Concurrent Validity of Digital Vascular Auscultation for the Assessment of Blood Flow Obliteration on the Radial Artery in Healthy Subjects

 ,
,  ,
,  , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
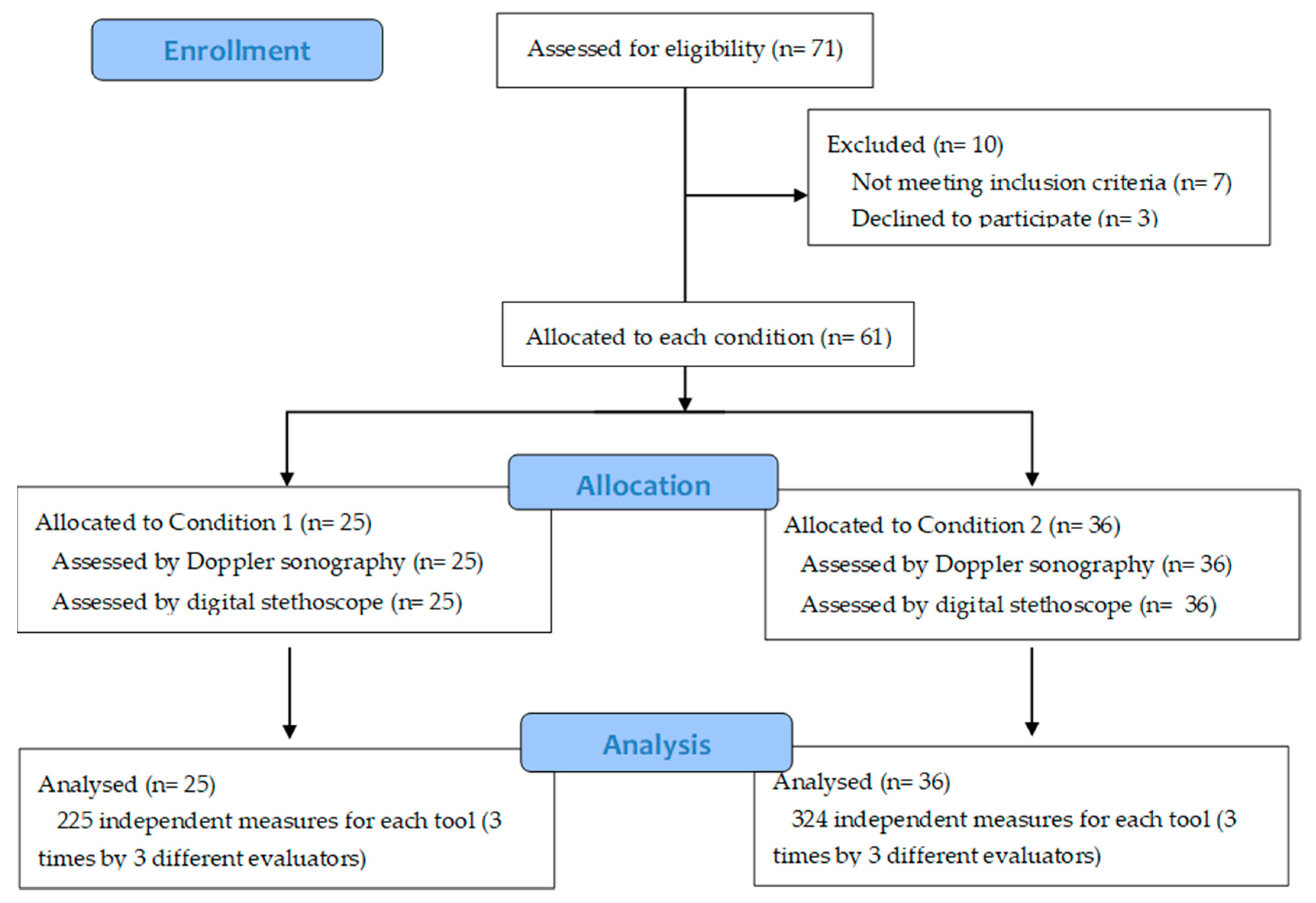
2.1. Subjects
2.2. Instruments
2.3. Procedure
Assessment
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Laulan, J.; Fouquet, B.; Rodaix, C.; Jauffret, P.; Roquelaure, Y.; Descatha, A. Thoracic outlet syndrome: Definition, aetiological factors, diagnosis, management and occupational impact. J. Occup. Rehabil. 2011, 21, 366–373. [Google Scholar] [CrossRef]
- Illig, K.A.; Donahue, D.; Duncan, A.; Freischlag, J.; Gelabert, H.; Johansen, K.; Jordan, S.; Sanders, R.; Thompson, R. Reporting standards of the Society for Vascular Surgery for thoracic outlet syndrome. J. Vasc. Surg. 2016, 64, e23–e35. [Google Scholar] [CrossRef]
- Ferrante, M.A.; Ferrante, N.D. The thoracic outlet syndromes: Part 1. Overview of the thoracic outlet syndromes and review of true neurogenic thoracic outlet syndrome. Muscle Nerve 2017, 55, 782–793. [Google Scholar] [CrossRef] [PubMed]
- Ferrante, M.A.; Ferrante, N.D. The thoracic outlet syndromes: Part 2. The Arterial, Venous, Neurovascular and Disputed Thoracic Outlet Syndrome. Muscle Nerve 2017, 56, 663–673. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.; Xu, Z.; Chen, J.; Liu, Z.; Wang, T.; Hu, Y.; Shen, L.; Xue, F. A novel approach for imaging of thoracic outlet syndrome using contrast-enhanced magnetic resonance angiography (CE-MRA), short inversion time inversion recovery sampling perfection with application-optimized contrasts using different flip angle evolution. Med. Sci. Monit. 2019, 25, 7617–7623. [Google Scholar] [CrossRef] [PubMed]
- Weaver, M.; Lum, Y. New Diagnostic and Treatment Modalities for Neurogenic Thoracic Outlet Syndrome. Diagnostics 2017, 7, 28. [Google Scholar] [CrossRef] [PubMed]
- Povlsen, S.; Povlsen, B. Diagnosing thoracic outlet syndrome: Current approaches and future directions. Diagnostics 2018, 8, 21. [Google Scholar] [CrossRef]
- Masocatto, N.O.; Da-Matta, T.; Prozzo, T.G.; Couto, W.J.; Porfirio, G. Thoracic outlet syndrome: A narrative review. Revista do Colégio Brasileiro de Cirurgiões 2019, 46, 1–7. [Google Scholar]
- Hixson, K.; Horris, H.; Valovich-McLeod, T.; Welch-Bacon, C. The Diagnostic Accuracy of Clinical Diagnostic Tests for Thoracic Outlet Syndrome. J. Sport Rehabil. 2017, 26, 456–465. [Google Scholar] [CrossRef]
- Dessureault-Dober, I.; Bronchti, G.; Bussières, A. Diagnostic Accuracy of Clinical Tests for Neurogenic and Vascular Thoracic Outlet Syndrome: A Systematic Review. J. Manip. Physiol. Ther. 2018, 41, 789–799. [Google Scholar] [CrossRef]
- Jones, M.R.; Prabhakar, A.; Viswanath, O.; Urits, I.; Green, J.B.; Kendrick, J.B.; Brunk, A.J.; Eng, M.R.; Orhurhu, V.; Cornett, E.M.; et al. Thoracic Outlet Syndrome: A Comprehensive Review of Pathophysiology, Diagnosis, and Treatment. Pain Ther. 2019, 8, 5–18. [Google Scholar] [CrossRef]
- Gillard, J.; Pérez-Cousin, M.; Hachulla, É.; Remy, J.; Hurtevent, J.F.; Vinckier, L.; Thevénon, A.; Duquesnoy, B. Diagnosing thoracic outlet syndrome: Contribution of provocative tests, ultrasonography, electrophysiology, and helical computed tomography in 48 patients. Jt. Bone Spine 2001, 68, 416–424. [Google Scholar] [CrossRef]
- Likes, K.; Rochlin, D.H.; Salditch, Q.; Dapash, T.; Baker, Y.; Deguzman, R.; Selvarajah, S.; Freischlag, J.A. Diagnostic accuracy of physician and self-referred patients for thoracic outlet syndrome is excellent. Ann. Vasc. Surg. 2014, 28, 1100–1105. [Google Scholar] [CrossRef] [PubMed]
- Hardy, A.; Pougès, C.; Wavreille, G.; Behal, H.; Demondion, X.; Lefebvre, G. Thoracic Outlet Syndrome: Diagnostic Accuracy of MRI. Orthop. Traumatol. Surg. Res. 2019, 105, 1563–1569. [Google Scholar] [CrossRef] [PubMed]
- Molina, J.E.; D’Cunha, J. The vascular component in neurogenic-arterial thoracic outlet syndrome. Int. J. Angiol. 2008, 17, 83–87. [Google Scholar] [CrossRef] [PubMed]
- Özcan, H.N.; Kara, M.; Özcan, F.; Bostanoǧlu, S.; Karademir, M.A.; Erkin, G.; Özçakar, L. Dynamic doppler evaluation of the radial and ulnar arteries in patients with carpal tunnel syndrome. Am. J. Roentgenol. 2011, 197, 817–820. [Google Scholar] [CrossRef]
- Hartley, C.; Reddy, A.; Madala, S.; Entman, M.; Taffet, G. Feasibility of dual Doppler velocity measurements to estimate volume pulsations of an arterial segment. Ultrasound Med. Biol. 2010, 36, 1169–1175. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3624763/pdf/nihms412728.pdf (accessed on 18 March 2020). [CrossRef]
- Demondion, X.; Vidal, C.; Herbinet, P.; Gautier, C.; Duquesnoy, B.; Cotton, A. Ultrasonographic assessment of arterial cross-sectional area in the thoracic outlet on postural maneuvers measured with power Doppler ultrasonography in both asymptomatic and symptomatic populations. J. Ultrasound Med. 2006, 25, 217–224. [Google Scholar] [CrossRef]
- Makaryus, A.N.; Makaryus, J.N.; Figgatt, A.; Mulholland, D.; Kushner, H.; Semmlow, J.L.; Mieres, J.; Taylor, A.J. Utility of an advanced digital electronic stethoscope in the diagnosis of coronary artery disease compared with coronary computed tomographic angiography. Am. J. Cardiol. 2013, 111, 786–792. [Google Scholar] [CrossRef]
- Sztajzel, J.M.; Picard-Kossovsky, M.; Lerch, R.; Vuille, C.; Sarasin, F.P. Accuracy of cardiac auscultation in the era of Doppler-echocardiography: A comparison between cardiologists and internists. Int. J. Cardiol. 2010, 138, 308–310. [Google Scholar] [CrossRef]
- Takahashi, O.; Shimbo, T.; Rahman, M.; Musa, R.; Kurokawa, W.; Yoshinaka, T.; Fukui, T. Validation of the auscultatory method for diagnosing peripheral arterial disease. Fam. Pract. 2006, 23, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Carmo, G.; Mandil, A.; Nascimento, B.R.; Arantes, B.D.; Bittencourt, J.C.; Falqueto, E.B.; Ribeiro, A.L. Can we measure the ankle—Brachial index using only a stethoscope? A pilot study. Fam. Pract. 2009, 26, 22–26. [Google Scholar] [PubMed]
- Jou, L.D.; Mawad, M.E. Indirect measurement of aneurysm wall thickness using digital stethoscope. Neurol. Res. 2010, 32, 661–665. [Google Scholar] [CrossRef] [PubMed]
- Van Der Hoeven, N.V.; Van Den Born, B.J.H.; Van Montfrans, G.A. Reliability of palpation of the radial artery compared with auscultation of the brachial artery in measuring SBP. J. Hypertens. 2011, 29, 51–55. [Google Scholar] [CrossRef] [PubMed]
- Whiting, P.; Rutjes, W.; Westwood, M.; Mallet, S.; Deeks, J.; Reitsma, J.; Leeflang, M.M.G.; Sterne, J.A.C.; Bossuyt, P.M.M. QUADAS-2: A Revised Tool for the Quality Assessment of Diagnostic Accuracy Studies. Ann. Intern. Med. 2011, 55, 529–538. [Google Scholar] [CrossRef]
- Mokkink, L.B.; Terwee, C.B.; Patrick, D.L.; Alonso, J.; Stratford, P.W.; Knol, D.L.; Bouter, L.M.; de Vet, H.C.W. The COSMIN checklist for assessing the methodological quality of studies on measurement properties of health status measurement instruments: An international Delphi study. Qual. Life Res. 2010, 19, 539–549. [Google Scholar] [CrossRef] [PubMed]
- Perloff, D.; Grim, C.; Flack, J.; Frohlich, E.D.; Hill, M.; McDonald, M.; Morgenstern, B.Z. Human Blood Pressure Determination by Sphygmomanometry. Circulation 1993, 88, 2460–2470. [Google Scholar] [CrossRef]
- Endres, H.G.; Hucke, C.; Holland-Letz, T.; Trampisch, J. A new efficient trial design for assessing reliability of ankle-brachial index measures by three different observer groups. BMC Cardiovasc. Disord. 2006, 6, 1–10. [Google Scholar] [CrossRef]
- Chesbro, S.B.; Asongwed, E.T.; Brown, J.; John, E.B. Reliability of doppler and stethoscope methods of determining systolic blood pressures: Considerations for calculating an ankle-brachial index. J. Natl. Med. Assoc. 2011, 103, 863–869. [Google Scholar] [CrossRef]
- Kaufmann, C.; Jacomella, V.; Kovacicova, L.; Husmann, M.; Clemens, R.K.; Thalhammer, C.; Amannvesti, B. Predictive value of auscultation of femoropopliteal arteries. Swiss Med. Wkly. 2013, 143, 1–5. [Google Scholar] [CrossRef]


{kind=link}
| Sample Characteristics | Study Group | Total | Chi-Squared | p-Value | ||
|---|---|---|---|---|---|---|
| Condition 1 | Condition 2 | |||||
| Gender | Male | 8 | 10 | 18 | 0.126 | 0.722 |
| Female | 17 | 26 | 43 | |||
| Aged | 20–29 | 3 | 7 | 10 | 2.622 | 0.758 |
| 30–39 | 1 | 2 | 3 | |||
| 40–49 | 4 | 5 | 9 | |||
| 50–59 | 2 | 6 | 8 | |||
| 60–69 | 13 | 15 | 28 | |||
| 70–79 | 2 | 1 | 3 | |||
| Handedness | Right | 23 | 34 | 57 | 0.114 | 0.704 |
| Left | 2 | 2 | 4 | |||
| Tobacco consumption | Smoker | 3 | 3 | 6 | 1.740 | 0.419 |
| Former smoker | 4 | 11 | 15 | |||
| Non-smoker | 18 | 22 | 40 | |||
| Treatment for Hypertension | Yes | 13 | 17 | 30 | 0.135 | 0.714 |
| No | 12 | 19 | 31 | |||
| Diabetes | Yes | 4 | 7 | 11 | 0.118 | 0.731 |
| No | 21 | 29 | 50 | |||
| Hypertension non-diabetic(BP of [140/90] mmHg) | Yes | 13 | 16 | 29 | 0.338 | 0.561 |
| No | 12 | 20 | 32 | |||
| Hypertension diabetic(BP of [130/80] mmHg) | Yes | 4 | 6 | 10 | 0.005 | 0.945 |
| No | 21 | 30 | 51 | |||
| Tool | Study Group | p-Value | ||
|---|---|---|---|---|
| Condition 1 | Condition 2 | |||
| Doppler | No change | 220 | 1 | <0.0001 |
| Change | 5 | 323 | ||
| Stethoscope | No change | 224 | 12 | <0.0001 |
| Change | 1 | 312 | ||
| Tool | Doppler | Total | Kappa | ASE | p-Value | ||
|---|---|---|---|---|---|---|---|
| No Change | Change | ||||||
| Stethoscope | No change | 220 (40.1%) | 16 (2.9%) | 236 | 0.936 | 0.015 | <0.0001 |
| Change | 1 (2%) | 312 (56.8%) | 313 | ||||
| Total | 221 (40.3%) | 328 (59.7%) | 549 | ||||
| Tool | Doppler | ||||
|---|---|---|---|---|---|
| Yes | No | Total | |||
| Stethoscope | Yes | 312 | 1 | 313 | |
| No | 16 | 220 | 236 | ||
| Total | 328 | 221 | 549 | ||
| Se 0.95 (95%) | Sp 0.99 (99%) | PPV 0.99 (99%) | NPV 0.93 (93%) | LR+ 95 | LR− 0.05 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cortés-Vega, M.-D.; Casuso-Holgado, M.J.; Oliva-Pascual-Vaca, Á.; García-Bernal, M.-I.; González-García, P.; Rodríguez-Blanco, C. Concurrent Validity of Digital Vascular Auscultation for the Assessment of Blood Flow Obliteration on the Radial Artery in Healthy Subjects. Diagnostics 2020, 10, 494. https://doi.org/10.3390/diagnostics10070494
Cortés-Vega M-D, Casuso-Holgado MJ, Oliva-Pascual-Vaca Á, García-Bernal M-I, González-García P, Rodríguez-Blanco C. Concurrent Validity of Digital Vascular Auscultation for the Assessment of Blood Flow Obliteration on the Radial Artery in Healthy Subjects. Diagnostics. 2020; 10(7):494. https://doi.org/10.3390/diagnostics10070494
Chicago/Turabian StyleCortés-Vega, María-Dolores, María Jesús Casuso-Holgado, Ángel Oliva-Pascual-Vaca, María-Isabel García-Bernal, Paula González-García, and Cleofás Rodríguez-Blanco. 2020. "Concurrent Validity of Digital Vascular Auscultation for the Assessment of Blood Flow Obliteration on the Radial Artery in Healthy Subjects" Diagnostics 10, no. 7: 494. https://doi.org/10.3390/diagnostics10070494
APA StyleCortés-Vega, M.-D., Casuso-Holgado, M. J., Oliva-Pascual-Vaca, Á., García-Bernal, M.-I., González-García, P., & Rodríguez-Blanco, C. (2020). Concurrent Validity of Digital Vascular Auscultation for the Assessment of Blood Flow Obliteration on the Radial Artery in Healthy Subjects. Diagnostics, 10(7), 494. https://doi.org/10.3390/diagnostics10070494