
Right Colectomy with Complete Mesocolic Excision and Intracorporeal Anastomosis: A Monocentric, Single-Surgeon Comparison of Dexter, DaVinci and Laparoscopic Approaches

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Patients
2.2. Variables and Definitions
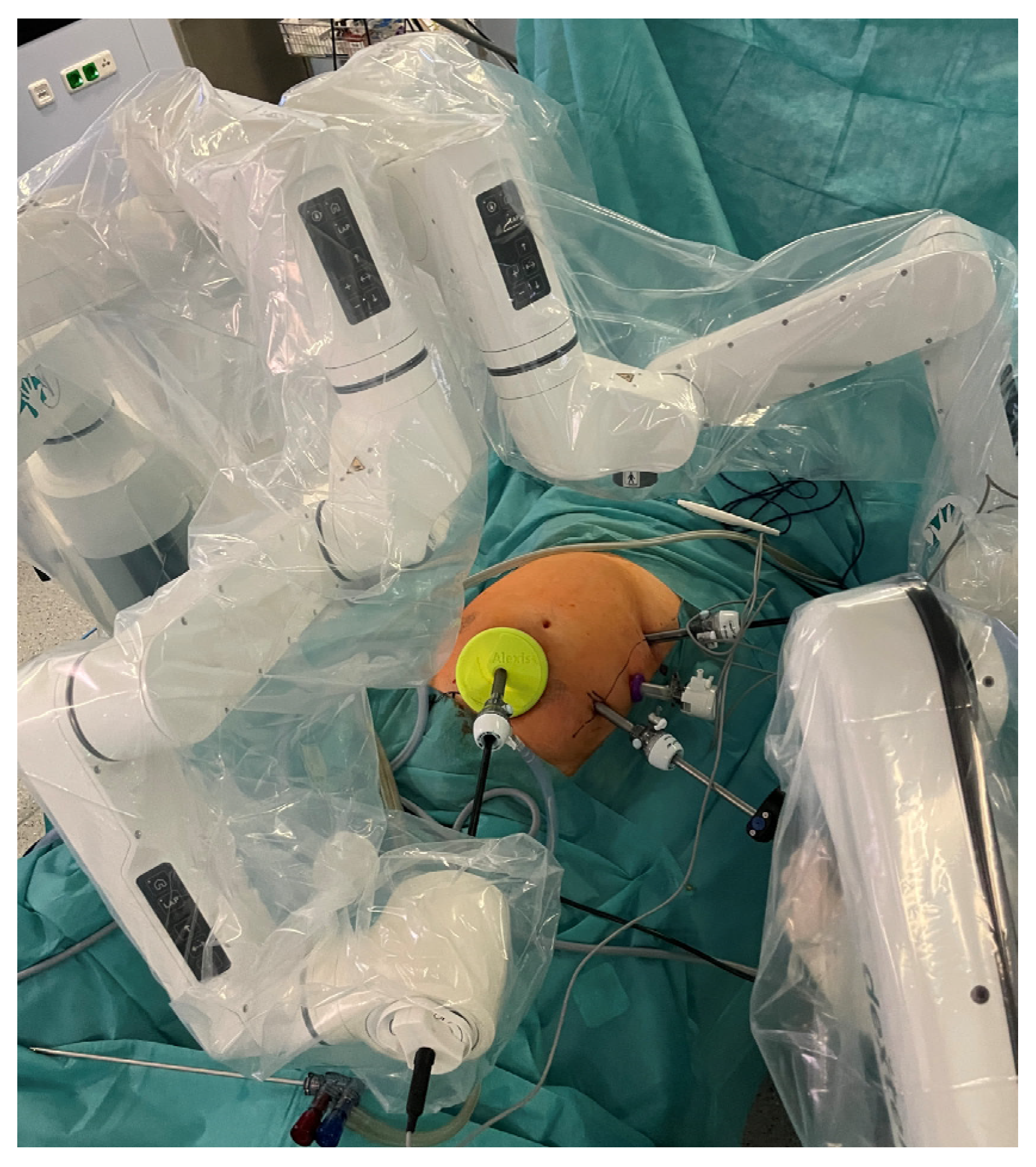
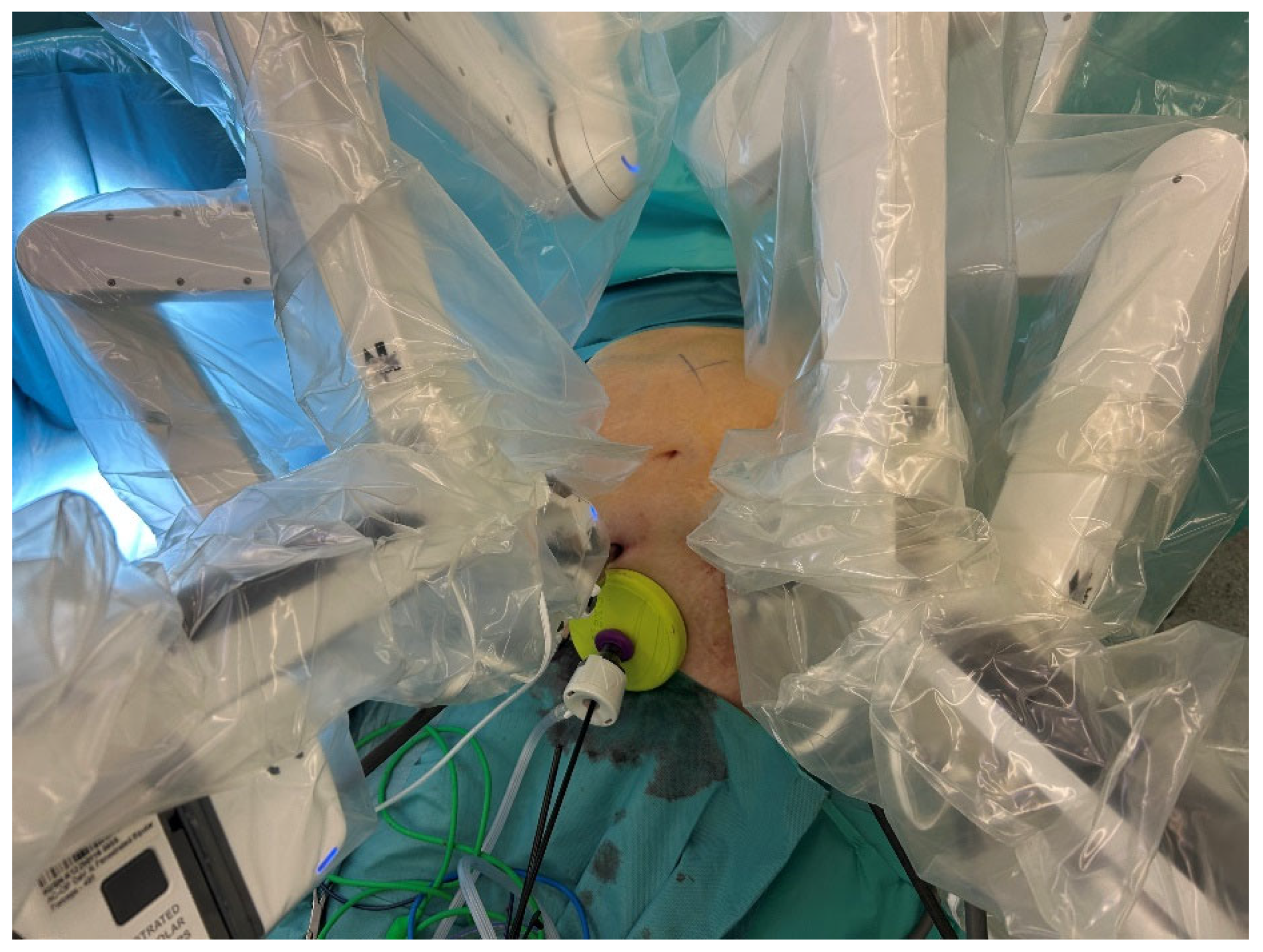
2.3. Surgical Technique
2.4. Statistical Analysis
3. Results

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| DXRC | DVRC | LRC | p-Value | |
|---|---|---|---|---|
| N | 25 | 25 | 25 | |
| Age | 67.1 ± 13.3 | 67.0 ± 14.7 | 68.1 ± 11.5 | 0.95 |
| Female gender | 13 (52.0) | 9 (36.0) | 13 (52.0) | 0.42 |
| BMI | 26.3 ± 4.3 | 27.1 ± 4.2 | 25.3 ± 4.2 | 0.34 |
| Pre-existing diseases | ||||
| Cardiovascular | 8 (32) | 9 (36) | 7 (28) | 0.83 |
| Arterial hypertension | 11 (44) | 6 (24) | 14 (56) | 0.07 |
| Pulmonary | 0 | 3 (12) | 2 (8) | 0.22 |
| Metabolic | 4 (16) | 5 (20) | 5 (20) | 0.92 |
| Renal | 1 (4) | 0 | 1 (4) | 0.60 |
| ASA ≥ 3 | 6 (24.0) | 7 (28.0) | 3 (12.0) | 0.36 |
| Previous abdominal surgery | 8 (32) | 11 (44) | 7 (28) | 0.47 |
| Tumor stage (UICC) | ||||
| HGIEN | 3 (12) | 2 (8) | 1 (4) | |
| I | 5 (20) | 4 (16) | 4 (16) | |
| II | 8 (32) | 9 (36) | 12 (48) | |
| III | 5 (20) | 7 (28) | 4 (16) | |
| IV | 4 (16) | 3 (12) | 4 (16) | 0.93 |
| MMR deficiency | 10 (40) | 8 (32) | 6 (24) | 0.46 |
| DXRC | DVRC | LRC | p-Value | |
|---|---|---|---|---|
| Type of anastomosis | ||||
| Extracorporeal hand-sewn | 0 | 1 (4) | 11 (44) | |
| Intracorporeal stapled | 20 (80) | 18 (72) | 14 (56) | |
| Intracorporeal hand-sewn | 5 (20) | 6 (24) | 0 | <0.01 |
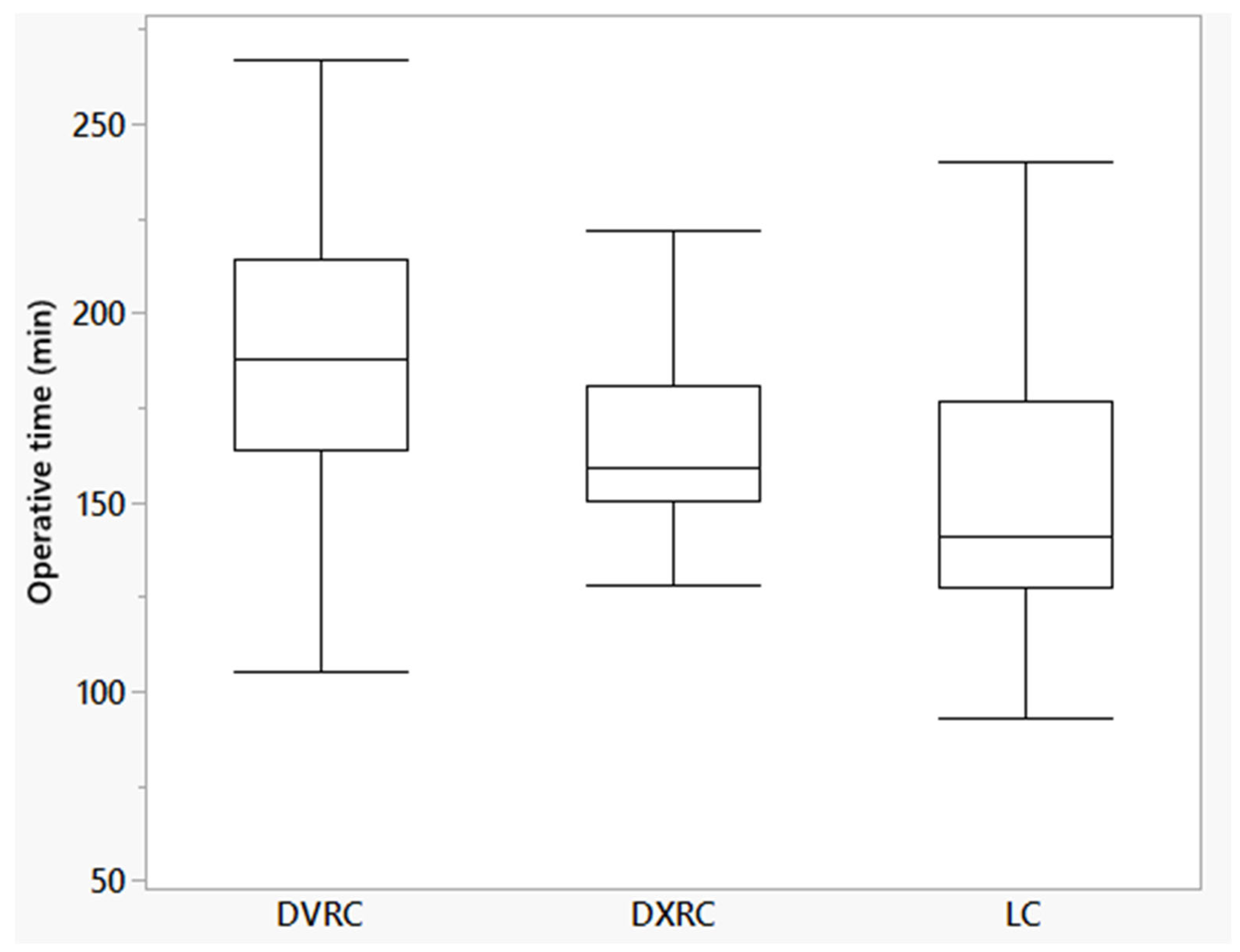
| Operative time (min [95% confidence interval]) | 164.8 (151.7–178.0) | 190.5 (177.3–203.7) | 152.6 (139.4–165-7) | <0.01 |
| Initial docking (min) | 5.6 ± 2.5 | 9.6 ± 3.4 | n/a | <0.01 |
| TAP-block | 13 (52.0) | 7 (28.0) | 5 (20.0) | 0.04 |
| Height of staples (mm) | ||||
| 1.5–2.5 (blue) | 22 (88) | 11 (44) | 18 (72) | |
| 3.0–4.0 (purple) | 3 (12) | 10 (40) | 7 (28) | |
| 1.8–3.0 (gold) | 0 | 1 (4) | 0 | |
| 4.3 (green) | 0 | 3 (12) | 0 | 0.02 |
| Conversion to open | 0 | 0 | 1 (4) | 0.88 |
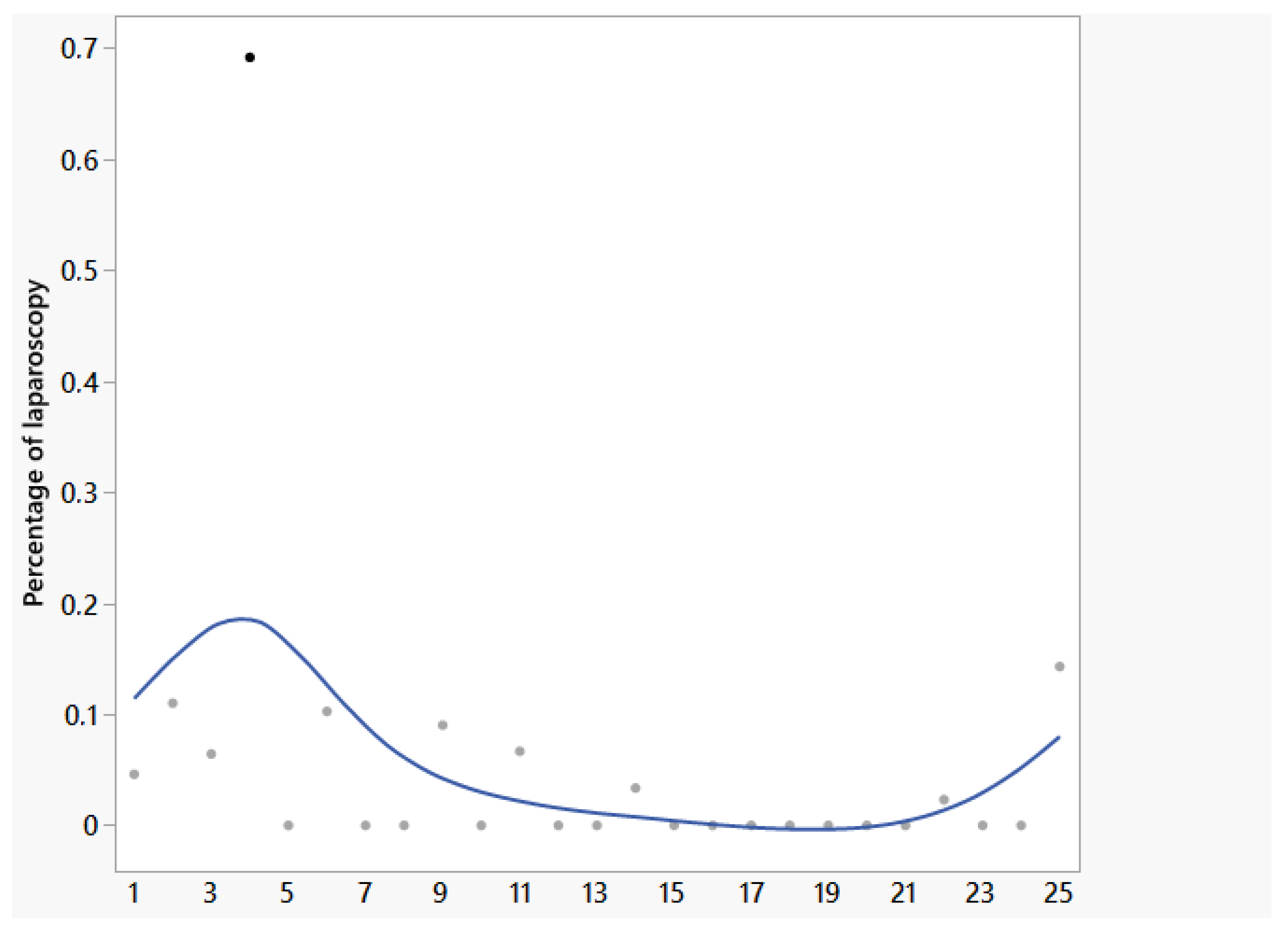
| Percentage of laparoscopy (%) | 0 (0–69) | 0 | 100 | - |
| Harvested lymph nodes | 22 (10–60) | 28 (12–46) | 26 (10–47) | 0.18 |
| CME fulfilled | 24 (96) | 22 (88) | 22 (88) | 0.53 |
| Pathological classification Benz-type 0 if CME fulfilled | 24 (100) | 20 (90.9) | 21 (95.5) | 0.32 |
| Intra-abdominal drainage | 1 (4) | 16 (64) | 6 (24) | <0.01 |
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ASA | American Society of Anesthesiologists Physical Status System |
| BMI | Body Mass Index |
| CD | Clavien–Dindo Classification |
| CME | Complete mesocolic excision |
| HGIEN | High-grade intraepithelial neoplasia |
| MMR | Mismatch repair |
| UICC | Union Internationale Contre le Cancer |
References
- Alkatout, I.; Mechler, U.; Mettler, L.; Pape, J.; Maass, N.; Biebl, M.; Gitas, G.; Laganà, A.S.; Freytag, D. The Development of Laparoscopy-A Historical Overview. Front. Surg. 2021, 8, 799442. [Google Scholar] [CrossRef]
- Kelley, W.E. The evolution of laparoscopy and the revolution in surgery in the decade of the 1990s. J. Soc. Laparoendosc. Surg. 2008, 12, 351–357. [Google Scholar]
- Buunen, M.; Veldkamp, R.; Hop, W.C.J.; Kuhry, E.; Jeekel, J.; Haglind, E.; Påhlman, L.; Cuesta, M.A.; Msika, S.; Morino, M.; et al. Survival after laparoscopic surgery versus open surgery for colon cancer: Long-term outcome of a randomised clinical trial. Lancet Oncol. 2009, 10, 44–52. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, R.H.; Francis, E.A.; Wharton, R.; Blazeby, J.M.; Quirke, P.; West, N.P.; Dutton, S.J. Multicenter randomized controlled trial of conventional versus laparoscopic surgery for colorectal cancer within an enhanced recovery programme: EnROL. J. Clin. Oncol. 2014, 32, 1804–1811. [Google Scholar] [CrossRef] [PubMed]
- Jayne, D.G.; Guillou, P.J.; Thorpe, H.; Quirke, P.; Copeland, J.; Smith, A.M.H.; Heath, R.M.; Brown, J.M. Randomized trial of laparoscopic-assisted resection of colorectal carcinoma: 3-year results of the UK MRC CLASICC Trial Group. J. Clin. Oncol. 2007, 25, 3061–3068. [Google Scholar] [CrossRef] [PubMed]
- Dohrn, N.; Klein, M.F.; Gögenur, I. Robotic versus laparoscopic right colectomy for colon cancer: A nationwide cohort study. Int. J. Colorectal Dis. 2021, 36, 2147–2158. [Google Scholar] [CrossRef]
- Miller, P.E.; Dao, H.; Paluvoi, N.; Bailey, M.; Margolin, D.; Shah, N.; Vargas, H.D. Comparison of 30-Day Postoperative Outcomes after Laparoscopic vs Robotic Colectomy. J. Am. Coll. Surg. 2016, 223, 369–373. [Google Scholar] [CrossRef]
- Clarke, E.M.; Rahme, J.; Larach, T.; Rajkomar, A.; Jain, A.; Hiscock, R.; Warrier, S.; Smart, P. Robotic versus laparoscopic right hemicolectomy: A retrospective cohort study of the Binational Colorectal Cancer Database. J. Robotic Surg. 2022, 16, 927–933. [Google Scholar] [CrossRef]
- Aiolfi, A.; Bona, D.; Rausa, E.; Manara, M.; Biondi, A.; Basile, F.; Campanelli, G.; Kelly, M.E.; Bonitta, G.; Bonavina, L. Effect of complete mesocolic excision (cme) on long-term survival after right colectomy for cancer: Multivariate meta-analysis and restricted mean survival time estimation. Langenbecks Arch. Surg. 2024, 409, 80. [Google Scholar] [CrossRef]
- Creavin, B.; Balasubramanian, I.; Common, M.; McCarrick, C.; El Masry, S.; Carton, E.; Faul, E. Intracorporeal vs extracorporeal anastomosis following neoplastic right hemicolectomy resection: A systematic review and meta-analysis of randomized control trials. Int. J. Colorectal Dis. 2021, 36, 645–656. [Google Scholar] [CrossRef]
- Brown, R.F.; Cleary, R.K. Intracorporeal anastomosis versus extracorporeal anastomosis for minimally invasive colectomy. J. Gastrointest. Oncol. 2020, 11, 500–507. [Google Scholar] [CrossRef] [PubMed]
- Lee, L.; Abou-Khalil, M.; Liberman, S.; Boutros, M.; Fried, G.M.; Feldman, L.S. Incidence of incisional hernia in the specimen extraction site for laparoscopic colorectal surgery: Systematic review and meta-analysis. Surg. Endosc. 2017, 31, 5083–5093. [Google Scholar] [CrossRef] [PubMed]
- Catanzarite, T.; Tan-Kim, J.; Whitcomb, E.L.; Menefee, S. Ergonomics in Surgery: A Review. Female Pelvic Med. Reconstr. Surg. 2018, 24, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Di Lascia, A.; Tartaglia, N.; Petruzzelli, F.; Pacilli, M.; Maddalena, F.; Fersini, A.; Pavone, G.; Vovola, F.; Ambrosi, A. Right hemicolectomy: Laparoscopic versus robotic approach. Ann. Ital. Chir. 2020, 91, 478–485. [Google Scholar]
- Yuval, J.B.; Thompson, H.M.; Verheij, F.S.; Fiasconaro, M.; Patil, S.; Widmar, M.; Wei, I.H.; Pappou, E.P.; Smith, J.J.; Nash, G.M.; et al. Comparison of Robotic, Laparoscopic, and Open Resections of Nonmetastatic Colon Cancer. Dis. Colon Rectum 2023, 66, 1347–1358. [Google Scholar] [CrossRef]
- Meyer, J.; Meyer, E.; Meurette, G.; Liot, E.; Toso, C.; Ris, F. Robotic versus laparoscopic right hemicolectomy: A systematic review of the evidence. J. Robot. Surg. 2024, 18, 116. [Google Scholar] [CrossRef]
- Marchegiani, F.; Siragusa, L.; Zadoroznyj, A.; Laterza, V.; Mangana, O.; Schena, C.; Ammendola, M.; Memeo, R.; Bianchi, P.; Spinoglio, G.; et al. New Robotic Platforms in General Surgery: What’s the Current Clinical Scenario? Medicina 2023, 59, 1264. [Google Scholar] [CrossRef]
- Hahnloser, D.; Rrupa, D.; Grass, F. Feasibility of on-demand robotics in colorectal surgery: First cases. Surg. Endosc. 2023, 37, 8594–8600. [Google Scholar] [CrossRef]
- Thillou, D.; Robin, H.; Ricolleau, C.; Benali, N.A.; Forgues, A.; Emeriau, D.; Mignot, H.; Hugues, G. Robot-assisted Radical Prostatectomy with the Dexter Robotic System: Initial Experience and Insights into On-demand Robotics. Eur. Urol. 2024, 85, 185–189. [Google Scholar] [CrossRef]
- Böhlen, D.; Gerber, R. First Ever Radical Prostatectomy Performed with the New Dexter Robotic System™. Eur. Urol. 2023, 83, 479–480. [Google Scholar] [CrossRef]
- Alkatout, I.; O’Sullivan, O.; Peters, G.; Maass, N. Expanding Robotic-Assisted Surgery in Gynecology Using the Potential of an Advanced Robotic System. Medicina 2024, 60, 53. [Google Scholar] [CrossRef]
- Alkatout, I.; Becker, T.; Nuhn, P.; Pochhammer, J.; Peters, G.; Donald, K.M.; Mettler, L.; Ackermann, J. The first robotic-assisted hysterectomy below the bikini line with the Dexter robotic system™. Facts Views Vis. ObGyn 2024, 16, 87–91. [Google Scholar] [CrossRef]
- Mignot, H.; Diack, B.; Capitaine, J.; Emeriau, D. Retrospective evaluation of a single surgeon’s experience in robot-assisted inguinal repair with the Dexter System™ during the learning curve. Int. J. Abdom. Wall Hernia Surg. 2024, 7, 75–82. [Google Scholar] [CrossRef]
- Gantner, L.; Mignot, H.; Pochhammer, J.; Grieder, F.; Breitenstein, S. Robotic minimally invasive inguinal hernia repair with the Dexter robotic system™: A prospective multicenter clinical investigation. Surg. Endosc. 2024, 38, 7647–7655. [Google Scholar] [CrossRef] [PubMed]
- Conrad, P.V.; Mehdorn, A.-S.; Alkatout, I.; Becker, T.; Beckmann, J.H.; Pochhammer, J. The Combination of Laparoscopic and Robotic Surgery: First Experience with the Dexter Robotic System™ in Visceral Surgery. Life 2024, 14, 874. [Google Scholar] [CrossRef] [PubMed]
- Strey, C.W.; Wullstein, C.; Adamina, M.; Agha, A.; Aselmann, H.; Becker, T.; Grützmann, R.; Kneist, W.; Maak, M.; Mann, B.; et al. Laparoscopic right hemicolectomy with CME: Standardization using the “critical view” concept. Surg. Endosc. 2018, 32, 5021–5030. [Google Scholar] [CrossRef] [PubMed]
- Dindo, D.; Demartines, N.; Clavien, P.-A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Horan, T.C.; Gaynes, R.P.; Martone, W.J.; Jarvis, W.R.; Emori, T.G. CDC definitions of nosocomial surgical site infections, 1992: A modification of CDC definitions of surgical wound infections. Infect. Control Hosp. Epidemiol. 1992, 13, 606–608. [Google Scholar] [CrossRef]
- Benz, S. Adoption of standardized approach to right hemicolectomy with complete mesocolic excision using the critical view concept and open-book model for robotic surgery—A video vignette. Colorectal Dis. 2021, 23, 2216–2217. [Google Scholar] [CrossRef]
- Benz, S.; Tannapfel, A.; Tam, Y.; Grünenwald, A.; Vollmer, S.; Stricker, I. Proposal of a new classification system for complete mesocolic excison in right-sided colon cancer. Tech. Coloproctol. 2019, 23, 251–257. [Google Scholar] [CrossRef]
- de Lange, G.; Davies, J.; Toso, C.; Meurette, G.; Ris, F.; Meyer, J. Complete mesocolic excision for right hemicolectomy: An updated systematic review and meta-analysis. Tech. Coloproctol. 2023, 27, 979–993. [Google Scholar] [CrossRef]
- Ahmad, A.; Ahmad, Z.F.; Carleton, J.D.; Agarwala, A. Robotic surgery: Current perceptions and the clinical evidence. Surg. Endosc. 2017, 31, 255–263. [Google Scholar] [CrossRef] [PubMed]
- Tian, Y.; Xiong, D.; Xu, M.; Fan, Q.; Zheng, H.; Shen, H.; Huang, B.; Wang, L.; Li, C.; Zhang, A.; et al. Robotic versus laparoscopic right hemicolectomy with complete mesocolic excision: A retrospective multicenter study with propensity score matching. Front. Oncol. 2023, 13, 1187476. [Google Scholar] [CrossRef] [PubMed]
- Merola, G.; Sciuto, A.; Pirozzi, F.; Andreuccetti, J.; Pignata, G.; Corcione, F.; Milone, M.; de Palma, G.D.; Castaldo, R.; Pecchia, L.; et al. Is robotic right colectomy economically sustainable? a multicentre retrospective comparative study and cost analysis. Surg. Endosc. 2020, 34, 4041–4047. [Google Scholar] [CrossRef] [PubMed]
- Negrut, R.L.; Cote, A.; Caus, V.A.; Maghiar, A.M. Systematic Review and Meta-Analysis of Laparoscopic versus Robotic-Assisted Surgery for Colon Cancer: Efficacy, Safety, and Outcomes-A Focus on Studies from 2020-2024. Cancers 2024, 16, 1552. [Google Scholar] [CrossRef]
- Kim, H.S.; Noh, G.T.; Chung, S.S.; Lee, R.-A. Long-term oncological outcomes of robotic versus laparoscopic approaches for right colon cancer: A systematic review and meta-analysis. Tech. Coloproctol. 2023, 27, 1183–1189. [Google Scholar] [CrossRef]
- Grass, F.; Hahnloser, D. On-demand robotics-The best of both worlds for robotic-assisted laparoscopic surgery. Surgery 2024, 176, 1534–1537. [Google Scholar] [CrossRef]
- Post, S.; Vilz, T. S3-Leitlinie “Perioperatives Management bei gastrointestinalen Tumoren (POMGAT)”. Chirurgie 2023, 94, 468. [Google Scholar] [CrossRef]
| DXRC | DVRC | LRC | p-Value | |
|---|---|---|---|---|
| Length of stay | 4 (3–10) | 4 (3–48) | 5 (2–35) | 0.14 |
| Complications within 30 days | ||||
| Acute pancreatitis (CD II) | 0 | 0 | 1 (4) | |
| Intraluminal bleeding | 0 | 1 (4) | 0 | |
| Colonoscopy (IIIa) | 0 | |||
| Intraabdominal bleeding | 0 | 1 (4) | ||
| Re-laparoscopy (CD IIIb) | ||||
| Anastomotic leakage (CD IIIb) | 1 (4) | 1 (4) | 2 (8) | |
| Mortality due to cardiac arrest (CD V) | 1 (4) | 0 | 0 | |
| Surgical site infections | 1 (4) | 0 | 2 (8) | 0.35 |
| Follow-up | 8 (1–24) | 17 (1–51) | 19 (1–56) | <0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pochhammer, J.; Franke, F.; Martin, M.; Beckmann, J.H.; Osmonov, D.; Alkatout, I.; Becker, T. Right Colectomy with Complete Mesocolic Excision and Intracorporeal Anastomosis: A Monocentric, Single-Surgeon Comparison of Dexter, DaVinci and Laparoscopic Approaches. Life 2025, 15, 1122. https://doi.org/10.3390/life15071122
Pochhammer J, Franke F, Martin M, Beckmann JH, Osmonov D, Alkatout I, Becker T. Right Colectomy with Complete Mesocolic Excision and Intracorporeal Anastomosis: A Monocentric, Single-Surgeon Comparison of Dexter, DaVinci and Laparoscopic Approaches. Life. 2025; 15(7):1122. https://doi.org/10.3390/life15071122
Chicago/Turabian StylePochhammer, Julius, Frederike Franke, Matthias Martin, Jan Henrik Beckmann, Daniar Osmonov, Ibrahim Alkatout, and Thomas Becker. 2025. "Right Colectomy with Complete Mesocolic Excision and Intracorporeal Anastomosis: A Monocentric, Single-Surgeon Comparison of Dexter, DaVinci and Laparoscopic Approaches" Life 15, no. 7: 1122. https://doi.org/10.3390/life15071122
APA StylePochhammer, J., Franke, F., Martin, M., Beckmann, J. H., Osmonov, D., Alkatout, I., & Becker, T. (2025). Right Colectomy with Complete Mesocolic Excision and Intracorporeal Anastomosis: A Monocentric, Single-Surgeon Comparison of Dexter, DaVinci and Laparoscopic Approaches. Life, 15(7), 1122. https://doi.org/10.3390/life15071122