Postnatal Outcome and Associated Anomalies of Prenatally Diagnosed Right Aortic Arch with Concomitant Right Ductal Arch: A Systematic Review and Meta-Analysis

 ,
,  ,
, 
Abstract
1. Introduction
1.1. Rationale
1.2. Objectives
2. Materials and Methods
2.1. Search Strategy, Information Sources and Eligibility
2.2. Study Selection, Data Collection, and Outcomes
2.3. Study Quality Assessment
2.4. Statistical Analysis
3. Results
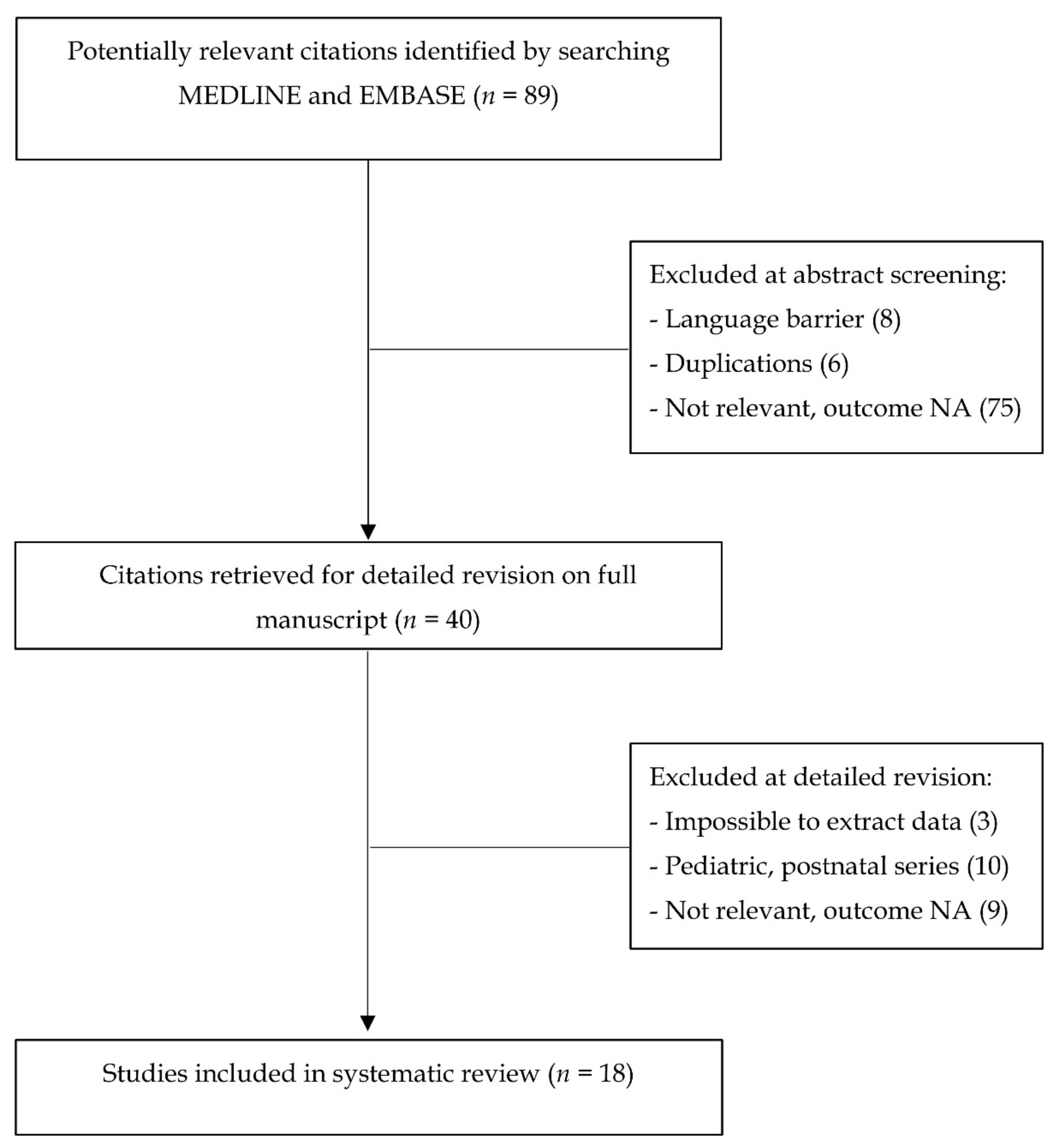
3.1. Study Selection and Characteristics
3.2. Synthesis of Results
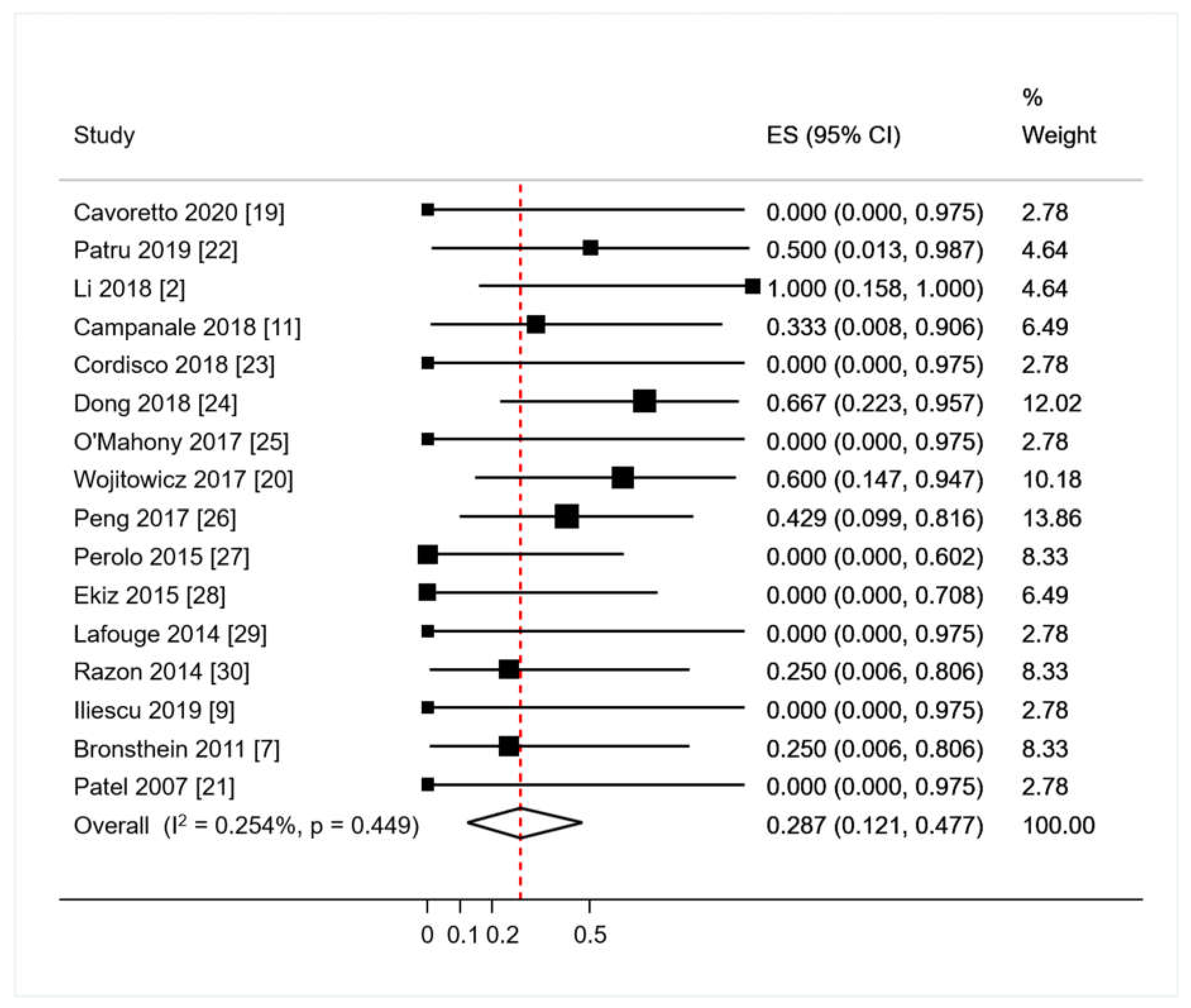
3.2.1. Primary Analysis: Proportions of Abnormal Outcomes in RAA/RDA
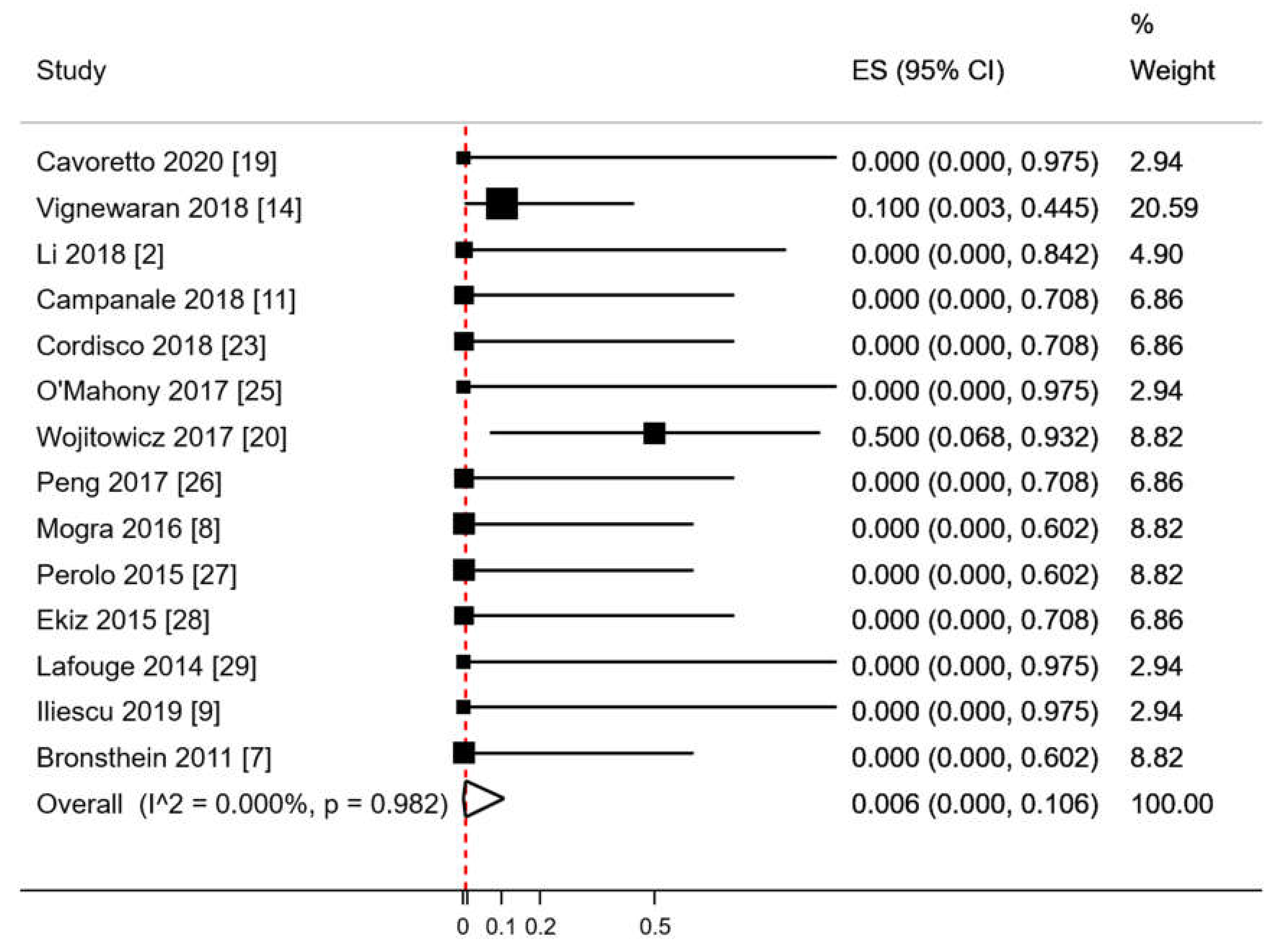
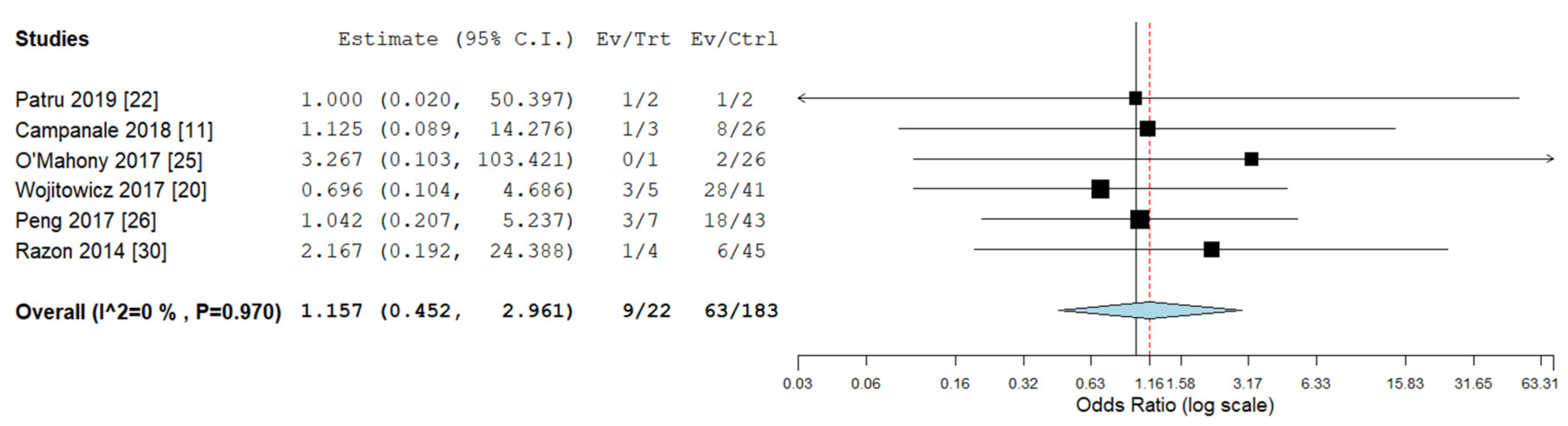
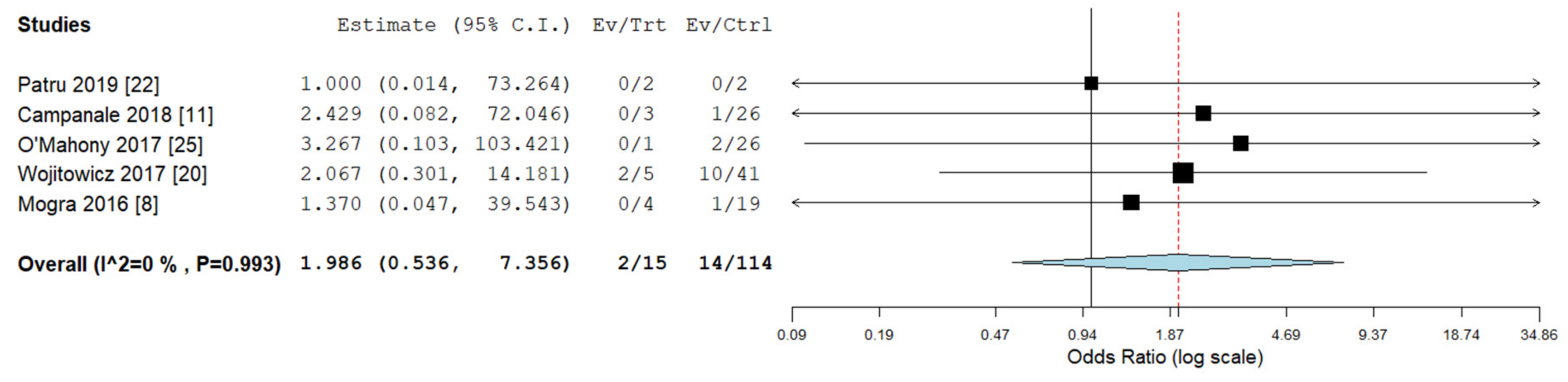
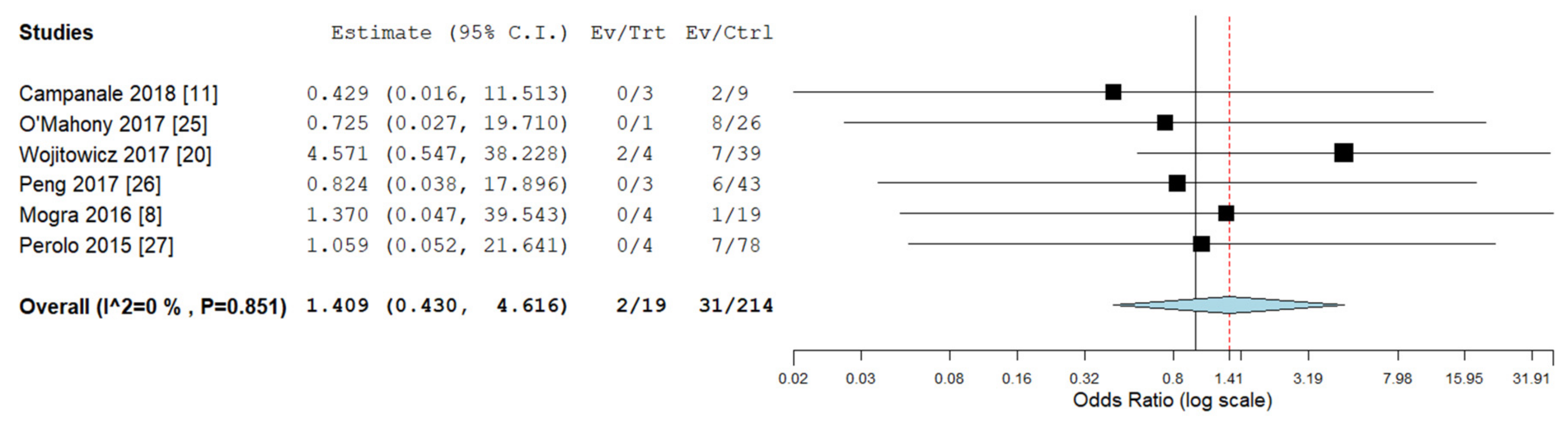
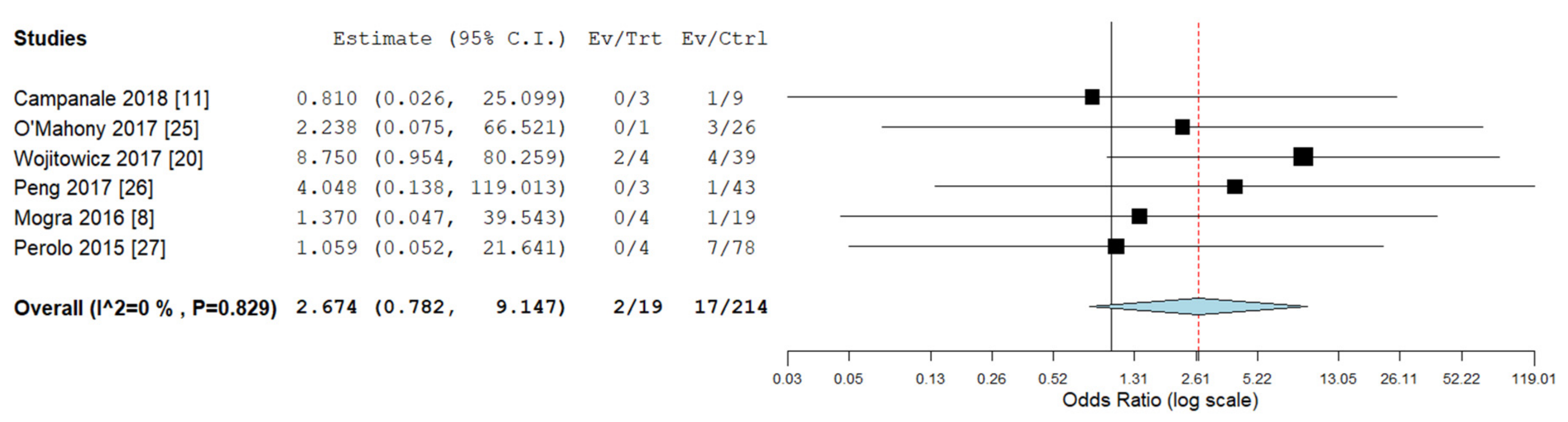
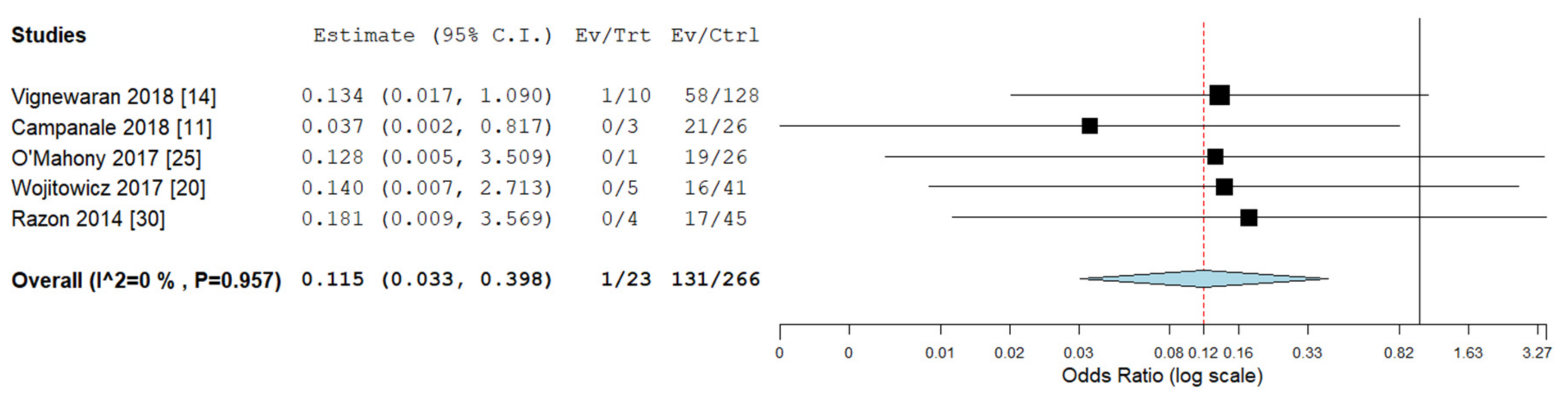
3.2.2. Secondary Analyses: Outcomes in RAA/RDA versus RAA/LDA
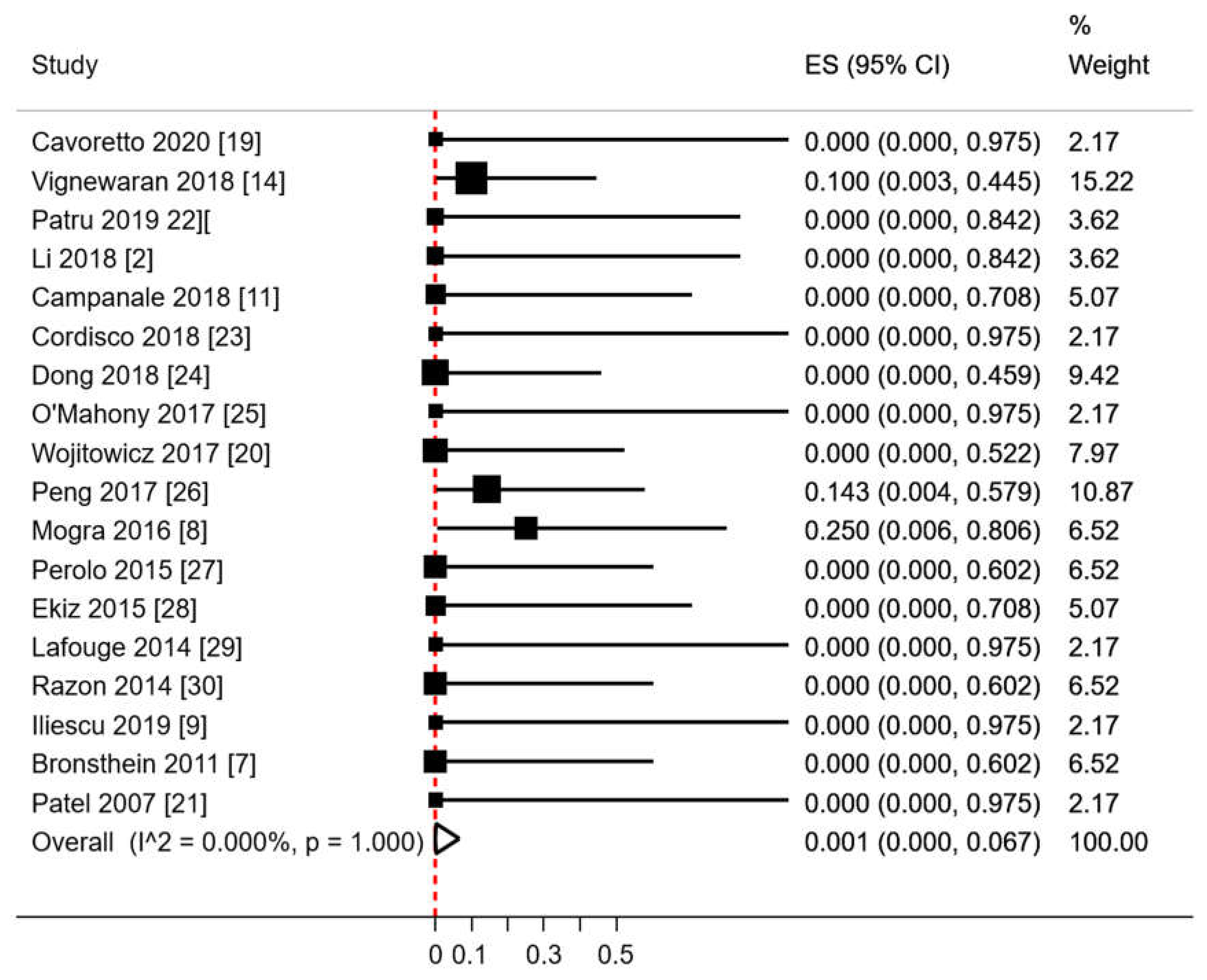
3.2.3. Other Results
3.3. Risk of Bias Assessment
4. Discussion
4.1. Summary of Key Findings
4.2. Interpretation
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| ALSA | aberrant left subclavian artery |
| DA | ductus arteriosus |
| ECA | extra-cardiac abnormalities |
| ICA | intra-cardiac abnormalities |
| LAA | left sided aortic arch |
| LDA: | left sided ductal arch |
| ISUOG | International Society of Ultrasound in Obstetrics and Gynecology (ISUOG) |
| NICE | National Institute for Health and Care Excellence (United Kingdom) |
| NIH | National Institute of Health (United States of America) |
| RAA | right sided aortic arch |
| RDA | right sided ductal arch |
| RAA/RDA | right aortic arch with concomitant right ductal arch |
References
- Li, S.; Luo, G.; Norwitz, E.R.; Wang, C.; Ouyang, S.; Yao, Y.; Chen, C.; Wen, H.; Chen, X.; Bi, J. Prenatal diagnosis of congenital vascular rings and slings: Sonographic features and perinatal outcome in 81 consecutive cases. Prenat. Diagn. 2011, 31, 334–346. [Google Scholar] [CrossRef] [PubMed]
- Li, S.L.; Wen, H.; Liang, M.; Luo, D.; Qin, Y.; Liao, Y.; Ouyang, S.; Bi, J.; Tian, X.; Norwitz, E.R.; et al. Congenital abnormalities of the aortic arch: Revisiting the 1964 Stewart classification. Cardiovasc. Pathol. 2019, 39, 38–50. [Google Scholar] [CrossRef] [PubMed]
- Ottaviani, G.; Buja, L.M. Congenital heart disease: Pathology, natural history and interventions. In Cardiovascular Pathology, 4th ed.; Buja, L.M., Butany, J., Eds.; Elsevier Academic Press: Cambridge, MA, USA, 2016; pp. 611–647. [Google Scholar] [CrossRef]
- Yagel, S.; Arbel, R.; Anteby, E.Y.; Raveh, D.; Achiron, R. The three vessels and trachea view (3VT) in fetal cardiac scanning. Ultrasound Obstet. Gynecol. 2002, 20, 340–345. [Google Scholar] [CrossRef] [PubMed]
- Lee, V.L.; Allan, L.; Carvalho, J.S.; Chaoui, R.; Copel, J.; Devore, G.; Hecher, K.; Munoz, H.; Nelson, T.; Paladini, D.; et al. ISUOG consensus statement: What constitutes a fetal echocardiogram? Ultrasound Obstet. Gynecol. 2008, 32, 239–242. [Google Scholar] [CrossRef] [PubMed]
- D’Antonio, F.; Khalil, A.; Zidere, V.; Carvalho, J.S. Fetuses with right aortic arch Multicentre cohort study and meta-analysis. Ultrasound Obstet. Gynecol. 2016, 47, 423–432. [Google Scholar] [CrossRef]
- Bronshtein, M.; Zimmer, E.Z.; Blazer, S.; Blumenfeld, Z. Right ductus arteriosus: Facts and theory. Eur. J. Obstet. Gynecol. Reprod. Biol. 2011, 159, 282–288. [Google Scholar] [CrossRef]
- Mogra, R.; Kesby, G.; Sholler, G.; Hyett, J. Identification and management of fetal isolated right-sided aortic arch in an unselected population. Ultrasound Obstet. Gynecol. 2016, 48, 739–743. [Google Scholar] [CrossRef]
- Iliescu, D.; Comanescu, A.C.; Tudorache, S.; Cernea, N. Right aortic arch with patent right ductus arteriosus and normal heart. Ultrasound Obstet. Gynecol. 2012, 40, 115–116. [Google Scholar] [CrossRef]
- Achiron, R.; Rotstein, Z.; Heggesh, J.; Bronshtein, M.; Zimand, S.; Lipitz, S.; Yagel, S. Anomalies of the fetal aortic arch: A novel sonographic approach toin-uterodiagnosis. Ultrasound Obstet. Gynecol. 2002, 20, 553–557. [Google Scholar] [CrossRef] [PubMed]
- Campanale, C.M.; Pasquini, L.; Santangelo, T.P.; Iorio, F.S.; Bagolan, P.; Sanders, S.P.; Toscano, A. Prenatal echocardiographic assessment of right aortic arch. Ultrasound Obstet. Gynecol. 2019, 54, 96–102. [Google Scholar] [CrossRef] [PubMed]
- Berg, C.; Bender, F.; Soukup, M.; Geipel, A.; Axt-Fliedner, R.; Breuer, J.; Herberg, U.; Gembruch, U. Right aortic arch detected in fetal life. Ultrasound Obstet. Gynecol. 2006, 28, 882–889. [Google Scholar] [CrossRef] [PubMed]
- Zidere, V.; Tsapakis, E.G.; Huggon, I.C.; Allan, L. Right aortic arch in the fetus. Ultrasound Obstet. Gynecol. 2006, 28, 876–881. [Google Scholar] [CrossRef] [PubMed]
- Vigneswaran, T.V.; Allan, L.; Charakida, M.; Durward, A.; Simpson, J.M.; Nicolaides, K.H.; Zidere, V. Prenatal diagnosis and clinical implications of an apparently isolated right aortic arch. Prenat. Diagn. 2018, 38, 1055–1061. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Efthimiou, O. Practical guide to the meta-analysis of rare events. Evid. Based Ment. Health 2018, 21, 72–76. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Cavoretto, P.I.; Fesslova, V.; Spinillo, S.; Pozzoni, M.; Girardelli, A.; Galdini, G.; Gaeta, G.; Farina, A.; Candiani, M. Postnatal outcome of prenatally diagnosed isolated right aortic arch with concomitant right ductal arch: Systematic review. In Proceedings of the International Society of Ultrasound in Obstetrics and Gynecology (ISUOG); Virtual World Congress on Ultrasound in Obstetrics and Gynecology, 16–18 October 2020. [Google Scholar]
- Wojtowicz, A.; Respondek-Liberska, M.; Słodki, M.; Kordjalik, P.; Pluzanska, J.; Knafel, A.; Huras, H. The significance of a prenatal diagnosis of right aortic arch. Prenat. Diagn. 2017, 37, 365–374. [Google Scholar] [CrossRef]
- Patel, C.R.; Smith, G.L.; Lane, J.R.; Robinson, H.B. Prenatal echocardiographic diagnosis of a right aortic arch and bilateral arterial duct with isolation of the left subclavian artery from the left pulmonary artery. J. Ultrasound Med. 2007, 26, 1107–1110. [Google Scholar] [CrossRef]
- Pătru, C.L.; Tudorache, Ş.; Marinaş, M.C.; Drăgușin, R.C.; Zorilă, G.L.; Nagy, R.D.; Pascu, R.M.; Cernea, N. First trimester ultrasound diagnosis of right aortic arch (RAA). Curr Health Sci J. 2019, 45, 296–300. [Google Scholar]
- Cordisco, A.; Murzi, B.; Chiappa, E. Right aortic arch with bilateral arterial duct and nonconfluent pulmonary arteries without associated cardiac defects: Prenatal diagnosis and successful postnatal treatment. J. Obstet. Gynaecol. Res. 2018, 44, 1828–1831. [Google Scholar] [CrossRef]
- Dong, S.-Z.; Zhu, M. Utility of fetal cardiac magnetic resonance imaging to assess fetuses with right aortic arch and right ductus arteriosus. J. Matern. Fetal. Neonatal Med. 2018, 31, 1627–1631. [Google Scholar] [CrossRef]
- O’Mahony, E.; Hutchinson, D.P.; McGillivray, G.; Nisbet, D.L.; Palma-Dias, R. Right-sided aortic arch in the age of microarray. Prenat. Diagn. 2017, 37, 440–445. [Google Scholar] [CrossRef] [PubMed]
- Peng, R.; Xie, H.-N.; Zheng, J.; Zhou, Y.; Lin, M.F. Fetal right aortic arch: Associated anomalies, genetic anomalies with chromosomal microarray analysis, and postnatal outcome. Prenat. Diagn. 2017, 37, 329–335. [Google Scholar] [CrossRef]
- Perolo, A.; De Robertis, V.; Cataneo, I.; Volpe, N.; Campobasso, G.; Frusca, T.; Ghi, T.; Prandstraller, D.; Pilu, G.; Volpe, P. The risk of 22q11.2 deletion in foetuses with a right aortic arch and without intracardiac anomalies. Ultrasound Obstet. Gynecol. 2016, 48, 200–203. [Google Scholar] [CrossRef]
- Ekiz, A.; Gul, A.; Uludogan, M.; Bornaun, H. Prenatal diagnosis and postnatal outcome of persistent right ductus arteriosus: A report of three cases. J. Med. Ultrason. 2015, 42, 571–574. [Google Scholar] [CrossRef]
- Lafouge, A.; Quarello, E. Right aortic arch and ductus arteriosus: A case diagnosed during the first trimester of pregnancy. Diagn. Interv. Imaging 2014, 95, 877–879. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Razon, Y.; Berant, M.; Fogelman, R.; Amir, G.; Birk, E. Prenatal diagnosis and outcome of right aortic arch without significant intracardiac anomaly. J. Am. Soc. Echocardiogr. 2014, 27, 1352–1358. [Google Scholar] [CrossRef]
- NHS Fetal Anomaly Screening Programme Handbook. Available online: https://www.gov.uk/government/publications/fetal-anomaly-screening-programme-handbook (accessed on 8 October 2020).
- Scala, C.; Maggiore, U.L.R.; Candiani, M.; Venturini, P.P.L.; Ferrero, S.; Greco, T.; Cavoretto, P. Aberrant right subclavian artery in fetuses with Down syndrome: A systematic review and meta-analysis. Ultrasound Obstet. Gynecol. 2015, 46, 266–276. [Google Scholar] [CrossRef] [PubMed]
- Inversetti, A.; Fesslova, V.; Deprest, J.; Candiani, M.; Giorgione, V.; Cavoretto, P. Prenatal growth in fetuses with isolated cyanotic and non-cyanotic congenital heart defects. Fetal Diagn. Ther. 2020, 47, 411–419. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Country | RAA RDA | RAA LDA | GA Diagnosis of RAA + RDA (Mean) | Outcomes Observed | GRADE AHQR Standards |
|---|---|---|---|---|---|---|
| Cavoretto (2020) [19] | Italy | 1 | NA | 20 | ICA, ECA and CA | fair |
| Patru (2019) [22] | Romania | 2 | 2 | Second trimester | ICA, ECA and CA | fair |
| Vigneswaran (2018) [14] | UK | 10 | NS | median 21 (range 11–36) | ICA, ECA and CA | good |
| Li (2019) [2] | China | 2 | 0 | NA | ICA, ECA and CA | good |
| Campanale (2018) [11] | Italy | 3 | 26 | mean 26 ± 5 | ICA, ECA and CA | fair |
| Cordisco (2018) [23] | Italy | 1 | NA | 25 | ICA, ECA and CA (bilateral DA) | fair |
| Dong (2018) [24] | China | 6 | 0 | 28.2 (range 24–35) | ICA, ECA CA = 0 | good |
| O’Mahony (2017) [25] | Australia | 1 | 29 | 20 | ICA, ECA and CA | good |
| Wòjtowicz (2017) [20] | Poland | 5 | 41 | 24.6 (range 20–31) | ICA, ECA and CA | good |
| Peng (2017) [26] | China | 7 | 43 | mean 24 | ICA, and CA ECA = 0 | fair |
| Mogra (2016) [8] | Australia | 4 | 19 | mean 19 | ICA, ECA and CA | fair |
| Perolo (2016) [27] | Italy | 4 | NA | mean 20.9 ± 3 | ICA, ECA and CA | fair |
| Ekiz (2015) [28] | Turkey | 3 | 0 | 31 + 6; 22 + 4; NA | ICA, ECA and CA | good |
| Lafouge (2014) [29] | France | 1 | NA | 11 + 6 | ICA, ECA and CA | fair |
| Razon (2014) [30] | Israel | 4 | 45 | mean 22.7 | ICA and ECA CA = 0 | fair |
| Iliescu (2012) [9] | Romania | 1 | NA | first trimester | ICA, ECA and CA | fair |
| Bronsthein (2011) [7] | Israel | 4 | 0 | 89% between 14–16 weeks | ICA and ECA CA = 0 | good |
| Patel (2007) [21] | USA | 1 | NA | 25 | ICA, ECA and CA | fair |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cavoretto, P.I.; Sotiriadis, A.; Girardelli, S.; Spinillo, S.; Candiani, M.; Amodeo, S.; Farina, A.; Fesslova, V. Postnatal Outcome and Associated Anomalies of Prenatally Diagnosed Right Aortic Arch with Concomitant Right Ductal Arch: A Systematic Review and Meta-Analysis. Diagnostics 2020, 10, 831. https://doi.org/10.3390/diagnostics10100831
Cavoretto PI, Sotiriadis A, Girardelli S, Spinillo S, Candiani M, Amodeo S, Farina A, Fesslova V. Postnatal Outcome and Associated Anomalies of Prenatally Diagnosed Right Aortic Arch with Concomitant Right Ductal Arch: A Systematic Review and Meta-Analysis. Diagnostics. 2020; 10(10):831. https://doi.org/10.3390/diagnostics10100831
Chicago/Turabian StyleCavoretto, Paolo Ivo, Alexandros Sotiriadis, Serena Girardelli, Silvia Spinillo, Massimo Candiani, Silvia Amodeo, Antonio Farina, and Vlasta Fesslova. 2020. "Postnatal Outcome and Associated Anomalies of Prenatally Diagnosed Right Aortic Arch with Concomitant Right Ductal Arch: A Systematic Review and Meta-Analysis" Diagnostics 10, no. 10: 831. https://doi.org/10.3390/diagnostics10100831
APA StyleCavoretto, P. I., Sotiriadis, A., Girardelli, S., Spinillo, S., Candiani, M., Amodeo, S., Farina, A., & Fesslova, V. (2020). Postnatal Outcome and Associated Anomalies of Prenatally Diagnosed Right Aortic Arch with Concomitant Right Ductal Arch: A Systematic Review and Meta-Analysis. Diagnostics, 10(10), 831. https://doi.org/10.3390/diagnostics10100831