Left Atrial Strain Identifies Increased Atrial Ectopy in Patients with Beta-Thalassemia Major

 , , , ,
, , , ,  and
and
Abstract
1. Introduction
2. Patients and Methods
2.1. Study Population
2.2. Study Protocol
2.2.1. Conventional Echocardiography
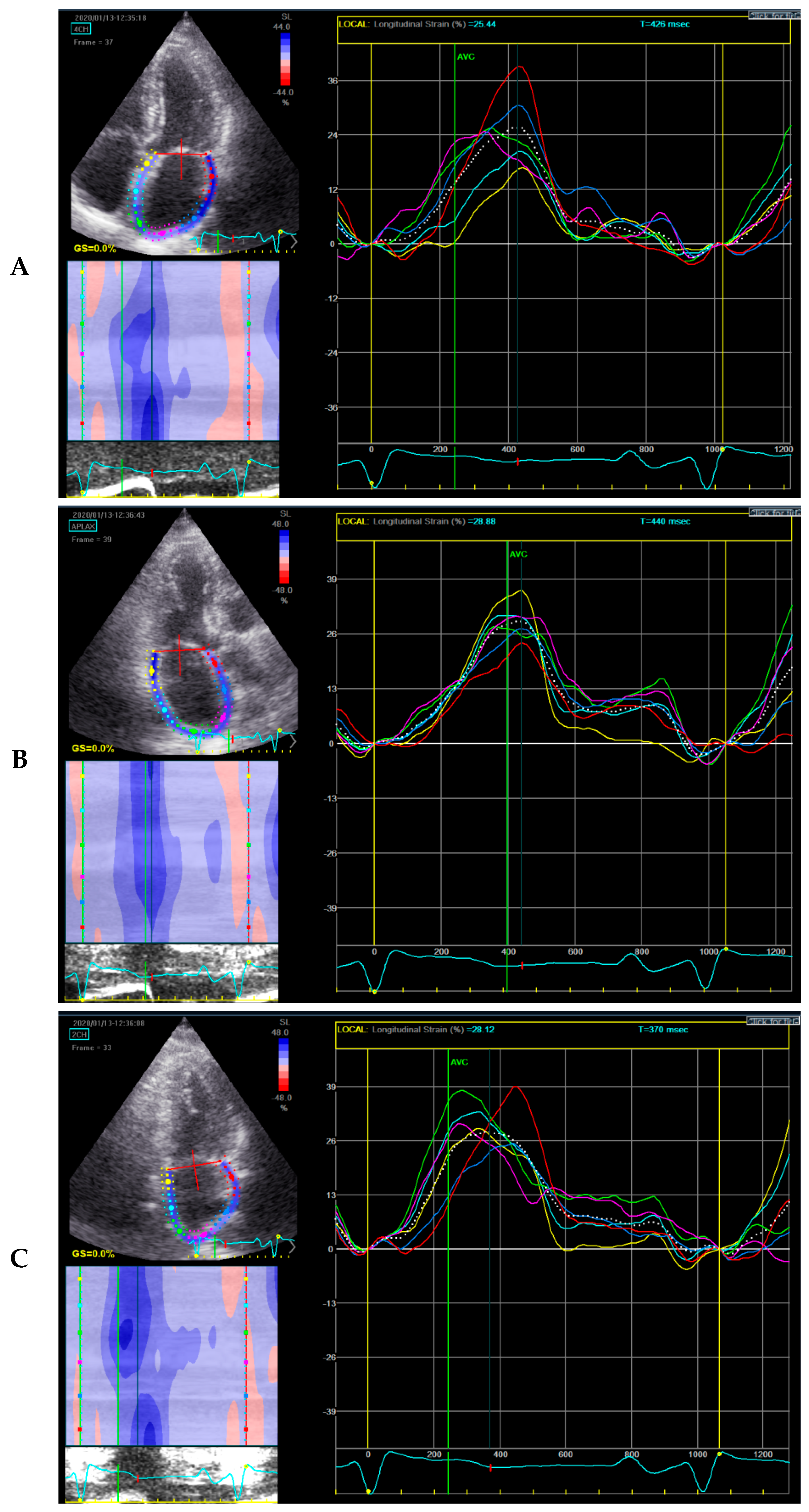
2.2.2. Speckle Tracking Echocardiography
2.2.3. CMR-T2*
2.2.4. 24-Hour Holter Recording
2.3. Statistical Analysis
3. Results
3.1. Patients Characteristics
3.2. Cardiac Imaging Parameters of the Patients
3.3. Associates of PACs in β-TM Patients
4. Discussion
4.1. Arrhythmias in β-ΤM Patients.
4.2. LA Peak Systolic Strain and Arrhythmias
4.3. Study Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| β-TM | beta-thalassemia major |
| CI | confidence interval |
| CMR | cardiac magnetic resonance |
| E | trans-mitral early filling wave |
| E′ | early diastolic wave |
| LA | left atrium/left atrial |
| LV | left ventricle/left ventricular |
| OR | odds ratio |
| PACs | premature atrial contractions |
References
- Pennell, D.J.; Udelson, J.E.; Arai, A.E.; Bozkurt, B.; Cohen, A.R.; Galanello, R.; Hoffman, T.M.; Kiernan, M.S.; Lerakis, S.; Piga, A.; et al. Cardiovascular Function and Treatment in β-Thalassemia Major a Consensus Statement from the American Heart Association. Circulation 2013, 128, 281–308. [Google Scholar] [CrossRef] [PubMed]
- Berdoukas, V.; Coates, T.D.; Cabantchik, Z.I. Iron and oxidative stress in cardiomyopathy in thalassemia. Free Radic. Biol. Med. 2015, 88, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Kirk, P.; Roughton, M.; Porter, J.; Walker, J.; Tanner, M.; Patel, J.; Wu, D.; Taylor, J.; Westwood, M.; Anderson, L.; et al. Cardiac T2* magnetic resonance for prediction of cardiac complications in Thalassemia Major. Circulation 2009, 120, 1961–1968. [Google Scholar] [CrossRef] [PubMed]
- Conen, D.; Adam, M.; Roche, F.; Barthelemy, J.C.; Felber Dietrich, D.; Imboden, M.; Künzli, N.; von Eckardstein, A.; Regenass, S.; Hornemann, T.; et al. Premature atrial contractions in the general population: Frequency and risk factors. Circulation 2012, 126, 2302–2308. [Google Scholar] [CrossRef]
- Marcus, G.M.; Dewland, T.A. Premature Atrial Contractions: A Wolf in Sheep’s Clothing? J. Am. Coll. Cardiol. 2015, 66, 242–244. [Google Scholar] [CrossRef]
- Himmelreich, J.C.L.; Lucassen, W.A.M.; Heugen, M.; Bossuyt, P.M.M.; Tan, H.L.; Harskamp, R.E.; Van Etten-Jamaludin, F.S.; Van Weert, H.C.P.M. Frequent premature atrial contractions are associated with atrial fibrillation, brain ischaemia, and mortality: A systematic review and meta-Analysis. Europace 2019, 21, 698–707. [Google Scholar] [CrossRef]
- Donal, E.; Lip, G.Y.H.; Galderisi, M.; Goette, A.; Shah, D.; Marwan, M.; Lederlin, M.; Mondillo, S.; Edvardsen, T.; Sitges, M.; et al. EACVI/EHRA Expert Consensus Document on the role of multi-modality imaging for the evaluation of patients with atrial fibrillation. Eur. Heart J. Cardiovasc. Imaging 2016, 17, 355–383. [Google Scholar] [CrossRef]
- Delgado, V.; Bucciarelli-Ducci, C.; Bax, J.J. Diagnostic and prognostic roles of echocardiography and cardiac magnetic resonance. J. Nucl. Cardiol. 2016, 23, 1399–1410. [Google Scholar] [CrossRef]
- Papadopoulos, C.H.; Oikonomidis, D.; Lazaris, E.; Nihoyannopoulos, P. Echocardiography and cardiac arrhythmias. Hell. J. Cardiol. 2018, 59, 140–149. [Google Scholar] [CrossRef]
- Catanzaro, J.N.; Makaryus, J.N.; Makaryus, A.N.; Sison, C.; Vavasis, C.; Fan, D.; Jadonath, R. Echocardiographic predictors of ventricular tachycardia. Clin. Med. Insights Cardiol. 2014, 8, 37–42. [Google Scholar] [CrossRef]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39.e14. [Google Scholar] [CrossRef] [PubMed]
- Rudski, L.G.; Lai, W.W.; Afilalo, J.; Hua, L.; Handschumacher, M.D.; Chandrasekaran, K.; Solomon, S.D.; Louie, E.K.; Schiller, N.B. Guidelines for the Echocardiographic Assessment of the Right Heart in Adults: A Report from the American Society of Echocardiography. J. Am. Soc. Echocardiogr. 2010, 23, 685–713. [Google Scholar] [CrossRef] [PubMed]
- Kamperidis, V.; Joyce, E.; Debonnaire, P.; Katsanos, S.; van Rosendael, P.J.; van der Kley, F.; Sianos, G.; Bax, J.J.; Marsan, N.A.; Delgado, V. Left ventricular functional recovery and remodeling in low-flow low-gradient severe aortic stenosis after transcatheter aortic valve implantation. J. Am. Soc. Echocardiogr. 2014, 27, 817–825. [Google Scholar] [CrossRef] [PubMed]
- Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P.; Byrd, B.F.; Dokainish, H.; Evardsen, T.; Flachskampf, F.A.; Gillebert, T.C.; Klein, A.L.; Lancelotti, P.; et al. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging I. General Principles for Echocardiographic Asses. J. Am. Soc. Echocardiogr. 2016, 29, 277–314. [Google Scholar] [CrossRef]
- Mor-Avi, V.; Lang, R.M.; Badano, L.P.; Belohlavek, M.; Cardim, N.; Derumeaux, G.; Galderisi, M.; Marwick, T.H.; Nagueh, S.F.; Sengupta, P.P.; et al. Current and evolving echocardiographic techniques for the quantitative evaluation of cardiac mechanics: ASE/EAE consensus statement on methodology and indications: Endorsed by the Japanese Society of Echocardiography. J. Am. Soc. Echocardiogr. 2011, 24, 277–313. [Google Scholar] [CrossRef]
- Modin, D.; Biering-Sørensen, S.R.; Møgelvang, R.; Alhakak, A.S.; Jensen, J.S.; Biering-Sørensen, T. Prognostic value of left atrial strain in predicting cardiovascular morbidity and mortality in the general population. Eur. Heart J. Cardiovasc. Imaging 2019, 20, 804–815. [Google Scholar] [CrossRef]
- Badano, L.P.; Kolias, T.J.; Muraru, D.; Abraham, T.P.; Aurigemma, G.; Edvardsen, T.; D’Hooge, J.; Donal, E.; Fraser, A.G.; Marwick, T.; et al. Standardization of left atrial, right ventricular, and right atrial deformation imaging using two-dimensional speckle tracking echocardiography: A consensus document of the EACVI/ASE/Industry Task Force to standardize deformation imaging. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 591–600. [Google Scholar] [CrossRef]
- Cameli, M.; Miglioranza, M.H.; Magne, J.; Mandoli, G.E.; Benfari, G.; Ancona, R.; Sibilio, G.; Reskovic Luksic, V.; Griseli, L.; Van De Heyning, C.M.; et al. Multicentric Atrial Strain COmparison between Two Different Modalities: MASCOT HIT Study. Diagnostics 2020, 10, 946. [Google Scholar] [CrossRef]
- Anderson, L.; Holden, S.; Davis, B.; Prescott, E.; Charrier, C.; Bunce, N.; Firmin, D.; Wonke, B.; Porter, J.; Walker, J.; et al. Cardiovascular T2-star (T2*) magnetic resonance for the early diagnosis of myocardial iron overload. Eur. Heart J. 2001, 22, 2171–2179. [Google Scholar] [CrossRef]
- Youden, W.J. Index for rating diagnostic tests. Cancer 1950, 3, 32–35. [Google Scholar] [CrossRef]
- Russo, V.; Rago, A.; Papa, A.A.; Nigro, G. Electrocardiographic Presentation, Cardiac Arrhythmias, and Their Management in β-Thalassemia Major Patients. Ann. Noninvasive Electrocardiol. 2016, 21, 335–342. [Google Scholar] [CrossRef] [PubMed]
- Kremastinos, D.T.; Farmakis, D. Iron overload cardiomyopathy in clinical practice. Circulation 2011, 124, 2253–2263. [Google Scholar] [CrossRef] [PubMed]
- Engle, M.A.; Erlandson, M.; Smith, C.H. Late Cardiac Complications of Chronic, Severe, Refractory Anemia with Hemochromatosis. Circulation 1964, 30, 698–705. [Google Scholar] [CrossRef] [PubMed]
- Gaita, F.; Castagno, D. Do supraventricular premature beats identify patients at high risk for atrial fibrillation? J. Cardiovasc. Med. 2017, 18, e117–e120. [Google Scholar] [CrossRef] [PubMed]
- Inaba, Y.; Yuda, S.; Kobayashi, N.; Hashimoto, A.; Uno, K.; Nakata, T.; Tsuchihashi, K.; Miura, T.; Ura, N.; Shimamoto, K. Strain rate imaging for noninvasive functional quantification of the left atrium: Comparative studies in controls and patients with atrial fibrillation. J. Am. Soc. Echocardiogr. 2005, 18, 729–736. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.; Addetia, K.; Maffessanti, F.; Mor-Avi, V.; Lang, R.M. LA Strain for Categorization of LV Diastolic Dysfunction. JACC Cardiovasc. Imaging 2017, 10, 735–743. [Google Scholar] [CrossRef]
- Mondillo, S.; Cameli, M.; Caputo, M.; Lisi, M.; Palmerini, E.; Padeletti, M.; Ballo, P. Early detection of left atrial strain abnormalities by speckle-tracking in hypertensive and diabetic patients with normal left atrial size. J. Am. Soc. Echocardiogr. 2011, 24, 898–908. [Google Scholar] [CrossRef]
- Kurt, M.; Wang, J.; Torre-Amione, G.; Nagueh, S.F. Left atrial function in diastolic heart failure. Circ. Cardiovasc. Imaging 2009, 2, 10–15. [Google Scholar] [CrossRef]
- Pathan, F.; D’Elia, N.; Nolan, M.T.; Marwick, T.H.; Negishi, K. Normal Ranges of Left Atrial Strain by Speckle-Tracking Echocardiography: A Systematic Review and Meta-Analysis. J. Am. Soc. Echocardiogr. 2017, 30, 59–70.e8. [Google Scholar] [CrossRef]
- Shaikh, A.Y.; Maan, A.; Khan, U.A.; Aurigemma, G.P.; Hill, J.C.; Kane, J.L.; Tighe, D.A.; Mick, E.O.; McManus, D.D. Speckle echocardiographic left atrial strain and stiffness index as predictors of maintenance of sinus rhythm after cardioversion for atrial fibrillation: A prospective study. Cardiovasc. Ultrasound 2012, 10, 1. [Google Scholar] [CrossRef]
- Ma, X.X.; Boldt, L.H.; Zhang, Y.L.; Zhu, M.R.; Hu, B.; Parwani, A.; Belyavskiy, E.; Radha Krishnan, A.K.; Krisper, M.; Köhncke, C.; et al. Clinical Relevance of Left Atrial Strain to Predict Recurrence of Atrial Fibrillation after Catheter Ablation: A Meta-Analysis. Echocardiography 2016, 33, 724–733. [Google Scholar] [CrossRef] [PubMed]
- Parwani, A.S.; Morris, D.-A.; Blaschke, F.; Huemer, M.; Pieske, B.; Haverkamp, W.; Boldt, L.-H. Left atrial strain predicts recurrence of atrial arrhythmias after catheter ablation of persistent atrial fibrillation. Open Heart 2017, 4, e000572. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| PACs ≤ 24 (n = 25) | PACs > 24 (n = 25) | p-Value | |
|---|---|---|---|
| Clinical Characteristics | |||
| Age (years) | 33.8 ± 8.6 | 41.4 ± 8.2 | 0.002 |
| Male gender, n (%) | 15(60) | 10 (40) | 0.258 |
| BSA (m²) | 1.7 ± 0.2 | 1.8 ± 0.2 | 0.281 |
| Blood Transfusions Duration (years) | 32 ± 8.9 | 39 ± 8.6 | 0.007 |
| Blood Transfusion Frequency (days) | 15 ± 3.7 | 14 ± 4.6 | 0.16 |
| Smoking, n(%) | 8 (16) | 7 (14) | 0.73 |
| Hypertension, n (%) | 0 (0) | 0 (0) | 1 |
| Diabetes, n (%) | 3 (6) | 2 (4) | 1 |
| Dyslipidemia, n (%) | 1 (2) | 0(0) | 1 |
| Chronic Kidney Disease, n (%) | 0(0) | 0(0) | 1 |
| Osteoporosis, n (%) | 7(14) | 7(14) | 1 |
| Splenectomy, n (%) | 10 (20) | 13 (26) | 0.571 |
| Biochemical Parameters | |||
| Hemoglobin (g/dL) | 10.2 ± 0.7 | 10.2 ± 0.7 | 0.877 |
| Total Bilirubin (mg/dL) | 2.04 ± 1.2 | 1.5 ± 0.7 | 0.059 |
| Direct Bilirubin (mg/dL) | 0.56 ± 0.23 | 0.42 ± 0.19 | 0.053 |
| Indirect Bilirubin (mg/dL) | 1.49 ± 1 | 1.1 ± 0.6 | 0.122 |
| LDH (U/L) | 258.1 ± 87 | 261.4 ± 116.2 | 0.915 |
| Ferritin (ng/mL) | 1008.3 ± 790 | 1037.4 ± 1198.5 | 0.92 |
| 24-Hour Holter Parameters | |||
| Minimum HR (bpm) | 59.7 ± 5.3 | 57 ± 6.5 | 0.885 |
| Maximum HR (bpm) | 126.4 ± 14.4 | 127 ± 18.4 | 0.132 |
| Mean HR (bpm)Median value of PACs | 84.1 ± 7.42 (0–9) | 79.5 ± 8.8131 (61–288) | 0.05<0.001 |
| Patients with PVCs, n (%) | 9 (18) | 17 (34) | 0.061 |
| PACs ≤ 24 (n = 25) | PACs > 24 (n = 25) | p-Value | |
|---|---|---|---|
| Echocardiographic Parameters | |||
| Left Ventricular Ejection Fraction(%) | 61.7 ± 4.2 | 62.6 ± 5.9 | 0.546 |
| Stroke Volume index (ml/m²) | 41.4 ± 7.6 | 38.4 ± 6.7 | 0.162 |
| Cardiac index (L/min m²) | 3.1 ± 0.6 | 2.9 ± 0.5 | 0.145 |
| Left Ventricular End-Diastolic Diameter (cm) | 4.6 ± 0.5 | 4.9 ± 0.4 | 0.04 |
| Left Ventricular End-Systolic Diameter (cm) | 3 ± 0.5 | 3 ± 0.5 | 0.712 |
| Left Ventricular Mass index (g/ m²) | 73.4 ± 16.7 | 82.6 ± 16.9 | 0.076 |
| Relative Wall Thickness | 0.36 ± 0.05 | 0.35 ± 0.06 | 0.492 |
| Left Atrial Volume index (ml/m²) | 30.5 ± 12.7 | 33.1 ± 10 | 0.422 |
| Left Atrial Peak Systolic Strain (%) | 37.2 ± 6.5 | 30.4 ± 7.8 | 0.002 |
| Left Ventricular Global Longitudinal Strain (%) | 20.5 ± 3 | 19.5 ± 2.4 | 0.206 |
| Mitral Valve E/A velocity ratio | 1.42 ± 0.4 | 1.41 ± 0.5 | 0.935 |
| Mitral Valve E/E’ ratio average | 6.6 ± 1.8 | 8.3 ± 2.9 | 0.02 |
| Right Ventricular End-Diastolic Basal Diameter (cm) | 3.2 ± 0.5 | 3.3 ± 0.5 | 0.523 |
| Right Atrium Area (cm²) | 13.1 ± 2.5 | 13.6 ± 2.4 | 0.456 |
| Right Ventricular Fractional Area Change (%) | 49.9 ± 8.7 | 50 ± 5.8 | 0.979 |
| TAPSE (cm) | 2.4 ± 0.2 | 2.4 ± 0.3 | 0.745 |
| Right Ventricular S’ (cm/s) | 15.6 ± 2.7 | 14.5 ± 2.3 | 0.103 |
| Tricuspid Regurgitation maximal velocity(m/s) | 2.0 ± 0.4 | 2.4 ± 0.4 | 0.001 |
| Right Ventricular Systolic Pressure (mm Hg) | 21.1 ± 6 | 27.2 ± 7 | 0.003 |
| Right Atrial Pressure (mmHg) | 3.7 ± 2.6 | 3.2 ± 1 | 0.389 |
| Cardiac Magnetic ResonanceT2* | |||
| T2* (ms) | 35.6 ± 9.8 | 30.5 ± 9.3 | 0.068 |
| Univariate Analysis | |||
|---|---|---|---|
| OR | 95% CI | p-Value | |
| ClinicalParameters | |||
| Age (years) | 1.121 | 1.032–1.217 | 0.007 |
| Male | 0.444 | 0.143–1.378 | 0.160 |
| BSA (m²) | 4.678 | 0.291–75.255 | 0.276 |
| Blood Transfusions Duration (years) | 1.101 | 1.019–1.188 | 0.014 |
| Blood transfusion frequency (days) | 0.906 | 0.789–1.041 | 0.163 |
| Smokers | 1.658 | 0.405–6.785 | 0.482 |
| Diabetes | 0.638 | 0.097–4.188 | 0.639 |
| Osteoporosis | 0.944 | 0.273–3.263 | 0.928 |
| Splenectomy | 1.773 | 0.571–5.507 | 0.322 |
| Biochemical Parameters | |||
| Hemoglobin (g/dL) | 1.065 | 0.489–2.322 | 0.874 |
| Total Bilirubin (mg/dL) | 0.549 | 0.288–1.049 | 0.069 |
| Direct Bilirubin (mg/dL) | 0.064 | 0.003–1.257 | 0.07 |
| Indirect Bilirubin (mg/dL) | 0.563 | 0.268–1.184 | 0.130 |
| LDH (U/L) | 1 | 0.994–1.006 | 0.913 |
| Ferritin (ng/mL) | 1 | 0.999–1.001 | 0.918 |
| 24-Hour Holter Parameters | |||
| Minimum HR (bpm) | 0.932 | 0.850–1.022 | 0.134 |
| Maximum HR (bpm) | 1.003 | 0.969–1.038 | 0.882 |
| Mean HR (bpm) | 0.930 | 0.864–1.002 | 0.056 |
| Patients with PVCs (n, %) | 2.372 | 0.803–7.006 | 0.118 |
| Multivariable Analysis | Model Comparison | |||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value * | −2 log Likelihood | Chi-Square | p-Value † | |
| Model 1 (Clinical) | 61.709 | 7.61 | - | |||
| Blood transfusion duration, years | 1.10 | 1.02–1.19 | 0.014 | |||
| Model 2 (Clinical + biochemical) | 54.290 | 9.39 | 0.009 | |||
| Blood transfusion duration, years | 1.09 | 1.01–1.18 | 0.03 | |||
| Total Bilirubin, mg/dl | 0.67 | 0.34–1.33 | 0.25 | |||
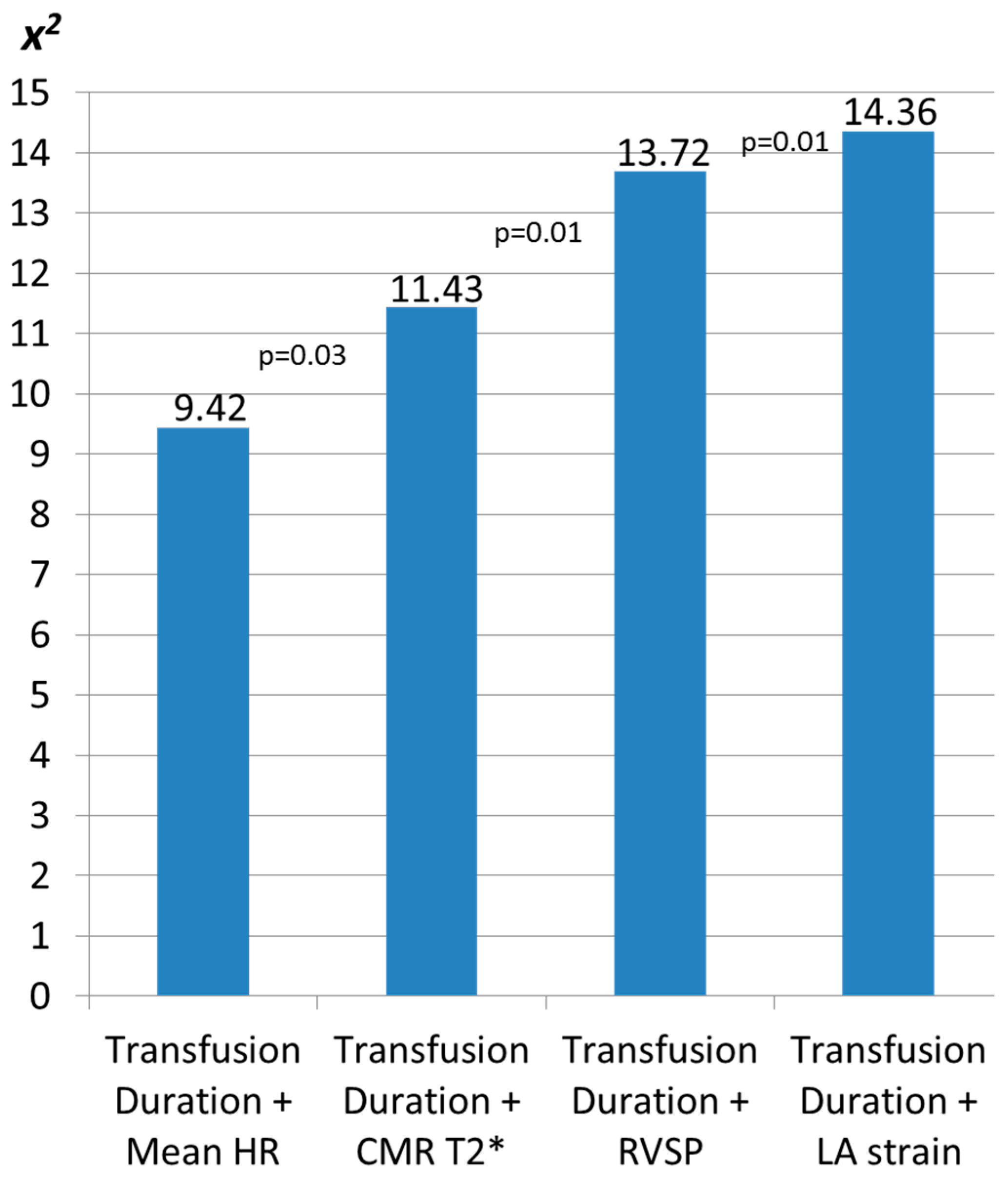
| Model 3 (Clinical + Holter) | 59.89 | 9.43 | 0.009 | |||
| Blood transfusion duration, years | 1.09 | 1.01–1.18 | 0.03 | |||
| Mean heart rate, beats per minute | 0.95 | 0.88–1.03 | 0.19 | |||
| Univariate Analysis | |||
|---|---|---|---|
| OR | 95% CI | p-Value | |
| Echocardiographic Parameters | |||
| Left Ventricular Ejection Fraction (%) | 1.036 | 0.926–1.158 | 0.538 |
| Stroke Volume index (mL/m²) | 0.941 | 0.864–1.025 | 0.165 |
| Cardiac Output index (L/min m²) | 0.427 | 0.134–1.364 | 0.151 |
| Left Ventricular End-Diastolic Diameter (cm) | 4.522 | 1.009–20.280 | 0.049 |
| Left Ventricular End-Systolic Diameter (cm) | 0.801 | 0.255–2.517 | 0.704 |
| Left Ventricular Mass index (g/m²) | 1.036 | 0.995–1.078 | 0.086 |
| Relative Wall Thickness | 0.018 | 0.001–1429 | 0.484 |
| Left Atrial Volume index (mL/m²) | 1.021 | 0.971–1.074 | 0.417 |
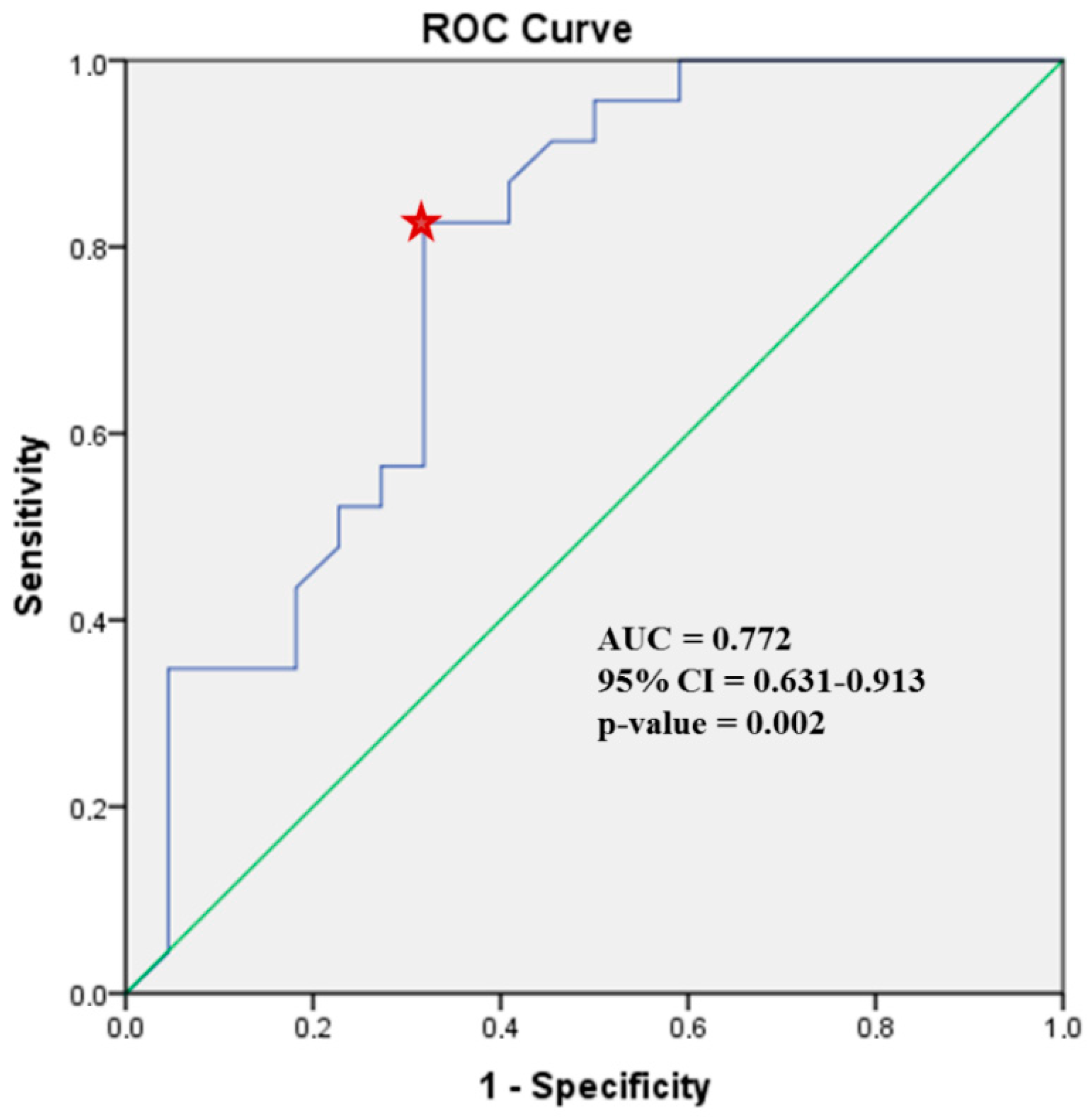
| Left Atrial Peak Systolic Strain (%) | 0.869 | 0.783–0.964 | 0.008 |
| Left Ventricular Global Longitudinal Strain (%) | 0.870 | 0702–1.079 | 0.205 |
| Mitral Valve E/A velocity ratio | 0.947 | 0.268–3.353 | 0.933 |
| Mitral Valve E/E’ ratio average | 1.407 | 1.028–1.926 | 0.033 |
| Right Ventricular End-Diastolic Basal Diameter (cm) | 1.535 | 0.423–5.565 | 0.514 |
| Right Atrium Area (cm²) | 1.101 | 0.858–1.411 | 0.446 |
| Right Ventricular Fractional Area Change (%) | 1.001 | 0.924–1.085 | 0.978 |
| TAPSE (cm) | 0.669 | 0.064–7.036 | 0.738 |
| Right Ventricular S’ (cm/s) | 0.820 | 0.644–1.045 | 0.108 |
| Right Ventricular Systolic Pressure (mm Hg) | 1.147 | 1.039–1.266 | 0.006 |
| Right Atrial Pressure (mmHg) | 0.857 | 0.590–1.245 | 0.418 |
| Cardiac Magnetic Resonance T2* | |||
| T2* (ms) | 0.937 | 0.870–1.009 | 0.086 |
| Multivariable Analysis | Model Comparison | |||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value * | −2 log Likelihood | Chi-Square | p-Value † | |
| Model 1 (CMR) | 65.59 | 3.72 | - | |||
| CMR T2*, msecs | 0.94 | 0.87–1.01 | 0.08 | |||
| Model 2 (CMR + ECHO) | 55.95 | 6.41 | 0.04 | |||
| CMR T2*, msecs | 0.95 | 0.88–1.03 | 0.20 | |||
| LVEDd, cm | 3.89 | 0.85–17.85 | 0.08 | |||
| Model 3 (CMR + ECHO) | 60.96 | 8.35 | 0.02 | |||
| CMR T2*, msecs | 0.95 | 0.88–1.02 | 0.17 | |||
| E/e’ ratio average | 1.37 | 0.99–1.90 | 0.06 | |||
| Model 4 (CMR + ECHO) | 55.57 | 11.84 | 0.003 | |||
| CMR T2*, msecs | 0.93 | 0.85–1.02 | 0.12 | |||
| RVSP, mmHg | 1.15 | 1.04–1.27 | 0.008 | |||
| Model 5 (CMR + ECHO) | 50.52 | 12.34 | 0.002 | |||
| CMR T2*, msecs | 0.94 | 0.86–1.03 | 0.19 | |||
| LA Strain, % | 0.87 | 0.79–0.97 | 0.01 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vlachou, M.; Kamperidis, V.; Vlachaki, E.; Tziatzios, G.; Pantelidou, D.; Boutou, A.; Apostolou, C.; Papadopoulou, D.; Giannakoulas, G.; Karvounis, H. Left Atrial Strain Identifies Increased Atrial Ectopy in Patients with Beta-Thalassemia Major. Diagnostics 2021, 11, 1. https://doi.org/10.3390/diagnostics11010001
Vlachou M, Kamperidis V, Vlachaki E, Tziatzios G, Pantelidou D, Boutou A, Apostolou C, Papadopoulou D, Giannakoulas G, Karvounis H. Left Atrial Strain Identifies Increased Atrial Ectopy in Patients with Beta-Thalassemia Major. Diagnostics. 2021; 11(1):1. https://doi.org/10.3390/diagnostics11010001
Chicago/Turabian StyleVlachou, Maria, Vasileios Kamperidis, Efthymia Vlachaki, Georgios Tziatzios, Despoina Pantelidou, Afroditi Boutou, Chrysa Apostolou, Despoina Papadopoulou, George Giannakoulas, and Haralambos Karvounis. 2021. "Left Atrial Strain Identifies Increased Atrial Ectopy in Patients with Beta-Thalassemia Major" Diagnostics 11, no. 1: 1. https://doi.org/10.3390/diagnostics11010001
APA StyleVlachou, M., Kamperidis, V., Vlachaki, E., Tziatzios, G., Pantelidou, D., Boutou, A., Apostolou, C., Papadopoulou, D., Giannakoulas, G., & Karvounis, H. (2021). Left Atrial Strain Identifies Increased Atrial Ectopy in Patients with Beta-Thalassemia Major. Diagnostics, 11(1), 1. https://doi.org/10.3390/diagnostics11010001