Cardiac Masses: The Role of Cardiovascular Imaging in the Differential Diagnosis

 ,
, 
Abstract
1. Introduction
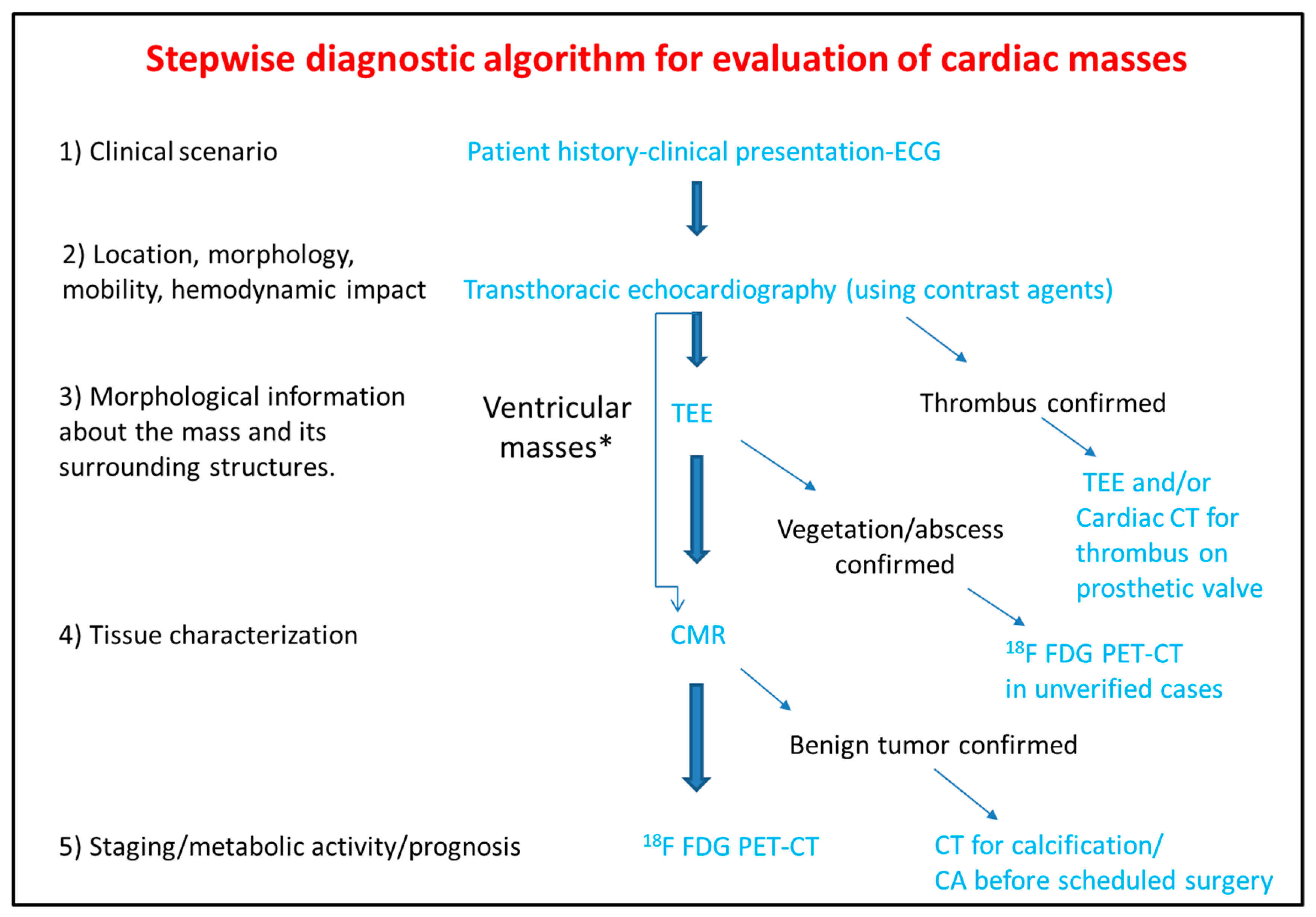
2. Diagnostic Approach of Patients Presenting with Cardiac Masses
3. Information Extracted by the Use of the Imaging Modalities
3.1. Transthoracic Echocardiography
3.2. Transesophageal Echocardiography
3.3. Computed Tomography
3.4. Cardiac Magnetic Resonance
- Tissue characterization on T1–T2 weighted images:
- Imaging characteristic of hemorrhagic pericardial effusion and clots depends on the age of the effusion.
- Contrast enhancement during the first pass T1 weighted imaging is indicative of increased vasculature.
- T1 hypo/isointensity with high T2 weighted signal intensity characterizes the majority of benign or malignant cardiac tumors
- Apical and hypertrophic cardiomyopathy may mimic cardiac tumors such as fibromas. In such cases fibromas appear hypointense in T2 weighted images while hypertrophic cardiomyopathy hyperintense. Moreover, CMR tagging can highlight the contractile nature of hypertrophic cardiomyopathy [53,54]. High T1 and low T2 weighted signal intensity is indicative of metastatic malignant melanoma.
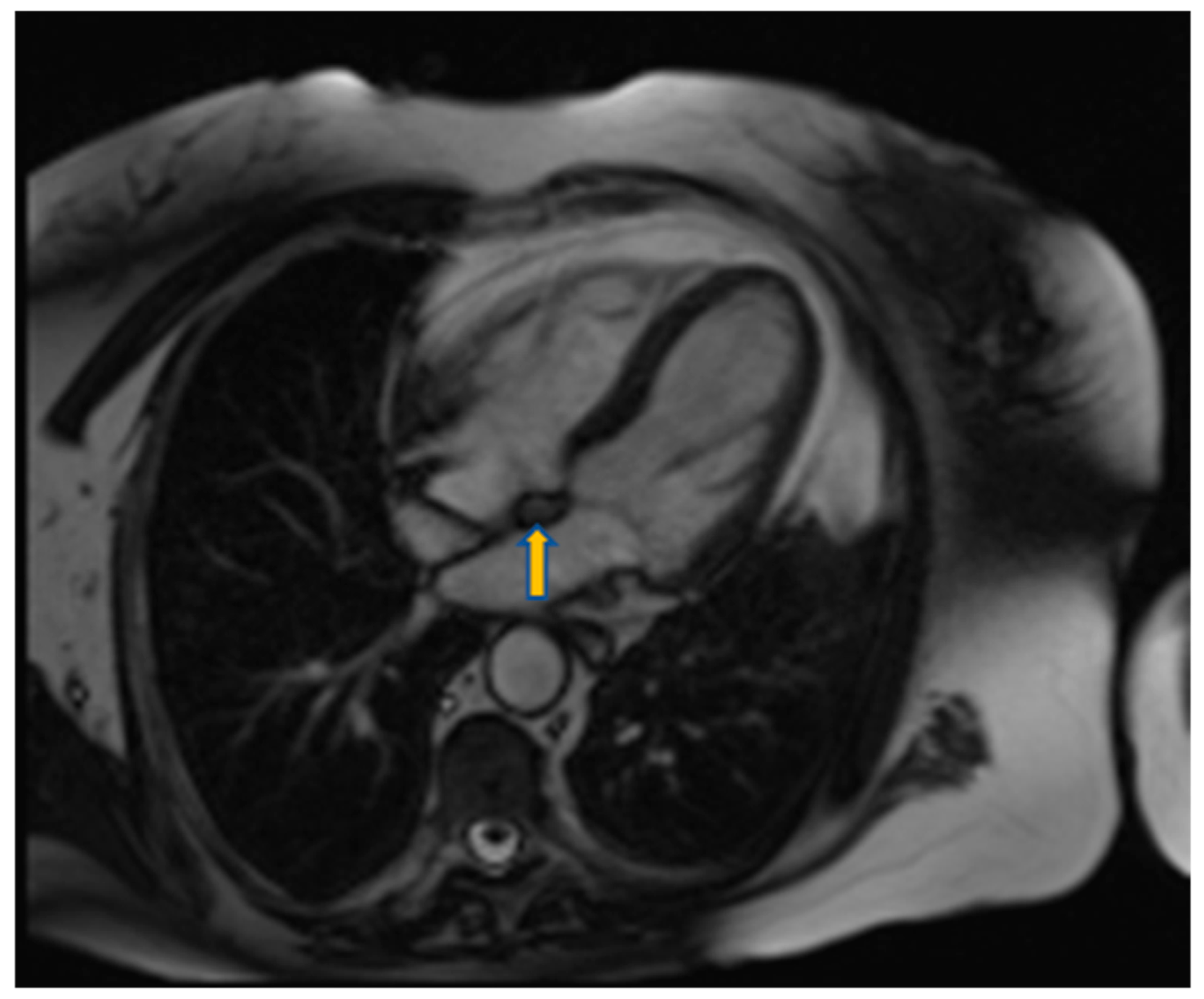
- High T1 signal intensity is also seen in lipomas. These masses and other lipomatoses can be recognized with fat suppression techniques (Figure 11).
- Early gadolinium enhancement (EGE) which identifies thrombus from the adjacent hypokinetic cardiac wall.
- Late gadolinium enhancement (LGE) that is ideal for fibrosis and necrosis identification.
3.5. Positron Emission Tomography
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
Ethical Approval
References
- Basso, C.; Rizzo, S.; Valente, M.; Thiene, G. Cardiac masses and tumours. Heart 2016, 102, 1230–1245. [Google Scholar] [CrossRef]
- Butany, J.; Nair, V.; Naseemuddin, A.; Nair, G.M.; Catton, C.; Yau, T. Cardiac tumours: Diagnosis and management. Lancet Oncol. 2005, 6, 219–228. [Google Scholar] [CrossRef]
- Capotosto, L.; Elena, G.; Massoni, F.; De Sio, S.; Carnevale, A.; Ricci, S.; Vitarelli, A. Cardiac tumors: Echocardiographic diagnosis and forensic correlations. Am. J. Forensic Med. Pathol. 2016, 37, 306–316. [Google Scholar] [CrossRef]
- Rahouma, M.; Arisha, M.J.; Elmously, A.; El-Sayed Ahmed, M.M.; Spadaccio, C.; Mehta, K.; Baudo, M.; Kamel, M.; Mansor, E.; Ruan, Y.; et al. Cardiac tumors prevalence and mortality: A systematic review and meta-analysis. Int. J. Surg. 2020, 76, 178–189. [Google Scholar] [CrossRef]
- Taguchi, S. Comprehensive review of the epidemiology and treatments for malignant adult cardiac tumors. Gen. Thorac. Cardiovasc. Surg. 2018, 66, 257–262. [Google Scholar] [CrossRef]
- Butany, J.; Leong, S.W.; Carmichael, K.; Komeda, M. A 30-year analysis of cardiac neoplasms at autopsy. Can. J. Cardiol. 2005, 21, 675–680. [Google Scholar]
- Lemasle, M.; Lavie Badie, Y.; Cariou, E.; Fournier, P.; Porterie, J.; Rousseau, H.; Petermann, A.; Hitzel, A.; Carrié, D.; Galinier, M.; et al. Contribution and performance of multimodal imaging in the diagnosis and management of cardiac masses. Int. J. Cardiovasc. Imaging 2020, 36, 971–981. [Google Scholar] [CrossRef]
- Anvari, M.S.; Naderan, M.; Babaki, A.E.S.; Shoar, S.; Boroumand, M.A.; Abbasi, K. Clinicopathologic review of non-myxoma cardiac tumors: A 10-year single-center experience. Cardiology 2014, 129, 199–202. [Google Scholar] [CrossRef]
- Wang, J.G.; Wang, B.; Hu, Y.; Liu, J.H.; Liu, B.; Liu, H.; Zhao, P.; Zhang, L.; Li, Y.J. Clinicopathologic features and outcomes of primary cardiac tumors: A 16-year-experience with 212 patients at a Chinese medical center. Cardiovasc. Pathol. 2018, 33, 45–54. [Google Scholar] [CrossRef]
- Basso, C.; Valente, M.; Poletti, A.; Casarotto, D.; Thiene, G. Surgical pathology of primary cardiac and pericardial tumors. Eur. J. Cardio-Thorac. Surg. 1997, 12, 730–738. [Google Scholar] [CrossRef]
- Grebenc, M.L.; Rosado De Christenson, M.L.; Burke, A.P.; Green, C.E.; Galvin, J.R. Primary cardiac and pericardial neoplasms: Radiologic-pathologic correlation. Radiographics 2000, 20, 1073–1103. [Google Scholar] [CrossRef] [PubMed]
- Abraham, K.P.; Reddy, V.; Gattuso, P. Neoplasms metastatic to the heart: Review of 3314 consecutive autopsies. Am. J. Cardiovasc. Pathol. 1990, 3, 195–198. [Google Scholar] [PubMed]
- Burazor, I.; Aviel-Ronen, S.; Imazio, M.; Goitein, O.; Perelman, M.; Shelestovich, N.; Radovanovic, N.; Kanjuh, V.; Barshack, I.; Adler, Y. Metastatic cardiac tumors: From clinical presentation through diagnosis to treatment. BMC Cancer 2018, 18, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Bussani, R.; De-Giorgio, F.; Abbate, A.; Silvestri, F. Cardiac metastases. J. Clin. Pathol. 2007, 60, 27–34. [Google Scholar] [CrossRef]
- Lee, E.; Mahani, M.G.; Lu, J.C.; Dorfman, A.L.; Srinivasan, A.; Agarwal, P.P. Primary cardiac tumors associated with genetic syndromes: A comprehensive review. Pediatr. Radiol. 2018, 48, 156–164. [Google Scholar] [CrossRef]
- Beghetti, M.; Gow, R.M.; Haney, I.; Mawson, J.; Williams, W.G.; Freedom, R.M. Pediatric primary benign cardiac tumors: A 15-year review. Am. Heart J. 1997, 134, 1107–1114. [Google Scholar]
- Shi, L.; Wu, L.; Fang, H.; Han, B.; Yang, J.; Ma, X.; Liu, F.; Zhang, Y.; Xiao, T.; Huang, M.; et al. Identification and clinical course of 166 pediatric cardiac tumors. Eur. J. Pediatr. 2017, 176, 253–260. [Google Scholar] [CrossRef]
- Paraskevaidis, I.A.; Michalakeas, C.A.; Papadopoulos, C.H.; Anastasiou-Nana, M. Cardiac Tumors. ISRN Oncol. 2011, 2011, 208929. [Google Scholar] [CrossRef]
- Burazor, I.; Aviel-Ronen, S.; Imazio, M.; Markel, G.; Grossman, Y.; Yosepovich, A.; Adler, Y. Primary malignancies of the heart and pericardium. Clin. Cardiol. 2014, 37, 582–588. [Google Scholar] [CrossRef]
- Yanagawa, B.; Chan, E.Y.; Cusimano, R.J.; Reardon, M.J. Approach to Surgery for Cardiac Tumors: Primary Simple, Primary Complex, and Secondary. Cardiol. Clin. 2019, 37, 525–531. [Google Scholar] [CrossRef]
- Yusuf, S.W.; Reardon, M.J.; Banchs, J. Cardiac tumors. Cardiology 2014, 129, 197–198. [Google Scholar] [CrossRef] [PubMed]
- Burke, A.; Tavora, F. The 2015 WHO Classification of tumors of the heart and pericardium. J. Thorac. Oncol. 2016, 11, 441–452. [Google Scholar] [CrossRef] [PubMed]
- Colin, G.C.; Gerber, B.L.; Amzulescu, M.; Bogaert, J. Cardiac myxoma: A contemporary multimodality imaging review. Int. J. Cardiovasc. Imaging 2018, 34, 1789–1808. [Google Scholar] [CrossRef] [PubMed]
- Neuville, A.; Collin, F.; Bruneval, P.; Parrens, M.; Thivolet, F.; Gomez-Brouchet, A.; Terrier, P.; De Montpreville, V.T.; Le Gall, F.; Hostein, I.; et al. Intimal sarcoma is the most frequent primary cardiac sarcoma: Clinicopathologic and molecular retrospective analysis of 100 primary cardiac sarcomas. Am. J. Surg. Pathol. 2014, 38, 461–469. [Google Scholar] [CrossRef]
- Tsugu, T.; Nagatomo, Y.; Endo, J.; Kawakami, T.; Murata, M.; Yamazaki, M.; Shimizu, H.; Fukuda, K.; Mitamura, H.; Lancellotti, P. Multiple papillary fibroelastomas attached to left ventricular side and aortic side of the aortic valve: A report of new case and literature review. Echocardiography 2019, 36, 1194–1199. [Google Scholar] [CrossRef]
- Yanagawa, B.; Mazine, A.; Chan, E.Y.; Barker, C.M.; Gritti, M.; Reul, R.M.; Ravi, V.; Ibarra, S.; Shapira, O.M.; Cusimano, R.J.; et al. Surgery for Tumors of the Heart. Semin. Thorac. Cardiovasc. Surg. 2018, 30, 385–397. [Google Scholar] [CrossRef]
- Castillo, J.G.; Silvay, G. Characterization and management of cardiac tumors. Semin. Cardiothorac. Vasc. Anesth. 2010, 14, 6–20. [Google Scholar] [CrossRef]
- Altbach, M.I.; Squire, S.W.; Kudithipudi, V.; Castellano, L.; Sorrell, V.L. Cardiac MRI is complementary to echocardiography in the assessment of cardiac masses. Echocardiography 2007, 24, 286–300. [Google Scholar] [CrossRef]
- Ragland, M.M.; Tak, T. The role of echocardiography in diagnosing space-occupying lesions of the heart. Clin. Med. Res. 2006, 4, 22–32. [Google Scholar] [CrossRef]
- Wang, X.; Li, Y.; Ren, W.; Yu, X.; Tan, X. Clinical diagnostic value of contrast-enhanced ultrasonography in the diagnosis of cardiac masses: A pilot study. Echocardiography 2020, 37, 231–238. [Google Scholar] [CrossRef]
- Palaskas, N.; Thompson, K.; Gladish, G.; Agha, A.M.; Hassan, S.; Iliescu, C.; Kim, P.; Durand, J.B.; Lopez-Mattei, J.C. Evaluation and Management of Cardiac Tumors. Curr. Treat. Options Cardiovasc. Med. 2018, 20, 29. [Google Scholar] [CrossRef] [PubMed]
- Strachinaru, M.; Damry, N.; Duttmann, R.; Wauthy, P.; Catez, E.; Lutea, M.; Costescu, I.; Morissens, M. Ultrasound Contrast Quantification for the Diagnosis of Intracardiac Masses. JACC Cardiovasc. Imaging 2016, 9, 747–750. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.M.; Bergquist, P.J.; Srichai, M.B. Multimodality Imaging in the Evaluation of Intracardiac Masses. Curr. Treat. Options Cardiovasc. Med. 2019, 21, 55. [Google Scholar] [CrossRef] [PubMed]
- Zaragosa-Macias, E.; Chen, M.A.; Gill, E.A. Real time three-dimensional echocardiography evaluation of intracardiac masses. Echocardiography 2012, 29, 207–219. [Google Scholar] [CrossRef] [PubMed]
- Aggeli, C.; Poulidakis, E.; Felekos, I.; Aggeli, A.; Stefanadis, C. An octopus-like myxoma depicted by real-time 3D transesophageal echocardiography. Hell. J. Cardiol. 2012, 53, 470–471. [Google Scholar]
- Li, X.; Chen, Y.; Liu, J.; Xu, L.; Li, Y.; Liu, D.; Sun, Z.; Wen, Z. Cardiac magnetic resonance imaging of primary cardiac tumors. Quant. Imaging Med. Surg. 2020, 10, 294–313. [Google Scholar] [CrossRef]
- Araoz, P.A.; Mulvagh, S.L.; Tazelaar, H.D.; Julsrud, P.R.; Breen, J.F. CT and MR imaging of benign primary cardiac neoplasms with echocardiographic correlation. Radiographics 2000, 20, 1303–1319. [Google Scholar] [CrossRef]
- Hoffmann, U.; Globits, S.; Schima, W.; Loewe, C.; Puig, S.; Oberhuber, G.; Frank, H. Usefulness of magnetic resonance imaging of cardiac and paracardiac masses. Am. J. Cardiol. 2003, 92, 890–895. [Google Scholar] [CrossRef]
- Auger, D.; Pressacco, J.; Marcotte, F.; Tremblay, A.; Dore, A.; Ducharme, A. Cardiac masses: An integrative approach using echocardiography and other imaging modalities. Heart 2011, 97, 1101–1109. [Google Scholar] [CrossRef]
- Kassop, D.; Donovan, M.S.; Cheezum, M.K.; Nguyen, B.T.; Gambill, N.B.; Blankstein, R.; Villines, T.C. Cardiac Masses on Cardiac CT: A Review. Curr. Cardiovasc. Imaging Rep. 2014, 7, 1–13. [Google Scholar] [CrossRef]
- Hong, Y.J.; Hur, J.; Kim, Y.J.; Lee, H.J.; Hong, S.R.; Suh, Y.J.; Kim, H.Y.; Lee, J.W.; Choi, B.W. Dual-energy cardiac computed tomography for differentiating cardiac myxoma from thrombus. Int. J. Cardiovasc. Imaging 2014, 30, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Liddy, S.; McQuade, C.; Walsh, K.P.; Loo, B.; Buckley, O. The Assessment of Cardiac Masses by Cardiac CT and CMR Including Pre-op 3D Reconstruction and Planning. Curr. Cardiol. Rep. 2019, 21, 103. [Google Scholar] [CrossRef] [PubMed]
- Nicol, E.D.; Norgaard, B.L.; Blanke, P.; Ahmadi, A.; Weir-McCall, J.; Horvat, P.M.; Han, K.; Bax, J.J.; Leipsic, J. The Future of Cardiovascular Computed Tomography: Advanced Analytics and Clinical Insights. JACC Cardiovasc. Imaging 2019, 12, 1058–1072. [Google Scholar] [CrossRef] [PubMed]
- Pazos-López, P.; Pozo, E.; Siqueira, M.E.; García-Lunar, I.; Cham, M.; Jacobi, A.; Macaluso, F.; Fuster, V.; Narula, J.; Sanz, J. Value of CMR for the differential diagnosis of cardiac masses. JACC Cardiovasc. Imaging 2014, 7, 896–905. [Google Scholar] [CrossRef]
- Luna, A.; Ribes, R.; Caro, P.; Vida, J.; Erasmus, J.J. Evaluation of cardiac tumors with magnetic resonance imaging. Eur. Radiol. 2005, 15, 1446–1455. [Google Scholar] [CrossRef]
- Giusca, S.; Mereles, D.; Ochs, A.; Buss, S.; André, F.; Seitz, S.; Riffel, J.; Fortner, P.; Andrulis, M.; Schönland, S.; et al. Incremental value of cardiac magnetic resonance for the evaluation of cardiac tumors in adults: Experience of a high volume tertiary cardiology centre. Int. J. Cardiovasc. Imaging 2017, 33, 879–888. [Google Scholar] [CrossRef]
- Mousavi, N.; Cheezum, M.K.; Aghayev, A.; Padera, R.; Vita, T.; Steigner, M.; Hulten, E.; Bittencourt, M.S.; Dorbala, S.; Di Carli, M.F.; et al. Assessment of Cardiac Masses by Cardiac Magnetic Resonance Imaging: Histological Correlation and Clinical Outcomes. J. Am. Heart Assoc. 2019, 8, e007829. [Google Scholar] [CrossRef]
- Tumma, R.; Dong, W.; Wang, J.; Litt, H.; Han, Y. Evaluation of cardiac masses by CMR—Strengths and pitfalls: A tertiary center experience. Int. J. Cardiovasc. Imaging 2016, 32, 913–920. [Google Scholar] [CrossRef]
- O’Donnell, D.H.; Abbara, S.; Chaithiraphan, V.; Yared, K.; Killeen, R.P.; Cury, R.C.; Dodd, J.D. Cardiac tumors: Optimal cardiac MR sequences and spectrum of imaging appearances. Am. J. Roentgenol. 2009, 193, 377–387. [Google Scholar] [CrossRef]
- Tzani, A.; Doulamis, I.P.; Mylonas, K.S.; Avgerinos, D.V.; Nasioudis, D. Cardiac Tumors in Pediatric Patients: A Systematic Review. World J. Pediatr. Congenit. Heart Surg. 2017, 8, 624–632. [Google Scholar] [CrossRef]
- Beroukhim, R.S.; Prakash, A.; Valsangiacomo Buechel, E.R.; Cava, J.R.; Dorfman, A.L.; Festa, P.; Hlavacek, A.M.; Johnson, T.R.; Keller, M.S.; Krishnamurthy, R.; et al. Characterization of cardiac tumors in children by cardiovascular magnetic resonance imaging: A multicenter experience. J. Am. Coll. Cardiol. 2011, 58, 1044–1054. [Google Scholar] [CrossRef] [PubMed]
- Fournier, E.; Séguéla, P.-E.; Sauvestre, F.; Jalal, Z.; Thomas, J.; Iriart, X.; Bonello, B.; Thambo, J.-B. Imaging Aspects of Pediatric Cardiac Tumors. J. Am. Coll. Cardiol. Cardiovasc. Imaging 2020, 13, 2245–2253. [Google Scholar] [CrossRef] [PubMed]
- Nucifora, G.; Pasotti, E.; Pedrazzini, G.; Moccetti, T.; Faletra, F.F.; Gallino, A. Cardiac fibroma mimicking hypertrophic cardiomyopathy: Role of magnetic resonance imaging in the differential diagnosis. Int. J. Cardiol. 2012, 154, e11–e13. [Google Scholar] [CrossRef] [PubMed]
- Noureldin, R.A.; Liu, S.; Nacif, M.S.; Judge, D.P.; Halushka, M.K.; Abraham, T.P.; Ho, C.; Bluemke, D.A. The diagnosis of hypertrophic cardiomyopathy by cardiovascular magnetic resonance. J. Cardiovasc. Magn. Reson. 2012, 14, 17. [Google Scholar] [CrossRef]
- Meng, J.; Zhao, H.; Liu, Y.; Chen, D.; Hacker, M.; Wei, Y.; Li, X.; Zhang, X.; Kreissl, M.C. Assessment of cardiac tumors by 18F-FDG PET/CT imaging: Histological correlation and clinical outcomes. J. Nucl. Cardiol. 2020. [Google Scholar] [CrossRef]
- Chalian, H.; O’Donnell, J.K.; Bolen, M.; Rajiah, P. Incremental value of PET and MRI in the evaluation of cardiovascular abnormalities. Insights Imaging 2016, 7, 485–503. [Google Scholar] [CrossRef]
- Fathala, A.; Abouzied, M.; AlSugair, A.-A. Cardiac and pericardial tumors: A potential application of positron emission tomography-magnetic resonance imaging. World J. Cardiol. 2017, 9, 600. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Common Age at Presentation | Common Location at Heart | Clinical Manifestations | Echocardiography | CT | CMR | |
|---|---|---|---|---|---|---|
| Benign primary heart tumors | ||||||
| Myxoma | Early (familial) or middle adulthood | LA, atrial septum, any other site | Emboli, flow obstruction, systemic symptoms | Mildly lobar, heterogeneous echodensity, usually mobile (with or without stalk) | Heterogeneous, low attenuation, may be calcified | Isointense T1w, High T2w, heterogeneous LGE |
| Papillary fibroelastoma | Middle or late adulthood | Cardiac valves | Usually asymptomatic, emboli | Circular, pedunculated, non-protruding, usually not causing valve dysfunction | Smooth, pedunculated | Iso/hypointense T1w, high T2w, LGE, highly mobile, consider TEE |
| Lipoma | Adulthood | Left ventricle, any other site | Usually asymptomatic, arrhythmias, flow obstruction | Homogeneous | Smooth, homogenous encapsulated, fat attenuation, no enhancement with contrast | High T1w, T2w, no LGE, suppressed with SPIR |
| Rhabdomyoma | Infancy or early childhood | Ventricles, atrioventricular valves | Usually asymptomatic, flow obstruction, heart failure, arrhythmias | Homogenous, slightly echogenic, can be multiple | Attenuation similar to myocardium, intramural | Isointense T1w, iso/hyperintense T2w, no LGE |
| Fibroma | Early childhood | Intraventricular septum, ventricles | Usually asymptomatic, arrhythmias | Heterogeneous, echogenic, non-contractible, can mimic HCM | Soft tissue attenuation, low contrast enhancement, may be calcified | Isointense T1w, Low T2w, high LGE |
| Hemangioma | Any age | Any other site | Usually asymptomatic, dyspnoea | Highly echogenic with contrast infusion, may resemble a cavity | Heterogeneous, high contrast enhancement, may be calcified | Heterogeneous, high T1w, Very high T2w, centripetal progression on first pass, heterogeneous LGE, |
| Malignant primary heart tumors | ||||||
| Angiosarcoma | Early and middle adulthood | RA, pericardium | Constitutional symptoms, heart failure, pericardial effusion | Heterogeneous, highly echogenic with contrast infusion | Heterogeneous, irregular, low attenuation | Heterogeneous T1w, T2w LGE, early enhancement at first pass |
| Rhabomyosarcoma | Childhood, early adulthood | Ventricles, any other site | Heart failure | Normal-high echodensity | Irregular, low attenuation | Isointense T1w, high T2w, usually homogenous LGE |
| UPS/Myxofibrosarcoma | Early and middle adulthood | Left atrium, any other site | Flow obstruction/heart failure, pericardial effusion, metastatic | Heterogeneous, normal-high echodensity | Heterogeneous, low attenuation | Heterogeneous T1w, T2w LGE |
| Lymphoma | Adulthood | RA, any other site | Pericardial effusion, flow obstruction/heart failure | Any size and shape | Normal to low attenuation, heterogeneous contrast enhacncement | Isointentse T1w, T2w, minimal LGE |
| Mesothelioma | Adulthood | Pericardium | Pericardial effusion | Heterogeneous | Variable characteristics | Isointense T1w, Heterogeneous T2w, high LGE |
| Metastatic tumors | ||||||
| Melanoma | Adulthood | Any site | Flow obstruction/heart failure, pericardial effusion | Heterogeneous, highly echogenic with contrast infusion | Similar to soft tissue, hard to recognize | High T1w, low T2w heterogeneous LGE |
| Other metastatic tumors | Adulthood | Pericardium, any site | Flow obstruction/heart failure, pericardial effusion | Heterogeneous, highly echogenic with contrast infusion | Solid, similar to soft tissue attenuation, moderate to high contrast enhancement | Low T1w, high T2w, heterogeneous LGE |
| Non-neoplasmatic heart masses | ||||||
| Clots | Adulthood | LAA, LV apex | Emboli | Acute: Low echodensity Chronic: High echodensity No perfusion with contrast agents | No contrast enhancement, may be calcified | No EGE/LGE Acute: Isointense to high T1w, T2w Subacute: High T1w, Low T2w Chronic: Low T1w, T2w |
| Vegetation | Adulthood | Cardiac valves | Valve dysfunction, emboli, heart failure | Highly mobile, oscillating protruding, valve dysfunction, | Low attenuation, may recognize, perivalvular extension, fistulas, abscess | Highly mobile, consider TEE |
| Non-neoplasmatic calcified masses | Adulthood | Usually posterior mitral annulus | Usually asymptomatic | Very high echodensity | Heterogeneous, calcified | Signal loss, consider CT |
| Pericardial cysts | Adulthood | Pericardium | Usually asymptomatic, external compression | Low echodensity, typically no perfusion with contrast agents | Presence of wall, fluid attenuation | Depends on the fluid, usually isointense T1w, high T2w, no LGE |
| Lipomatous Hypertrophy | Late adulthood | Atrial septum | Usually asymptomatic, arrhythmias | Homogeneous dumbbell appearance of atrial septum | Fat attenuation | High T1w, T2w, no LGE, suppressed with SPIR |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aggeli, C.; Dimitroglou, Y.; Raftopoulos, L.; Sarri, G.; Mavrogeni, S.; Wong, J.; Tsiamis, E.; Tsioufis, C. Cardiac Masses: The Role of Cardiovascular Imaging in the Differential Diagnosis. Diagnostics 2020, 10, 1088. https://doi.org/10.3390/diagnostics10121088
Aggeli C, Dimitroglou Y, Raftopoulos L, Sarri G, Mavrogeni S, Wong J, Tsiamis E, Tsioufis C. Cardiac Masses: The Role of Cardiovascular Imaging in the Differential Diagnosis. Diagnostics. 2020; 10(12):1088. https://doi.org/10.3390/diagnostics10121088
Chicago/Turabian StyleAggeli, Constantina, Yannis Dimitroglou, Leonidas Raftopoulos, Georgia Sarri, Sophie Mavrogeni, Joyce Wong, Eleftherios Tsiamis, and Costas Tsioufis. 2020. "Cardiac Masses: The Role of Cardiovascular Imaging in the Differential Diagnosis" Diagnostics 10, no. 12: 1088. https://doi.org/10.3390/diagnostics10121088
APA StyleAggeli, C., Dimitroglou, Y., Raftopoulos, L., Sarri, G., Mavrogeni, S., Wong, J., Tsiamis, E., & Tsioufis, C. (2020). Cardiac Masses: The Role of Cardiovascular Imaging in the Differential Diagnosis. Diagnostics, 10(12), 1088. https://doi.org/10.3390/diagnostics10121088