMed]
- Perou, C.M.; Sørlie, T.; Eisen, M.B.; Van De Rijn, M.; Jeffrey, S.S.; Rees, C.A.; Pollack, J.R.; Ross, D.T.; Johnsen, H.; Akslen, L.A. Molecular portraits of human breast tumours. Nature 2000, 406, 747–752. [Google Scholar] [CrossRef]
- Bhattacharjee, A.; Richards, W.G.; Staunton, J.; Li, C.; Monti, S.; Vasa, P.; Ladd, C.; Beheshti, J.; Bueno, R.; Gillette, M. Classification of human lung carcinomas by mRNA expression profiling reveals distinct adenocarcinoma subclasses. Proc. Natl. Acad. Sci. USA 2001, 98, 13790–13795. [Google Scholar] [CrossRef] [PubMed]
- Chauhan, S.; Kaur, J.; Kumar, M.; Matta, A.; Srivastava, G.; Alyass, A.; Assi, J.; Leong, I.; MacMillan, C.; Witterick, I. Prediction of recurrence-free survival using a protein expression-based risk classifier for head and neck cancer. Oncogenesis 2015, 4, e147. [Google Scholar] [CrossRef]
- Network, C.G.A. Comprehensive genomic characterization of head and neck squamous cell carcinomas. Nature 2015, 517, 576. [Google Scholar] [CrossRef]
- Edgar, R.; Domrachev, M.; Lash, A.E. Gene Expression Omnibus: NCBI gene expression and hybridization array data repository. Nucleic Acids Res. 2002, 30, 207–210. [Google Scholar] [CrossRef] [PubMed]
- Peng, C.-H.; Liao, C.-T.; Peng, S.-C.; Chen, Y.-J.; Cheng, A.-J.; Juang, J.-L.; Tsai, C.-Y.; Chen, T.-C.; Chuang, Y.-J.; Tang, C.-Y. A novel molecular signature identified by systems genetics approach predicts prognosis in oral squamous cell carcinoma. PLoS ONE 2011, 6, e23452. [Google Scholar] [CrossRef]
- Forster, M.; Mendes, R.; Fedele, S. Synthetic lethality and PARP-inhibitors in oral and head & neck cancer. Curr. Pharm. Des. 2012, 18, 5431–5441. [Google Scholar]
- Lee, J.S.; Das, A.; Jerby-Arnon, L.; Arafeh, R.; Auslander, N.; Davidson, M.; McGarry, L.; James, D.; Amzallag, A.; Park, S.G. Harnessing synthetic lethality to predict the response to cancer treatment. Nat. Commun. 2018, 9, 1–12. [Google Scholar] [CrossRef]
- Tiong, K.-L.; Chang, K.-C.; Yeh, K.-T.; Liu, T.-Y.; Wu, J.-H.; Hsieh, P.-H.; Lin, S.-H.; Lai, W.-Y.; Hsu, Y.-C.; Chen, J.-Y. CSNK1E/CTNNB1 are synthetic lethal to TP53 in colorectal cancer and are markers for prognosis. Neoplasia 2014, 16, 441–450. [Google Scholar] [CrossRef][Green Version]
- Chang, J.-G.; Chen, C.-C.; Wu, Y.-Y.; Che, T.-F.; Huang, Y.-S.; Yeh, K.-T.; Shieh, G.S.; Yang, P.-C. Uncovering synthetic lethal interactions for therapeutic targets and predictive markers in lung adenocarcinoma. Oncotarget 2016, 7, 73664. [Google Scholar] [CrossRef]
- Wang, H.-C.; Chiang, C.-J.; Liu, T.-C.; Wu, C.-C.; Chen, Y.-T.; Chang, J.-G.; Shieh, G.-S. Immunohistochemical Expression of Five Protein Combinations Revealed as Prognostic Markers in Asian Oral Cancer. Front. Genet. 2021, 12. [Google Scholar] [CrossRef]
- Amin, M.B.; Edge, S.B. AJCC Cancer Staging Manual; Springer: Berlin/Heidelberg, Germany, 2017. [Google Scholar]
- Brierley, J.; Gospodarowicz, M.; Wittekind, C. Cervix Uteri. TNM Classification of Malignant Tumors; Wiley-Blackwell: Chichester, UK, 2017. [Google Scholar]
- Al-Dabooni, S.; Wunsch, D. Model Order Reduction Based on Agglomerative Hierarchical Clustering. IEEE Trans. Neural Netw. Learn Syst. 2019, 30, 1881–1895. [Google Scholar] [CrossRef] [PubMed]
- Hanif, T.; Laulajainen-Hongisto, A.; Luukkainen, A.; Numminen, J.; Kaariainen, J.; Myller, J.; Kalogjera, L.; Huhtala, H.; Kankainen, M.; Renkonen, R.; et al. Hierarchical clustering in evaluating inflammatory upper airway phenotypes; increased symptoms in adults with allergic multimorbidity. Asian Pac. J. Allergy Immunol. 2019, 38, 239–250. [Google Scholar]
- Hoffmann, J.; Fiser, K.; Liebetrau, C.; Staubach, N.; Kost, D.; Voss, S.; Heiden, A.Z.; Dorr, O.; Lipps, C.; Nef, H.M.; et al. High-Content Immunophenotyping and Hierarchical Clustering Reveal Sources of Heterogeneity and New Surface Markers of Human Blood Monocyte Subsets. Thromb. Haemost 2020, 120, 141–155. [Google Scholar] [CrossRef]
- Huang, S.-F.; Chien, H.-T.; Chuang, W.-Y.; Lai, C.-H.; Cheng, S.-D.; Liao, C.-T.; Wang, H.-M. Epidermal growth factor receptor intron-1 CA repeat polymorphism on protein expression and clinical outcome in Taiwanese oral squamous cell carcinoma. Sci. Rep. 2017, 7, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Cao, R.; Wu, Q.; Li, Q.; Yao, M.; Zhou, H. A 3-mRNA-based prognostic signature of survival in oral squamous cell carcinoma. PeerJ 2019, 7, e7360. [Google Scholar] [CrossRef]
- Ditsch, N.; Heublein, S.; Jeschke, U.; Sattler, C.; Kuhn, C.; Hester, A.; Czogalla, B.; Trillsch, F.; Mahner, S.; Engel, J. Cytoplasmic versus nuclear THR alpha expression determines survival of ovarian cancer patients. J. Cancer Res. Clin. Oncol. 2020, 146, 1923–1932. [Google Scholar] [CrossRef]
- Seraya-Bareket, C.; Weisz, A.; Shinderman-Maman, E.; Teper-Roth, S.; Stamler, D.; Arbib, N.; Kadan, Y.; Fishman, A.; Kidron, D.; Edelstein, E. The identification of nuclear αvβ3 integrin in ovarian cancer: Non-paradigmal localization with cancer promoting actions. Oncogenesis 2020, 9, 1–12. [Google Scholar] [CrossRef]
- Wells, A.; Marti, U. Signalling shortcuts: Cell-surface receptors in the nucleus? Nat. Rev. Mol. Cell Biol. 2002, 3, 697–702. [Google Scholar] [CrossRef]
- Cohen, E.R.; Reis, I.M.; Gomez-Fernandez, C.; Smith, D.; Pereira, L.; Freiser, M.E.; Marotta, G.; Thomas, G.R.; Sargi, Z.B.; Franzmann, E.J. CD44 and associated markers in oral rinses and tissues from oral and oropharyngeal cancer patients. Oral Oncol. 2020, 106, 104720. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Zhang, Q.; Zhang, M.; Luo, Y.; Fu, Y. Downregulation of nuclear ING3 expression and translocalization to cytoplasm promotes tumorigenesis and progression in head and neck squamous cell carcinoma (HNSCC). Histol. Histopathol. 2019, 35, 681–690. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | n (%) |
|---|---|
| Cases | 102 |
| Age, mean ± SD | 55.1 ± 10.4 |
| Sex | |
| Female | 6 (5.9%) |
| Male | 96 (94.1%) |
| Alcohol | 37 (36.3%) |
| Betel | 75 (73.5%) |
| Cigarette | 87 (85.3%) |
| Site | |
| Non-buccal | 42 (41.2%) |
| Buccal | 60 (58.8%) |
| Grade | |
| 1 | 48 (47.1%) |
| 2 | 52 (51%) |
| 3 | 2 (2%) |
| LVI | 10 (9.8%) |
| PNI | 13 (12.7%) |
| Margin not free | 6 (5.9%) |
| ENE | 9 (8.8%) |
| Tumor size (cm), mean ± SD | 2.4 ± 1.5 |
| Lymph node invasion | |
| Positive | 76 (74.5%) |
| Negative | 26 (25.5%) |
| Pathological stage | |
| I–II | 61 (59.8%) |
| III–IV | 41 (40.2%) |
| Death | 26 (25.5%) |
| Progressed | 36 (35.3%) |
| No | Cluster | High-Risk Strata | n a (%) | n b (%) | Low-Risk Strata | n a (%) | n b (%) | pa | pb |
|---|---|---|---|---|---|---|---|---|---|
| 1 | p16_cy, p16_nu | 88 | 29 (80.6%) | 23 (88.5%) | 14 | 7 (19.4%) | 3 (11.5%) | 0.182 | 0.764 |
| 2 | RB1_cy, RAD54B_nu, P53_nu, PARP1_nu | 49 | 20 (55.6%) | 15 (57.7%) | 53 | 16 (44.4%) | 11 (42.3%) | 0.341 | 0.350 |
| 3 | RB1_nu, BRCA1_nu, PhosphoMet_nu, POLB_nu, SHC1_cy, SHC1_nu, CDH3_nu, STK17A_nu, PIM1_nu | 64 | 25 (69.4%) | 19 (73.1%) | 38 | 11 (30.6%) | 7 (26.9%) | 0.427 | 0.283 |
| 4 | EGFR_cy, CDH3_cy | 91 | 34 (94.4%) | 25 (96.2%) | 11 | 2 (5.6%) | 1 (3.8%) | 0.151 | 0.212 |
| 5 | EGFR_mem, CDK6_nu, PIM1_cy | 101 | 36 (100%) | 25 (96.2%) | 1 | 0 (0%) | 1 (3.8%) | 0.619 | 0.015 * |
| 6 | MSH2_nu, CDK6_cy, CNSK1E_cy | 68 | 22 (61.1%) | 16 (61.5%) | 34 | 14 (38.9%) | 10 (38.5%) | 0.161 | 0.354 |
| 7 | Kras_cy, STK17A_cy, FLNA_cy | 85 | 27 (75.0%) | 20 (76.9%) | 17 | 9 (25.0%) | 6 (23.1%) | 0.087 | 0.354 |
| 8 | PLK1_cy, PhosphoMet_cy, SGK2_cy | 53 | 25 (69.4%) | 17 (65.4%) | 49 | 11 (30.6%) | 9 (34.6%) | 0.012 * | 0.152 |
| 9 | POLB_cy, FEN1_cy | 66 | 25 (69.4%) | 18 (69.2%) | 36 | 11 (30.6%) | 8 (30.8%) | 0.279 | 0.379 |
| 10 | FLNA_nu | 64 | 22 (61.1%) | 18 (69.2%) | 38 | 14 (38.9%) | 8 (30.8%) | 0.649 | 0.644 |
| Predictors | Comparison | Univariate | Multivariate | ||
|---|---|---|---|---|---|
| HR (95%CI) | p | HR (95%CI) | p | ||
| 8th protein staining cluster | High vs. low-risk | 2.41 (1.19–4.91) | 0.015 * | 2.33 (1.14–4.75) | 0.020 * |
| Age | Years | 1.01 (0.98–1.04) | 0.500 | - | |
| Sex | Male vs. female | 1.17 (0.28–4.88) | 0.828 | - | |
| Alcohol | Yes vs. no | 1.01 (0.51–2.00) | 0.971 | - | |
| Betel | Yes vs. no | 0.78 (0.38–1.58) | 0.487 | - | |
| Cigarrate | Yes vs. no | 0.86 (0.36–2.07) | 0.735 | - | |
| Site | Buccal vs. non-buccal | 1.44 (0.73–2.85) | 0.290 | - | |
| Grade | Grade 2–3 vs. 1 | 2.03 (1.02–4.01) | 0.043 * | 1.85 (0.93–3.67) | 0.079 |
| LVI | Yes vs. no | 1.92 (0.75–4.95) | 0.176 | - | |
| PNI | Yes vs. no | 1.99 (0.87–4.55) | 0.104 | - | |
| Margin | Not free vs. free | 1.59 (0.49–5.20) | 0.443 | - | |
| ECS | Yes vs. no | 2.87 (1.11–7.46) | 0.030 * | 2.66 (1.02–6.95) | 0.045 * |
| Tumor size | cm | 1.02 (0.81–1.28) | 0.863 | - | |
| Lymph node invasion | Positive vs. negative | 1.30 (0.63–2.70) | 0.479 | - | |
| Pathological stage | III–IV vs. I–II | 1.71 (0.89–3.30) | 0.109 | - | |
| Predictors | Comparison | Univariate | Multivariate | ||
|---|---|---|---|---|---|
| HR (95%CI) | p | HR (95%CI) | p | ||
| 8th protein staining cluster | High vs. low-risk | 1.79 (0.80–4.02) | 0.157 | - | |
| Age | Years | 1.00 (0.96–1.04) | 0.868 | - | |
| Sex | Male vs. female | 1.61 (0.22–11.91) | 0.640 | - | |
| Alcohol | Yes vs. no | 1.82 (0.73–4.53) | 0.200 | - | |
| Betel | Yes vs. no | 0.52 (0.23–1.14) | 0.100 | - | |
| Cigarrate | Yes vs. no | 2.08 (0.49–8.81) | 0.319 | - | |
| Site | Buccal vs. non-buccal | 1.09 (0.50–2.38) | 0.824 | - | |
| Grade | Grade 2–3 vs. 1 | 3.65 (1.46–9.10) | 0.006 * | 3.05 (1.17–7.90) | 0.022 * |
| LVI | Yes vs. no | 2.19 (0.75–6.38) | 0.151 | ||
| PNI | Yes vs. no | 3.84 (1.66–8.89) | 0.002 * | 2.31 (0.82–6.47) | 0.111 |
| Margin | Not free vs. free | 2.09 (0.63–6.96) | 0.232 | ||
| ECS | Yes vs. no | 6.94 (2.71–17.82) | <0.001 * | 3.46 (1.05–11.41) | 0.042 * |
| Tumor size | cm | 1.38 (1.13–1.70) | 0.002 * | 1.16 (0.86–1.55) | 0.334 |
| Lymph node invasion | Positive vs. negative | 3.14 (1.45–6.81) | 0.004 * | 0.87 (0.26–2.96) | 0.829 |
| Pathological stage | III–IV vs. I–II | 3.13 (1.39–7.02) | 0.006 * | 1.45 (0.42–4.98) | 0.557 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, H.-C.; Chou, M.-C.; Wu, C.-C.; Chan, L.-P.; Moi, S.-H.; Pan, M.-R.; Liu, T.-C.; Yang, C.-H. Application of the Interaction between Tissue Immunohistochemistry Staining and Clinicopathological Factors for Evaluating the Risk of Oral Cancer Progression by Hierarchical Clustering Analysis: A Case-Control Study in a Taiwanese Population. Diagnostics 2021, 11, 925. https://doi.org/10.3390/diagnostics11060925
Wang H-C, Chou M-C, Wu C-C, Chan L-P, Moi S-H, Pan M-R, Liu T-C, Yang C-H. Application of the Interaction between Tissue Immunohistochemistry Staining and Clinicopathological Factors for Evaluating the Risk of Oral Cancer Progression by Hierarchical Clustering Analysis: A Case-Control Study in a Taiwanese Population. Diagnostics. 2021; 11(6):925. https://doi.org/10.3390/diagnostics11060925
Chicago/Turabian StyleWang, Hui-Ching, Meng-Chun Chou, Chun-Chieh Wu, Leong-Perng Chan, Sin-Hua Moi, Mei-Ren Pan, Ta-Chih Liu, and Cheng-Hong Yang. 2021. "Application of the Interaction between Tissue Immunohistochemistry Staining and Clinicopathological Factors for Evaluating the Risk of Oral Cancer Progression by Hierarchical Clustering Analysis: A Case-Control Study in a Taiwanese Population" Diagnostics 11, no. 6: 925. https://doi.org/10.3390/diagnostics11060925
APA StyleWang, H.-C., Chou, M.-C., Wu, C.-C., Chan, L.-P., Moi, S.-H., Pan, M.-R., Liu, T.-C., & Yang, C.-H. (2021). Application of the Interaction between Tissue Immunohistochemistry Staining and Clinicopathological Factors for Evaluating the Risk of Oral Cancer Progression by Hierarchical Clustering Analysis: A Case-Control Study in a Taiwanese Population. Diagnostics, 11(6), 925. https://doi.org/10.3390/diagnostics11060925