
Dynamic Doppler Ultrasound Assessment of Tissue Perfusion Is a Better Tool than a Single Vessel Doppler Examination in Differentiating Malignant and Inflammatory Pancreatic Lesions


Abstract
1. Introduction
2. Methods
2.1. Doppler Flow Assessment
2.2. Statistics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mario, C.; Marilisa, F.; Kryssia, I.R.C.; Pellegrino, C.; Ginevra, C.; Chiara, M.; Alberto, B.; Antonio, N.; Gioacchino, L.; Tiziana, M. Epidemiology and risk factors of pan-creatic cancer. Acta Biomed. 2018, 89, 141–146. [Google Scholar]
- Drouillard, A.; Manfredi, S.; Lepage, C.; Bouvier, A.-M. Épidémiologie du cancer du pancréas. Bull. Cancer 2018, 105, 63–69. [Google Scholar] [CrossRef] [PubMed]
- McGuigan, A.; Kelly, P.; Turkington, R.C.; Jones, C.; Coleman, H.G.; McCain, R.S. Pancreatic cancer: A review of clinical diagnosis, epidemiology, treatment and outcomes. World J. Gastroenterol. 2018, 24, 4846–4861. [Google Scholar] [CrossRef]
- Ilic, M.; Ilic, I. Epidemiology of pancreatic cancer. World J. Gastroenterol. 2016, 22, 9694–9705. [Google Scholar] [CrossRef] [PubMed]
- Stark, A.P.; Sacks, G.D.; Rochefort, M.M.; Donahue, T.R.; Reber, H.A.; Tomlinson, J.S.; Dawson, D.W.; Eibl, G.; Hines, O.J. Long-term survival in patients with pan-creatic ductal adenocarcinoma. Surgery 2016, 159, 1520–1527. [Google Scholar] [CrossRef] [PubMed]
- Dyrla, P.; Lubas, A.; Gil, J.; Niemczyk, S. Doppler tissue perfusion parameters in recognizing pancreatic malignant tumors. J. Gastroenterol. Hepatol. 2016, 31, 691–695. [Google Scholar] [CrossRef] [PubMed]
- Dyrla, P.; Gil, J.; Kosik, K.; Schneditz, D.; Saracyn, M.; Niemczyk, S.; Lubas, A. Doppler tissue perfusion measurement is a sensitive and specific tool for a differentiation between malignant and inflammatory pancreatic tumors. PLoS ONE 2019, 14, e0215944. [Google Scholar] [CrossRef] [PubMed]
- Scholbach, T.; Scholbach, J.; Di Martino, E. Dynamic Sonographic Tissue Perfusion Measurement. J. Med. Ultrasound 2009, 17, 71–85. [Google Scholar] [CrossRef]
- Nakai, Y.; Takahara, N.; Mizuno, S.; Kogure, H.; Koike, K. Current Status of Endoscopic Ultrasound Techniques for Pancreatic Neoplasms. Clin. Endosc. 2019, 52, 527–532. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, T.; Yamashita, Y.; Kitano, M. Endoscopic Ultrasound for Early Diagnosis of Pancreatic Cancer. Diagnostics 2019, 9, 81. [Google Scholar] [CrossRef] [PubMed]
- Lubas, A.; Kade, G.; Saracyn, M.; Niemczyk, S.; Dyrla, P. Dynamic tissue perfusion assessment reflects associations between anti-hypertensive treatment and renal cortical perfusion in patients with chronic kidney disease and hypertension. Int. Urol. Nephrol. 2018, 50, 509–516. [Google Scholar] [CrossRef] [PubMed]
- Scholbach, T. Dynamic Tissue Perfusion Measurement—Basics and Applications. In Sonography; Intech Open: London, UK, 2012. [Google Scholar] [CrossRef]
- Iglesias-Garcia, J.; Lindkvist, B.; Lariño-Noia, J.; Abdulkader-Nallib, I.; Dominguez-Muñoz, J.E. Differential diagnosis of solid pan-creatic masses: Contrast-enhanced harmonic (CEH-EUS), quantitative-elastography (QE-EUS), or both? United Eur. Gastroenterol. J. 2017, 5, 236–246. [Google Scholar] [CrossRef] [PubMed]
- Mei, S.; Wang, M.; Sun, L. Contrast-Enhanced EUS for Differential Diagnosis of Pancreatic Masses: A Meta-Analysis. Gastroenterol. Res. Pract. 2019, 2019, 1670183. [Google Scholar] [CrossRef] [PubMed]
- Kitano, M.; Kudo, M.; Sakamoto, H.; Nakatani, T.; Maekawa, K.; Mizuguchi, N.; Ito, Y.; Miki, M.; Matsui, U.; von Schrenck, T. Preliminary study of contrast-enhanced har-monic endosonography with second-generation contrast agents. J. Med. Ultrason. 2008, 35, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Jin, H.; Liao, D.; Qian, B.; Zhang, Y.; Xu, M.; Han, S. Contrast-enhanced harmonic endoscopic ultrasonography for the differential diagnosis of pancreatic masses: A systematic review and meta-analysis. Mol. Clin. Oncol. 2019, 11, 425–433. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, Y.; Shimokawa, T.; Napoléon, B.; Fusaroli, P.; Gincul, R.; Kudo, M.; Kitano, M. Value of contrast-enhanced harmonic endo-scopic ultrasonography with enhancement pattern for diagnosis of pancreatic cancer: A meta-analysis. Dig. Endosc. 2019, 31, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Emanuel, A.L.; Meijer, R.I.; Van Poelgeest, E.; Spoor, P.; Serné, E.H.; Eringa, E. Contrast-enhanced ultrasound for quantification of tissue perfusion in humans. Microcirculation 2019, 27, e12588. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.; Xin, X.J.; Mu, J.; Mao, Y.R.; Zhang, S. Comparative analysis of superb microvascular imaging and contrast-enhanced ultrasound in diagnosis of small renal masses. Zhonghua Yi Xue Za Zhi 2019, 99, 1778–1781. [Google Scholar] [PubMed]
- Ohno, Y.; Fujimoto, T.; Shibata, Y.; Ohno, Y. A New Era in Diagnostic Ultrasound, Superb Microvascular Imaging: Preliminary Results in Pediatric Hepato-Gastrointestinal Disorders. Eur. J. Pediatr. Surg. 2016, 27, 020–025. [Google Scholar]
- He, M.-N.; Lv, K.; Jiang, Y.-X.; Jiang, T.-A. Application of superb microvascular imaging in focal liver lesions. World J. Gastroenterol. 2017, 23, 7765–7775. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Neoplastic Lesions (n = 40) | Inflammatory Lesions (n = 29) | Significance (p) | |||
|---|---|---|---|---|---|
| TFV [cm/s] | 1.422 | ±0.742 | 2.653 | ±0.733 | <0.001 |
| TRI | 1.000 | (1.000–1.000) | 0.776 | (0.601–0.880) | <0.001 |
| TPI [cm/s] | 0.004 | (0.001–0.007) | 0.016 | (0.010–0.024) | <0.001 |
| FV [cm/s] | 1.592 | (0.953–3.148) | 3.397 | (2.696–4.350) | 0.001 |
| RI | 1.000 | (1.000–1.000) | 0.843 | (0.648–1.000) | 0.002 |
| VolF [mL/s] | 0.010 | (0.004–0.035) | 0.032 | (0.022–0.059) | <0.001 |
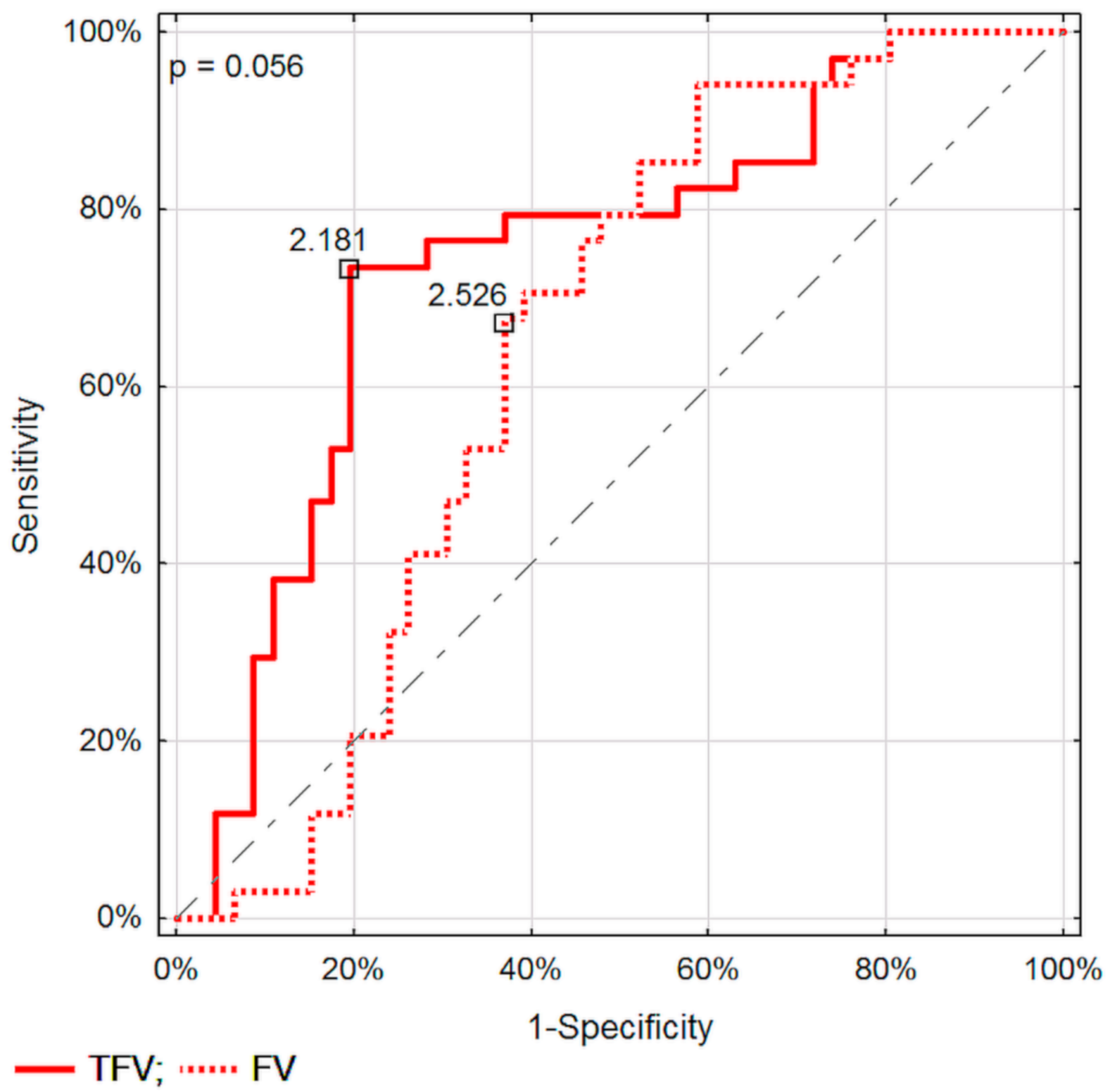
| Nadir Value | Sensitivity | Specificity | ACC | AUC | Significance (p) | |
|---|---|---|---|---|---|---|
| TFV [cm/s] | 2.181 | 0.862 | 0.900 | 0.884 | 0.883 | <0.001 |
| TRI | 0.909 | 0.850 | 0.793 | 0.862 | 0.831 | <0.001 |
| TPI [cm/s] | 0.009 | 0.793 | 0.925 | 0.870 | 0.899 | <0.001 |
| FV [cm/s] | 2.526 | 0.793 | 0.700 | 0.739 | 0.731 | <0.001 |
| RI | 0.877 | 0.850 | 0.586 | 0.739 | 0.698 | 0.003 |
| VolF [mL/s] | 0.015 | 0.931 | 0.600 | 0.739 | 0.765 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dyrla, P.; Lubas, A.; Gil, J.; Saracyn, M.; Gonciarz, M. Dynamic Doppler Ultrasound Assessment of Tissue Perfusion Is a Better Tool than a Single Vessel Doppler Examination in Differentiating Malignant and Inflammatory Pancreatic Lesions. Diagnostics 2021, 11, 2289. https://doi.org/10.3390/diagnostics11122289
Dyrla P, Lubas A, Gil J, Saracyn M, Gonciarz M. Dynamic Doppler Ultrasound Assessment of Tissue Perfusion Is a Better Tool than a Single Vessel Doppler Examination in Differentiating Malignant and Inflammatory Pancreatic Lesions. Diagnostics. 2021; 11(12):2289. https://doi.org/10.3390/diagnostics11122289
Chicago/Turabian StyleDyrla, Przemysław, Arkadiusz Lubas, Jerzy Gil, Marek Saracyn, and Maciej Gonciarz. 2021. "Dynamic Doppler Ultrasound Assessment of Tissue Perfusion Is a Better Tool than a Single Vessel Doppler Examination in Differentiating Malignant and Inflammatory Pancreatic Lesions" Diagnostics 11, no. 12: 2289. https://doi.org/10.3390/diagnostics11122289
APA StyleDyrla, P., Lubas, A., Gil, J., Saracyn, M., & Gonciarz, M. (2021). Dynamic Doppler Ultrasound Assessment of Tissue Perfusion Is a Better Tool than a Single Vessel Doppler Examination in Differentiating Malignant and Inflammatory Pancreatic Lesions. Diagnostics, 11(12), 2289. https://doi.org/10.3390/diagnostics11122289