Diagnosis of Hodgkin Lymphoma from Cell Block: A Reliable and Helpful Tool in “Selected” Diagnostic Practice

 ,
,  ,
,  , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
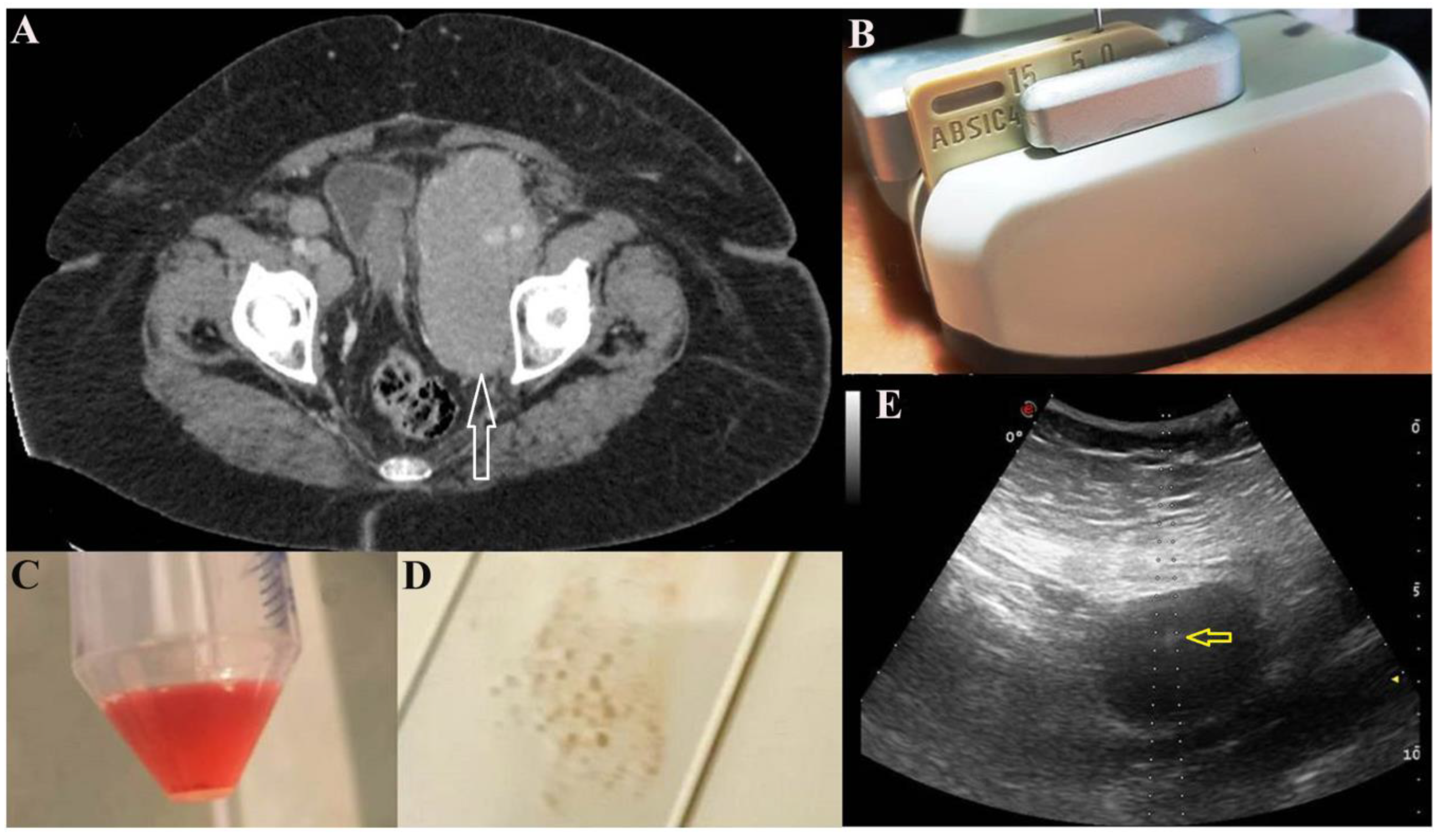
2.1. US-FNA Procedure
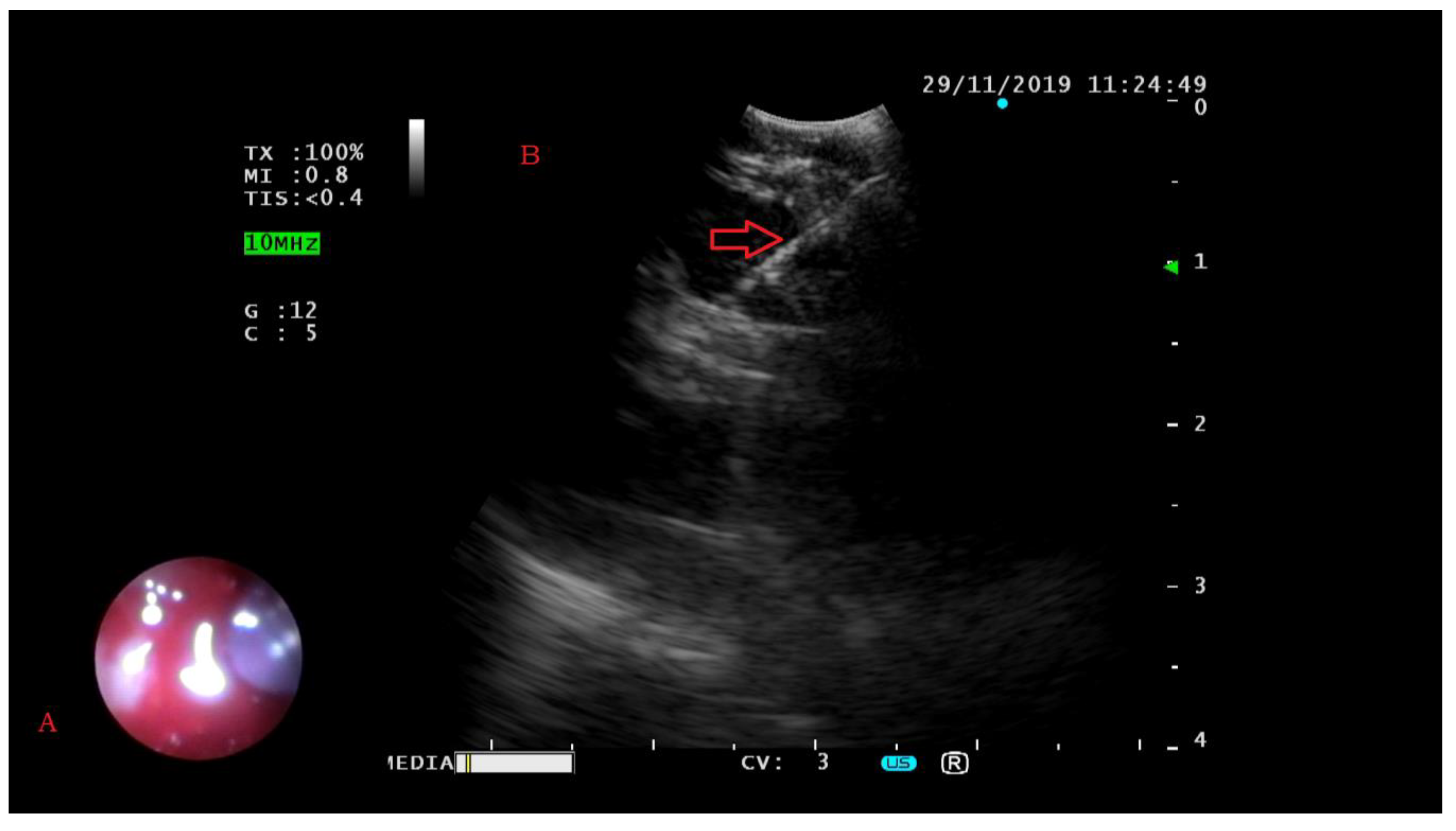
2.2. EBUS-FNA Procedure
2.3. Drainage Procedure
2.4. Complications of Procedures
2.5. CC Procedure
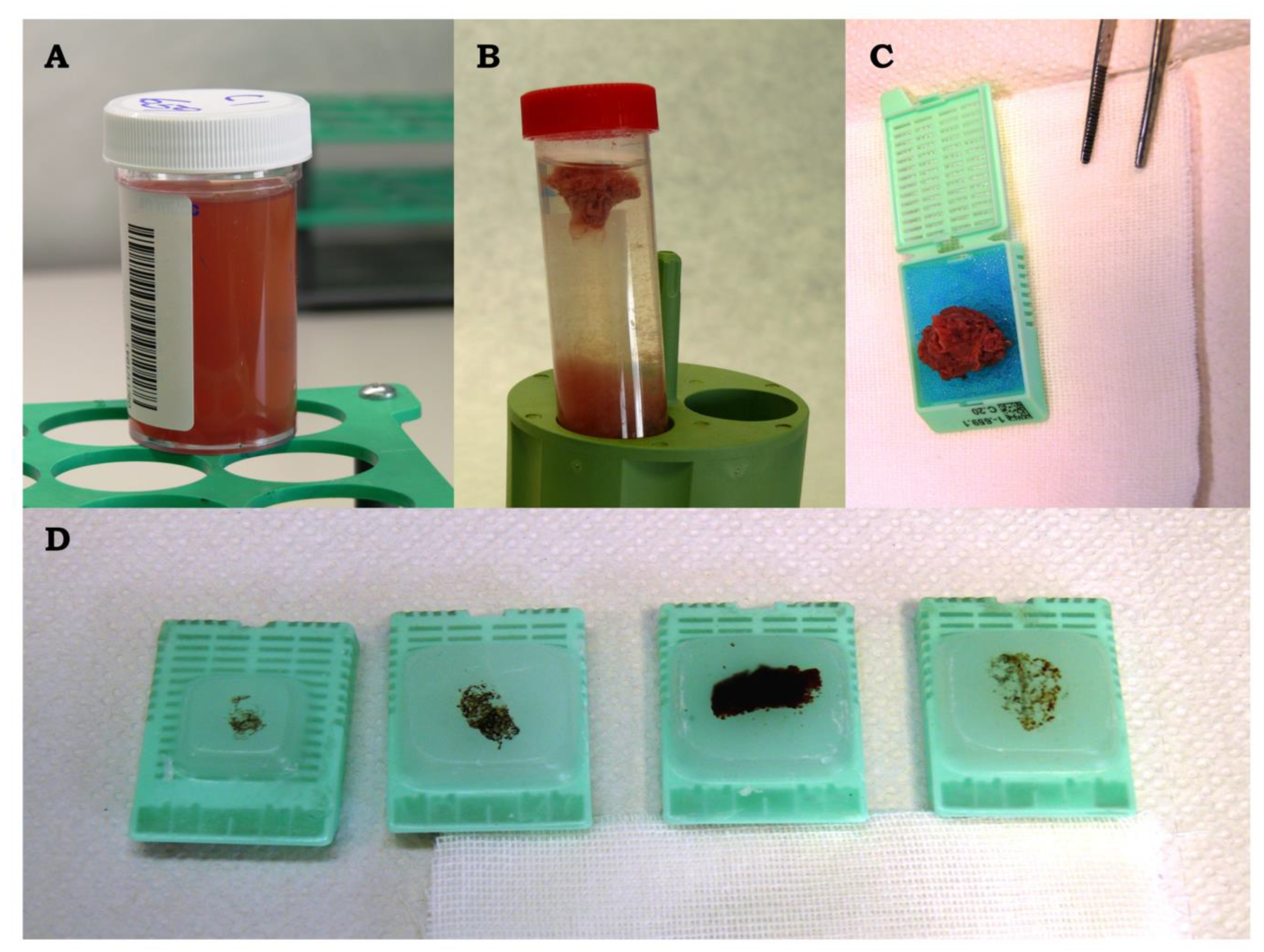
2.6. CB Procedure
2.7. Immunocytochemical Analysis
2.8. FISH Procedure
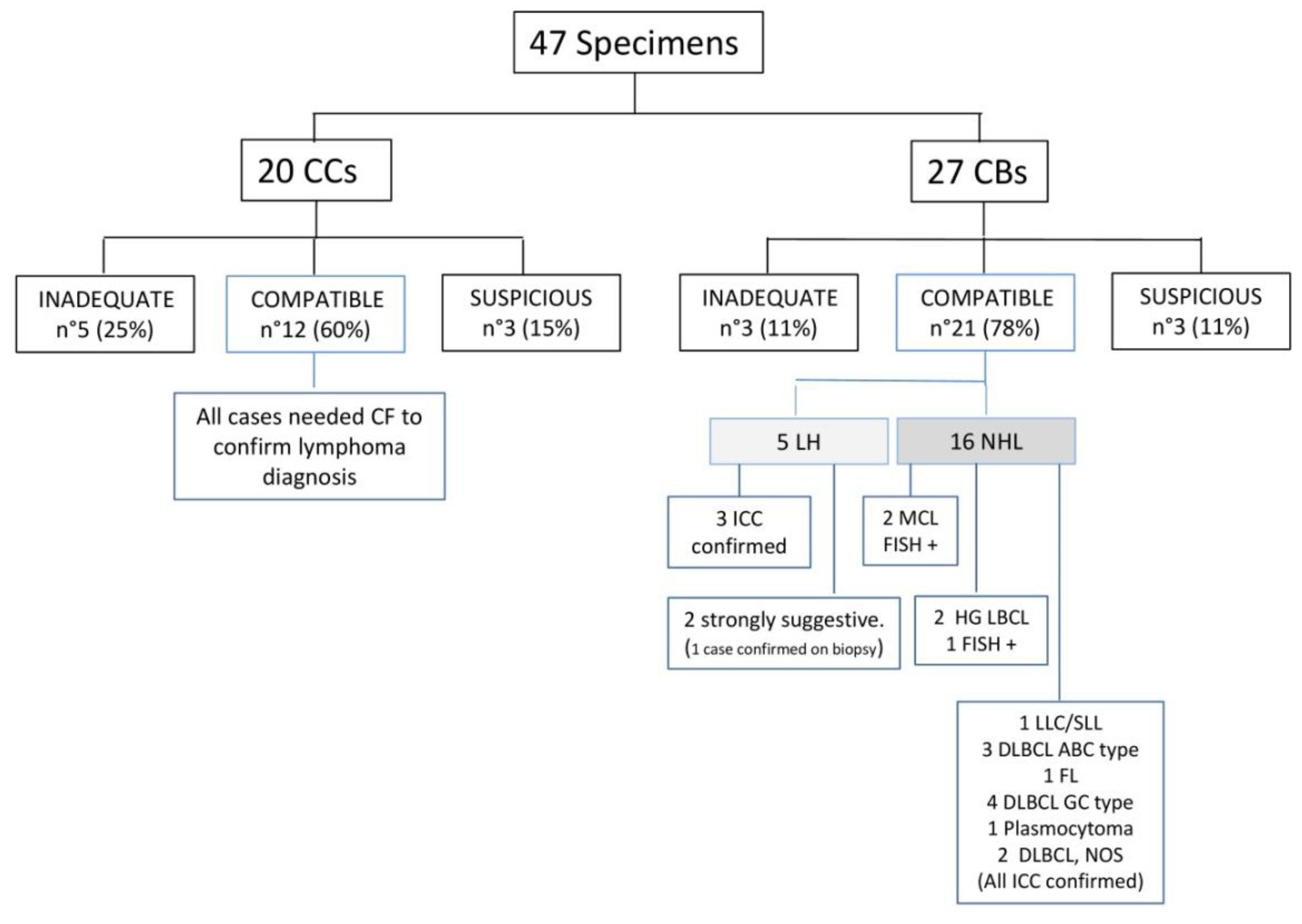
3. Results
3.1. Cytological Samples and Disease Location
3.2. Cytological Diagnosis and Ancillary Studies
3.3. Statistical Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Disclosure
Conflicts of Interest
References
- Yu, L.; Chen, K.; Xu, Y.; Wang, S.; Liu, Q.; Ye, Q.; Ye, T.; Sun, Y. The value of EUS in combination with cytological, flow cytometry, and gene rearrangement in the diagnosis of gastrointestinal lymphoma. Hematol. Oncol. 2017, 35, 303–309. [Google Scholar] [CrossRef] [PubMed]
- Jaffe, E.S.; Stein, H.T.; Swerdlow, S.H.C.E.; Campo, E.; Pileri, S.; Thiele, J.; Harris, N.L.; Wardiman, J.W. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues, Revised, 4th ed.; IARC: Lyon, France, 2017. [Google Scholar]
- Al-Haddad, M.; Savabi, M.S.; Sherman, S.; McHenry, L.; LeBlanc, J.; Cramer, H.; Emerson, R.; O’Neil, J.; Khashab, M.; DeWitt, J. Role of endoscopic ultrasound-guided fine-needle aspiration with flow cytometry to diagnose lymphoma: A single center experience. J. Gastroenterol. Hepatol. 2009, 24, 1826–1833. [Google Scholar] [CrossRef] [PubMed]
- Freedman, A.; Jacobsen, E. Follicular lymphoma: 2020 update on diagnosis and management. Am. J. Hematol. 2020, 95, 316–327. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Barta, S.K. Diffuse large B-cell lymphoma: 2019 update on diagnosis, risk stratification, and treatment. Am. J. Hematol. 2019, 94, 604–616. [Google Scholar] [CrossRef] [PubMed]
- Mehra, M.; Tamhane, A.; Eloubeidi, M.A. EUS-guided FNA combined with flow cytometry in the diagnoses of suspected or recurrent intrathoracic or retroperitoneal lymphoma. Gastrointest. Endosc. 2005, 62, 508–513. [Google Scholar] [CrossRef]
- Jin, M.; Wakely, P.E., Jr. Lymph node cytopathology: Essential ancillary studies as applied to lymphoproliferative neoplasms. Cancer Cytopathol. 2018, 126 (Suppl. 8), 615–626. [Google Scholar] [CrossRef]
- Ribeiro, A.; Pereira, D.; Escalón, M.P.; Goodman, M.; Byrne, G.E. EUS-guided biopsy for the diagnosis and classification of lymphoma. Gastrointest. Endosc. 2010, 71, 851–855. [Google Scholar] [CrossRef]
- Chen, L.; Zhang, J.S.; Liu, D.G.; Cui, D.; Meng, Z.L. An algorithmic approach to diagnose haematolymphoid neoplasms in effusion by combining morphology, immunohistochemistry and molecular cytogenetics. Cytopathology 2018, 29, 10–21. [Google Scholar] [CrossRef]
- Bode-Lesniewska, B. Flow Cytometry and Effusions in Lymphoproliferative Processes and Other Hematologic Neoplasias. Acta Cytol. 2016, 60, 354–364. [Google Scholar] [CrossRef]
- Rodriguez, E.F.; Pastorello, R.; Osmani, L.; Hopkins, M.; Kryatova, M.; Kawamoto, S.; Maleki, Z. Ultrasound-Guided Transthoracic Fine-Needle Aspiration: A Reliable Tool in Diagnosis and Molecular Profiling of Lung Masses. Acta Cytol. 2020, 64, 208–215. [Google Scholar] [CrossRef]
- Assawasaksakul, T.; Boonsarngsuk, V.; Incharoen, P. A comparative study of conventional cytology and cell block method in the diagnosis of pleural effusion. J. Thorac. Dis. 2017, 9, 3161–3167. [Google Scholar] [CrossRef] [PubMed]
- Shivakumarswamy, U.; Karigowdar, M.; Arakeri, S.; Yelikar, B. Diagnostic utility of the cell block method versus the conventional smear study in pleural fluid cytology. J. Cytol. 2012, 29, 11. [Google Scholar] [CrossRef] [PubMed]
- Sperandeo, M.; Dimitri, L.; Pirri, C.; Trovato, F.M.; Catalano, D.; Trovato, G.M. Advantages of Thoracic Ultrasound-Guided Fine-Needle Aspiration Biopsy in Lung Cancer and Mesothelioma. Chest 2014, 146, e178–e179. [Google Scholar] [CrossRef] [PubMed]
- Parente, P.; Zanelli, M.; Zizzo, M.; Carosi, I.; Di Candia, L.; Sperandeo, M.; Lacedonia, D.; Fesce, V.F.; Ascani, S.; Graziano, P. Primary pulmonary Hodgkin lymphoma presenting as multiple cystic lung lesions: Diagnostic usefulness of cell block. Cytopathology 2020, 31, 236–239. [Google Scholar] [CrossRef]
- Jaffe, E.S. Diagnosis and classification of lymphoma: Impact of technical advances. Semin Hematol. 2019, 56, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Sundling, K.E.; Cibas, E.S. Ancillary studies in pleural, pericardial, and peritoneal effusion cytology. Cancer Cytopathol. 2018, 126, 590–598. [Google Scholar] [CrossRef]
- Ansel, S.M. Hodgkin Lymphoma: Diagnosis and Treatment. Mayo Clin. Proc. 2015, 90, 1574–1583. [Google Scholar] [CrossRef]
- Ansell, S.M. Hodgkin lymphoma: A 2020 update on diagnosis, risk-stratification, and management. Am. J. Hematol. 2020, 95, 978–989. [Google Scholar] [CrossRef]
- Jin, M.; Wakely, P.E., Jr. FNA diagnosis of deep-seated lymphoma: An institutional experience. J. Am. Soc. Cytopathol. 2017, 6, 114–119. [Google Scholar] [CrossRef]
- Jing, X.; Li, Q.K.; Bedrossian, U.; Michael, C.W. Morphologic and Immunocytochemical Performances of Effusion Cell Blocks Prepared Using 3 Different Methods. Am. J. Clin. Pathol. 2013, 139, 177–182. [Google Scholar] [CrossRef]
- Jiménez-Heffernan, J.A.; Vicandi, B.; López-Ferrer, P.; Hardisson, D.; Viguer, J.M. Value of Fine Needle Aspiration Cytology in the Initial Diagnosis of Hodgkin’s Disease. Acta Cytol. 2001, 45, 300–306. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.; Dey, P.; Mitra, S.; Rajwanshi, A.; Nijhawan, R.; Srinivasan, R.; Gupta, N.; Das, A. Nodular sclerosis classical Hodgkin lymphoma grade 2: A diagnostic challenge to the cytopathologists. Cancer Cytopathol. 2017, 125, 104–113. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Gupta, S.; Long, S.R.; Natkunam, Y.; Kong, C.S.; Gupta, N.K.; Gratzinger, D. Role of FNA with core biopsy or cell block in patients with nodular lymphocyte-predominant Hodgkin lymphoma. Cancer Cytopathol. 2020, 128, 570–579. [Google Scholar] [CrossRef] [PubMed]
- Subhawong, A.P.; Ali, S.Z.; Tatsas, A.D. Nodular lymphocyte-predominant Hodgkin lymphoma. Cancer Cytopathol. 2012, 120, 254–260. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case Number | Sex | Age at Diagnosis | Procedure | Site | Method | Clinical Indications | Clinical Queries | Cytological Diagnosis | ICC | FISH |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | M | 75 | Drainage | PLE | CB | Pleural effusion | Carcinoma | LLC/SLL | Yes | |
| 2 | F | 19 | US-FNA | MM | CB | Follow-up in HL | Carcinoma | Strongly suggestive for HL | Yes | |
| 3 | M | 79 | US-FNA | LN | CB + Sm | Soft tissue mass | Lymphoma | DLBCL, ABC type | Yes | |
| 4 | M | 62 | US-FNA | ST | Sm | Follow-up in NHL | Lymphoma | Compatible with NHL B | Inadequate | |
| 5 | F | 78 | Drainage | PE | Sm | Retroperitoneal mass | Carcinoma | Compatible with NHL B | Inadequate | |
| 6 | M | 74 | US-FNA | SP | Sm | MD | Lymphoma | Compatible with NHL B | Inadequate | |
| 7 | M | 78 | Drainage | PLE | Cc | NHL | Lymphoma | Compatible with NHL B | Inadequate | |
| 8 | M | 45 | US-FNA | SP | Sm | Suspicious lymphoma | Lymphoma | Compatible with NHL B | Inadequate | |
| 9 | M | 33 | US-FNA | ST | Sm | MM | Lymphoma | Compatible with lymphoma | Inadequate | |
| 10 | M | 52 | US-FNA | SP | Sm | Suspicious HCL | Lymphoma | Compatible with NHL B | Inadequate | |
| 11 | F | 80 | US-FNA | SP | Sm | Splenic mass | Lymphoma | Compatible with lymphoma | Inadequate | |
| 12 | F | 29 | US-FNA | Lung | Sm | Lung consolidation | Lobar pneumonia | Compatible with lymphoma | Inadequate | |
| 13 | F | 89 | US-FNA | ST | Sm | Localized lymphadenopathy | Carcinoma | Compatible with NHL B | Inadequate | |
| 14 | F | 48 | Drainage | PLE | Cc | Follow-up in NHL | Lymphoma | Compatible with NHL T | Yes | |
| 15 | F | 55 | US-FNA | ST | Sm | Lymphadenomegaly | NQ | Inadequate | Inadequate | |
| 16 | F | 70 | US-FNA | LN | CB + Sm | Follow-up in NHL | Lymphoma | Suspicious for lymphoma | Yes | |
| 17 | F | 83 | US-FNA | MM | CB | Follow-up in NHL | Lymphoma | DLBCL, GC type | Yes | |
| 18 | M | 82 | US-FNA | LN | CB + Sm | Retroperitoneal mass | Lymphoma | NHL B, FL | Yes | |
| 19 | F | 68 | EBUS-FNA | MM | CB | Suspicious carcinoma | Carcinoma | HL | Yes | |
| 20 | M | 74 | US-FNA | ST | CB | Suspicious carcinoma | Carcinoma | MCL | Yes | Yes |
| 21 | M | 74 | Drainage | PLE | CB | Suspicious carcinoma | Carcinoma | DLBCL, ABC type | Yes | Yes |
| 22 | M | 74 | US-FNA | Liver | CB | Suspicious carcinoma | Carcinoma | DLBCL, ABC type | Yes | |
| 23 | F | 70 | US-FNA | ST | CB | Bone and pulmonary lesion | Carcinoma | Plasmocytoma | Yes | |
| 24 | F | 18 | US-FNA | Lung | CB | Cystic pulmonary lesion | TB | HL | Yes | |
| 25 | M | 41 | EBUS-FNA | MM | CB | Penile carcinoma and MM | Carcinoma | HL | Yes | |
| 26 | F | 65 | US-FNA | MM | CB | Mediastinic mass | Carcinoma | Suspicious for lymphoma | Inadequate | |
| 27 | M | 72 | US-FNA | MM | CB + Sm | Suspicious lymphoma | Lymphoma | DLBCL, ABC type | Yes | |
| 28 | M | 26 | US-FNA | LN | Sm | Lymphadenomegaly | Lymphoma | Suspicious for lymphoma | Inadequate | |
| 29 | F | 54 | US-FNA | LN | CB + Sm | Follow-up in NHL | Lymphoma | DLBCL, GC type | Yes | |
| 30 | M | 30 | US-FNA | MM | CB + Sm | Mediastinic mass | Thymoma/lymphoma | Strongly suggestive for HL | Yes | |
| 31 | M | 78 | Drainage | PE | Cc | Suspicious lymphoma | Lymphoma | Compatible with NHL | Inadequate | |
| 32 | M | 42 | US-FNA | Liver | CB + Sm | Suspicious lymphoma | Lymphoma | DLBCL, NOS | Yes | |
| 33 | F | 75 | Drainage | PE | CB + Cc | Peritoneal effusion | Lymphoma | DLBCL, NOS | Yes | Yes |
| 34 | F | 57 | US-FNA | LN | CB | Lymphadenomegaly | Carcinoma | DLBCL, GC type | Yes | |
| 35 | F | 88 | Drainage | PLE | Sm | Follow-up in HL | Lymphoma | Inadequate | Inadequate | |
| 36 | F | 77 | US-FNA | ST | CB | Abdominal mass | Lymphoma | DLBCL, GC type | Yes | |
| 37 | F | 93 | US-FNA | ST | CB + Sm | Soft tissue mass | Carcinoma | DLBCL, NOS | Yes | |
| 38 | M | 73 | EBUS-FNA | LN | CB | Pulmonary mass | Carcinoma | Suspicious for lymphoma | Inadequate | |
| 39 | M | 35 | US-FNA | ST | CB + Sm | Acute leukemia | Carcinoma | Inadequate | Inadequate | |
| 40 | F | 55 | US-FNA | MM | CB + Sm | Suspicious lymphoma | Lymphoma | Inadequate | Inadequate | |
| 41 | F | 55 | US-FNA | MM | Sm | Suspicious lymphoma | Lymphoma | Suspicious for lymphoma | Inadequate | |
| 42 | F | 67 | US-FNA | LN | Sm | Suspicious lymphoma | Lymphoma | Suspicious for lymphoma | Inadequate | |
| 43 | F | 40 | US-FNA | LN | Sm | Suspicious lymphoma | Lymphoma | Inadequate | Inadequate | |
| 44 | F | 48 | US-FNA | LN | Sm | Suspicious lymphoma | Lymphoma | Inadequate | Inadequate | |
| 45 | F | 76 | US-FNA | MM | CB + Sm | Suspicious lymphoma | Lymphoma | Inadequate | Inadequate | |
| 46 | M | 64 | US-FNA | LN | Sm | Suspicious lymphoma | Lymphoma | Inadequate | Inadequate | |
| 47 | M | 68 | US-FNA | ST | CB | Follow-up in NHL-mantle cell | Lymphoma | MCL | Yes | Yes |
| Results | CCs | CBs | p-Value | Test Used and Result | ||
|---|---|---|---|---|---|---|
| n = 20 | n = 27 | |||||
| n | % | n | % | |||
| Inadequate | 5 | 25 | 3 | 11 | p = 0.394 | df2 overall (Fisher Exact Test) |
| Compatibile | 12 | 60 | 21 | 78 | p = 0.187 | df1 Compatibile vs. Inadeguate&Suspicious (Pearson Chi-square Test) |
| Suspicious | 3 | 15 | 3 | 11 | p = 0.258 | df1 Inadeguate vs. Compatibile&Suspicious (Fisher Exact Test) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parente, P.; Covelli, C.; Zanelli, M.; Trombetta, D.; Carosi, I.; Carbonelli, C.; Sperandeo, M.; Mastracci, L.; Biancofiore, G.; Zizzo, M.; et al. Diagnosis of Hodgkin Lymphoma from Cell Block: A Reliable and Helpful Tool in “Selected” Diagnostic Practice. Diagnostics 2020, 10, 748. https://doi.org/10.3390/diagnostics10100748
Parente P, Covelli C, Zanelli M, Trombetta D, Carosi I, Carbonelli C, Sperandeo M, Mastracci L, Biancofiore G, Zizzo M, et al. Diagnosis of Hodgkin Lymphoma from Cell Block: A Reliable and Helpful Tool in “Selected” Diagnostic Practice. Diagnostics. 2020; 10(10):748. https://doi.org/10.3390/diagnostics10100748
Chicago/Turabian StyleParente, Paola, Claudia Covelli, Magda Zanelli, Domenico Trombetta, Illuminato Carosi, Cristiano Carbonelli, Marco Sperandeo, Luca Mastracci, Giovanni Biancofiore, Maurizio Zizzo, and et al. 2020. "Diagnosis of Hodgkin Lymphoma from Cell Block: A Reliable and Helpful Tool in “Selected” Diagnostic Practice" Diagnostics 10, no. 10: 748. https://doi.org/10.3390/diagnostics10100748
APA StyleParente, P., Covelli, C., Zanelli, M., Trombetta, D., Carosi, I., Carbonelli, C., Sperandeo, M., Mastracci, L., Biancofiore, G., Zizzo, M., Taurchini, M., Ascani, S., & Graziano, P. (2020). Diagnosis of Hodgkin Lymphoma from Cell Block: A Reliable and Helpful Tool in “Selected” Diagnostic Practice. Diagnostics, 10(10), 748. https://doi.org/10.3390/diagnostics10100748