
Diagnostic Added-Value of Serum CA-125 on the IOTA Simple Rules and Derivation of Practical Combined Prediction Models (IOTA SR X CA-125)

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Design and Setting
2.2. Study Patients and Data Collection
2.3. The IOTA Simple Rules
2.4. Reference Standard
2.5. Statistical Analysis
2.5.1. Evaluation of Diagnostic Added-Value
2.5.2. Prediction Model Development
2.5.3. Prediction Model Performance
2.5.4. Diagnostic Accuracy of the Models
3. Results
3.1. Baseline Characteristics of the Study Patients
3.2. The Added-Value of CA-125
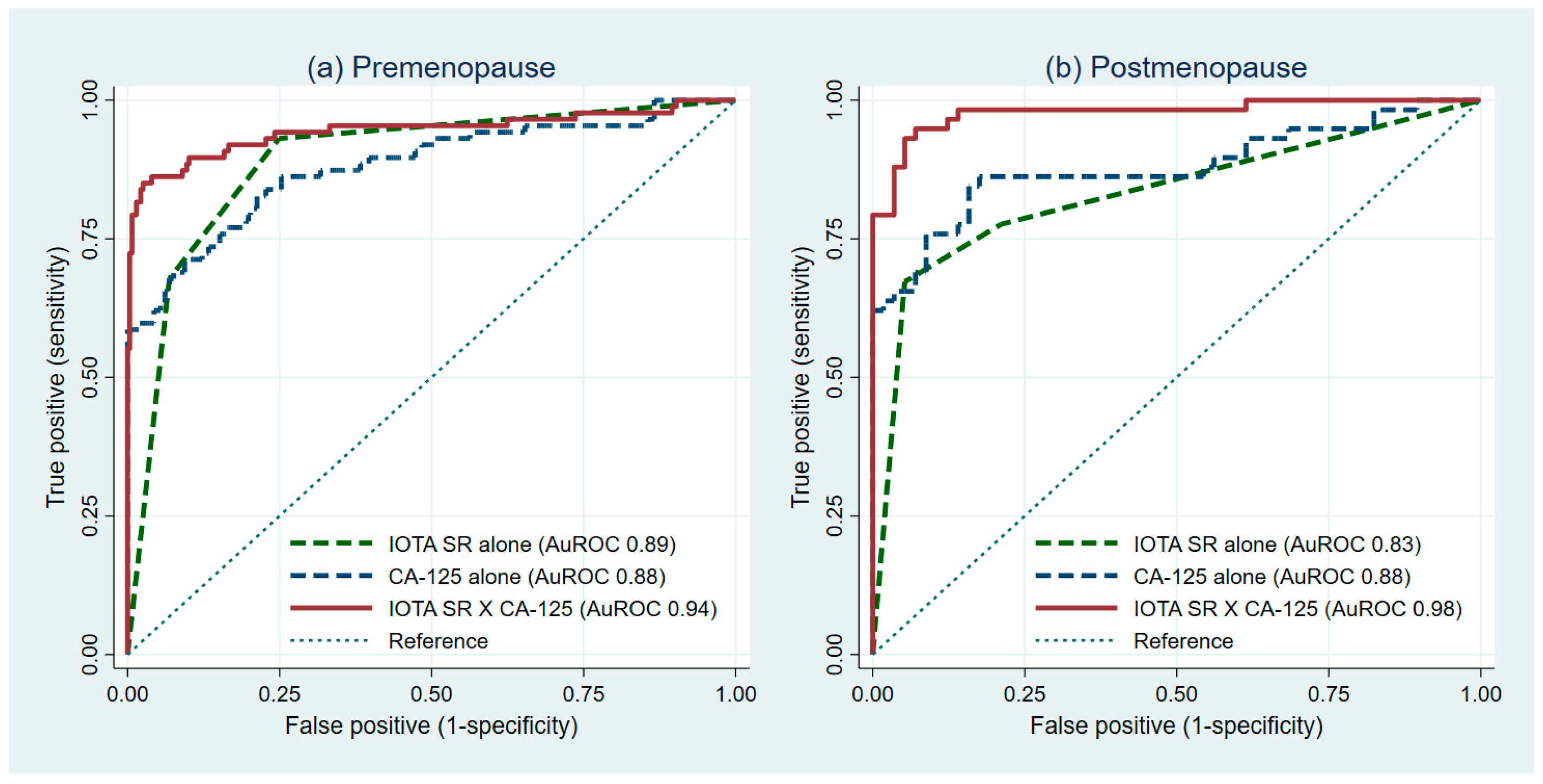
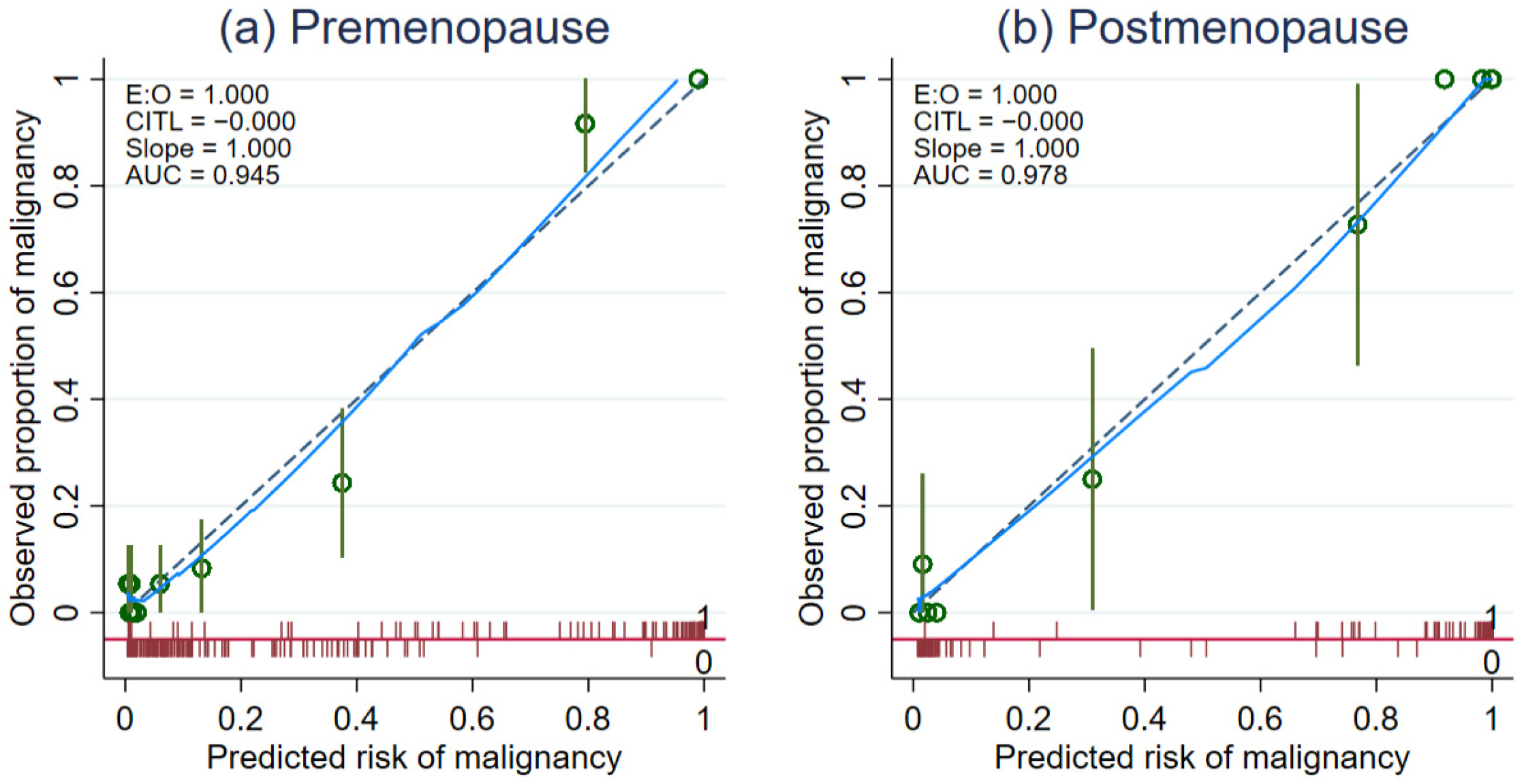
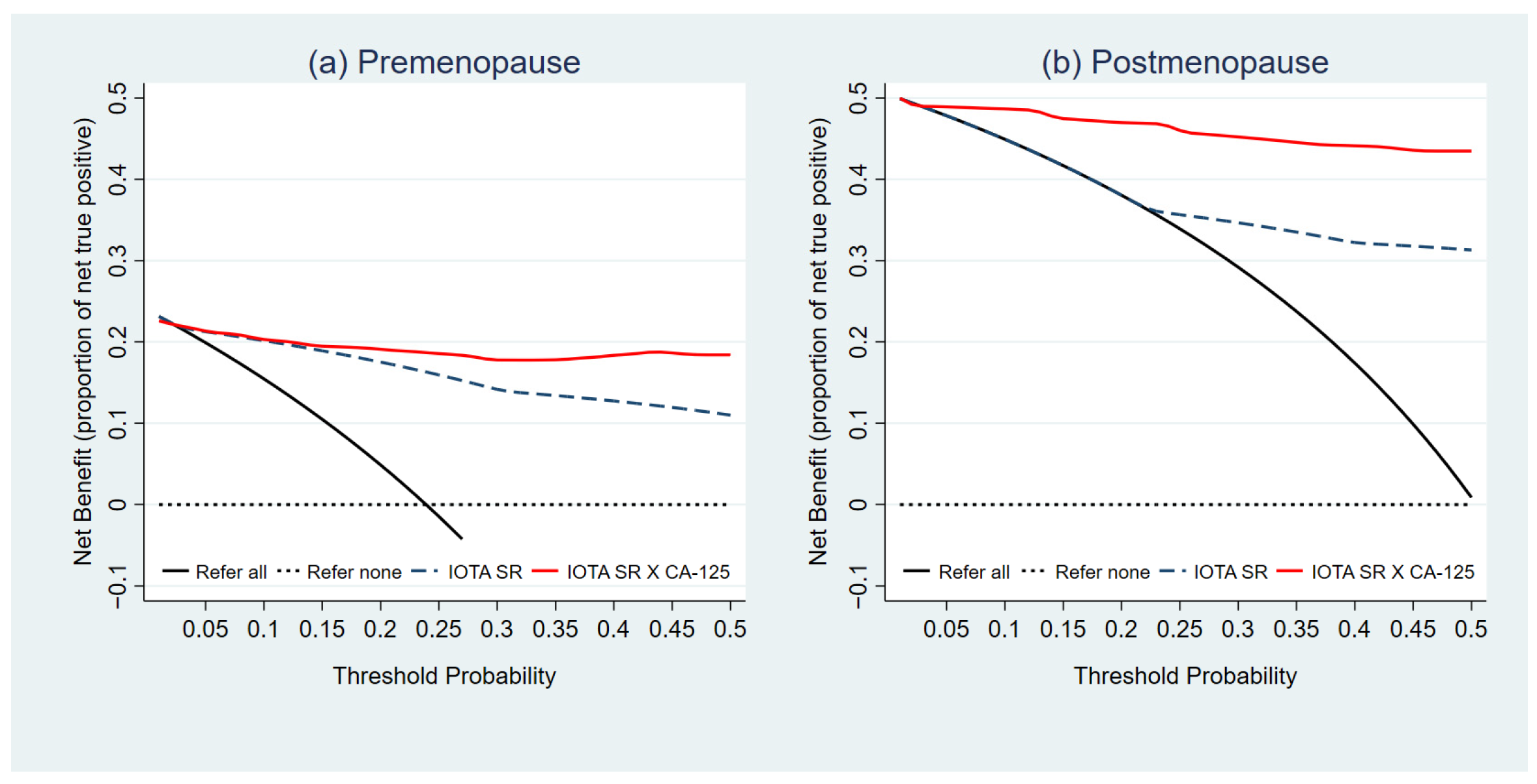
3.3. Prediction Model Performance
3.4. Comparative Validation of Diagnostic Performance
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kaijser, J.; Bourne, T.; Valentin, L.; Sayasneh, A.; Van Holsbeke, C.; Vergote, I.; Testa, A.C.; Franchi, D.; Van Calster, B.; Timmerman, D. Improving Strategies for Diagnosing Ovarian Cancer: A Summary of the International Ovarian Tumor Analysis (IOTA) Studies. Ultrasound Obstet. Gynecol. Off. J. Int. Soc. Ultrasound Obstet. Gynecol. 2013, 41, 9–20. [Google Scholar] [CrossRef] [PubMed]
- Elattar, A.; Bryant, A.; Winter-Roach, B.A.; Hatem, M.; Naik, R. Optimal Primary Surgical Treatment for Advanced Epithelial Ovarian Cancer. Cochrane Database Syst. Rev. 2011, 2011, CD007565. [Google Scholar] [CrossRef] [PubMed]
- American College of Obstetricians and Gynecologists’ Committee. Practice Bulletins—Gynecology Practice Bulletin No. 174: Evaluation and Management of Adnexal Masses. Obstet. Gynecol. 2016, 128, e210–e226. [Google Scholar] [CrossRef] [PubMed]
- Gorp, T.V.; Veldman, J.; Calster, B.V.; Cadron, I.; Leunen, K.; Amant, F.; Timmerman, D.; Vergote, I. Subjective Assessment by Ultrasound Is Superior to the Risk of Malignancy Index (RMI) or the Risk of Ovarian Malignancy Algorithm (ROMA) in Discriminating Benign from Malignant Adnexal Masses. Eur. J. Cancer 2012, 48, 1649–1656. [Google Scholar] [CrossRef] [PubMed]
- Timmerman, D. The Use of Mathematical Models to Evaluate Pelvic Masses; Can They Beat an Expert Operator? Best Pract. Res. Clin. Obstet. Gynaecol. 2004, 18, 91–104. [Google Scholar] [CrossRef] [PubMed]
- Sayasneh, A.; Wynants, L.; Preisler, J.; Kaijser, J.; Johnson, S.; Stalder, C.; Husicka, R.; Abdallah, Y.; Raslan, F.; Drought, A.; et al. Multicentre External Validation of IOTA Prediction Models and RMI by Operators with Varied Training. Br. J. Cancer 2013, 108, 2448–2454. [Google Scholar] [CrossRef] [PubMed]
- Holsbeke, C.V.; Calster, B.V.; Bourne, T.; Ajossa, S.; Testa, A.C.; Guerriero, S.; Fruscio, R.; Lissoni, A.A.; Czekierdowski, A.; Savelli, L.; et al. External Validation of Diagnostic Models to Estimate the Risk of Malignancy in Adnexal Masses. Clin. Cancer Res. 2012, 18, 815–825. [Google Scholar] [CrossRef] [PubMed]
- Kaijser, J.; Sayasneh, A.; Van Hoorde, K.; Ghaem-Maghami, S.; Bourne, T.; Timmerman, D.; Van Calster, B. Presurgical Diagnosis of Adnexal Tumours Using Mathematical Models and Scoring Systems: A Systematic Review and Meta-Analysis. Hum. Reprod. Update 2014, 20, 449–462. [Google Scholar] [CrossRef]
- Auekitrungrueng, R.; Tinnangwattana, D.; Tantipalakorn, C.; Charoenratana, C.; Lerthiranwong, T.; Wanapirak, C.; Tongsong, T. Comparison of the Diagnostic Accuracy of International Ovarian Tumor Analysis Simple Rules and the Risk of Malignancy Index to Discriminate between Benign and Malignant Adnexal Masses. Int. J. Gynaecol. Obstet. Off. Organ Int. Fed. Gynaecol. Obstet. 2019, 146, 364–369. [Google Scholar] [CrossRef]
- Alcázar, J.L.; Pascual, M.Á.; Olartecoechea, B.; Graupera, B.; Aubá, M.; Ajossa, S.; Hereter, L.; Julve, R.; Gastón, B.; Peddes, C.; et al. IOTA Simple Rules for Discriminating between Benign and Malignant Adnexal Masses: Prospective External Validation. Ultrasound Obstet. Gynecol. 2013, 42, 467–471. [Google Scholar] [CrossRef]
- Meys, E.M.J.; Kaijser, J.; Kruitwagen, R.F.P.M.; Slangen, B.F.M.; Van Calster, B.; Aertgeerts, B.; Verbakel, J.Y.; Timmerman, D.; Van Gorp, T. Subjective Assessment versus Ultrasound Models to Diagnose Ovarian Cancer: A Systematic Review and Meta-Analysis. Eur. J. Cancer Oxf. Engl. 1990 2016, 58, 17–29. [Google Scholar] [CrossRef] [PubMed]
- Dochez, V.; Caillon, H.; Vaucel, E.; Dimet, J.; Winer, N.; Ducarme, G. Biomarkers and Algorithms for Diagnosis of Ovarian Cancer: CA125, HE4, RMI and ROMA, a Review. J. Ovarian Res. 2019, 12, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Moore, R.G.; McMeekin, D.S.; Brown, A.K.; DiSilvestro, P.; Miller, M.C.; Allard, W.J.; Gajewski, W.; Kurman, R.; Bast, R.C.; Skates, S.J. A Novel Multiple Marker Bioassay Utilizing HE4 and CA125 for the Prediction of Ovarian Cancer in Patients with a Pelvic Mass. Gynecol. Oncol. 2009, 112, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Dearking, A.C.; Aletti, G.D.; McGree, M.E.; Weaver, A.L.; Sommerfield, M.-K.; Cliby, W.A. How Relevant Are ACOG and SGO Guidelines for Referral of Adnexal Mass? Obstet. Gynecol. 2007, 110, 841–848. [Google Scholar] [CrossRef] [PubMed]
- Timmerman, D.; Testa, A.C.; Bourne, T.; Ameye, L.; Jurkovic, D.; Holsbeke, C.V.; Paladini, D.; Calster, B.V.; Vergote, I.; Huffel, S.V.; et al. Simple Ultrasound-Based Rules for the Diagnosis of Ovarian Cancer. Ultrasound Obstet. Gynecol. 2008, 31, 681–690. [Google Scholar] [CrossRef]
- Zou Kelly, H.; O’Malley, A. James; Mauri Laura Receiver-Operating Characteristic Analysis for Evaluating Diagnostic Tests and Predictive Models. Circulation 2007, 115, 654–657. [Google Scholar] [CrossRef]
- Vickers, A.J.; Van Calster, B.; Steyerberg, E.W. Net Benefit Approaches to the Evaluation of Prediction Models, Molecular Markers, and Diagnostic Tests. BMJ 2016, 352, i6. [Google Scholar] [CrossRef]
- Vickers, A.J.; Elkin, E.B. Decision Curve Analysis: A Novel Method for Evaluating Prediction Models. Med. Decis. Mak. Int. J. Soc. Med. Decis. Mak. 2006, 26, 565–574. [Google Scholar] [CrossRef]
- Vickers, A.J.; van Calster, B.; Steyerberg, E.W. A Simple, Step-by-Step Guide to Interpreting Decision Curve Analysis. Diagn. Progn. Res. 2019, 3, 18. [Google Scholar] [CrossRef]
- What Are IOTA Easy Descriptors and Simple Rules: How to Use Them. Ultrasound Med. Biol. 2019, 45, S19. [CrossRef]
- Tinnangwattana, D.; Vichak-Ururote, L.; Tontivuthikul, P.; Charoenratana, C.; Lerthiranwong, T.; Tongsong, T. IOTA Simple Rules in Differentiating between Benign and Malignant Adnexal Masses by Non-Expert Examiners. Asian Pac. J. Cancer Prev. APJCP 2015, 16, 3835–3838. [Google Scholar] [CrossRef] [PubMed]
- Tantipalakorn, C.; Wanapirak, C.; Khunamornpong, S.; Sukpan, K.; Tongsong, T. IOTA Simple Rules in Differentiating between Benign and Malignant Ovarian Tumors. Asian Pac. J. Cancer Prev. APJCP 2014, 15, 5123–5126. [Google Scholar] [CrossRef] [PubMed]
- Nunes, N.; Ambler, G.; Foo, X.; Naftalin, J.; Widschwendter, M.; Jurkovic, D. Use of IOTA Simple Rules for Diagnosis of Ovarian Cancer: Meta-Analysis. Ultrasound Obstet. Gynecol. Off. J. Int. Soc. Ultrasound Obstet. Gynecol. 2014, 44, 503–514. [Google Scholar] [CrossRef] [PubMed]
- Piovano, E.; Cavallero, C.; Fuso, L.; Viora, E.; Ferrero, A.; Gregori, G.; Grillo, C.; Macchi, C.; Mengozzi, G.; Mitidieri, M.; et al. Diagnostic Accuracy and Cost-Effectiveness of Different Strategies to Triage Women with Adnexal Masses: A Prospective Study. Ultrasound Obstet. Gynecol. 2017, 50, 395–403. [Google Scholar] [CrossRef]
- Al-Musalhi, K.; Al-Kindi, M.; Ramadhan, F.; Al-Rawahi, T.; Al-Hatali, K.; Mula-Abed, W.-A. Validity of Cancer Antigen-125 (CA-125) and Risk of Malignancy Index (RMI) in the Diagnosis of Ovarian Cancer. Oman Med. J. 2015, 30, 428–434. [Google Scholar] [CrossRef]
- Dikmen, Z.G.; Colak, A.; Dogan, P.; Tuncer, S.; Akbiyik, F. Diagnostic Performances of CA125, HE4, and ROMA Index in Ovarian Cancer. Eur. J. Gynaecol. Oncol. 2015, 36, 457–462. [Google Scholar]
- Liao, X.-Y.; Huang, G.-J.; Gao, C.; Wang, G.-H. A Meta-Analysis of Serum Cancer Antigen 125 Array for Diagnosis of Ovarian Cancer in Chinese. J. Cancer Res. Ther. 2014, 10, C222–C224. [Google Scholar] [CrossRef]
- Huy, N.V.Q.; Van Khoa, V.; Tam, L.M.; Vinh, T.Q.; Tung, N.S.; Thanh, C.N.; Chuang, L. Standard and Optimal Cut-off Values of Serum ca-125, HE4 and ROMA in Preoperative Prediction of Ovarian Cancer in Vietnam. Gynecol. Oncol. Rep. 2018, 25, 110–114. [Google Scholar] [CrossRef]
- Dawson, N.V.; Weiss, R. Dichotomizing Continuous Variables in Statistical Analysis: A Practice to Avoid. Med. Decis. Mak. 2012, 32, 225–226. [Google Scholar] [CrossRef]
- Moons, K.G.M.; Altman, D.G.; Reitsma, J.B.; Ioannidis, J.P.A.; Macaskill, P.; Steyerberg, E.W.; Vickers, A.J.; Ransohoff, D.F.; Collins, G.S. Transparent Reporting of a Multivariable Prediction Model for Individual Prognosis or Diagnosis (TRIPOD): Explanation and Elaboration. Ann. Intern. Med. 2015, 162, W1–W73. [Google Scholar] [CrossRef]
- Royston, P.; Sauerbrei, W. Multivariable Model-Building: A Pragmatic Approach to Regression Anaylsis Based on Fractional Polynomials for Modelling Continuous Variables; John Wiley & Sons: Hoboken, NJ, USA, 2008; ISBN 978-0-470-77078-8. [Google Scholar]
- Timmerman, D.; Van Calster, B.; Jurkovic, D.; Valentin, L.; Testa, A.C.; Bernard, J.-P.; Van Holsbeke, C.; Van Huffel, S.; Vergote, I.; Bourne, T. Inclusion of CA-125 Does Not Improve Mathematical Models Developed to Distinguish between Benign and Malignant Adnexal Tumors. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2007, 25, 4194–4200. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.H.; Sohn, G.S.; Chay, D.B.; Cho, H.B.; Kim, J.-H. Preoperative Serum Levels of Cancer Antigen 125 and Carcinoembryonic Antigen Ratio Can Improve Differentiation between Mucinous Ovarian Carcinoma and Other Epithelial Ovarian Carcinomas. Obstet. Gynecol. Sci. 2018, 61, 344–351. [Google Scholar] [CrossRef] [PubMed]
- Cambruzzi, E.; de Lima, R.; Teixeira, S.L.; Pêgas, K.L. The Relationship between Serum Levels of CA 125 and the Degree of Differentiation in Ovarian Neoplasms. J. Bras. Patol. E Med. Lab. 2014, 50, 20–25. [Google Scholar] [CrossRef][Green Version]
- Vittinghoff, E.; McCulloch, C.E. Relaxing the Rule of Ten Events per Variable in Logistic and Cox Regression. Am. J. Epidemiol. 2007, 165, 710–718. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Parameters | Malignant (n = 145) | Benign (n = 334) | p-Value | ||
|---|---|---|---|---|---|
| n | (%) | n | (%) | ||
| Clinical characteristics | |||||
| Age (year) * | 45.4 | ±14.8 | 40.6 | ±11.0 | <0.001 |
| Nulliparity | 75 | (51.7) | 137 | (41.0) | 0.035 |
| Post-menopause | 58 | (40.0) | 57 | (17.1) | <0.001 |
| Biomarker | |||||
| Serum CA-125, (U/mL) ** | 405.8 | (122.4, 714.8) | 39.0 | (23.6, 56.9) | <0.001 |
| Range (min-max) | (13.7–2023.6) | (5.4–278.3) | |||
| IOTA Simple Rules features | |||||
| Malignant tumor (M-features) | |||||
| M1 | 73 | (50.3) | 16 | (4.8) | <0.001 |
| M2 | 34 | (23.5) | 11 | (3.3) | <0.001 |
| M3 | 32 | (22.1) | 26 | (7.8) | <0.001 |
| M4 | 74 | (51.0) | 26 | (7.8) | <0.001 |
| M5 | 96 | (66.2) | 35 | (10.5) | <0.001 |
| Benign tumor (B-features) | |||||
| B1 | 9 | (6.2) | 169 | (50.6) | <0.001 |
| B2 | 1 | (0.7) | 17 | (5.1) | 0.018 |
| B3 | 5 | (3.5) | 66 | (19.8) | <0.001 |
| B4 | 17 | (11.7) | 78 | (23.4) | 0.004 |
| B5 | 42 | (29.0) | 297 | (88.9) | <0.001 |
| IOTA Simple Rules diagnosis | |||||
| Benign | 19 | (13.1) | 253 | (75.8) | NA |
| Malignant | 98 | (67.6) | 22 | (6.6) | NA |
| Inconclusive | 28 | (19.3) | 59 | (17.6) | 0.699 |
| Models | Predictors Included | ß | (95%CI) | p-Value | AuROC (95%CI) |
|---|---|---|---|---|---|
| Premenopausal women (n = 364) | |||||
| PRE1 | IOTA Simple Rules | ||||
| Benign | Ref | Ref | 0.89 (0.86, 0.93) | ||
| Inconclusive | 2.72 | (1.77, 3.68) | <0.001 | ||
| Malignant | 4.68 | (3.72, 5.64) | <0.001 | ||
| PRE2 | Log serum CA-125 (FP1) § | 0.02 | (0.01, 0.03) | <0.001 | 0.88 (0.83, 0.93) |
| PRE3 | IOTA Simple Rules | ||||
| Benign | Ref | Ref | 0.94 (0.91, 0.98) | ||
| Inconclusive | 2.10 | (0.99, 3.21) | <0.001 | ||
| Malignant | 4.27 | (3.11, 5.42) | <0.001 | ||
| Log serum CA-125 (FP1) § | 0.02 | (0.01, 0.03) | <0.001 | ||
| Intercept (constant) | −4.01 | (−4.95,−3.06) | <0.001 | ||
| Postmenopausal women (n = 115) | |||||
| POST1 | IOTA Simple Rules | ||||
| Benign | Ref | Ref | 0.83 (0.76, 0.90) | ||
| Inconclusive | 0.84 | (−0.37, 2.04) | 0.173 | ||
| Malignant | 3.81 | (2.48, 5.13) | <0.001 | ||
| POST2 | Log serum CA-125 (FP1) † | 0.02 | (0.01, 0.03) | <0.001 | 0.88 (0.81, 0.95) |
| POST3 | IOTA Simple Rules | ||||
| Benign | Ref | Ref | 0.98 (0.95, 1.00) | ||
| Inconclusive | 0.71 | (−1.63, 3.05) | 0.551 | ||
| Malignant | 5.30 | (3.17, 7.43) | <0.001 | ||
| Log serum CA-125 (FP1) † | 0.03 | (0.01, 0.04) | <0.001 | ||
| Intercept (constant) | −2.23 | (−3.52,−0.93) | |||
| Comparison | AuROC | p-Value * | Log Likelihood | p-Value ** |
|---|---|---|---|---|
| Premenopausal women (n = 364) | ||||
| PRE1 vs. PRE3 | 0.89 vs. 0.95 | <0.001 | −114.9805 vs.−74.2167 | <0.001 |
| Postmenopausal women (n = 115) | ||||
| POST1 vs. POST3 | 0.83 vs. 0.98 | <0.001 | −51.76 vs.−21.1981 | <0.001 |
| Malignant | Benign | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) | LR+ | |
|---|---|---|---|---|---|---|---|
| n | n | (95%CI) | (95%CI) | (95%CI) | (95%CI) | (95%CI) | |
| Premenopausal women (n = 364) | |||||||
| IOTA SR–refer women with inconclusive results | |||||||
| Malignant and inconclusive | 81 | 69 | 93.1 | 75.1 | 54.0 | 97.2 | 3.74 |
| Benign | 6 | 208 | (85.6, 97.4) | (69.6, 80.1) | (45.7, 62.2) | (94.0, 99.0) | (3.02, 4.62) |
| IOTA SR X CA-125 for premenopausal women | |||||||
| Predicted risk ≥10% | 80 | 59 | 92.0 | 78.7 | 57.6 | 96.9 | 4.32 |
| 7 | 218 | (84.1, 96.7) | (73.4, 83.4) | (48.9, 65.9) | (93.7, 98.7) | (3.41, 5.46) | |
| Predicted risk ≥20% | 78 | 34 | 89.7 | 87.7 | 69.6 | 96.4 | 7.30 |
| 9 | 243 | (81.3, 95.2) | (83.3, 91.3) | (60.2, 78.0) | (93.3, 98.4) | (5.29, 10.09) | |
| Predicted risk ≥30% | 75 | 25 | 86.2 | 91.0 | 75.0 | 95.5 | 9.55 |
| 12 | 252 | (77.1, 92.7) | (87.0, 94.1) | (65.3, 83.1) | (92.2, 97.6) | (6.51, 14.01) | |
| Predicted risk ≥40% | 75 | 12 | 86.2 | 95.7 | 86.2 | 95.7 | 19.90 |
| 12 | 265 | (77.1, 92.7) | (92.6, 97.7) | (77.1, 92.7) | (92.6, 97.7) | (11.37, 34.83) | |
| Predicted risk ≥50% | 71 | 4 | 81.6 | 98.6 | 94.7 | 94.5 | 56.51 |
| 16 | 273 | (71.9, 89.1) | (96.3, 99.6) | (86.9, 98.5) | (91.2, 96.8) | (21.25, 150.28) | |
| Malignant | Benign | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) | LR+ | |
|---|---|---|---|---|---|---|---|
| n | n | (95%CI) | (95%CI) | (95%CI) | (95%CI) | (95%CI) | |
| Postmenopausal women (n = 115) | |||||||
| IOTA SR–refer women with inconclusive results | |||||||
| Malignant and inconclusive | 45 | 12 | 77.6 | 78.9 | 78.9 | 77.6 | 3.69 |
| Benign | 13 | 45 | (64.7, 87.5) | (66.1, 88.6) | (66.1, 88.6) | (64.7, 87.5) | (2.19, 6.21) |
| IOTA SR X CA-125 for postmenopausal women | |||||||
| Predicted risk ≥10% | 57 | 9 | 98.3 | 84.2 | 86.4 | 98.0 | 6.22 |
| 1 | 48 | (90.8, 100.0) | (72.1, 92.5) | (75.7, 93.6) | (89.1, 99.9) | (3.41, 11.35) | |
| Predicted risk ≥20% | 56 | 8 | 96.6 | 86.0 | 87.5 | 96.1 | 6.88 |
| 2 | 49 | (88.1, 99.6) | (74.2, 93.7) | (76.8, 94.4) | (86.5, 99.5) | (3.61, 13.10) | |
| Predicted risk ≥30% | 55 | 7 | 94.8 | 87.7 | 88.7 | 94.3 | 7.72 |
| 3 | 50 | (85.6, 98.9) | (76.3, 94.9) | (78.1, 95.3) | (84.3, 98.8) | (3.85, 15.49) | |
| Predicted risk ≥40% | 55 | 6 | 94.8 | 89.5 | 90.2 | 94.4 | 9.01 |
| 3 | 51 | (85.6, 98.9) | (78.5, 96.0) | (79.8, 96.3) | (84.6, 98.8) | (4.22, 19.25) | |
| Predicted risk ≥50% | 55 | 5 | 94.8 | 91.2 | 91.7 | 94.5 | 10.81 |
| 3 | 52 | (85.6, 98.9) | (80.7, 97.1) | (81.6, 97.2) | (84.9, 98.9) | (4.67, 25.02) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Phinyo, P.; Patumanond, J.; Saenrungmuaeng, P.; Chirdchim, W.; Pipanmekaporn, T.; Tantraworasin, A.; Tongsong, T.; Tantipalakorn, C. Diagnostic Added-Value of Serum CA-125 on the IOTA Simple Rules and Derivation of Practical Combined Prediction Models (IOTA SR X CA-125). Diagnostics 2021, 11, 173. https://doi.org/10.3390/diagnostics11020173
Phinyo P, Patumanond J, Saenrungmuaeng P, Chirdchim W, Pipanmekaporn T, Tantraworasin A, Tongsong T, Tantipalakorn C. Diagnostic Added-Value of Serum CA-125 on the IOTA Simple Rules and Derivation of Practical Combined Prediction Models (IOTA SR X CA-125). Diagnostics. 2021; 11(2):173. https://doi.org/10.3390/diagnostics11020173
Chicago/Turabian StylePhinyo, Phichayut, Jayanton Patumanond, Panprapha Saenrungmuaeng, Watcharin Chirdchim, Tanyong Pipanmekaporn, Apichat Tantraworasin, Theera Tongsong, and Charuwan Tantipalakorn. 2021. "Diagnostic Added-Value of Serum CA-125 on the IOTA Simple Rules and Derivation of Practical Combined Prediction Models (IOTA SR X CA-125)" Diagnostics 11, no. 2: 173. https://doi.org/10.3390/diagnostics11020173
APA StylePhinyo, P., Patumanond, J., Saenrungmuaeng, P., Chirdchim, W., Pipanmekaporn, T., Tantraworasin, A., Tongsong, T., & Tantipalakorn, C. (2021). Diagnostic Added-Value of Serum CA-125 on the IOTA Simple Rules and Derivation of Practical Combined Prediction Models (IOTA SR X CA-125). Diagnostics, 11(2), 173. https://doi.org/10.3390/diagnostics11020173