Laboratory Diagnosis of Paratyphoid Fever: Opportunity of Surface Plasmon Resonance

 ,
,  , , , , and
, , , , and
Abstract
1. Introduction
2. Paratyphoid Fever
3. Laboratory Diagnostic Approaches
3.1. Bacterial Culture
3.2. Serology
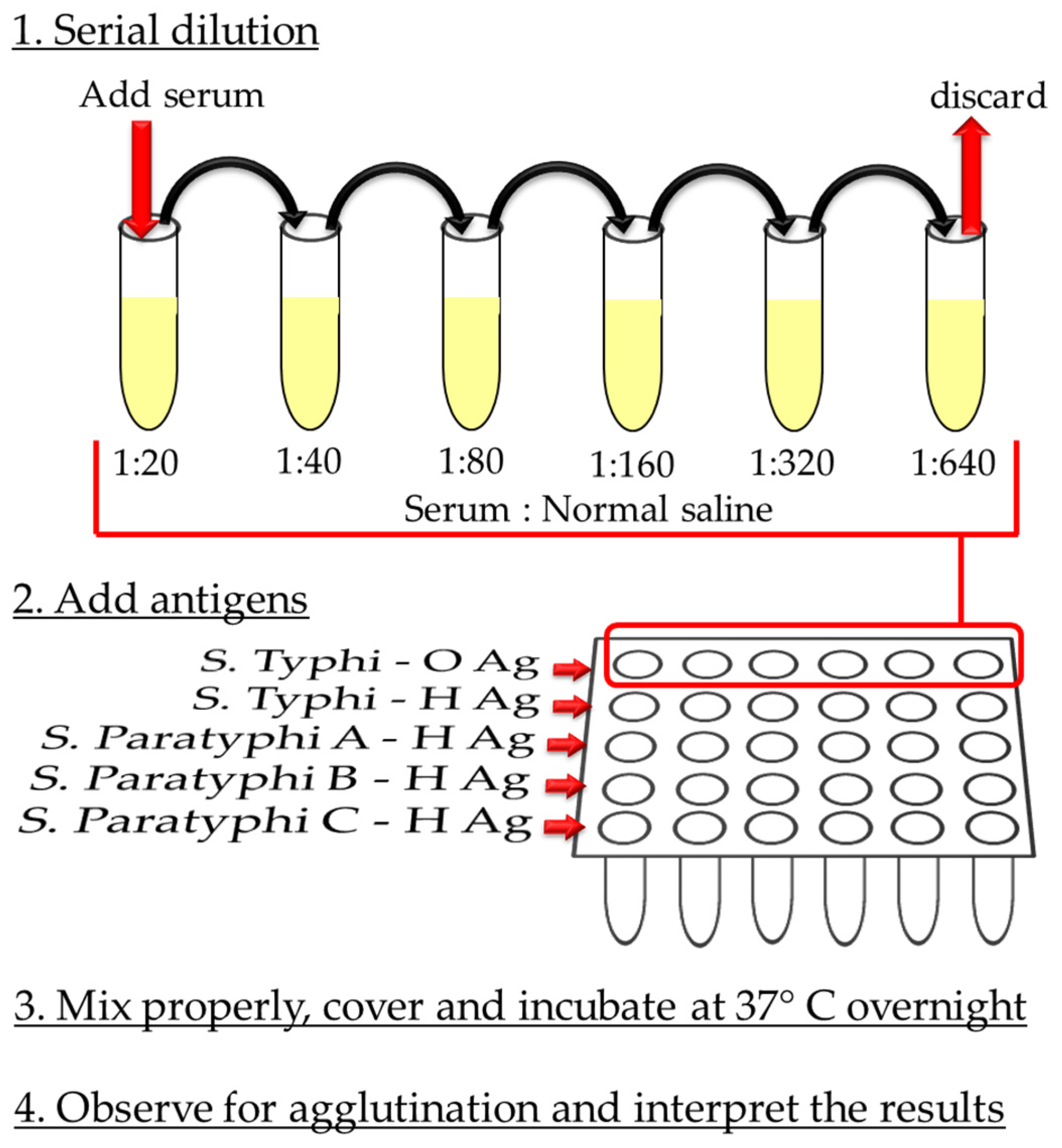
3.2.1. Widal Test
3.2.2. ELISA
3.2.3. Other Tests
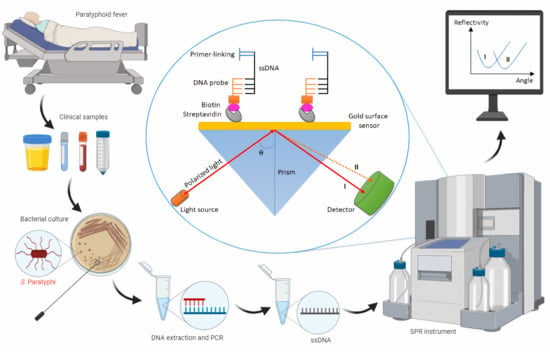
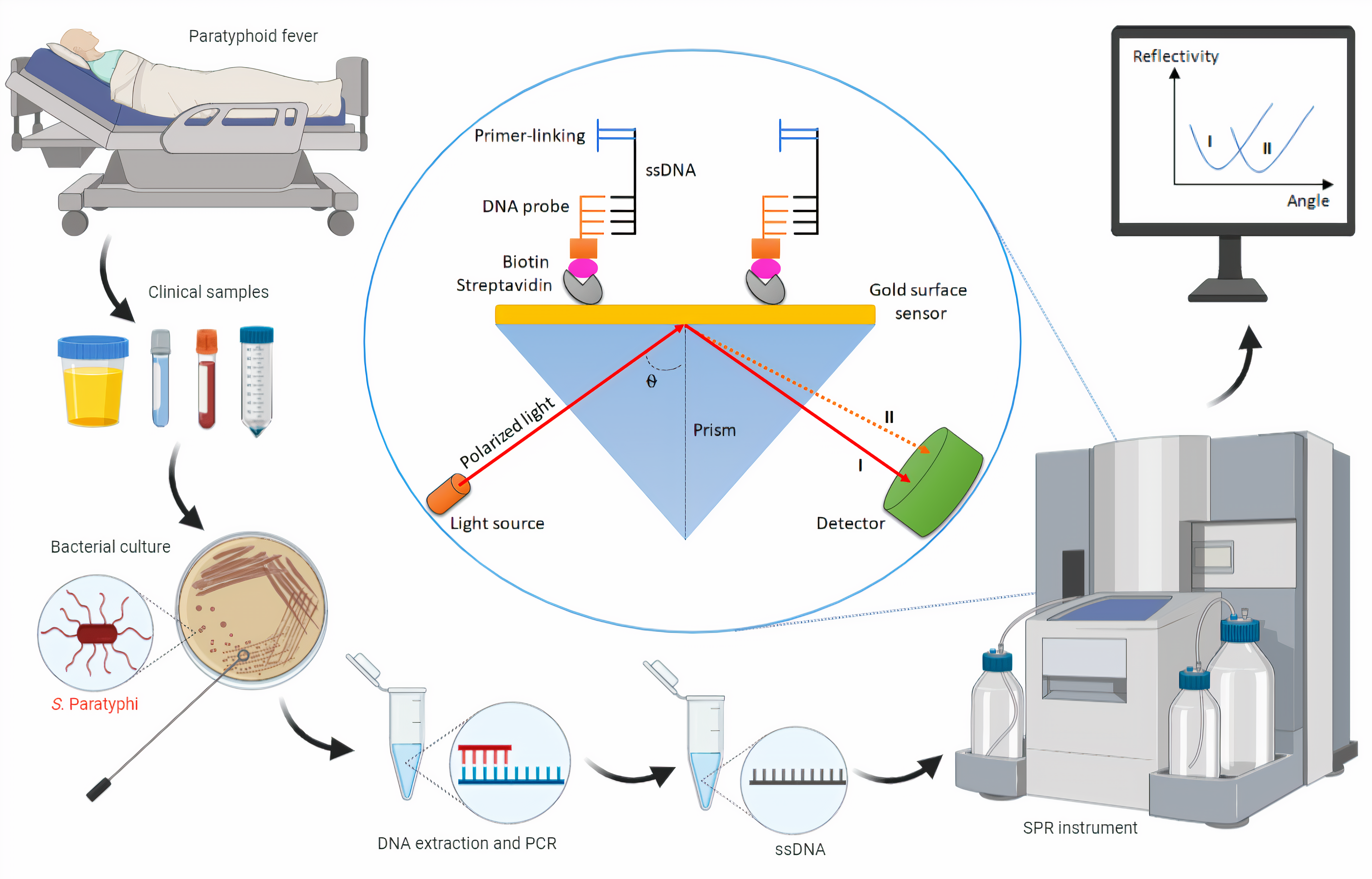
3.3. Nucleic Acid-Based Diagnostics
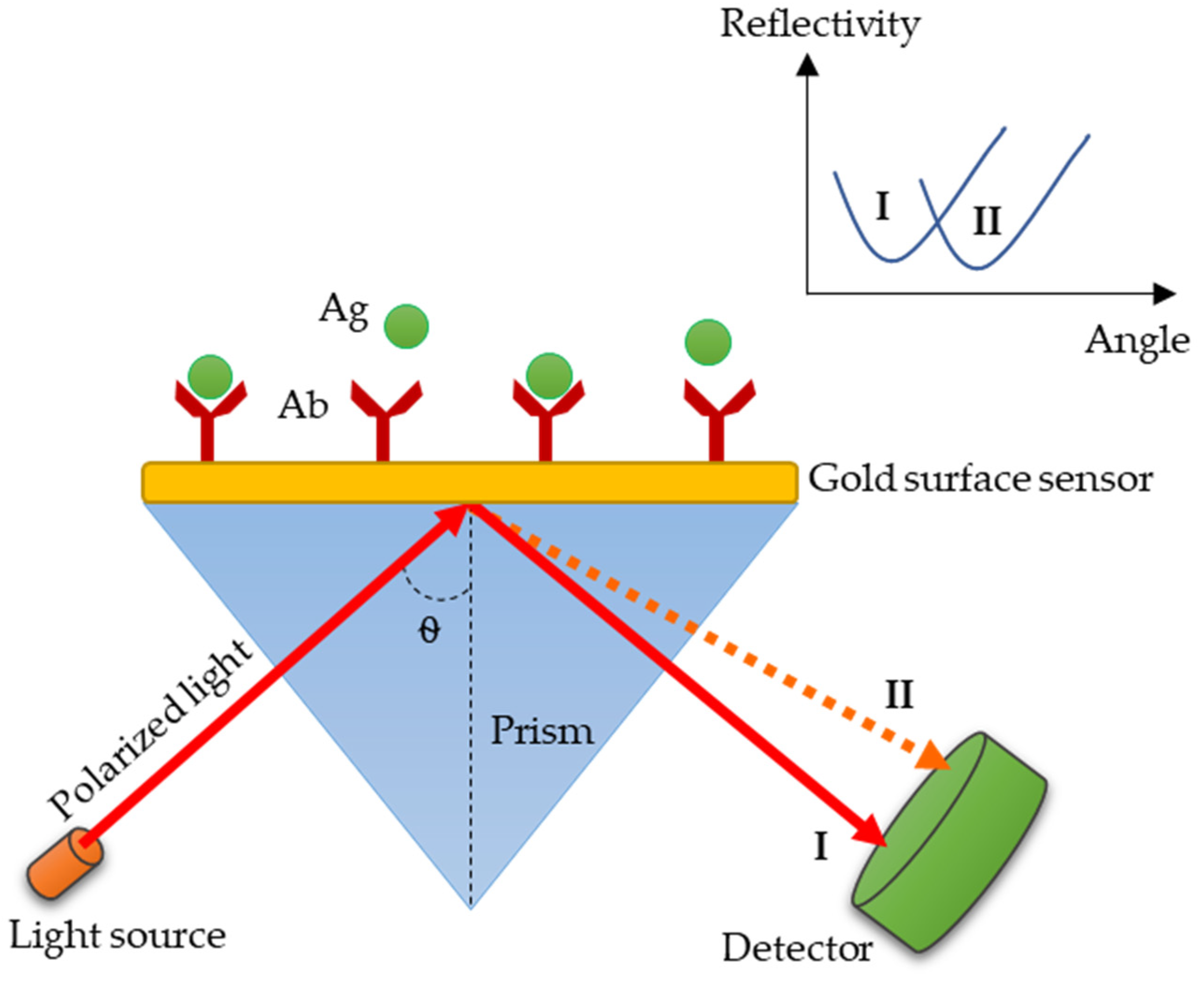
3.4. SPR: A Promising Technology for Paratyphoid Diagnosis
4. Conclusions and Future Directions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ryan, M.P.; O’Dwyer, J.; Adley, C.C. Evaluation of the Complex Nomenclature of the Clinically and Veterinary Significant Pathogen Salmonella. BioMed. Res. Int. 2017, 2017, 1–6. [Google Scholar] [CrossRef]
- Morse, S.A.; Mietzner, T.A.; Miller, S.; Riedel, S. Jawetz Melnick & Adelbergs Medical Microbiology 28 E; McGraw-Hill Education: New York, NY, USA, 2019. [Google Scholar]
- Grimont, P.A.; Weill, F.-X. Antigenic Formulae of the Salmonella Serovars; WHO Collaborating Centre for Reference and Research on Salmonella: Paris, France, 2007; pp. 1–166. [Google Scholar]
- Centers-for-Disease-Control-and-Prevention. Serotypes and the Importance of Serotyping Salmonella. Available online: https://www.cdc.gov/salmonella/reportspubs/salmonella-atlas/serotyping-importance.html (accessed on 16 April 2020).
- Jajere, S.M. A review of Salmonella enterica with focus on the pathogenicity and virulence factors, host specificity and antimicrobial resistance including multidrug resistance. Vet. World 2019, 12, 504–521. [Google Scholar] [CrossRef]
- Shelobolina, E.S.; Sullivan, S.A.; O’Neill, K.R.; Nevin, K.P.; Lovley, D.R. Isolation, Characterization, and U(VI)-Reducing Potential of a Facultatively Anaerobic, Acid-Resistant Bacterium from Low-pH, Nitrate- and U(VI)-Contaminated Subsurface Sediment and Description of Salmonella subterranea sp. nov. Appl. Environ. Microbiol. 2004, 70, 2959–2965. [Google Scholar] [CrossRef]
- Brenner, F.W.; Villar, R.G.; Angulo, F.J.; Tauxe, R.; Swaminathan, B. Salmonella Nomenclature. J. Clin. Microbiol. 2000, 38, 2465–2467. [Google Scholar] [CrossRef] [PubMed]
- Porwollik, S.; Boyd, E.F.; Choy, C.; Cheng, P.; Florea, L.; Proctor, E.; McClelland, M. Characterization of Salmonella enterica Subspecies I Genovars by Use of Microarrays. J. Bacteriol. 2004, 186, 5883–5898. [Google Scholar] [CrossRef] [PubMed]
- Gal-Mor, O.; Boyle, E.C.; Grassl, G.A. Same species, different diseases: How and why typhoidal and non-typhoidal Salmonella enterica serovars differ. Front. Microbiol. 2014, 5, 391. [Google Scholar] [CrossRef]
- Bennett, J.E.; Dolin, R.; Blaser, M.J. Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases; Elsevier: Amsterdam, The Netherlands, 2019. [Google Scholar]
- Vollaard, A.M.; Ali, S.; Widjaja, S.; van Asten, H.A.; Visser, L.G.; Surjadi, C.; van Dissel, J.T. Identification of typhoid fever and paratyphoid fever cases at presentation in outpatient clinics in Jakarta, Indonesia. Trans. R. Soc. Trop. Med. Hyg. 2005, 99, 440–450. [Google Scholar] [CrossRef]
- Bhan, M.K.; Bahl, R.; Bhatnagar, S. Typhoid, and paratyphoid fever. Lancet 2005, 366, 749–762. [Google Scholar] [CrossRef]
- Maskey, A.P.; Day, J.; Tuan, P.Q.; E Thwaites, G.; Campbell, J.I.; Zimmerman, M.; Farrar, J.; Basnyat, B. Salmonella enterica Serovar Paratyphi A and S. enterica Serovar Typhi Cause Indistinguishable Clinical Syndromes in Kathmandu, Nepal. Clin. Infect. Dis. 2006, 42, 1247–1253. [Google Scholar] [CrossRef] [PubMed]
- John, J.; van Aart, C.J.C.; Grassly, N.C. The Burden of Typhoid and Paratyphoid in India: Systematic Review and Meta-analysis. PLoS Neglect. Trop. Dis. 2016, 10, e0004616. [Google Scholar] [CrossRef]
- Sahastrabuddhe, S.; Carbis, R.; Wierzba, T.F.; Ochiai, L. Increasing rates of Salmonella paratyphi A and the status of its vaccine development. Expert Rev. Vaccines 2013, 12, 1021–1031. [Google Scholar] [CrossRef] [PubMed]
- Baker, S.; Favorov, M.; Dougan, G. Searching for the elusive typhoid diagnostic. BMC Infect. Dis. 2010, 10, 45. [Google Scholar] [CrossRef] [PubMed]
- Taj, M.K.; Panezai, M.; Nawaz, I.; Taj, I.; Panezai, M.; Panezai, N.; Zafar, U.; Muh, D.G.; Esso, S.A.; Muhammad, G. Isolation and Identification of Salmonella Paratyphi from Enteric Fever Patients at Different Hospitals of Quetta City. Pak. J. Boil. Sci. 2018, 21, 469–474. [Google Scholar] [CrossRef]
- Antillon, M.; Saad, N.J.; Baker, S.; Pollard, A.J.; Pitzer, V.E. The Relationship Between Blood Sample Volume and Diagnostic Sensitivity of Blood Culture for Typhoid and Paratyphoid Fever: A Systematic Review and Meta-Analysis. J. Infect. Dis. 2018, 218, S255–S267. [Google Scholar] [CrossRef]
- Ryan, E.T.; Hill, D.R.; Solomon, T.; Endy, T.P.; Aronson, N. Hunter’s Tropical Medicine and Emerging Infectious Diseases E-Book; Elsevier Health Sciences: Amsterdam, The Netherlands, 2019. [Google Scholar]
- Brunette, G.W. CDC Yellow Book 2018: Health Information for International Travel; Oxford University Press: Oxford, UK, 2017. [Google Scholar]
- Waddington, C.S.; Darton, T.C.; Pollard, A.J. The challenge of enteric fever. J. Infect. 2014, 68, S38–S50. [Google Scholar] [CrossRef]
- Appiah, G.D.; Hughes, M.J.; Chatham-Stephens, K. Typhoid & Paratyphoid Fever, Chapter 4. Travel-Related Infectious Diseases. In CDC Yellow Book; Centers of Disease Control and Prevention: Atlanta, GA, USA, 2014. [Google Scholar]
- Centers-for-Disease-Control-and-Prevention. Typhoid Fever and Paratyphoid Fever. Available online: https://www.cdc.gov/typhoid-fever/symptoms.html (accessed on 16 April 2020).
- Woh, P.Y.; Thong, K.L.; Lim, Y.A.L.; Behnke, J.M.; Lewis, J.W.; Zain, S.N.M. Microorganisms as an Indicator of Hygiene Status Among Migrant Food Handlers in Peninsular Malaysia. Asia Pac. J. Public Health 2017, 29, 599–607. [Google Scholar] [CrossRef] [PubMed]
- Vollaard, A.; Ali, S.; van Asten, H.A.G.H.; Widjaja, S.; Visser, L.G.; Surjadi, C.; van Dissel, J.T. Risk Factors for Typhoid and Paratyphoid Fever in Jakarta, Indonesia. JAMA 2004, 291, 2607. [Google Scholar] [CrossRef]
- Teh, C.S.J.; Chua, K.H.; Thong, K.L. Paratyphoid Fever: Splicing the Global Analyses. Int. J. Med. Sci. 2014, 11, 732–741. [Google Scholar] [CrossRef]
- Ngan, G.J.Y.; Ng, L.M.; Lin, R.T.; Teo, J.W. Development of a novel multiplex PCR for the detection and differentiation of Salmonella enterica serovars Typhi and Paratyphi A. Res. Microbiol. 2010, 161, 243–248. [Google Scholar] [CrossRef]
- Hu, L.; Li, B. Recent and the Latest Developments in Rapid and Efficient Detection of Salmonella in Food and Water. Adv. Tech. Boil. Med. 2017, 5. [Google Scholar] [CrossRef]
- Zhu, Q.; Lim, C.; Chan, Y. Detection of Salmonella typhi by polymerase chain reaction. J. Appl. Bacteriol. 1996, 80, 244–251. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Balakrishna, K.; Batra, H. Detection of Salmonella enterica serovar Typhi (S. Typhi) by selective amplification of invA, viaB, fliC-d and prt genes by polymerase chain reaction in mutiplex format. Lett. Appl. Microbiol. 2006, 42, 149–154. [Google Scholar] [CrossRef] [PubMed]
- Tennant, S.M.; Toema, D.; Qamar, F.; Iqbal, N.; Boyd, M.A.; Marshall, J.; Blackwelder, W.C.; Wu, Y.; Quadri, F.; Khan, A.; et al. Detection of Typhoidal and Paratyphoidal Salmonella in Blood by Real-time Polymerase Chain Reaction. Clin. Infect. Dis. 2015, 61, S241–S250. [Google Scholar] [CrossRef] [PubMed]
- Crump, J.A.; Sjölund-Karlsson, M.; Gordon, M.A.; Parry, C.M. Epidemiology, Clinical Presentation, Laboratory Diagnosis, Antimicrobial Resistance, and Antimicrobial Management of Invasive Salmonella Infections. Clin. Microbiol. Rev. 2015, 28, 901–937. [Google Scholar] [CrossRef]
- Wijedoru, L.; Mallett, S.; Parry, C.M. Rapid diagnostic tests for typhoid and paratyphoid (enteric) fever. Cochrane Database Syst. Rev. 2017, 5, CD008892. [Google Scholar] [CrossRef]
- Gordon, M.A.; Kankwatira, A.M.; Mwafulirwa, G.; Walsh, A.L.; Hopkins, M.J.; Parry, C.M.; Faragher, E.B.; Zijlstra, E.E.; Heyderman, R.S.; E Molyneux, M. Invasive Non-typhoid Salmonellae Establish Systemic Intracellular Infection in HIV-Infected Adults: An Emerging Disease Pathogenesis. Clin. Infect. Dis. 2010, 50, 953–962. [Google Scholar] [CrossRef]
- Wain, J.; Bay, P.V.B.; Vinh, H.; Duong, N.M.; Diep, T.S.; Walsh, A.L.; Parry, C.M.; Hasserjian, R.P.; Ho, V.A.; Hien, T.T.; et al. Quantitation of Bacteria in Bone Marrow from Patients with Typhoid Fever: Relationship between Counts and Clinical Features. J. Clin. Microbiol. 2001, 39, 1571–1576. [Google Scholar] [CrossRef]
- Parry, C.M.; Hien, T.T.; Dougan, G.; White, N.J.; Farrar, J. Typhoid Fever. N. Engl. J. Med. 2002, 347, 1770–1782. [Google Scholar] [CrossRef]
- Gal-Mor, O. Persistent Infection and Long-Term Carriage of Typhoidal and Nontyphoidal Salmonellae. Clin. Microbiol. Rev. 2018, 32, e00088-18. [Google Scholar] [CrossRef]
- Wain, J.; Diep, T.S.; Ho, V.A.; Walsh, A.M.; Hoa, N.T.T.; Parry, C.M.; White, N.J. Quantitation of Bacteria in Blood of Typhoid Fever Patients and Relationship between Counts and Clinical Features, Transmissibility, and Antibiotic Resistance. J. Clin. Microbiol. 1998, 36, 1683–1687. [Google Scholar] [CrossRef]
- Mogasale, V.; Ramani, E.; Mogasale, V.V.; Park, J. What proportion of Salmonella Typhi cases are detected by blood culture? A systematic literature reviews. Ann. Clin. Microbiol. Antimicrob. 2016, 15, 32. [Google Scholar] [CrossRef] [PubMed]
- Bharmoria, A. Typhoid Fever as a Challenge for Developing Countries and Elusive Diagnostic Approaches Available for the Enteric Fever. Int. J. Vaccine Res. 2017, 2, 1–16. [Google Scholar] [CrossRef]
- Sanderson, K.E.; Liu, S.-L.; Tang, L.; Johnston, R.N. Salmonella Typhi and Salmonella Paratyphi A. In Molecular Medical Microbiology; Elsevier BV: Amsterdam, The Netherlands, 2015; pp. 1275–1306. [Google Scholar]
- Pokhrel, B.M.; Karmacharya, R.; Mishra, S.K.; Koirala, J. Distribution of antibody titer against Salmonella enterica among healthy individuals in nepal. Ann. Clin. Microbiol. Antimicrob. 2009, 8, 1. [Google Scholar] [CrossRef]
- Andualem, G.; Abebe, T.; Kebede, N.; Gebreselassie, S.; Mihret, A.; Alemayehu, H. A comparative study of Widal test with blood culture in the diagnosis of typhoid fever in febrile patients. BMC Res. Notes 2014, 7, 653. [Google Scholar] [CrossRef]
- Aryal, S. Widal Test—Introduction, Principle, Procedure, Interpretation and Limitation. Microbiology Info. 2018. Available online: https://microbiologyinfo.com/widal-test-introduction-principle-procedure-interpretation-and-limitation/ (accessed on 16 April 2020).
- Olopoenia, L.; King, A.L. Widal agglutination test—100 years later: Still plagued by controversy. Postgrad. Med. J. 2000, 76, 80–84. [Google Scholar] [CrossRef]
- Kumar, S.; Balakrishna, K.; Batra, H.V. Enrichment-ELISA for Detection of Salmonella typhi From Food and Water Samples. Biomed. Environ. Sci. 2008, 21, 137–143. [Google Scholar] [CrossRef]
- Ng, S.P.; Tsui, C.O.; Roberts, D.; Chau, P.Y.; Ng, M.H. Detection, and serogroup differentiation of Salmonella spp. in food within 30 hours by enrichment-immunoassay with a T6 monoclonal antibody capture enzyme-linked immunosorbent assay. Appl. Environ. Microbiol. 1996, 62, 2294–2302. [Google Scholar] [CrossRef] [PubMed]
- Kuhn, K.G.; Falkenhorst, G.; Ceper, T.H.; Dalby, T.; Ethelberg, S.; Moelbak, K.; Krogfelt, K. Detecting non-typhoid Salmonella in humans by ELISAs: A literature review. J. Med. Microbiol. 2012, 61, 1–7. [Google Scholar] [CrossRef]
- Sojka, M.; Sayers, A.; Woodward, M.J. Analysis of expression of flagella by Salmonella enterica serotype Typhimurium by monoclonal antibodies recognising both phase specific and common epitopes. Vet. Microbiol. 2001, 78, 61–77. [Google Scholar] [CrossRef]
- Wang, W.; Liu, L.; Song, S.; Tang, L.; Kuang, H.; Xu, C. Highly Sensitive ELISA, and Immunochromatographic Strip for the Detection of Salmonella typhimurium in Milk Samples. Sensors 2015, 15, 5281–5292. [Google Scholar] [CrossRef]
- Alahi, E.E.; Mukhopadhyay, S. Detection Methodologies for Pathogen and Toxins: A Review. Sensors 2017, 17, 1885. [Google Scholar] [CrossRef] [PubMed]
- Min, J.; Song, E.K.; Kim, H.; Kim, K.T.; Park, T.J.; Kang, S. A Recombinant Secondary Antibody Mimic as a Target-specific Signal Amplifier, and an Antibody Immobilizer in Immunoassays. Sci. Rep. 2016, 6, 24159. [Google Scholar] [CrossRef] [PubMed]
- Sippel, J.; Bukhtiari, N.; Awan, M.B.; Krieg, R.; Duncan, J.F.; A Karamat, K.; Malik, I.A.; Igbal, L.M.; Legters, L. Indirect immunoglobulin G (IgG) and IgM enzyme-linked immunosorbent assays (ELISAs) and IgM capture ELISA for detection of antibodies to lipopolysaccharide in adult typhoid fever patients in Pakistan. J. Clin. Microbiol. 1989, 27, 1298–1302. [Google Scholar] [CrossRef]
- Sadallah, F.; Brighouse, G.; del Giudice, G.; Drager-Dayal, R.; Hodne, M.; Lambert, P.H. Production of Specific Monoclonal Antibodies to Salmonella typhi Flagellin and Possible Application to Immunodiagnosis of Typhoid Fever. J. Infect. Dis. 1990, 161, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.H.; Gong, J.; Zhang, J.; Wang, M.L.; Yang, J.; Wu, G.Z.; Quan, W.L.; Gong, H.M.; Szu, S.C. An outbreak of Salmonella Paratyphi A in a boarding school: A community-acquired enteric fever and carriage investigation. Epidemiol. Infect. 2010, 138, 1765–1774. [Google Scholar] [CrossRef] [PubMed]
- Ayyildiz, A.; Demir, Y.; Tuncel, E.; Babacan, M.; Leloğlu, S. Comparison of the Gruber-Widal and ELISA technics used to study Salmonella typhi and Salmonella paratyphi infections in patients. Mikrobiyol. Bulteni 1986, 20, 14–24. [Google Scholar]
- Li, M.-L.; Fang, H.-J.; Fan, X.; Zhang, J.; Yan, J.; Sun, A. Distribution of Salmonella paratyphi A outer membrane protein X gene and immune-protective effect related to its recombinant expressed products. Zhonghua Liu Xing Bing Xue Za Zhi 2013, 34, 1219–1222. [Google Scholar]
- Zhang, J.; Fan, X.; Ge, Y.; Yan, J.; Sun, A. Distribution of Salmonella paratyphi A pagC gene and immunoprotective effect of its recombinant expressed products. J. Zhejiang Univ. Med. Sci. 2013, 42, 171. [Google Scholar]
- Ruan, P.; Xia, X.-P.; Sun, D.; Ojcius, D.M.; Mao, Y.-F.; Yue, W.-Y.; Yan, J. Recombinant SpaO and H1a as immunogens for protection of mice from lethal infection with Salmonella paratyphi A: Implications for rational design of typhoid fever vaccines. Vaccine 2008, 26, 6639–6644. [Google Scholar] [CrossRef]
- Parry, C.M.; Wijedoru, L.; Arjyal, A.; Baker, S. The utility of diagnostic tests for enteric fever in endemic locations. Expert Rev. Anti-Infect. Ther. 2011, 9, 711–725. [Google Scholar] [CrossRef]
- Chart, H.; Cheasty, T.; de Pinna, E.; Siorvanes, L.; Wain, J.; Alam, D.; Nizami, Q.; Bhutta, Z.; Threlfall, E.J. Serodiagnosis of Salmonella enterica serovar Typhi and S. enterica serovars Paratyphi A, B and C human infections. J. Med. Microbiol. 2007, 56, 1161–1166. [Google Scholar] [CrossRef] [PubMed]
- Chaicumpa, W.; Thin-Inta, W.; Khusmith, S.; Tapchaisri, P.; Echeverria, P.; Kalambaheti, T.; Chongsa-Nguan, M. Detection with monoclonal antibody of Salmonella typhi antigen 9 in specimens from patients. J. Clin. Microbiol. 1988, 26, 1824–1830. [Google Scholar] [CrossRef]
- Appassakij, H.; Bunchuin, N.; Sarasombath, S.; Rungpitarangsi, B.; Manatsathit, S.; Komolpit, P.; Sukosol, T. Enzyme-linked immunosorbent assay for detection of Salmonella typhi protein antigen. J. Clin. Microbiol. 1987, 25, 273–277. [Google Scholar] [CrossRef]
- Khanam, F.; Sheikh, A.; Sayeed, A.; Bhuiyan, S.; Choudhury, F.K.; Salma, U.; Pervin, S.; Sultana, T.; Ahmed, D.; Goswami, D.; et al. Evaluation of a Typhoid/Paratyphoid Diagnostic Assay (TPTest) Detecting Anti-Salmonella IgA in Secretions of Peripheral Blood Lymphocytes in Patients in Dhaka, Bangladesh. PLoS Negl. Trop. Dis. 2013, 7, e2316. [Google Scholar] [CrossRef] [PubMed]
- Pastoor, R.; Hatta, M.; Abdoel, T.H.; Smits, H.L. Simple, rapid, and affordable point-of-care test for the serodiagnosis of typhoid fever. Diagn. Microbiol. Infect. Dis. 2008, 61, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Arora, P.; Thorlund, K.; Brenner, D.R.; Andrews, J.R. Comparative accuracy of typhoid diagnostic tools: A Bayesian latent-class network analysis. PLoS Negl. Trop. Dis. 2019, 13, e0007303. [Google Scholar] [CrossRef]
- Islam, K.; Sayeed, A.; Hossen, E.; Khanam, F.; Charles, R.C.; Andrews, J.; Ryan, E.T.; Qadri, F. Comparison of the Performance of the TPTest, Tubex, Typhidot and Widal Immunodiagnostic Assays and Blood Cultures in Detecting Patients with Typhoid Fever in Bangladesh, Including Using a Bayesian Latent Class Modeling Approach. PLoS Negl. Trop. Dis. 2016, 10, e0004558. [Google Scholar] [CrossRef]
- McClelland, M.; E Sanderson, K.; Clifton, S.W.; Latreille, P.; Porwollik, S.; Sabo, A.; Meyer, R.; Bieri, T.; Ozersky, P.; Harkins, C.R.; et al. Comparison of genome degradation in Paratyphi A and Typhi, human-restricted serovars of Salmonella enterica that cause typhoid. Nat. Genet. 2004, 36, 1268–1274. [Google Scholar] [CrossRef]
- Yamamoto, Y. PCR in Diagnosis of Infection: Detection of Bacteria in Cerebrospinal Fluids. Clin. Vaccine Immunol. 2002, 9, 508–514. [Google Scholar] [CrossRef]
- Lui, C.; Cady, N.C.; Batt, C.A. Nucleic Acid-based Detection of Bacterial Pathogens Using Integrated Microfluidic Platform Systems. Sensors 2009, 9, 3713–3744. [Google Scholar] [CrossRef]
- Schrader, C.; Schielke, A.; Ellerbroek, L.; Johne, R. PCR inhibitors—Occurrence, properties, and removal. J. Appl. Microbiol. 2012, 113, 1014–1026. [Google Scholar] [CrossRef] [PubMed]
- Abusalah, M.A.H.; Gan, S.H.; Al-Hatamleh, M.; Irekeola, A.A.; Shueb, R.H.; Yean, C.Y. Recent Advances in Diagnostic Approaches for Epstein–Barr Virus. Pathogens 2020, 9, 226. [Google Scholar] [CrossRef] [PubMed]
- Wages, J.M., Jr. Polymerase chain reaction. In Encyclopedia of Analytical Science, 2nd ed.; Worsfold, P., Townshend, A., Poole, C., Eds.; Elsevier: Amsterdam, The Netherlands, 2005; pp. 243–250. [Google Scholar]
- Espy, M.J.; Uhl, J.R.; Sloan, L.M.; Buckwalter, S.P.; Jones, M.F.; Vetter, E.A.; Yao, J.D.C.; Wengenack, N.L.; Rosenblatt, J.E.; Cockerill, F.R.; et al. Real-Time PCR in Clinical Microbiology: Applications for Routine Laboratory Testing. Clin. Microbiol. Rev. 2006, 19, 165–256. [Google Scholar] [CrossRef] [PubMed]
- Oscarsson, J.; Westermark, M.; Löfdahl, S.; Olsen, B.; Palmgren, H.; Mizunoe, Y.; Wai, S.N.; Uhlin, B.E. Characterization of a Pore-Forming Cytotoxin Expressed by Salmonella enterica Serovars Typhi and Paratyphi A. Infect. Immun. 2002, 70, 5759–5769. [Google Scholar] [CrossRef] [PubMed]
- Von Rhein, C.; Bauer, S.; Sanjurjo, E.J.L.; Benz, R.; Goebel, W.; Ludwig, A. ClyA cytolysin from Salmonella: Distribution within the genus, regulation of expression by SlyA, and pore-forming characteristics. Int. J. Med. Microbiol. 2009, 299, 21–35. [Google Scholar] [CrossRef]
- Ludwig, A.; von Rhein, C.; Bauer, S.; Huüttinger, C.; Goebel, W. Molecular Analysis of Cytolysin A (ClyA) in Pathogenic Escherichia coli Strains. J. Bacteriol. 2004, 186, 5311–5320. [Google Scholar] [CrossRef]
- Ali, A.; Haque, A.; Haque, A.; Sarwar, Y.; Mohsin, M.; Bashir, S.; Tariq, A. Multiplex PCR for differential diagnosis of emerging typhoidal pathogens directly from blood samples. Epidemiol. Infect. 2008, 137, 102–107. [Google Scholar] [CrossRef]
- Beauchamp, S.; D’Auria, S.; Pennacchio, A.; Lacroix, M. A new competitive fluorescence immunoassay for detection of Listeria monocytogenes. Anal. Methods 2012, 4, 4187. [Google Scholar] [CrossRef]
- Jain, S.; Chattopadhyay, S.; Jackeray, R.; Abid, C.Z.; Kohli, G.S.; Singh, H. Highly sensitive detection of Salmonella typhi using surface aminated polycarbonate membrane enhanced ELISA. Biosens. Bioelectron. 2012, 31, 37–43. [Google Scholar] [CrossRef]
- Ahmed, A.; Rushworth, J.V.; Hirst, N.A.; Millner, P.A. Biosensors for Whole-Cell Bacterial Detection. Clin. Microbiol. Rev. 2014, 27, 631–646. [Google Scholar] [CrossRef]
- Sharma, S.C. Surface Plasmon Resonance Sensors: Fundamental Concepts, Selected Techniques, Materials and Applications. In Advances in Sensors; Yurish, S., Ed.; IFSA Publishing: Barcelona, Spain, 2018; Volume 5, pp. 25–77. [Google Scholar]
- Nguyen, H.H.; Park, J.; Kang, S.; Kim, M. Surface Plasmon Resonance: A Versatile Technique for Biosensor Applications. Sensors 2015, 15, 10481–10510. [Google Scholar] [CrossRef] [PubMed]
- Kong, F.; Hu, F. Biomolecule immobilization techniques for bioactive paper fabrication. Anal. Bioanal. Chem. 2012, 403, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.; Zhang, B.; Skoumal, M.J.; Ramunno, B.; Li, X.; Wesdemiotis, C.; Liu, L.; Jia, L. Antifouling Poly(β-peptoid)s. Biomacromolecules 2011, 12, 2573–2582. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.W.; Sim, S.J.; Cho, S.M.; Lee, J. Characterization of a self-assembled monolayer of thiol on a gold surface and the fabrication of a biosensor chip based on surface plasmon resonance for detecting anti-GAD antibody. Biosens. Bioelectron. 2005, 20, 1422–1427. [Google Scholar] [CrossRef]
- Löfas, S.; Johnsson, B.; Edström, A.; Hansson, A.; Lindquist, G.; Hillgren, R.-M.M.; Stigh, L.; Lrofas, S. Methods for site-controlled coupling to carboxymethyldextran surfaces in surface plasmon resonance sensors. Biosens. Bioelectron. 1995, 10, 813–822. [Google Scholar] [CrossRef]
- Drescher, D.G.; Drescher, M.J.; Ramakrishnan, N.A. Surface Plasmon Resonance (SPR) Analysis of Binding Interactions of Proteins in Inner-Ear Sensory Epithelia. In Methods in Molecular Biology; Springer Science and Business Media LLC: Berlin/Heidelberg, Germany, 2009; Volume 493, pp. 323–343. [Google Scholar]
- Bergström, G.; Mandenius, C.-F. Orientation and capturing of antibody affinity ligands: Applications to surface plasmon resonance biochips. Sens. Actuators B Chem. 2011, 158, 265–270. [Google Scholar] [CrossRef]
- Wang, J.; Lv, R.; Xu, J.; Xu, D.; Chen, H. Characterizing the interaction between aptamers and human IgE by use of surface plasmon resonance. Anal. Bioanal. Chem. 2007, 390, 1059–1065. [Google Scholar] [CrossRef]
- Szunerits, S.; Rich, S.A.; Coffinier, Y.; Languille, M.-A.; Supiot, P.; Boukherroub, R. Preparation and characterization of thin organosilicon films deposited on SPR chip. Electrochim. Acta 2008, 53, 3910–3915. [Google Scholar] [CrossRef]
- Mahmoudpour, M.; Dolatabadi, J.E.N.; Torbati, M.; Homayouni-Rad, A. Nanomaterials based surface plasmon resonance signal enhancement for detection of environmental pollutions. Biosens. Bioelectron. 2019, 127, 72–84. [Google Scholar] [CrossRef]
- Wang, R. Immobilisation of DNA probes for the development of SPR-based sensing. Biosens. Bioelectron. 2004, 20, 967–974. [Google Scholar] [CrossRef]
- Singh, P. SPR Biosensors: Historical Perspectives and Current Challenges. Sens. Actuators B Chem. 2016, 229, 110–130. [Google Scholar] [CrossRef]
- Kim, N.-H.; Choi, M.; Kim, T.W.; Choi, W.; Park, S.Y.; Byun, K.M. Sensitivity and Stability Enhancement of Surface Plasmon Resonance Biosensors based on a Large-Area Ag/MoS2 Substrate. Sensors 2019, 19, 1894. [Google Scholar] [CrossRef] [PubMed]
- Byrne, B.; Stack, E.; Gilmartin, N.; O’Kennedy, R. Antibody-Based Sensors: Principles, Problems and Potential for Detection of Pathogens and Associated Toxins. Sensors 2009, 9, 4407–4445. [Google Scholar] [CrossRef] [PubMed]
- Liedberg, B.; Nylander, C.; Lunström, I. Surface plasmon resonance for gas detection and biosensing. Sens. Actuators 1983, 4, 299–304. [Google Scholar] [CrossRef]
- Fratamico, P.; Strobaugh, T.; Medina, M.; Gehring, A. Detection of Escherichia coli 0157:H7 using a surface plasmon resonance biosensor. Biotechnol. Tech. 1998, 12, 571–576. [Google Scholar] [CrossRef]
- Pattnaik, P. Surface Plasmon Resonance: Applications in Understanding Receptor–Ligand Interaction. Appl. Biochem. Biotechnol. 2005, 126, 79–92. [Google Scholar] [CrossRef]
- Homola, J.; Vaisocherová, H.; Dostálek, J.; Piliarik, M. Multi-analyte surface plasmon resonance biosensing. Methods 2005, 37, 26–36. [Google Scholar] [CrossRef]
- Singh, B.K.; Hillier, A.C. Surface Plasmon Resonance Imaging of Biomolecular Interactions on a Grating-Based Sensor Array. Anal. Chem. 2006, 78, 2009–2018. [Google Scholar] [CrossRef] [PubMed]
- Templier, V.; Roux, A.; Roupioz, Y.; Livache, T. Ligands for label-free detection of whole bacteria on biosensors: A review. TrAC Trends Anal. Chem. 2016, 79, 71–79. [Google Scholar] [CrossRef]
- Homola, J.; Hegnerová, K.; Vala, M. Surface plasmon resonance biosensors for detection of foodborne pathogens and toxins. Proceedings of Frontiers in Pathogen Detection: From Nanosensors to Systems, San Jose, CA, USA, 24–29 January 2009; SPIE Digital Library: San Jose, CA, USA, 2009; p. 716705. [Google Scholar]
- Mazumdar, S.D.; Barlen, B.; Kämpfer, P.; Keusgen, M. Surface plasmon resonance (SPR) as a rapid tool for serotyping of Salmonella. Biosens. Bioelectron. 2010, 25, 967–971. [Google Scholar] [CrossRef]
- Barlen, B.; Mazumdar, S.D.; Lezrich, O.; Kämpfer, P.; Keusgen, M. Detection of Salmonella by Surface Plasmon Resonance. Sensors 2007, 7, 1427–1446. [Google Scholar] [CrossRef]
- Perçin, I.; Idil, N.; Bakhshpour, M.; Yılmaz, E.; Mattiasson, B.; Denizli, A. Microcontact Imprinted Plasmonic Nanosensors: Powerful Tools in the Detection of Salmonella paratyphi. Sensors 2017, 17, 1375. [Google Scholar] [CrossRef] [PubMed]
- Oh, B.-K.; Lee, W.; Kim, Y.-K.; Lee, W.H.; Choi, J. Surface plasmon resonance immunosensor using self-assembled protein G for the detection of Salmonella paratyphi. J. Biotechnol. 2004, 111, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Fu, J.; Park, B.; Zhao, Y. Limitation of a localized surface plasmon resonance sensor for Salmonella detection. Sens. Actuators B Chem. 2009, 141, 276–283. [Google Scholar] [CrossRef]
- Aura, A.M. Surface Plasmon Resonamce Imaging Biosensors for the Detection of Pathogens and Toxins in Food; University of Catania: Catania, Italy, 2017. [Google Scholar]
- Arya, S.; Singh, A.; Naidoo, R.; Wu, P.; McDermott, M.; Evoy, S. Chemically immobilized T4-bacteriophage for specific Escherichia coli detection using surface plasmon resonance. Analyst 2011, 136, 486–492. [Google Scholar] [CrossRef]
- Bhandari, D.; Chen, F.-C.; Bridgman, R.C. Detection of Salmonella Typhimurium in Romaine Lettuce Using a Surface Plasmon Resonance Biosensor. Biosensors 2019, 9, 94. [Google Scholar] [CrossRef]
- Bhandari, D.; Chen, F.-C.; Hamal, S.; Bridgman, R.C. Kinetic Analysis and Epitope Mapping of Monoclonal Antibodies to Salmonella Typhimurium Flagellin Using a Surface Plasmon Resonance Biosensor. Antibodies 2019, 8, 22. [Google Scholar] [CrossRef]
- Barlen, B.; Mazumdar, S.D.; Keusgen, M. Immobilisation of biomolecules for biosensors. Phys. Status Solidi 2009, 206, 409–416. [Google Scholar] [CrossRef]
- Bokken, G.C.; Corbee, R.J.; van Knapen, F.; A Bergwerff, A. Immunochemical detection of Salmonella group B, D and E using an optical surface plasmon resonance biosensor. FEMS Microbiol. Lett. 2003, 222, 75–82. [Google Scholar] [CrossRef]
- Chen, J.; Park, B. Label-free screening of foodborne Salmonella using surface plasmon resonance imaging. Anal. Bioanal. Chem. 2017, 410, 5455–5464. [Google Scholar] [CrossRef]
- Eser, E.; Ekiz, O.Ö.; Çelik, H.; Sülek, S.; Dana, A.; Ekiz, H.İ. Rapid detection of foodborne pathogens by surface plasmon resonance biosensors. Int. J. Biosci. Biochem. Bioinform. 2015, 5, 329–335. [Google Scholar] [CrossRef]
- Jongerius-Gortemaker, B.G.M.; Goverde, R.; van Knapen, F.; A Bergwerff, A. Surface plasmon resonance (BIACORE) detection of serum antibodies against Salmonella enteritidis and Salmonella typhimurium. J. Immunol. Methods 2002, 266, 33–44. [Google Scholar] [CrossRef]
- Jyoung, J.-Y.; Hong, S.; Lee, W.; Choi, J. Immunosensor for the detection of Vibrio cholerae O1 using surface plasmon resonance. Biosens. Bioelectron. 2006, 21, 2315–2319. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.J.; Cho, H.S.; Park, N.Y.; Lee, J.I. Serodiagnostic Comparison Between Two Methods, ELISA, and Surface Plasmon Resonance for the Detection of Antibody Titres of Mycoplasma hyopneumoniae. J. Vet. Med. Ser. B 2006, 53, 87–90. [Google Scholar] [CrossRef] [PubMed]
- Koubová, V.; Brynda, E.; Karasová, L.; Škvor, J.; Homola, J.; Dostálek, J.; Tobiška, P.; Rosický, J. Detection of foodborne pathogens using surface plasmon resonance biosensors. Sens. Actuators B Chem. 2001, 74, 100–105. [Google Scholar] [CrossRef]
- Lan, Y.; Wang, S.-Z.; Yin, Y.-G.; Hoffmann, W.C.; Zheng, X. Using a Surface Plasmon Resonance Biosensor for Rapid Detection of Salmonella Typhimurium in Chicken Carcass. J. Bionic Eng. 2008, 5, 239–246. [Google Scholar] [CrossRef]
- Lukose, J.; Shetty, V.; Ballal, M.; Chidangil, S.; Sinha, R.K. Real-time and rapid detection of Salmonella Typhimurium using an inexpensive lab-built surface plasmon resonance setup. Laser Phys. Lett. 2018, 15, 075701. [Google Scholar] [CrossRef]
- Mazumdar, S.D.; Hartmann, M.; Kämpfer, P.; Keusgen, M. Rapid method for detection of Salmonella in milk by surface plasmon resonance (SPR). Biosens. Bioelectron. 2007, 22, 2040–2046. [Google Scholar] [CrossRef]
- Mazumdar, S.D.; Barlen, B.; Kramer, T.; Keusgen, M. A rapid serological assay for prediction of Salmonella infection status in slaughter pigs using surface plasmon resonance. J. Microbiol. Methods 2008, 75, 545–550. [Google Scholar] [CrossRef]
- Meeusen, C.A.; Alocilja, E.C.; Osburn, W.N. Detection of E. Coli O157:H7 Using a Miniaturized Surface Plasmon Resonance Biosensor. Trans. ASAE 2005, 48, 2409–2416. [Google Scholar] [CrossRef]
- Nguyen, H.H.; Yi, S.Y.; Woubit, A.; Kim, M. Portable Surface Plasmon Resonance Biosensor for Rapid Detection of Salmonella typhimurium. Appl. Sci. Converg. Technol. 2016, 25, 61–65. [Google Scholar] [CrossRef]
- Oh, B.-K.; Lee, W.; Chun, B.S.; Bae, Y.M.; Lee, W.H.; Choi, J. The fabrication of protein chip based on surface plasmon resonance for detection of pathogens. Biosens. Bioelectron. 2005, 20, 1847–1850. [Google Scholar] [CrossRef] [PubMed]
- Perkins, E. Development of instrumentation to allow the detection of microorganisms using light scattering in combination with surface plasmon resonance. Biosens. Bioelectron. 2000, 14, 853–859. [Google Scholar] [CrossRef]
- Si, S.-H.; Li, X.; Fung, Y.-S.; Zhu, D.-R. Rapid detection of Salmonella enteritidis by piezoelectric immunosensor. Microchem. J. 2001, 68, 21–27. [Google Scholar] [CrossRef]
- Singh, A.; Verma, H.N.; Arora, K. Surface Plasmon Resonance Based Label-Free Detection of Salmonella using DNA Self Assembly. Appl. Biochem. Biotechnol. 2014, 175, 1330–1343. [Google Scholar] [CrossRef]
- Subramanian, A.; Irudayaraj, J.; Ryan, T. A mixed self-assembled monolayer-based surface plasmon immunosensor for detection of E. coli O157:H7. Biosens. Bioelectron. 2006, 21, 998–1006. [Google Scholar] [CrossRef]
- Subramanian, A.S.; Irudayaraj, J.M. Surface plasmon resonance based immunosensing of E. coli O157:H7 in apple juice. Trans. ASABE 2006, 49, 1257–1262. [Google Scholar] [CrossRef]
- Subramanian, A.; Irudayaraj, J.; Ryan, T. Mono, and dithiol surfaces on surface plasmon resonance biosensors for detection of Staphylococcus aureus. Sens. Actuators B Chem. 2006, 114, 192–198. [Google Scholar] [CrossRef]
- Taheri, R.A.; Rezayan, A.H.; Rahimi, F.; Mohammadnejad, J.; Kamali, M. Development of an immunosensor using oriented immobilized anti-OmpW for sensitive detection of Vibrio cholerae by surface plasmon resonance. Biosens. Bioelectron. 2016, 86, 484–488. [Google Scholar] [CrossRef]
- Thomas, E.; Bouma, A.; van Eerden, E.; Landman, W.J.; van Knapen, F.; Stegeman, J.; A Bergwerff, A. Detection of egg yolk antibodies reflecting Salmonella enteritidis infections using a surface plasmon resonance biosensor. J. Immunol. Methods 2006, 315, 68–74. [Google Scholar] [CrossRef]
- Usachev, E.; Usacheva, O.; Agranovski, I. Surface plasmon resonance-based bacterial aerosol detection. J. Appl. Microbiol. 2014, 117, 1655–1662. [Google Scholar] [CrossRef] [PubMed]
- Waswa, J.; Debroy, C.; Irudayaraj, J. Rapid detection of Salmonella enteritidis and Escherichia coli using surface plasmon resonance biosensor. J. Food Process. Eng. 2006, 29, 373–385. [Google Scholar] [CrossRef]
- Waswa, J.; Irudayaraj, J.; Debroy, C. Direct detection of E. Coli O157:H7 in selected food systems by a surface plasmon resonance biosensor. LWT 2007, 40, 187–192. [Google Scholar] [CrossRef]
- Zhang, X.; Tsuji, S.; Kitaoka, H.; Kobayashi, H.; Tamai, M.; Honjoh, K.-I.; Miyamoto, T. Simultaneous Detection of Escherichia coli O157:H7, Salmonella enteritidis, and Listeria monocytogenes at a Very Low Level Using Simultaneous Enrichment Broth and Multichannel SPR Biosensor. J. Food Sci. 2017, 82, 2357–2363. [Google Scholar] [CrossRef] [PubMed]
- Park, H.-C.; Baig, I.; Lee, S.-C.; Moon, J.-Y.; Yoon, M.Y. Development of ssDNA Aptamers for the Sensitive Detection of Salmonella typhimurium and Salmonella enteritidis. Appl. Biochem. Biotechnol. 2014, 174, 793–802. [Google Scholar] [CrossRef]
- Lavín, Á.; de Vicente, J.; Holgado, M.; Laguna, M.F.; Casquel, R.; Santamaria, B.; Maigler, M.V.; Hernandez, A.L.; Ramirez, Y. On the Determination of Uncertainty and Limit of Detection in Label-Free Biosensors. Sensors 2018, 18, 2038. [Google Scholar] [CrossRef]
- Leuermann, J.; Fernandez-Gavela, A.; Torres-Cubillo, A.; Postigo, S.; Sánchez-Postigo, A.; Lechuga, L.M.; Halir, R.; Molina-Fernández, Í. Optimizing the Limit of Detection of Waveguide-Based Interferometric Biosensor Devices. Sensors 2019, 19, 3671. [Google Scholar] [CrossRef]
- Prabowo, B.A.; Purwidyantri, A.; Liu, K.-C. Surface Plasmon Resonance Optical Sensor: A Review on Light Source Technology. Biosensors 2018, 8, 80. [Google Scholar] [CrossRef]
- Yoo, S.M.; Lee, S.Y. Optical Biosensors for the Detection of Pathogenic Microorganisms. Trends Biotechnol. 2016, 34, 7–25. [Google Scholar] [CrossRef]
- Eser, E.; Ekiz, H.I. Antibody fragmentation technique for Salmonella detection by SPR based biosensor. J. Biotechnol. 2017, 256, S21. [Google Scholar] [CrossRef]
- Di, W.; Du, X.; Pan, M.; Wang, J. The SPR detection of Salmonella enteritidis in food using aptamers as recongnition elements. In Proceedings of the IOP Conference Series: Materials Science and Engineering, Singapore, 28–30 July 2017; IOP Publishing: Bristol, UK, 2017; Volume 231, p. 12114. [Google Scholar]
- Gopinath, S.C.; Yuan, Y.J.; Kumar, P.K.R. Regeneration of commercial Biacore chips to analyze biomolecular interactions. Opt. Eng. 2011, 50, 34402. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Antigen Name | Antigenic Virulence Factors | |||
|---|---|---|---|---|
| S. Paratyphi A | S. Paratyphi B | S. Paratyphi C | S. Typhi | |
| H flagellar | a, 1, 5 | b, 1, 2 | c, 1, 5 | d |
| O somatic | 1, 2, 12 | 1, 4, 5, 12 | 6, 7 | 9, 12 |
| Capsular antigen | - | - | Vi | Vi |
| Method | Advantage(s) | Disadvantage(s) | Reference(s) |
|---|---|---|---|
| Physical adsorption | For study of membrane-associated protein | The immobilized ligands are formed in random oriented order | [84,85] |
| Thiol-based | Covalent binding; thus, provides strong immobilization of ligand with thiol group and in homogenous orientation | Chemical synthesis and protein engineering need to be carried out if thiol group is lacking | [86,87] |
| Self-assembled monolayer based | Covalent binding; thus, provides strong immobilization of ligand with amine-coupling group and in homogenous orientation. This method is the simplest | Efficiency of immobilization can be decreased due to non-specific biding of ligand onto the surface | [88] |
| Capture | This method is used when the covalent immobilization process is not sufficient enough. Common techniques: streptavidin-biotin and antibody-antigen | Both analyte and ligand are removed during regeneration, so a new ligand is required, thus, increasing cost | [89,90] |
| Polymer film deposition | Provides high sensitivity | Weak binding to the sensor chip through non-covalent forces | [91,92] |
| Study ID [Reference] | Detected Bacteria | Sample | Principle of Immobilization | Limit of Detection |
|---|---|---|---|---|
| Arya 2011 [110] | Escherichia coli K12 | Bacterial culture | T4-based bioassay | 7 × 102 CFU/mL−1 |
| Aura 2017 [109] | Staphylococcal enterotoxin A, Staphylococcus aureus and Listeria monocytogenes | Milk | Ab/Ag immunoassay and PNA/SSO probes-based genoassay | 0.05 µg/mL |
| Bhandari 2019 [111] | S. Typhimurium | Romaine lettuce | Ab/Ag immunoassay | 0.9 log CFU/g |
| Bhandari 2019 [112] | S. Typhimurium | Bacterial culture | Ab/Ag immunoassay | - |
| Barlen 2007 [105] | S. Typhimurium and S. Enteritidis | Milk | Ab/Ag immunoassay | 2.50 × 105 cells/mL−1 |
| Barlen 2009 [113] | S. Enteritidis (antibodies) | Bacterial culture | Ab/Ag immunoassay | 1010 cells/mL−1 |
| Bokken 2003 [114] | Salmonella group B, D and E | Bacterial culture | Ab/Ag immunoassay | 107 CFU/mL−1 |
| Chen 2017 [115] | S. Enteritidis, S. Kentucky, S. Infantis, S. Javiana, S. Heidelberg and S. Typhimurium | Chicken carcass | Ab/Ag immunoassay | 2.1 × 106 CFU/mL |
| Eser 2015 [116] | S. Enteritidis | Bacterial culture | Ab/Ag immunoassay | 102 CFU/mL |
| Fratamico 1998 [98] | E. coli O157:H7 | Bacterial culture | Ab/Ag immunoassay | 107 CFU/mL |
| Fu 2009 [108] | S. Typhimurium | Bacterial culture | Ab/Ag immunoassay | 104 CFU/mL |
| Jongerius 2002 [117] | S. Enteritidis and S. Typhimurium (antibodies) | Serum from infected chickens | Ab/Ag immunoassay | - |
| Jyoung 2006 [118] | Vibrio cholerae O1 | Bacterial culture | Ab/Ag immunoassay | 105 cells/mL |
| Kim 2006 [119] | Mycoplasma hyopneumoniae (antibodies) | Serum from infected pigs | Ab/Ag immunoassay | - |
| Koubova 2001 [120] | S. Typhimurium and L. monocytogenes | Bacterial culture | Ab/Ag immunoassay | 106 cells/mL |
| Lan 2008 [121] | S. Typhimurium | Chicken carcass | Ab/Ag immunoassay | 106 CFU/mL |
| Lukose 2018 [122] | S. Typhimurium | Bacterial culture | Ab/Ag immunoassay | 106 CFU/mL−1 |
| Mazumdar 2007 [123] | S. Typhimurium | Milk | Ab/Ag immunoassay | 1.25 × 105 cells/mL−1 |
| Mazumdar 2008 [124] | S. Typhimurium (antibodies) | Serum from infected pigs | Ab/Ag immunoassay | 67.5 µg/mL−1 |
| Mazumdar 2010 [104] | Salmonella group B, C and D | Bacterial culture | Ab/Ag immunoassay | 1010 cells/mL−1 |
| Meeusen 2005 [125] | E. coli O157:H7 | Bacterial culture | Ab/Ag immunoassay | 8.7 × 106 CFU/mL |
| Nguyena 2016 [126] | S. Typhimurium | Bacterial culture | Ab/Ag immunoassay | 107 CFU/mL |
| Oh 2004 [107] | S. Paratyphi | Bacterial culture | Ab/Ag immunoassay | 102 CFU/mL |
| Oh 2005 [127] | E. coli O157:H7, S. Typhimurium, Legionella pneumophila and Yersinia enterocolitica | Bacterial culture | Ab/Ag immunoassay | 105 CFU/mL |
| Perçin 2017 [106] | S. Paratyphi | Bacterial culture | A special microcontact imprinted sensor chip programed to detect S. Paratyphi | 2.5 × 106 CFU/mL |
| Perkins 2000 [128] | Bacillus subtilis (spore) | Bacterial culture | Ab/Ag immunoassay | 107 mL−1 |
| Si 2001 [129] | S. Enteritidis | Bacterial culture | Ab/Ag immunoassay | 105 cells/mL |
| Singh 2014 [130] | S. Typhi | ssDNA extracted from bacterial culture | DNA self-assembly | 0.019 µg/mL−1 |
| Subramanian 2006 [131] | E. coli O157:H7 | Bacterial culture | Ab/Ag immunoassay | 104 CFU/mL |
| Subramanian 2006 [132] | E. coli O157:H7 | Apple juice | Ab/Ag immunoassay | 106 CFU/mL |
| Subramanian 2006 [133] | S. aureus | Bacterial culture | Ab/Ag immunoassay | 105 CFU/mL |
| Taheri 2016 [134] | V. cholerae O1 serovar Ogawa | Bacterial culture | Ab/Ag immunoassay | 43 cells/mL |
| Thomas 2006 [135] | S. Enteritidis (antibodies) | Eggs from chickens infected with Salmonella enteritidis | Ab/Ag immunoassay | - |
| Usachev 2014 [136] | E. coli K12 | Bacterial culture | Ab/Ag immunoassay | 1.5 × 103 CFU/mL−1 |
| Waswa 2006 [137] | S. Enteritidis, E. coli O26, K12, NM and H16 | Milk | Ab/Ag immunoassay | 23 CFU/mL |
| Waswa 2007 [138] | E. coli O157:H7 | Milk, apple juice and ground beef | Ab/Ag immunoassay | 102 CFU/mL |
| Zhang 2017 [139] | E. coli O157:H7, S. Enteritidis and L. monocytogenes | Bacterial culture | Ab/Ag immunoassay | 6 CFU/25 g |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alhaj-Qasem, D.M.; Al-Hatamleh, M.A.I.; Irekeola, A.A.; Khalid, M.F.; Mohamud, R.; Ismail, A.; Mustafa, F.H. Laboratory Diagnosis of Paratyphoid Fever: Opportunity of Surface Plasmon Resonance. Diagnostics 2020, 10, 438. https://doi.org/10.3390/diagnostics10070438
Alhaj-Qasem DM, Al-Hatamleh MAI, Irekeola AA, Khalid MF, Mohamud R, Ismail A, Mustafa FH. Laboratory Diagnosis of Paratyphoid Fever: Opportunity of Surface Plasmon Resonance. Diagnostics. 2020; 10(7):438. https://doi.org/10.3390/diagnostics10070438
Chicago/Turabian StyleAlhaj-Qasem, Dina M., Mohammad A. I. Al-Hatamleh, Ahmad Adebayo Irekeola, Muhammad Fazli Khalid, Rohimah Mohamud, Aziah Ismail, and Fatin Hamimi Mustafa. 2020. "Laboratory Diagnosis of Paratyphoid Fever: Opportunity of Surface Plasmon Resonance" Diagnostics 10, no. 7: 438. https://doi.org/10.3390/diagnostics10070438
APA StyleAlhaj-Qasem, D. M., Al-Hatamleh, M. A. I., Irekeola, A. A., Khalid, M. F., Mohamud, R., Ismail, A., & Mustafa, F. H. (2020). Laboratory Diagnosis of Paratyphoid Fever: Opportunity of Surface Plasmon Resonance. Diagnostics, 10(7), 438. https://doi.org/10.3390/diagnostics10070438