Early Detection of Coronary Artery Disease by Micro-RNA Analysis in Asymptomatic Patients Stratified by Coronary CT Angiography


 , and
, and
Abstract
1. Introduction
2. Methods
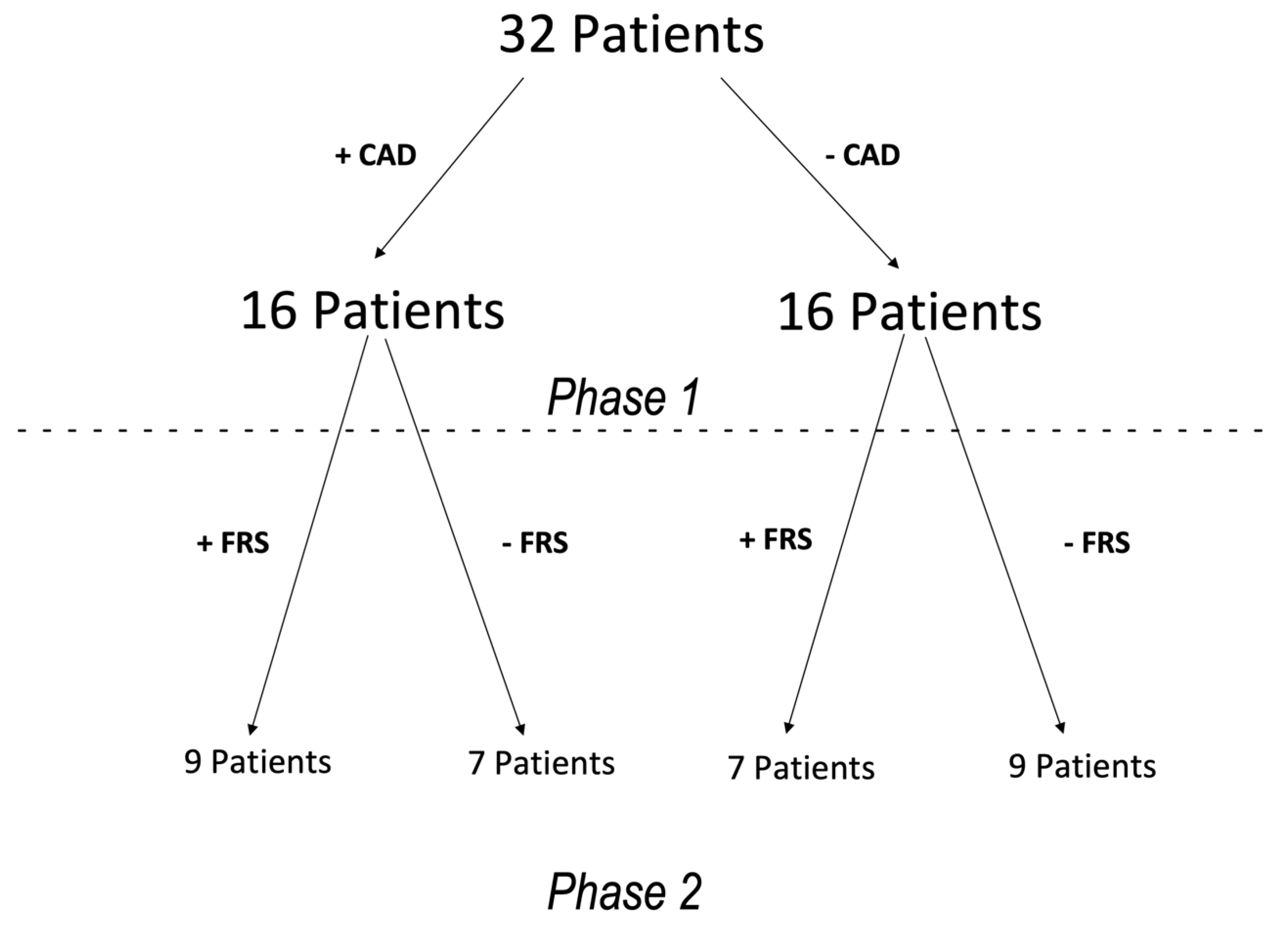
2.1. Patient Population
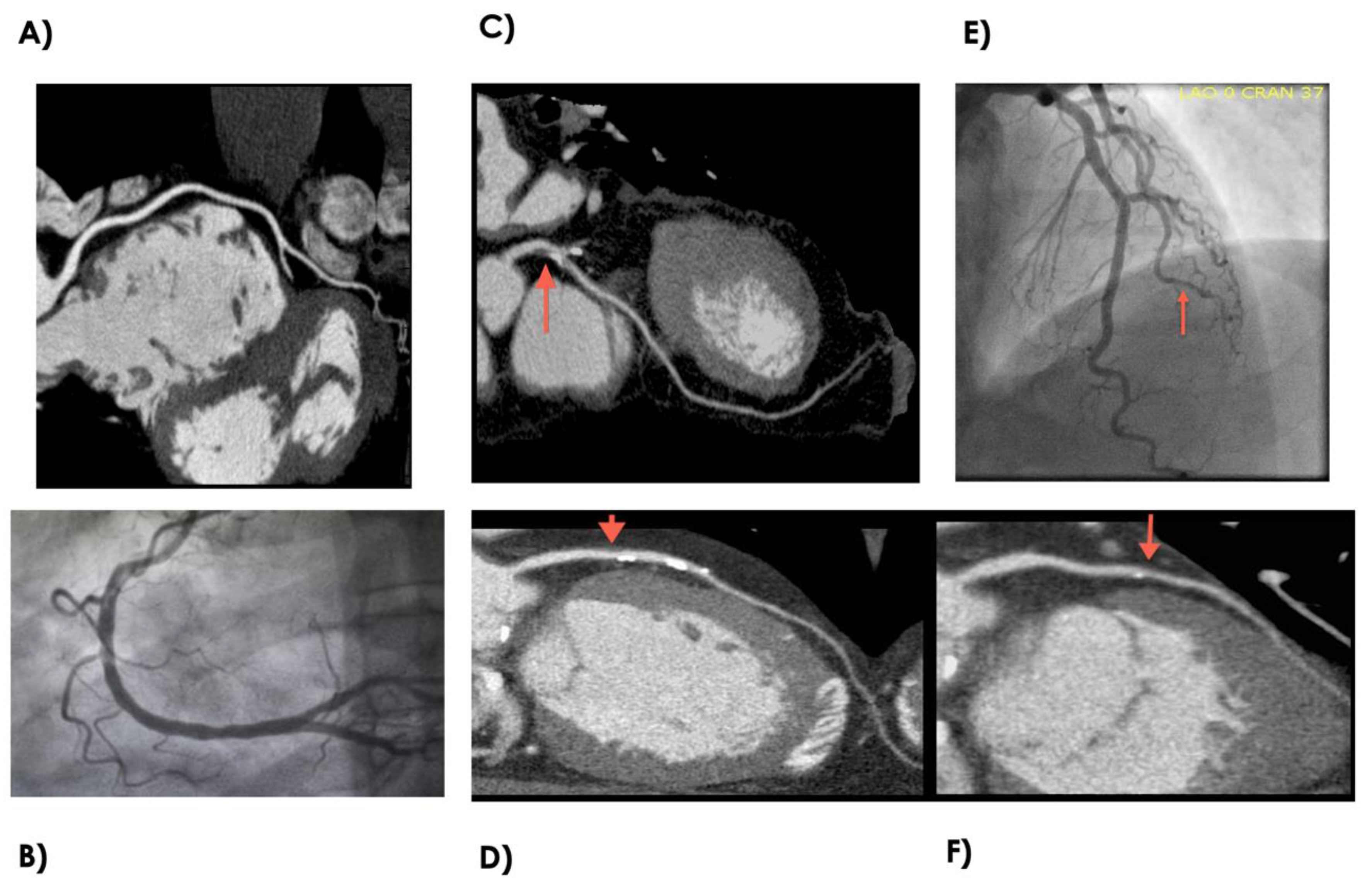
2.2. Coronary CTA
2.3. MiRNA Isolation and Purification
2.4. MiRNA Microarray
2.5. Statistical Analyses
3. Results
3.1. Study Population Characteristics
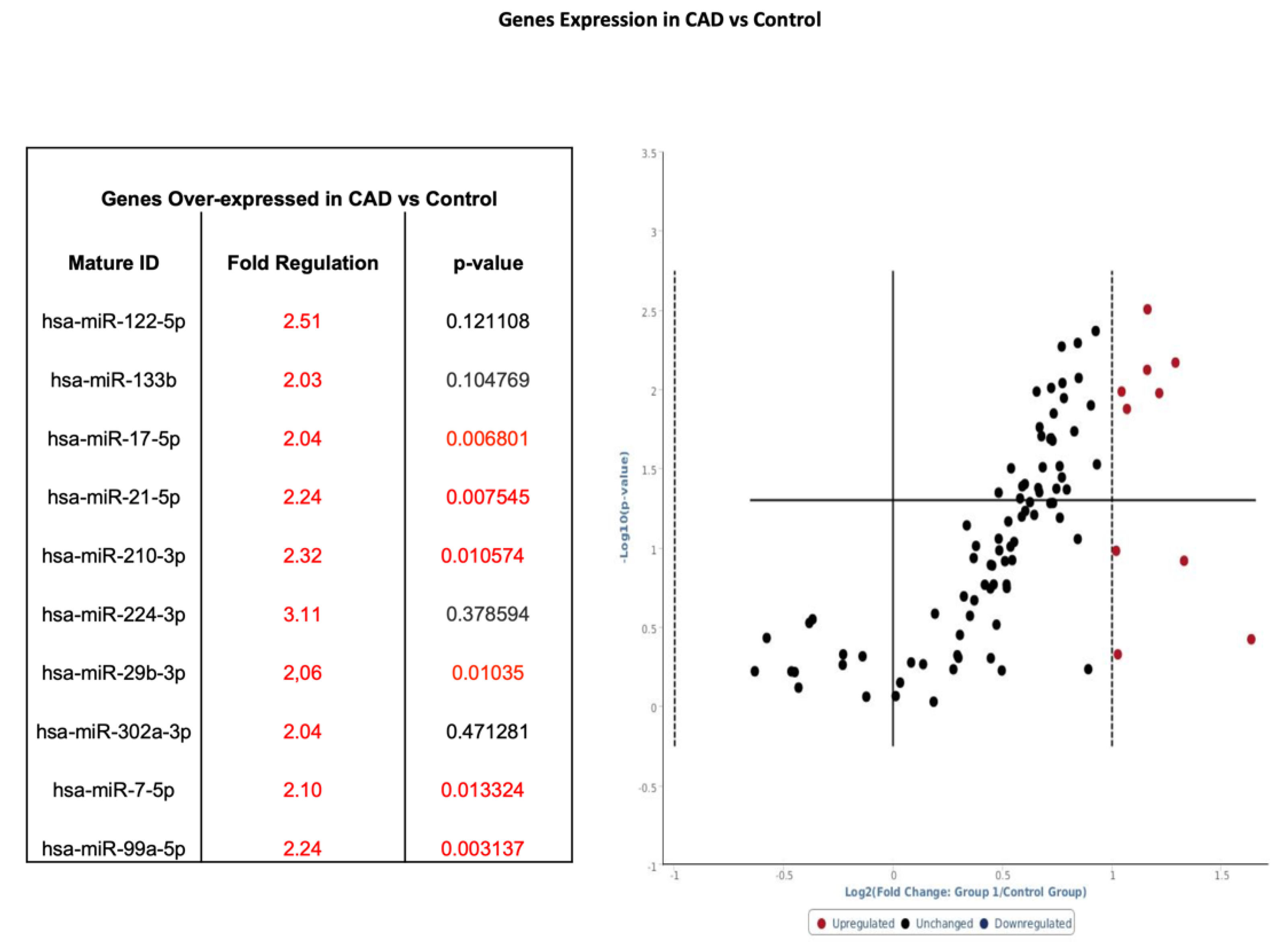
3.2. miRNA Profile in Subjects with CAD Versus Healthy Controls
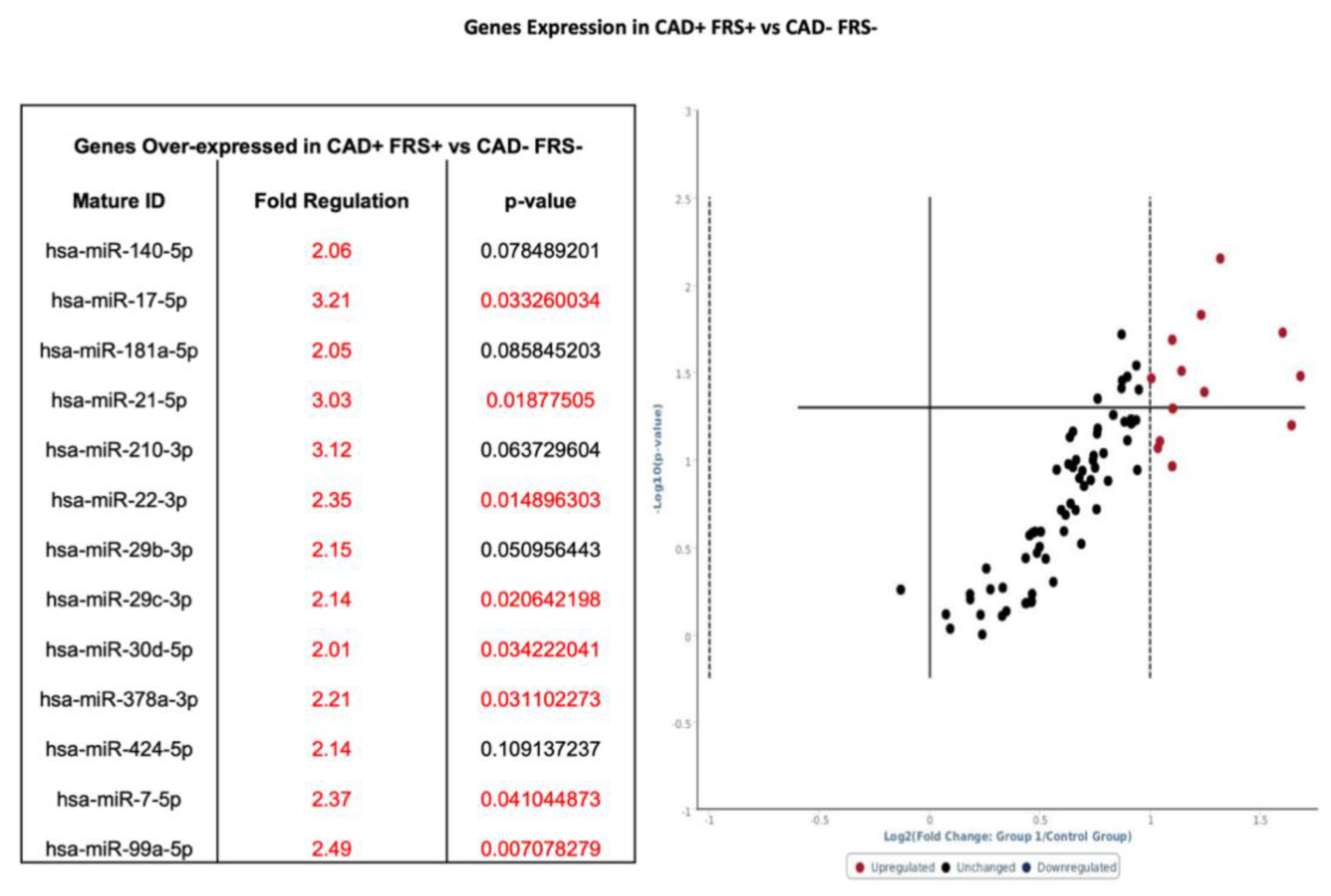
3.3. Group 1: miRNA Profile in Subjects with CAD and High FRS
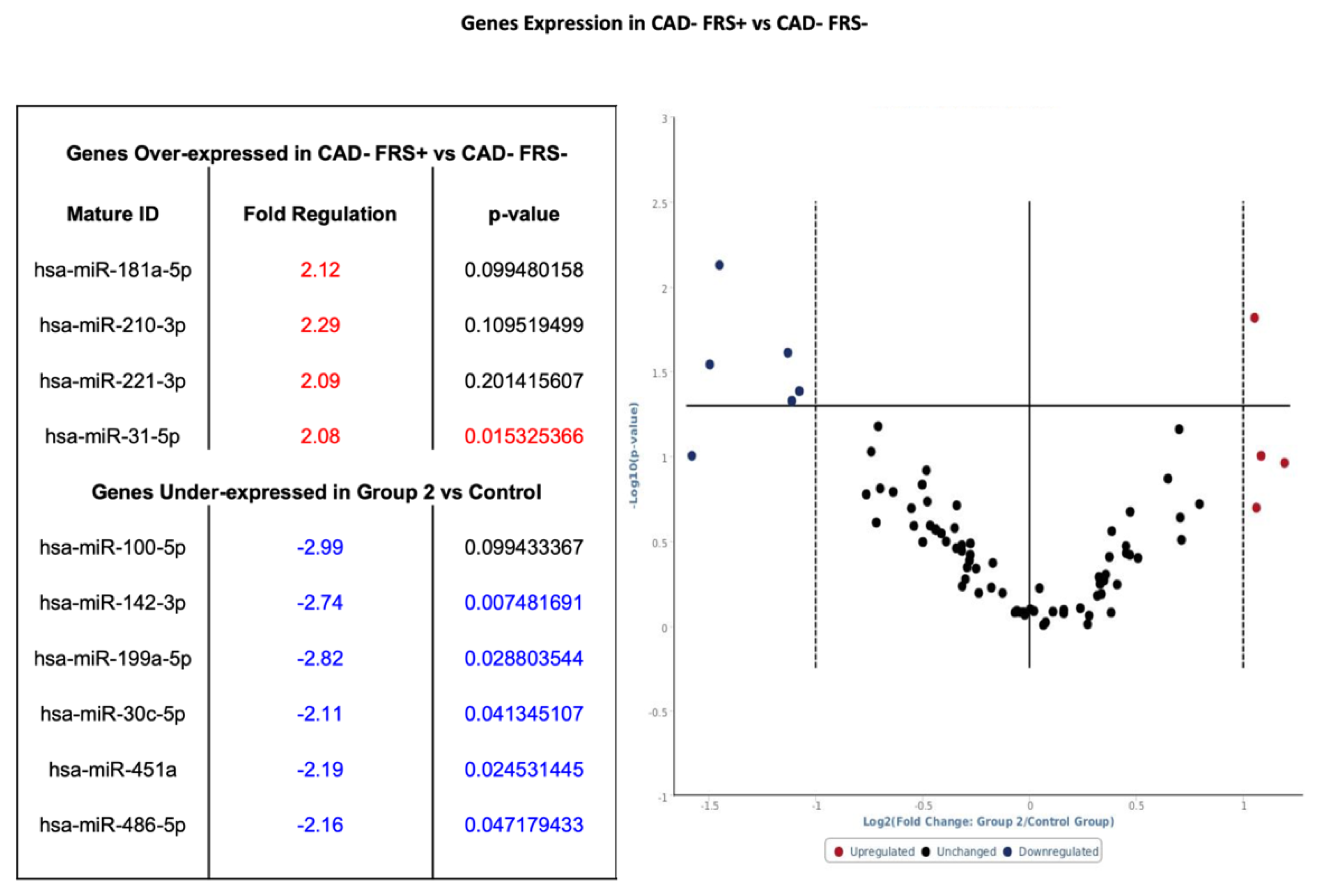
3.4. Group 2: miRNA Profile in Subjects without CAD and High FRS
3.5. Group 3: miRNA Profile in Subjects with CAD and Low FRS
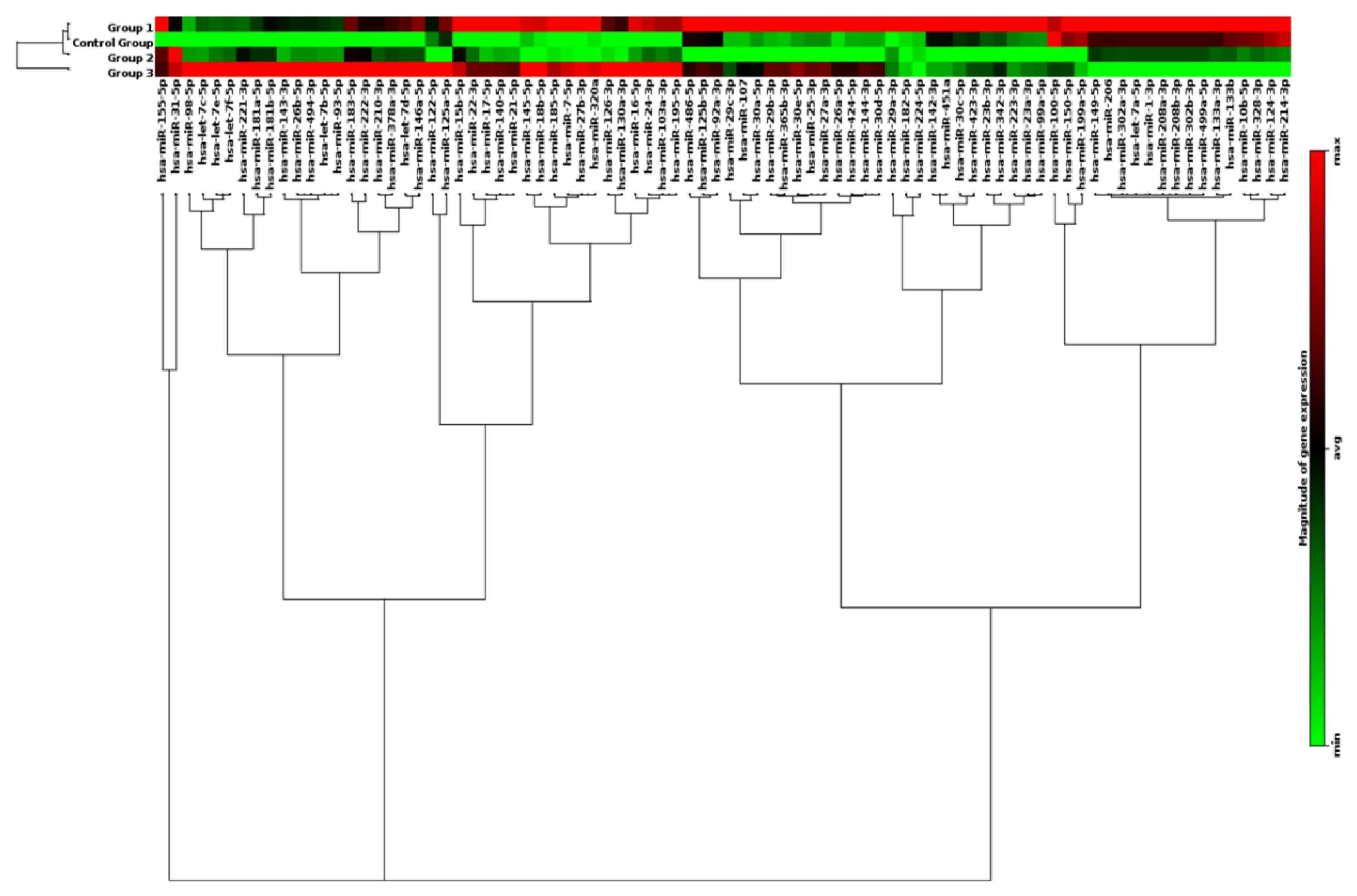
3.6. Clustergram of miRNA Profiles in Subdivided Groups
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Roger, V.L.; Go, A.S.; Lloyd-Jones, D.M.; Benjamin, E.J.; Berry, J.D.; Borden, W.B.; Bravata, D.M.; Dai, S.; Ford, E.S.; Fox, C.S.; et al. Heart Disease and Stroke Statistics-2012 Update. A Report from the American Heart Association. Circulation 2012, 125, e2. [Google Scholar]
- Celermajer, D.S.; Chow, C.K.; Marijon, E.; Anstey, N.M.; Woo, K.S. Cardiovascular Disease in the Developing World. Prevalences, Patterns, and the Potential of Early Disease Detection. J. Am. Coll. Cardiol. 2012, 60, 1207–1216. [Google Scholar] [CrossRef]
- Faxon, D.P.; Fuster, V.; Libby, P.; Beckman, J.A.; Hiatt, W.R.; Thompson, R.W.; Topper, J.N.; Annex, B.H.; Rundback, J.H.; Fabunmi, R.P.; et al. Atherosclerotic Vascular Disease Conference. Writing Group III: Pathophysiology. Circulation 2004, 109, 2617–2625. [Google Scholar] [CrossRef] [PubMed]
- Fihn, S.D.; Gardin, J.M.; Abrams, J.; Berra, K.; Blankenship, J.C.; Dallas, A.P.; Douglas, P.S.; Foody, J.M.; Gerber, T.C.; Hinderliter, A.L.; et al. 2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS Guideline for the Diagnosis and Management of Patients with Stable Ischemic Heart Disease. J. Am. Coll. Cardiol. 2012, 60, e44–e164. [Google Scholar] [CrossRef]
- Gibbons, R.J. ACC/AHA 2002 Guideline Update for Exercise Testing: Summary Article: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Update the 1997 Exercise Testing Guidelines). Circulation 2002, 106, 1883–1892. [Google Scholar]
- D’Agostino, R.B., Sr.; Vasan, R.S.; Pencina, M.J.; Wolf, P.A.; Cobain, M.; Massaro, J.M.; Kannel, W.B. General Cardiovascular Risk Profile for Use in Primary Care. The Framingham Heart Study. Circulation 2008, 117, 743–753. [Google Scholar] [CrossRef] [PubMed]
- Vasan, R.S.; Sullivan, L.M.; Wilson, P.W.; Sempos, C.T.; Sundström, J.; Kannel, W.B.; Levy, D.; D’agostino, R.B. Relative importance of borderline and elevated levels of coronary heart disease risk factors. Ann. Intern. Med. 2005, 142, 393–402. [Google Scholar] [CrossRef]
- Ahmadi, N.; Hajsadeghi, F.; Blumenthal, R.S.; Budoff, M.J.; Stone, G.W.; Ebrahimi, R. Mortality in Individuals Without Known Coronary Artery Disease but With Discordance Between the Framingham Risk Score and Coronary Artery Calcium. Am. J. Cardiol. 2011, 107, 799–804. [Google Scholar] [CrossRef]
- Brindle, P.; Jonathan, E.; Lampe, F.; Walker, M.; Whincup, P.; Fahey, T.; Ebrahim, S. Predictive accuracy of the Framingham coronary risk score in British men: Prospective cohort study. BMJ 2003, 327, 1267. [Google Scholar] [CrossRef]
- Pasquinelli, A.E. MicroRNAs and their targets: Recognition, regulation and an emerging reciprocal relationship. Nat. Rev. Genet. 2012, 3, 71–82. [Google Scholar] [CrossRef] [PubMed]
- Bartel, D.P. MicroRNAs: Genomics, biogenesis, mechanism, and function. Cell 2004, 116, 281–297. [Google Scholar] [CrossRef]
- Van Aelst, L.N.; Heymans, S. MicroRNAs as biomarkers for ischemic heart disease. J. Cardiovasc. Transl. Res. 2013, 6, 458–470. [Google Scholar] [CrossRef]
- Divakaran, V.; Mann, D.L. The Emerging Role of MicroRNAs in Cardiac Remodeling and Heart Failure. Circ. Res. 2008, 103, 1072–1083. [Google Scholar] [CrossRef]
- Fichtlscherer, S.; De Rosa, S.; Fox, H.; Schwietz, T.; Fischer, A.; Liebetrau, C.; Weber, M.; Hamm, C.W.; Röxe, T.; Müller-Ardogan, M.; et al. Circulating microRNAs in patients with coronary artery disease. Circ. Res. 2010, 107, 677–684. [Google Scholar] [CrossRef]
- Papageorgiou, N.; Tousoulis, D.; Charakida, M.; Briasoulis, A.; Androulakis, E.; Tentolouris, C.; Siasos, G.; Stefanadis, C. Prognostic role of miRNAs in coronary artery disease. Curr. Top. Med. Chem. 2013, 13, 1540–1547. [Google Scholar] [CrossRef]
- Sondermeijer, B.M.; Bakker, A.; Halliani, A.; de Ronde, M.W.; Marquart, A.A.; Tijsen, A.J.; Mulders, T.A.; Kok, M.G.; Battjes, S.; Maiwald, S.; et al. Platelets in patients with premature coronary artery disease exhibit upregulation of miRNA340* and miRNA624*. PLoS ONE 2011, 6, e25946. [Google Scholar] [CrossRef]
- Song, M.A.; Paradis, A.N.; Gay, M.S.; Shin, J.; Zhang, L. Differential expression of microRNAs in ischemic heart disease. Drug Discov. Today 2015, 20, 223–235. [Google Scholar] [CrossRef]
- Karakas, M.; Schulte, C.; Appelbaum, S.; Ojeda, F.; Lackner, K.J.; Münzel, T.; Schnabel, R.B.; Blankenberg, S.; Zeller, T. Circulating microRNAs strongly predict cardiovascular death in patients with coronary artery disease-results from the large AtheroGene study. Eur. Heart J. 2017, 38, 516–523. [Google Scholar] [CrossRef]
- Budoff, M.J.; Dowe, D.; Jollis, J.G.; Gitter, M.; Sutherland, J.; Halamert, E.; Scherer, M.; Bellinger, R.; Martin, A.; Benton, R.; et al. Diagnostic performance of 64-multidetector row coronary computed tomographic angiography for evaluation of coronary artery stenosis in individuals without known coronary artery disease: Results from the prospective multicenter ACCURACY (Assessment by Coronary Computed Tomographic Angiography of Individuals Undergoing Invasive Coronary Angiography) trial. J. Am. Coll. Cardiol. 2008, 52, 1724–1732. [Google Scholar]
- Meijboom, W.B.; Meijs, M.F.; Schuijf, J.D.; Cramer, M.J.; Mollet, N.R.; van Mieghem, C.A.; Nieman, K.; van Werkhoven, J.M.; Pundziute, G.; Weustink, A.C.; et al. Diagnostic accuracy of 64-slice computed tomography coronary angiography: A prospective, multicenter, multivendor study. J. Am. Coll. Cardiol. 2008, 52, 2135–2144. [Google Scholar] [CrossRef]
- van Velzen, J.E.; Schuijf, J.D.; de Graaf, F.R.; Boersma, E.; Pundziute, G.; Spanó, F.; Boogers, M.J.; Schalij, M.J.; Kroft, L.J.; de Roos, A.; et al. Diagnostic performance of non-invasive multidetector computed tomography coronary angiography to detect coronary artery disease using different endpoints: Detection of significant stenosis vs. detection of atherosclerosis. Eur. Heart J. 2011, 32, 637–645. [Google Scholar]
- Criqui, M.H.; Denenberg, J.O.; Ix, J.H.; McClelland, R.L.; Wassel, C.L.; Rifkin, D.E.; Carr, J.J.; Budoff, M.J.; Allison, M.A. Calcium density of coronary artery plaque and risk of incident cardiovascular events. JAMA 2014, 311, 271–278. [Google Scholar] [CrossRef]
- Hoffmann, U.; Truong, Q.A.; Schoenfeld, D.A.; Chou, E.T.; Woodard, P.K.; Nagurney, J.T.; Pope, J.H.; Hauser, T.H.; White, C.S.; Weiner, S.G.; et al. Coronary CT angiography versus standard evaluation in acute chest pain. N. Engl. J. Med. 2012, 367, 299–308. [Google Scholar] [CrossRef] [PubMed]
- Fordyce, C.B.; Newby, D.E.; Douglas, P.S. Diagnostic Strategies for the Evaluation of Chest Pain: Clinical Implications From SCOT-HEART and PROMISE. J. Am. Coll. Cardiol. 2016, 67, 843–852. [Google Scholar] [CrossRef] [PubMed]
- Greenland, P.; LaBree, L.; Azen, S.P.; Doherty, T.M.; Detrano, R.C. Coronary artery calcium score combined with Framingham score for risk prediction in asymptomatic individuals. JAMA 2004, 291, 210–215. [Google Scholar] [CrossRef] [PubMed]
- Carr, J.J.; Nelson, J.C.; Wong, N.D.; McNitt-Gray, M.; Arad, Y.; Jacobs, D.R., Jr.; Sidney, S.; Bild, D.E.; Williams, O.D.; Detrano, R.C. Calcified coronary artery plaque measurement with cardiac CT in population-based studies: Standardized protocol of Multi-Ethnic Study of Atherosclerosis (MESA) and Coronary Artery Risk Development in Young Adults (CARDIA) study. Radiology 2005, 234, 35–43. [Google Scholar] [CrossRef]
- Shi, J.; Bei, Y.; Kong, X.; Liu, X.; Lei, Z.; Xu, T.; Wang, H.; Xuan, Q.; Chen, P.; Xu, J.; et al. miR-17-3p Contributes to Exercise-Induced Cardiac Growth and Protects against Myocardial Ischemia-Reperfusion Injury. Theranostics 2017, 7, 664–676. [Google Scholar] [CrossRef]
- Sayed, D.; He, M.; Hong, C.; Gao, S.; Rane, S.; Yang, Z.; Abdellatif, M. MicroRNA-21 is a downstream effector of AKT that mediates its antiapoptotic effects via suppression of Fas ligand. J. Biol. Chem. 2010, 285, 20281–20290. [Google Scholar] [CrossRef]
- Yang, J.; Chen, L.; Yang, J.; Ding, J.; Li, S.; Wu, H.; Zhang, J.; Fan, Z.; Dong, W.; Li, X. MicroRNA-22 targeting CBP protects against myocardial ischemia-reperfusion injury through anti-apoptosis in rats. Mol. Biol. Rep. 2014, 41, 555–561. [Google Scholar] [CrossRef]
- Fang, J.; Song, X.W.; Tian, J.; Chen, H.Y.; Li, D.F.; Wang, J.F.; Ren, A.J.; Yuan, W.J.; Lin, L. Overexpression of microRNA-378 attenuates ischemia-induced apoptosis by inhibiting caspase-3 expression in cardiac myocytes. Apoptosis 2012, 17, 410–423. [Google Scholar] [CrossRef]
- Han, Z.; Guan, Y.; Liu, B.; Lin, Y.; Yan, Y.; Wang, H.; Wang, H.; Jing, B. MicroRNA-99a-5p alleviates atherosclerosis via regulating Homeobox A1. Life Sci. 2019, 232, 116664. [Google Scholar] [CrossRef]
- Jiang, W.; Zhang, Z.; Yang, H.; Lin, Q.; Han, C.; Qin, X. The Involvement of miR-29b-3p in Arterial Calcification by Targeting Matrix Metalloproteinase-2. BioMed Res. Int. 2017, 2017, 6713606. [Google Scholar] [CrossRef]
- Lee, S.T.; Chu, K.; Jung, K.H.; Yoon, H.J.; Jeon, D.; Kang, K.M.; Park, K.H.; Bae, E.K.; Kim, M.; Lee, S.K.; et al. MicroRNAs Induced During Ischemic Preconditioning. Stroke 2010, 41, 1646–1651. [Google Scholar] [CrossRef] [PubMed]
- Semenza, G.L. Hypoxia-inducible factor 1: Regulator of mitochondrial metabolism and mediator of ischemic preconditioning. Biochim. Biophys. Acta 2011, 1813, 1263–1268. [Google Scholar] [CrossRef] [PubMed]
- Rane, S.; He, M.; Sayed, D.; Vashistha, H.; Malhotra, A.; Sadoshima, J.; Vatner, D.E.; Vatner, S.F.; Abdellatif, M. Downregulation of miR-199a derepresses hypoxia-inducible factor-1alpha and Sirtuin 1 and recapitulates hypoxia preconditioning in cardiac myocytes. Circ. Res. 2009, 104, 879–886. [Google Scholar] [CrossRef]
- El Azzouzi, H.; Leptidis, S.; Dirkx, E.; Hoeks, J.; van Bree, B.; Brand, K.; McClellan, E.A.; Poels, E.; Sluimer, J.C.; Van den Hoogenhof, M.M.; et al. The hypoxia-inducible microRNA cluster miR-199a approximately 214 targets myocardial PPARdelta and impairs mitochondrial fatty acid oxidation. Cell Metab. 2013, 18, 341–354. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Ouyang, M.; Wang, Q.; Jian, Z. MicroRNA-142-3p inhibits hypoxia/reoxygenation induced apoptosis and fibrosis of cardiomyocytes by targeting high mobility group box 1. Intern. J. Mol. Med. 2016, 38, 1377–1386. [Google Scholar] [CrossRef]
- Shen, Y.; Shen, Z.; Miao, L.; Xin, X.; Lin, S.; Zhu, Y.; Guo, W.; Zhu, Y.Z. miRNA-30 family inhibition protects against cardiac ischemic injury by regulating cystathionine-gamma-lyase expression. Antioxid. Redox Signal. 2015, 22, 224–240. [Google Scholar] [CrossRef]
- Wang, X.; Zhu, H.; Zhang, X.; Liu, Y.; Chen, J.; Medvedovic, M.; Li, H.; Weiss, M.J.; Ren, X.; Fan, G.C. Loss of the miR-144/451 cluster impairs ischaemic preconditioning-mediated cardioprotection by targeting Rac-1. Cardiovasc. Res. 2012, 94, 379–390. [Google Scholar] [CrossRef]
- Sun, Y.; Su, Q.; Li, L.; Wang, X.; Lu, Y.; Liang, J. MiR-486 regulates cardiomyocyte apoptosis by p53-mediated BCL-2 associated mitochondrial apoptotic pathway. BMC Cardiovasc. Dis. 2017, 17, 119. [Google Scholar] [CrossRef]
- Ke, Z.P.; Xu, P.; Shi, Y.; Gao, A.M. MicroRNA-93 inhibits ischemia-reperfusion induced cardiomyocyte apoptosis by targeting PTEN. Oncotarget 2016, 7, 28796. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.; He, S.; Wara, A.K.M.; Icli, B.; Shvartz, E.; Tesmenitsky, Y.; Belkin, N.; Li, D.; Blackwell, T.S.; Sukhova, G.K.; et al. Systemic delivery of microRNA-181b inhibits nuclear factor-kappaB activation, vascular inflammation, and atherosclerosis in apolipoprotein E-deficient mice. Circ. Res. 2014, 114, 32–40. [Google Scholar] [CrossRef] [PubMed]
- Hu, S.; Huang, M.; Li, Z.; Jia, F.; Ghosh, Z.; Lijkwan, M.A.; Fasanaro, P.; Sun, N.; Wang, X.; Martelli, F.; et al. MicroRNA-210 as a novel therapy for treatment of ischemic heart disease. Circulation 2010, 122, S124–S131. [Google Scholar] [CrossRef] [PubMed]
- Yue, J.; Li, W.; Hong, W.; Yang, J.; Zhu, T.; Fang, Y.; Fu, W.G. MiR-210 inhibits apoptosis of vascular endothelial cells via JAK-STAT in arteriosclerosis obliterans. Eur. Rev. Med. Pharmacol. Sci. 2019, 23 (Suppl. 3), 319–326. [Google Scholar] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gene Symbol | Gene Symbol | Gene Symbol | Gene Symbol | Gene Symbol | Internal Controls |
|---|---|---|---|---|---|
| hsa-let-7a-5p | hsa-miR-130a-3p | hsa-miR-182-5p | hsa-miR-23a-3p | hsa-miR-31-5p | SNORD61 |
| hsa-let-7b-5p | hsa-miR-133a-3p | hsa-miR-183-5p | hsa-miR-23b-3p | hsa-miR-320a | SNORD68 |
| hsa-let-7c-5p | hsa-miR-133b | hsa-miR-185-5p | hsa-miR-24-3p | hsa-miR-328-3p | SNORD72 |
| hsa-let-7d-5p | hsa-miR-140-5p | hsa-miR-18b-5p | hsa-miR-25-3p | hsa-miR-342-3p | SNORD95 |
| hsa-let-7e-5p | hsa-miR-142-3p | hsa-miR-195-5p | hsa-miR-26a-5p | hsa-miR-365b-3p | SNORD96A |
| hsa-let-7f-5p | hsa-miR-143-3p | hsa-miR-199a-5p | hsa-miR-26b-5p | hsa-miR-378a-3p | RNU6-6P |
| hsa-miR-1-3p | hsa-miR-144-3p | hsa-miR-206 | hsa-miR-27a-3p | hsa-miR-423-3p | |
| hsa-miR-100-5p | hsa-miR-145-5p | hsa-miR-208a-3p | hsa-miR-27b-3p | hsa-miR-424-5p | |
| hsa-miR-103a-3p | hsa-miR-146a-5p | hsa-miR-208b-3p | hsa-miR-29a-3p | hsa-miR-451a | |
| hsa-miR-107 | hsa-miR-149-5p | hsa-miR-21-5p | hsa-miR-29b-3p | hsa-miR-486-5p | |
| hsa-miR-10b-5p | hsa-miR-150-5p | hsa-miR-210-3p | hsa-miR-29c-3p | hsa-miR-494-3p | |
| hsa-miR-122-5p | hsa-miR-155-5p | hsa-miR-214-3p | hsa-miR-302a-3p | hsa-miR-499a-5p | |
| hsa-miR-124-3p | hsa-miR-15b-5p | hsa-miR-22-3p | hsa-miR-302b-3p | hsa-miR-7-5p | |
| hsa-miR-125a-5p | hsa-miR-16-5p | hsa-miR-221-3p | hsa-miR-30a-5p | hsa-miR-92a-3p | |
| hsa-miR-125b-5p | hsa-miR-17-5p | hsa-miR-222-3p | hsa-miR-30c-5p | hsa-miR-93-5p | |
| hsa-miR-126-3p | hsa-miR-181a-5p | hsa-miR-223-3p | hsa-miR-30d-5p | hsa-miR-98-5p | |
| hsa-miR-181b-5p | hsa-miR-224-5p | hsa-miR-30e-5p | hsa-miR-99a-5p |
| Characteristics | Patients with CAD (n = 16) | Healthy Controls (n = 16) | p Value |
|---|---|---|---|
| Age (years) | 61.5 ± 11.6 | 46.1 ± 10.8 | <0.001 |
| Male Gender (X) | 16 | 12 | 0.013 |
| Framingham Score | 14.2 ± 7.7 | 8.1 ± 7.9 | 0.016 |
| CACS | 518.9 ± 631.6 | 0 | 0.001 |
| Systolic Blood Pressure | 129.8 ± 13.9 | 122.5 ± 22.1 | 0.326 |
| Type 2 Diabetes (n) | 5 (29%) | 2 (12.5%) | 0.124 |
| Dyslipidemia (n) | 11 (65%) | 5 (31%) | 0.029 |
| CHF (n) | 1 (6%) | 0 | 0.17 |
| Active Smoker (n) | 7 (41%) | 9 (56%) | 0.283 |
| Total Cholesterol | 173.2 ± 42.2 | 193.8 ± 45.1 | 0.098 |
| LDL-Cholesterol | 98.6 ± 40.5 | 116.4 ± 35.4 | 0.169 |
| HDL-Cholesterol | 45.9 ± 15.1 | 37.4 ± 17.7 | 0.075 |
| Medications (n) | |||
| Antiplatelet | 8 (47%) | 1 (6%) | 0.004 |
| β-Blockers | 8 (47%) | 2 (12.5%) | 0.016 |
| Stain | 9 (53%) | 8 (50%) | 0.435 |
| ACE or ARB | 9 (53%) | 3 (19%) | 0.045 |
| Calcium Channel Blocker | 4 (24%) | 2 (12.5%) | 0.214 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Patterson, A.J.; Song, M.A.; Choe, D.; Xiao, D.; Foster, G.; Zhang, L. Early Detection of Coronary Artery Disease by Micro-RNA Analysis in Asymptomatic Patients Stratified by Coronary CT Angiography. Diagnostics 2020, 10, 875. https://doi.org/10.3390/diagnostics10110875
Patterson AJ, Song MA, Choe D, Xiao D, Foster G, Zhang L. Early Detection of Coronary Artery Disease by Micro-RNA Analysis in Asymptomatic Patients Stratified by Coronary CT Angiography. Diagnostics. 2020; 10(11):875. https://doi.org/10.3390/diagnostics10110875
Chicago/Turabian StylePatterson, Andrew J., Minwoo A. Song, David Choe, Daliao Xiao, Gary Foster, and Lubo Zhang. 2020. "Early Detection of Coronary Artery Disease by Micro-RNA Analysis in Asymptomatic Patients Stratified by Coronary CT Angiography" Diagnostics 10, no. 11: 875. https://doi.org/10.3390/diagnostics10110875
APA StylePatterson, A. J., Song, M. A., Choe, D., Xiao, D., Foster, G., & Zhang, L. (2020). Early Detection of Coronary Artery Disease by Micro-RNA Analysis in Asymptomatic Patients Stratified by Coronary CT Angiography. Diagnostics, 10(11), 875. https://doi.org/10.3390/diagnostics10110875