Diagnostic Value of C-Reactive Protein in Discrimination between Uncomplicated and Complicated Parapneumonic Effusion

Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Methods
2.3. Statistical Analysis
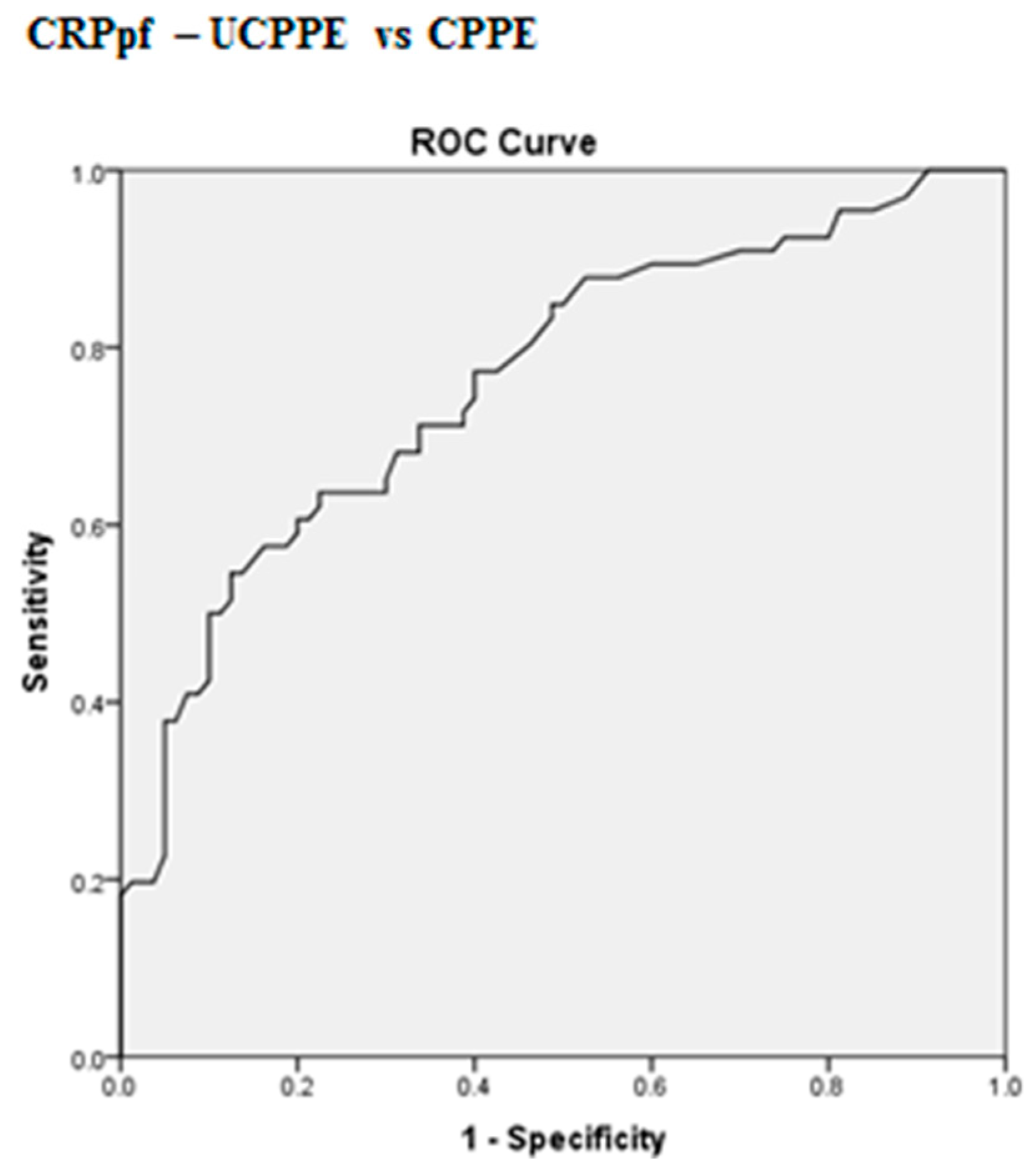
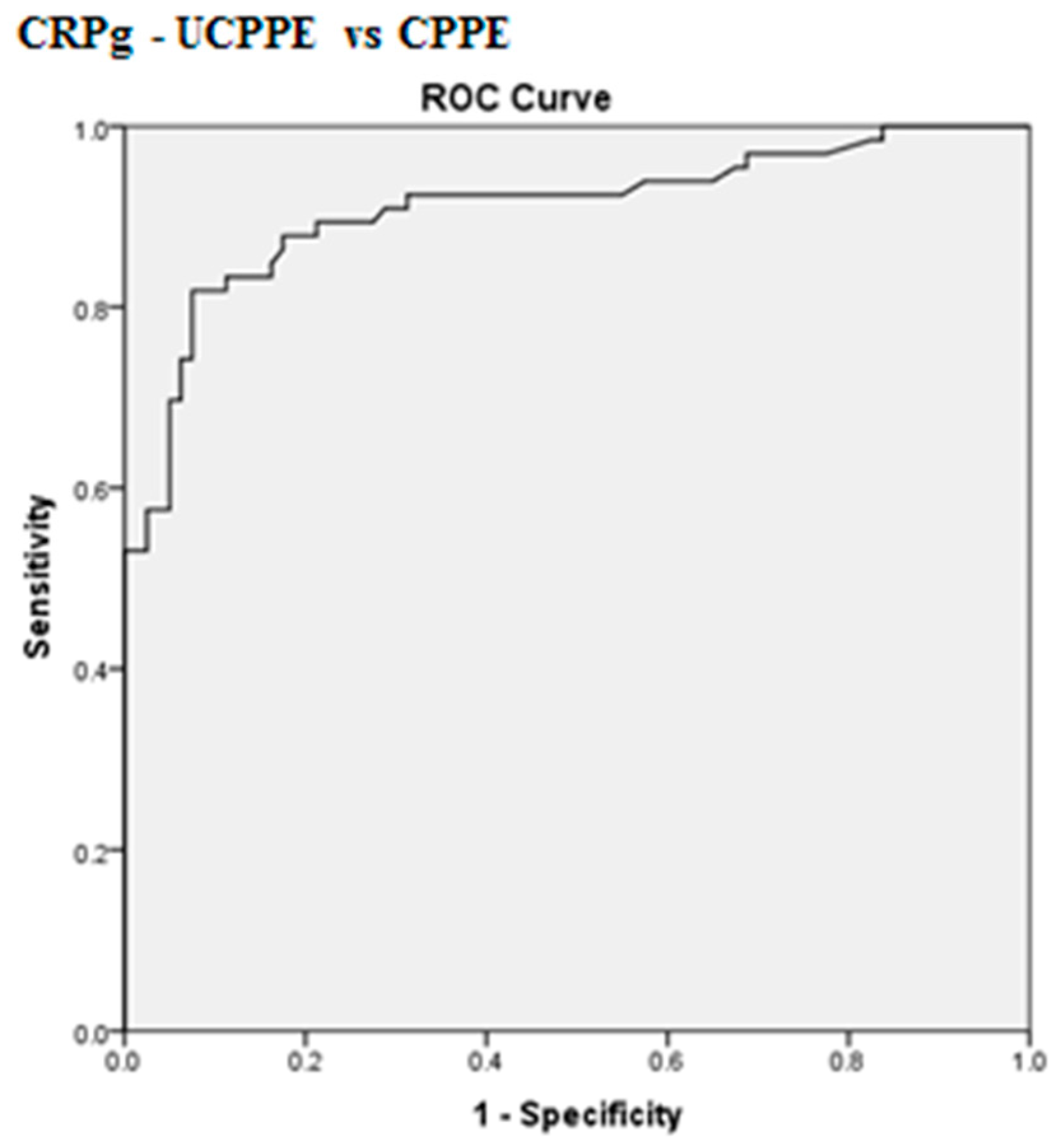
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Feller-Kopman, D.; Light, R. Pleural disease. N. Engl. J. Med. 2018, 378, 740–751. [Google Scholar] [CrossRef] [PubMed]
- Porcel, J.M.; Pardina, M.; Alemán, C.; Pallisa, E.; Light, R.W.; Bielsa, S. Computed tomography scoring system for discriminating between parapneumonic effusions eventually drained and those cured only with antibiotics. Respirology 2017, 22, 1199–1204. [Google Scholar] [CrossRef] [PubMed]
- Porcel, J.M. Distinguishing complicated from uncomplicated parapneumonic effusions. Curr. Opin. Pulm. Med. 2015, 21, 346–351. [Google Scholar] [CrossRef] [PubMed]
- Falguera, M.; Carratalà, J.; Bielsa, S.; García-Vidal, C.; Ruiz-González, A.; Chica, I.; Gudiol, F.; Porcel, J.M. Predictive factors, microbiology and outcome of patients with parapneumonic effusion. Eur. Respir. J. 2011, 38, 1173–1179. [Google Scholar] [CrossRef]
- Porcel, J.M. Pleural fluid tests to identify complicated parapneumonic effusions. Curr. Opin. Pulm. Med. 2010, 16, 357–361. [Google Scholar] [CrossRef]
- Raymond, D. Surgical intervention for thoracic infections. Surg. Clin. N. Am. 2014, 94, 1283–1303. [Google Scholar] [CrossRef]
- Porcel, J.M.; Esquerda, A.; Vives, M.; Bielsa, S. Etiology of pleural effusions: Analysis of more than 3000 consecutive thoracenteses. Arch. Bronconeumol. 2014, 50, 161–165. [Google Scholar] [CrossRef]
- Bedawi, E.O.; Hassan, M.; Rahman, N.M. Recent developments in the management of pleural infection: A comprehensive review. Clin. Respir. J. 2018, 12, 2309–2320. [Google Scholar] [CrossRef] [PubMed]
- Ferreiro, L.; San José, M.E.; Valdés, L. Management of parapneumonic pleural effusion in adults. Arch. Bronconeumol. 2015, 51, 637–646. [Google Scholar] [CrossRef]
- Davies, H.E.; Davies, R.J.O.; Davies, C.W.H. On behalf of the BTS Pleural Disease Guideline Group. Management of pleural infection in adults: British Thoracic Society Pleural Disease Guideline 2010. Thorax 2010, 65 (Suppl. S2), ii41–ii53. [Google Scholar] [CrossRef] [PubMed]
- Bielsa, S.; Valencia, H.; Ruiz-González, A.; Esquerda, A.; Porcel, J.M. Serum C-reactive protein as an adjunct for identifying complicated parapneumonic effusions. Lung 2014, 192, 577–581. [Google Scholar] [CrossRef] [PubMed]
- Porcel, J.M. Pleural fluid biomarkers: Beyond the Light criteria. Clin. Chest Med. 2013, 34, 27–37. [Google Scholar] [CrossRef] [PubMed]
- Rahman, N.M.; Mishra, E.K.; Davies, H.E.; Davies, R.J.; Lee, Y.C. Clinically important factors influencing the diagnostic measurement of pleural fluid pH and glucose. Am. J. Respir. Crit. Care Med. 2008, 178, 483–490. [Google Scholar] [CrossRef] [PubMed]
- Maskell, N.A.; Gleesonm, F.V.; Darby, M.; Davies, R.J. Diagnostically significant variations in pleural fluid pH in loculated parapneumonic effusions. Chest 2004, 126, 2022–2024. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Shen, Y.; Qin, J.; Wan, C.; Zeng, N.; Chen, L.; Dong, Y. Diagnostic performance of C-reactive protein for parapneumonic pleural effusion: A meta-analysis. Ann. Transl. Med. 2019, 7, 1. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.C.; Chen, W.; Hsu, W.H.; Yu, Y.H.; Shih, C.M. Role of pleural fluid C-reactive protein concentration in discriminating uncomplicated parapneumonic pleural effusions from complicated parapneumonic effusion and empyema. Lung 2006, 184, 141–145. [Google Scholar] [CrossRef] [PubMed]
- Porcel, J.M.; Galindo, C.; Esquerda, A.; Trujillano, J.; Ruiz-González, A.; Falguera, M.; Vives, M. Pleural fluid interleukin-8 and C-reactive protein for discriminating complicated non-purulent from uncomplicated parapneumonic effusions. Respirology 2008, 13, 58–62. [Google Scholar] [CrossRef]
- Porcel, J.M.; Vives, M.; Cao, G.; Bielsa, S.; Ruiz-González, A.; Martínez-Iribarren, A.; Esquerda, A. Biomarkers of infection for the differential diagnosis of pleural effusions. Eur. Respir. J. 2009, 34, 1383–1389. [Google Scholar] [CrossRef]
- Porcel, J.M.; Bielsa, S.; Esquerda, A.; Ruiz-González, A.; Falguera, M. Pleural fluid C-reactive protein contributes to the diagnosis and assessment of severity of parapneumonic effusions. Eur. J. Intern. Med. 2012, 23, 447–450. [Google Scholar] [CrossRef]
- Skouras, V.; Boultadakis, E.; Nikoulis, D.; Polychronopoulos, V.; Daniil, Z.; Kalomenidis, I.; Gourgoulianis, K.I. Prognostic value of C-reactive protein in parapneumonic effusions. Respirology 2012, 17, 308–314. [Google Scholar] [CrossRef]
- Porcel, J.M.; Valencia, H.; Bielsa, S. Factors influencing pleural drainage in parapneumonic effusions. Rev. Clin. Esp. 2016, 216, 361–366. [Google Scholar] [CrossRef] [PubMed]
- Marinkovic, S.P.; Topuzovska, I.K.; Stevanovic, M.; Anastasovska, A. Features of Parapneumonic Effusions. Pril (Makedon. Akad. Nauk. Umet. Odd. Med. Nauk.) 2018, 39, 131–141. [Google Scholar] [CrossRef]
- Petrusevska-Marinkovic, S.; Kondova-Topuzovska, I.; Milenkovic, Z.; Kondov, G.; Anastasovska, A. Clinical, Laboratory and Radiographic Features of Patients with Pneumonia and Parapneumonic Effusions. Open Access Maced. J. Med. Sci. 2016, 4, 428–434. [Google Scholar] [CrossRef] [PubMed]
- Wu, K.A.; Wu, C.C.; Liu, Y.C.; Hsueh, P.C.; Chin, C.Y.; Wang, C.L.; Chu, C.M.; Shih, L.J.; Yang, C.Y. Combined serum biomarkers in the noninvasive diagnosis of complicated parapneumonic effusions and empyema. BMC Pulm. Med. 2019, 19, 108. [Google Scholar] [CrossRef]
- Yilmaz Turay, U.; Yildirim, Z.; Türköz, Y.; Biber, C.; Erdoğan, Y.; Keyf, A.I.; Uğurman, F.; Ayaz, A.; Ergun, P.; Harputluoglu, Y. Use of pleural fluid C-reactive protein in diagnosis of pleural effusions. Respir. Med. 2000, 94, 432–435. [Google Scholar] [CrossRef] [PubMed]
- Elsammak, M.M.Y.; Morsi, T.S.; Khamis, H.I.; Ragab, M.S.; Zaki, M.A.; Abdel-Hadi, M.; Hassan, H.A. Osteopontin and C-reactive protein in Egyptian patients affected with tuberculous and malignant pleural effusion. Ann. Clin. Biochem. 2007, 44, 264–272. [Google Scholar] [CrossRef]
- Chierakul, N.; Kanitsap, A.; Chaiprasert, A.; Viriyataveekul, R. A simple C-reactive protein measurement for the differentiation between tuberculous and malignant pleural effusion. Respirology 2004, 9, 66–69. [Google Scholar] [CrossRef] [PubMed]
- Kiropoulos, T.S.; Kostikas, K.; Oikonomidi, S.; Tsilioni, I.; Nikoulis, D.; Germenis, A.; Gourgoulianis, K.I. Acute phase markers for the differentiation of infectious and malignant pleural effusions. Respir. Med. 2007, 1015, 910–918. [Google Scholar] [CrossRef][Green Version]
- Odeh, M.; Makhoul, B.; Sabo, E.; Srugo, I.; Oliven, A. The role of pleural fluid-serum gradient of tumor necrosis factor-alpha concentration in discrimination between complicated and uncomplicated parapneumonic effusion. Lung 2005, 183, 13–27. [Google Scholar] [CrossRef]
- Hutchinson, W.L.; Koenig, W.; Frohlich, M.; Sund, M.; Lowe, G.D.O.; Pepys, M.B. Immunoradiometric assay of circulating C-reactive protein: Age-related values in the adult general population. Clin. Chem. 2000, 46, 934–938. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | UCPPE (n = 86) | CPPE (n = 60) | p |
|---|---|---|---|
| Age (years) | 65.9 ± 18.1 | 74.1 ± 13.6 | <0.003 |
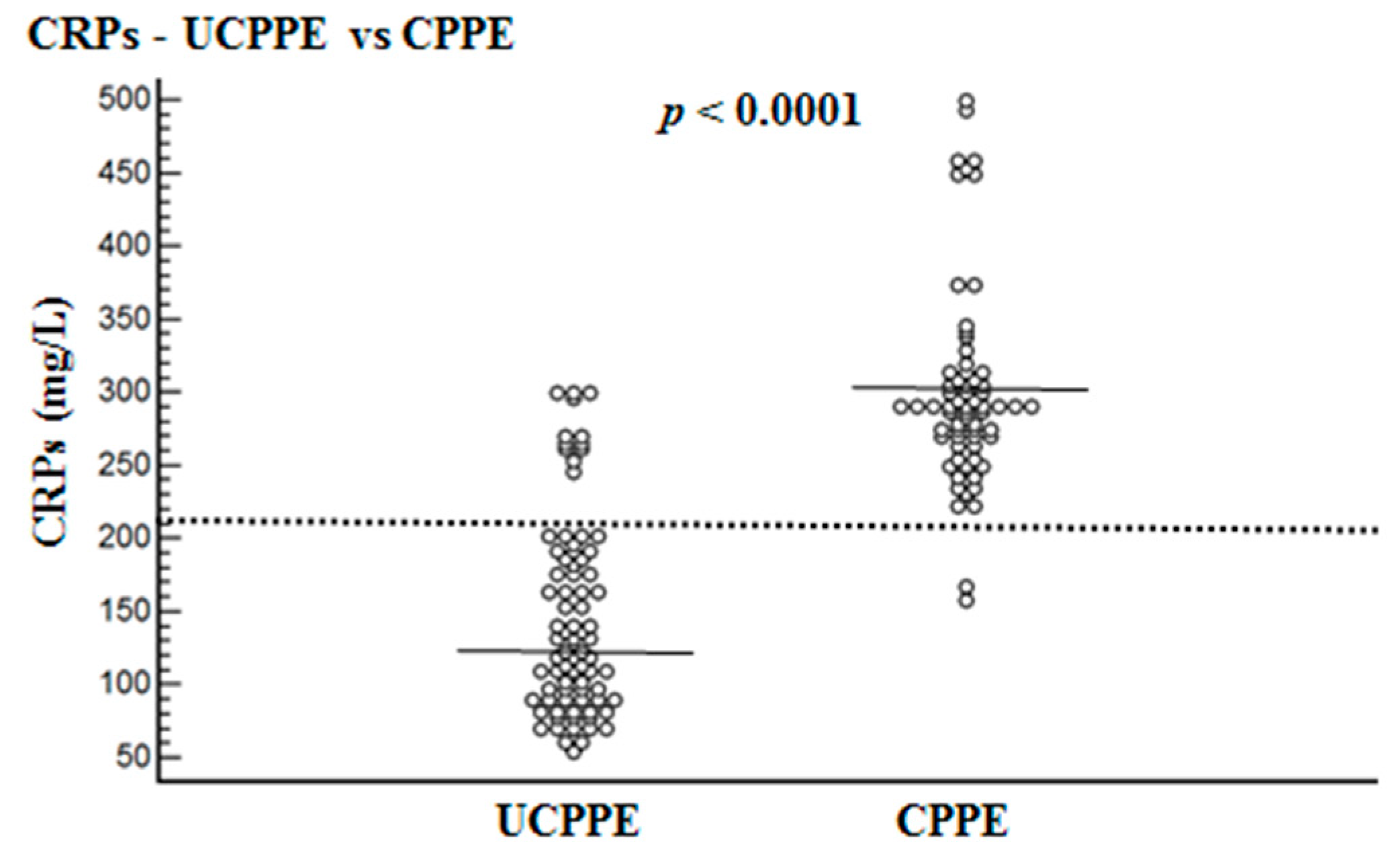
| CRPs (mg/L) 95% CI | 145.3 ± 67.6 130.5–160.1 | 302.2 ± 75.6 283.9–320.4 | <0.0001 |
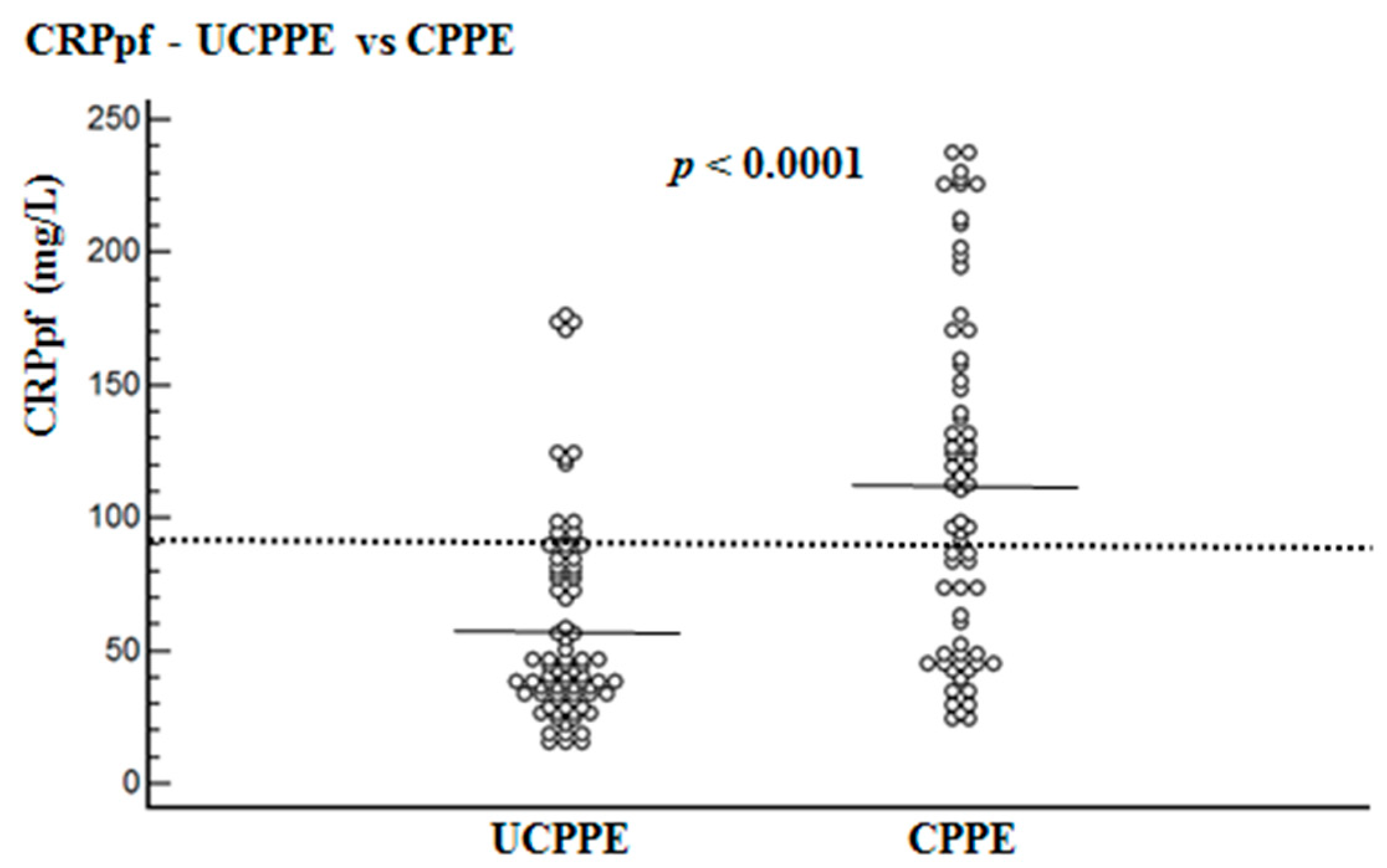
| CRPpf (mg/L) 95% CI | 58.5 ± 38.5 19.2–85.1 | 112.0 ± 65.0 96.0–128.0 | <0.0001 |
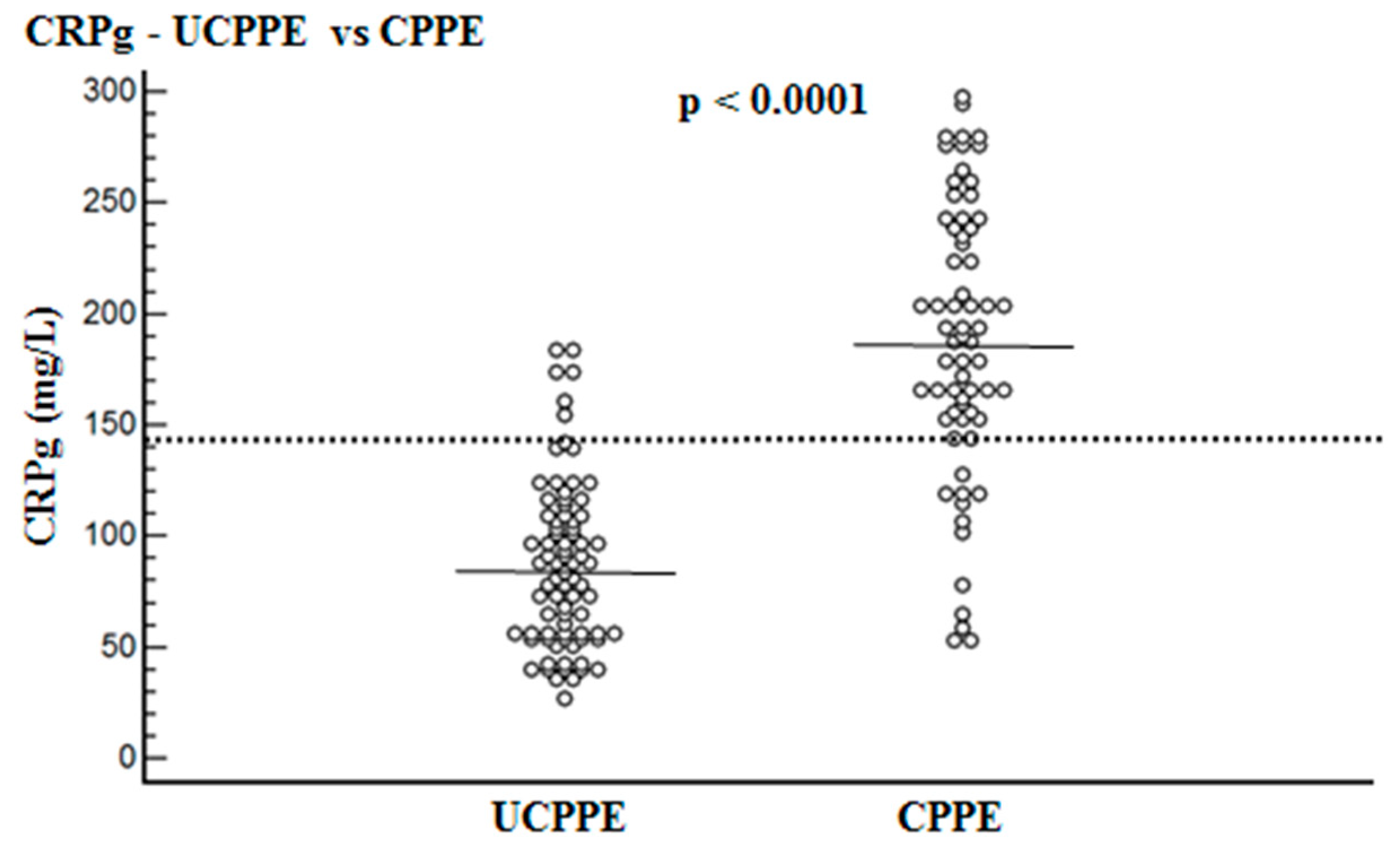
| CRPg (mg/L) 95% CI | 86.9 ± 37.3 48.6–99.2 | 188.3 ± 62.3 173.0–203.6 | <0.0001 |
| CRPr 95% CI | 0.39 ± 0.11 0.31–0.47 | 0.36 ± 0.19 0.25–0.39 | 0.26 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kogan, Y.; Sabo, E.; Odeh, M. Diagnostic Value of C-Reactive Protein in Discrimination between Uncomplicated and Complicated Parapneumonic Effusion. Diagnostics 2020, 10, 829. https://doi.org/10.3390/diagnostics10100829
Kogan Y, Sabo E, Odeh M. Diagnostic Value of C-Reactive Protein in Discrimination between Uncomplicated and Complicated Parapneumonic Effusion. Diagnostics. 2020; 10(10):829. https://doi.org/10.3390/diagnostics10100829
Chicago/Turabian StyleKogan, Yana, Edmond Sabo, and Majed Odeh. 2020. "Diagnostic Value of C-Reactive Protein in Discrimination between Uncomplicated and Complicated Parapneumonic Effusion" Diagnostics 10, no. 10: 829. https://doi.org/10.3390/diagnostics10100829
APA StyleKogan, Y., Sabo, E., & Odeh, M. (2020). Diagnostic Value of C-Reactive Protein in Discrimination between Uncomplicated and Complicated Parapneumonic Effusion. Diagnostics, 10(10), 829. https://doi.org/10.3390/diagnostics10100829