
The Impact of Biodex Balance on Improving Coordination and Static Balance in Patients with Diabetic Peripheral Neuropathy

 ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Intervention Protocol
2.4. Outcome Measures
- −
- BBS Tests: stability index (measuring postural sway in degrees), sensory integration tests (assessing balance with eyes open/closed), and weight distribution analysis;
- −
- Clinical Balance Tests: unstable surface balance test (eyes open/closed), Timed Up and Go Test, and Functional Reach Test;
- −
- Statistical Analysis: descriptive statistics (mean, standard deviation), Shapiro–Wilk normality test, Levene’s test for homogeneity of variances, paired t-tests/Welch’s t-tests for pre- and post-intervention comparisons, and effect size (Cohen’s d) to assess clinical significance.
2.5. Statistical Analysis
- Parametric tests: Independent samples t-test (Student or Welch) for between-group comparisons.
- Nonparametric alternatives were applied where assumptions were violated.
- Effect sizes (Cohen’s d) were reported to assess the magnitude of intervention effects (interpreted as small = 0.2, medium = 0.5, large > 0.8).
3. Results
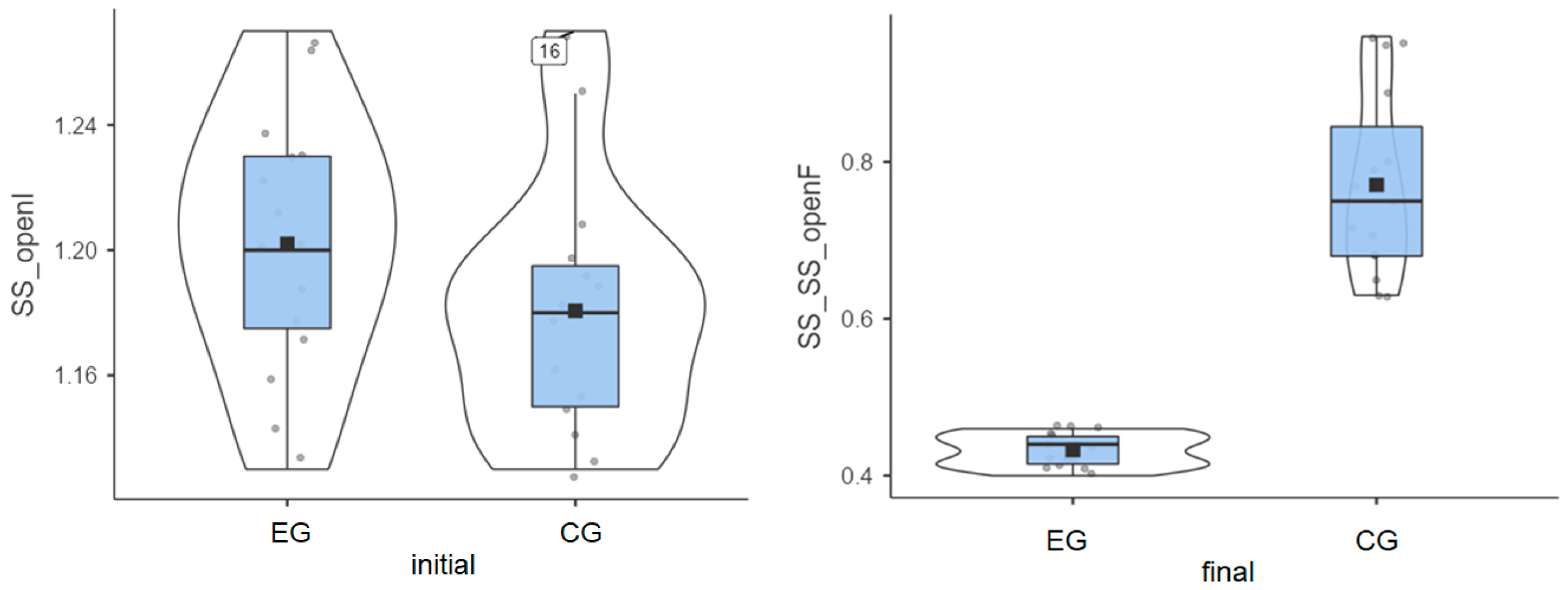
3.1. Stable Surface—Eyes Open
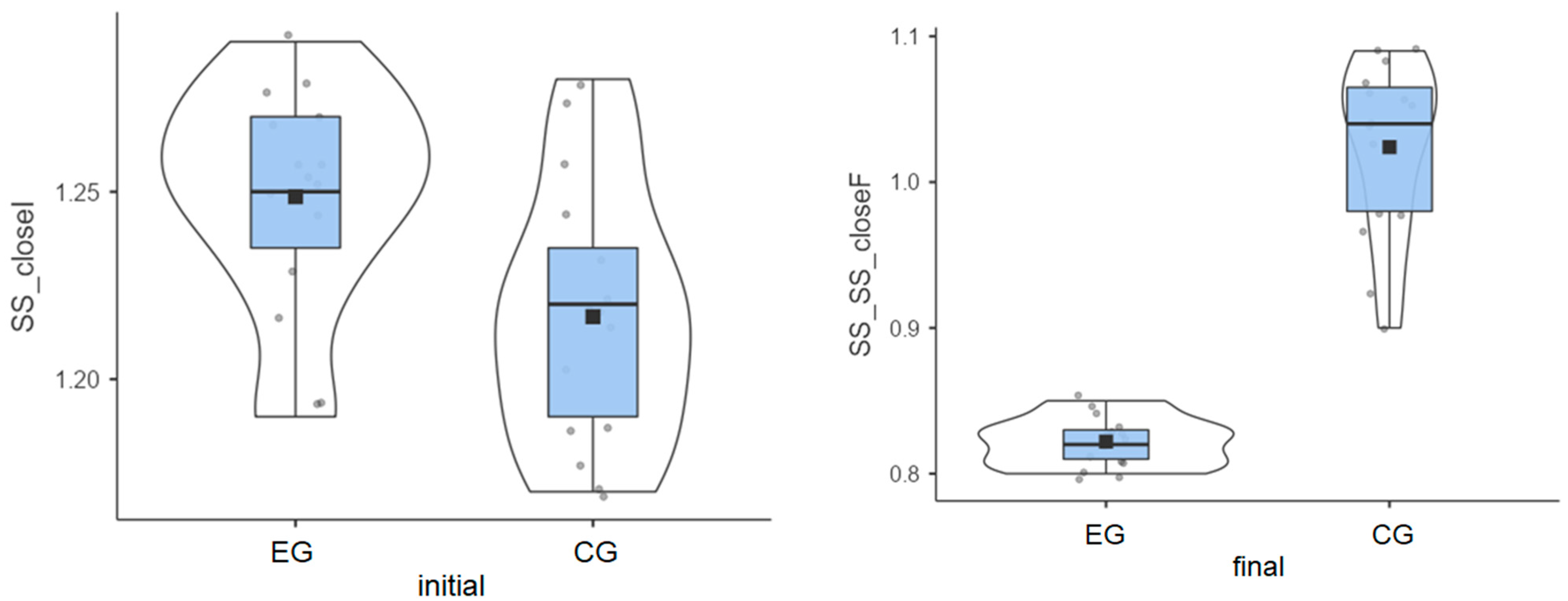
3.2. Stable Surface—Eyes Closed
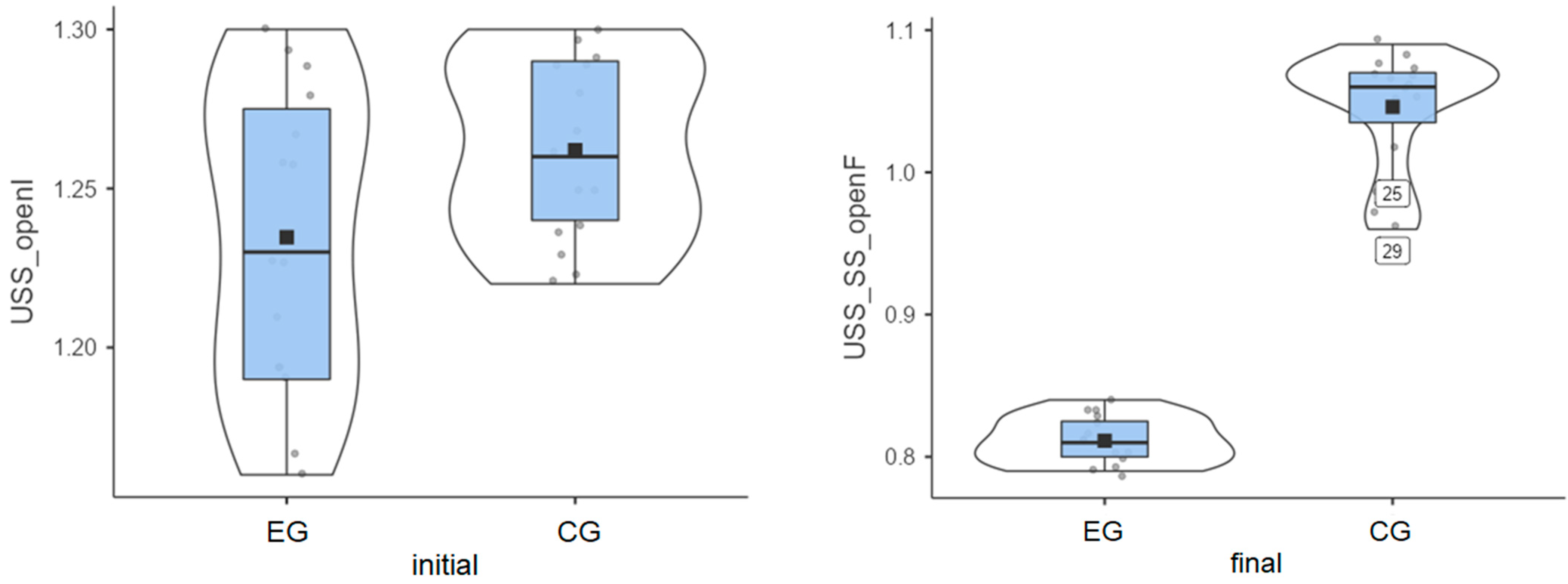
3.3. Unstable Surface—Eyes Open
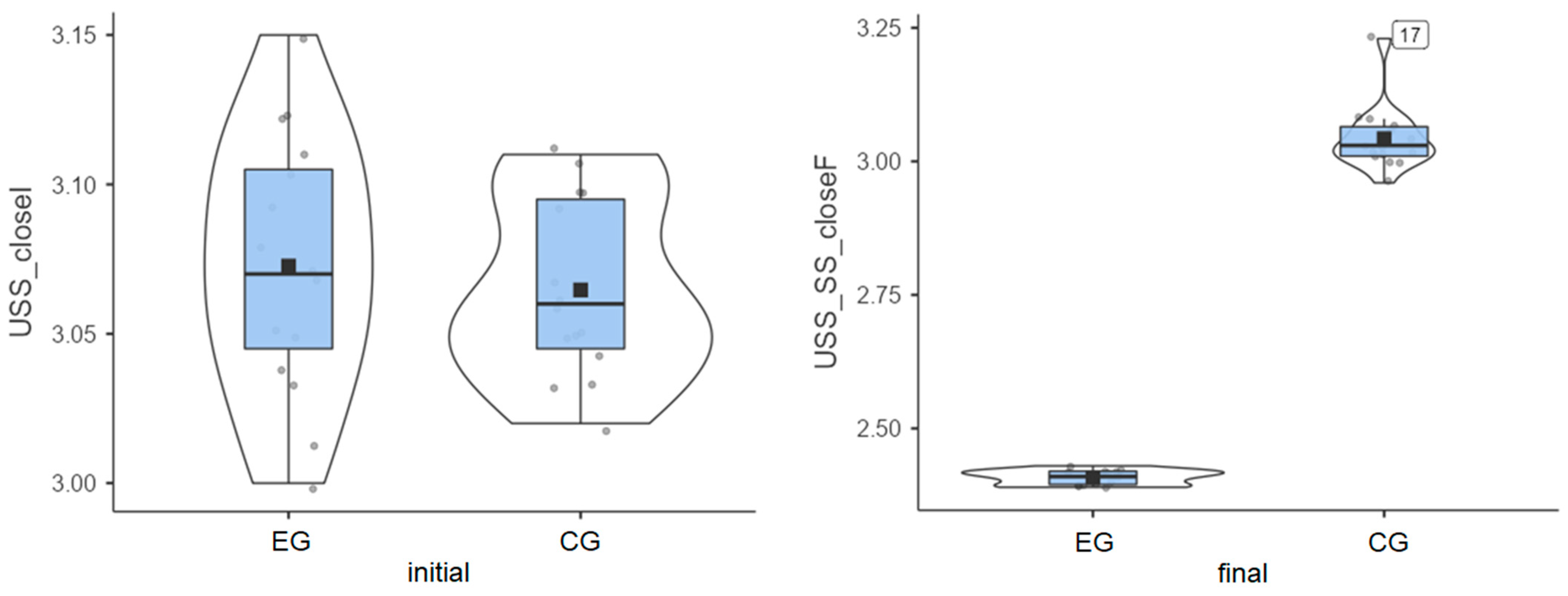
3.4. Unstable Surface—Eyes Closed (Most Challenging)
3.5. Independent Samples t-Test Results
- Age (p = 0.604): p > 0.05, so there is no significant age difference between groups, and Cohen’s d = 0.192, indicating a small effect size.
- Stable Surface (SS)—Eyes Open Initial (p = 0.166): p > 0.05, so balance scores before training were similar, showing no significant difference. Cohen’s d = 0.52, indicating a medium effect size.
- Stable Surface—Eyes Open Final (p < 0.001): p < 0.001, meaning that the experimental group showed much greater improvement, as the difference between groups is significant. Cohen’s d = −4.009, indicating a very large effect size.
- Stable Surface—Eyes Closed Initial (p = 0.012): p < 0.05, meaning that the experimental group had better balance even before training. The difference is significant. Cohen’s d = 0.979, indicating a large effect size.
- Stable Surface—Eyes Closed Final (p < 0.001): p < 0.001, so the experimental group improved significantly more. The difference is significant. Cohen’s d = −4.566, indicating a very large effect size.
- Unstable Surface (USS)—Eyes Open Initial (p = 0.066): p > 0.05, meaning that both groups started at a similar level. The difference is not significant. Cohen’s d = −0.699, indicating a medium effect size.
- Unstable Surface—Eyes Open Final (p < 0.001): p < 0.001, showing that the experimental group improved much more. Cohen’s d = −7.456, indicating an extremely large effect size.
- Unstable Surface—Eyes Closed Initial (p = 0.562): p > 0.05, meaning that both groups started at a similar level. The difference is not significant. Cohen’s d = 0.214, indicating a small effect size.
- Unstable Surface—Eyes Closed Final (p < 0.001): p < 0.001, showing that the experimental group improved much more. The difference is significant. Cohen’s d = −14.251, indicating a huge effect size.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| T2DM | type 2 diabetes mellitus |
| DPN | diabetic peripheral neuropathy |
| BBS | Biodex Balance System |
| SOT | sensory organization test |
| pLOS | mean peak sway amplitude |
| SMMSE | Standardized Mini-Mental Scale |
| GSI | general stability index |
| FPI | frontal–posterior index |
| MLI | medial–lateral index |
References
- Timar, B.; Timar, R.; Gaita, L.; Oancea, C.; Levai, C.; Lungeanu, D. The impact of diabetic neuropathy on balance and on the risk of falls in patients with type 2 diabetes mellitus: A cross-sectional study. PLoS ONE 2016, 11, e0154654. [Google Scholar] [CrossRef] [PubMed]
- Zimmet, P.; Alberti, K.G.; Magliano, D.J.; Bennett, P.H. Diabetes mellitus statistics on prevalence and mortality: Facts and fallacies. Nat. Rev. Endocrinol. 2016, 12, 616–622. [Google Scholar] [CrossRef]
- Boyle, J.P.; Thompson, T.J.; Gregg, E.W.; Barker, L.E.; Williamson, D.F. Projection of the year 2050 burden of diabetes in the US adult population: Dynamic modeling of incidence, mortality, and prediabetes prevalence. Popul. Health Metr. 2010, 8, 29. [Google Scholar] [CrossRef]
- Javeed, N.; Matveyenko, A.V. Circadian etiology of type 2 diabetes mellitus. Physiology 2018, 33, 138–150. [Google Scholar] [CrossRef]
- Domínguez-Muñoz, F.J.; Villafaina, S.; García-Gordillo, M.A.; Hernández-Mocholi, M.A.; Collado-Mateo, D.; Adsuar, J.C.; Gusi, N. Effects of 8-week whole-body vibration training on the HbA1c, quality of life, physical fitness, body composition, and foot health status in people with T2DM: A double-blinded randomized controlled trial. Int. J. Environ. Res. Public Health 2020, 17, 1317. [Google Scholar] [CrossRef] [PubMed]
- Bodman, M.A.; Dreyer, M.A.; Varacallo, M.A. Diabetic Peripheral Neuropathy; StatPearls [Internet]. StatPearls Publ. L. L. C.: St. Petersburg, FL, USA, 2025. Available online: https://www.ncbi.nlm.nih.gov/books/NBK442009/ (accessed on 15 April 2025).
- American Diabetes Association. Understanding Neuropathy and Your Diabetes. 2025. Available online: https://diabetes.org/about-diabetes/complications/neuropathy (accessed on 15 April 2025).
- Diabetes, U.K. Diabetic Neuropathy [Nerve Damage]. 2025. Available online: https://www.diabetes.org.uk/about-diabetes/complications/nerves-neuropathy (accessed on 15 April 2025).
- Pušnik, L.; Gabor, A.; Radochová, B.; Janáček, J.; Saudek, F.; Alibegović, A.; Serša, I.; Cvetko, E.; Umek, N.; Snoj, Ž. High-Field Diffusion Tensor Imaging of Median, Tibial, and Sural Nerves in Type 2 Diabetes With Morphometric Analysis. J Neuroimaging 2025, 35, e70025. [Google Scholar] [CrossRef]
- Daud, S.A.H.; Rahman, M.U.; Arsh, A.; Junaid, M. Effect of balance training with Biodex Balance System to improve balance in patients with diabetic neuropathy: A quasi experimental study. Pak. J. Med. Sci. 2021, 37, 389–392. [Google Scholar] [CrossRef]
- Stolarczyk, A.; Jarzemski, I.; Maciąg, B.M.; Radzimowski, K.; Świercz, M.; Stolarczyk, M. Balance and motion coordination parameters can be improved in patients with type 2 diabetes with physical balance training: Non-randomized controlled trial. BMC Endocr. Disord. 2021, 21, 143. [Google Scholar] [CrossRef] [PubMed]
- Ravand, M.; Ghasemi, M.; Rahimi, A.; Mohajeri-Tehrani, M.R.; Akbarzadeh Baghban, A. Dynamic balance and neuropathic changes following ankle proprioceptive training in type II diabetic patients with peripheral neuropathy. Iran. Red Crescent Med. J. 2021, 23, e406. [Google Scholar]
- Reyhanıoglu, D.A.; Yıldırım, G.; Sengun, I.Ş.; Kara, B. Effects of computer-based balance exercises on balance, pain, clinical presentation and nerve function in patients with diabetic peripheral neuropathy: A randomized controlled study. J. Musculoskelet. Neuronal Interact. 2024, 24, 168–177. [Google Scholar]
- Alaee, S.J.; Barati, K.; Hajiaghaei, B.; Ghomian, B.; Moradi, S.; Poorpirali, M. Immediate effect of textured insoles on the balance in patients with diabetic neuropathy. J. Diabetes Investig. 2023, 14, 435–440. [Google Scholar] [CrossRef] [PubMed]
- WebMD. Peripheral Neuropathy Risk Factors and Symptoms. 2025. Available online: https://www.webmd.com/diabetes/peripheral-neuropathy-risk-factors-symptoms (accessed on 15 April 2025).
- Eftekhar-Sadat, B.; Azizi, R.; Aliasgharzadeh, A.; Toopchizadeh, V.; Ghojazadeh, M. Effect of balance training with Biodex Stability System on balance in diabetic neuropathy. Ther. Adv. Endocrinol. Metab. 2015, 6, 233–240. [Google Scholar] [CrossRef]
- Marchant, A.; Wallwork, S.B.; Witchalls, J.; Ball, N.; Waddington, G. The effect of a combined compression-tactile stimulating sock on postural stability. Front. Sports Act. Living 2024, 6, 1516182. [Google Scholar] [CrossRef]
- Cadore, E.L.; Bays Moneo, A.B.; Martinez Mensat, M.; Rozas Muñoz, A.; Casas-Herrero, A.; Rodriguez-Mañas, L.; Izquierdo, M. Positive effects of resistance training in frail elderly patients with dementia after long-term physical restraint. Age 2014, 36, 801–811. [Google Scholar] [CrossRef]
- Nouraeinejad, A. Postural stability in strabismus and amblyopia. Strabismus 2023, 31, 202–209. [Google Scholar] [CrossRef] [PubMed]
- Wafa, T.; Zalewski, C.; Tamaki, C.; Barac-Cikoja, D.; Bakke, M.; Brewer, C. A new paradigm for assessing postural stability. Gait Posture 2023, 100, 188–192. [Google Scholar] [CrossRef] [PubMed]
- Salehi, E.N.; Fard, S.J.; Jaberzadeh, S. Mental fatigue impairs postural stability in older adults. Res. Q. Exerc. Sport 2023, 94, 401–408. [Google Scholar] [CrossRef]
- Loyd, B.J.; Agnew, L.; Fangman, A.; Thackeray, A.; Peterson, D.S.; Schubert, M.C.; Dibble, L. Characterizing gaze and postural stability deficits in people with multiple sclerosis. Mult. Scler. Relat. Disord. 2021, 55, 103205. [Google Scholar] [CrossRef]
- Sariyeva Aydam, A.; Cetin, E.; Sariyeva Ismayilov, A. Which is superior for postural stability: Contact lens or spectacles? Clin. Exp. Optom. 2024, 107, 281–284. [Google Scholar] [CrossRef]
- Salihu, A.T.; Hill, K.D.; Jaberzadeh, S. Effect of cognitive task complexity on dual task postural stability: A systematic review and meta-analysis. Exp. Brain Res. 2022, 240, 703–731. [Google Scholar] [CrossRef]
- Saurabh Kumar, M.; Gupta, A. Relationship between cognitive impairment and postural stability in the elderly population. Sport Sci. Health 2023, 19, 545–551. [Google Scholar] [CrossRef]
- Aliperti, C.; Steckenrider, J.; Sattari, D.; Peterson, J.; Bell, C.; Zifchock, R. Leveraging sensor technology to characterize the postural control spectrum. Sensors 2024, 24, 7420. [Google Scholar] [CrossRef]
- Min, S.N.; Subramaniyam, M.; Parnianpour, M.; Kim, D.J. Postural and spinal stability analysis for different floor sitting styles. Heliyon 2024, 10, e37379. [Google Scholar] [CrossRef] [PubMed]
- Dawson, N.; Dzurino, D.; Karleskint, M.; Tucker, J. Examining the reliability, correlation, and validity of commonly used assessment tools to measure balance. Health Sci. Rep. 2018, 1, e98. [Google Scholar] [CrossRef] [PubMed]
- El-Wishy, A.; Elsayed, E. Effect of proprioceptive training program on balance in patients with diabetic neuropathy: A controlled randomized study. Bull. Fac. Phys. Ther. 2012, 17, 1–8. [Google Scholar]
- Malwanage, K.T.; Liyanage, E.; Weerasinghe, V.; Antonypillai, C.; Nanayakkara, I. A novel proprioceptive rehabilitation program: A pilot randomized controlled trail as an approach to address proprioceptive deficits in patients with diabetic polyneuropathy. PLoS ONE 2024, 19, e0305055. [Google Scholar] [CrossRef]
- Gherghel, C.L.; Teodorescu, V.; Iordan, D.A.; Sardaru, D.P.; Onu, I. Analysis of oscillations of the center of pressure in postural control. Balneo PRM Res. J. 2024, 15, 698. [Google Scholar] [CrossRef]
- Afsharmand, Z.; Akoochakian, M.; Daneshmandi, H.; Sokhanguei, Y. The effect of training on stable and unstable surfaces on static balance in healthy elderly. Phys. Treat. Specif. Phys. Ther. J. 2018, 8, 143–152. [Google Scholar] [CrossRef]
- Ulbrich, M. Training postural control with eyes-closed vs eyes-open and effects on postural control improvement. A Thesis Presented to The Faculty of Humboldt State University In Partial Fulfillment of the Requirements for the Degree Master of Science in Kinesiology. 2020. Available online: https://digitalcommons.humboldt.edu/cgi/viewcontent.cgi?article=1404&context=etd (accessed on 24 June 2025).
- Salsabili, H.; Bahrpeyma, F.; Forogh, B.; Rajabali, S. Dynamic stability training improves standing balance control in neuropathic patients with type 2 diabetes. J. Rehabil. Res. Dev. 2011, 48, 775–786. [Google Scholar] [CrossRef]
- Irrgang, J.J.; Whitney, S.L.; Cox, E.D. Balance and Proprioceptive Training for Rehabilitation of the Lower Extremity. J. Sport Rehabil. 1994, 3, 68–83. [Google Scholar] [CrossRef]
- Badau, D.; Badau, A. Identifying the incidence of exercise dependence attitudes, levels of body perception, and preferences for use of fitness technology monitoring. Int. J. Environ. Res. Public Health 2018, 15, 2614. [Google Scholar] [CrossRef] [PubMed]
- Badau, A.; Badau, D.; Serban, C.; Tarcea, M.; Rus, V. Wellness integrative profile 10 (WIP10)—An integrative educational tool of nutrition, fitness and health. J. Pak. Med. Assoc. 2018, 68, 882–887. [Google Scholar] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Descriptives | N | Mean | Standard Deviation | Minimum | Maximum | Shapiro–Wilk W | Shapiro–Wilk p | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Group | 1 | 2 | 1 | Dif. 1 | 2 | Dif. 2 | 1.00 | 2.00 | 1 | 2 | 1 | 2 | 1 | 2 | 1 | 2 |
| Age | 15 | 15 | 60.3 | 59.7 | 3.28 | 2.97 | 55 | 55 | 66 | 64 | 0.975 | 0.95 | 0.923 | 0.5 | ||
| SS_openI | 15 | 15 | 1.2 | 0.77 | 1.18 | 0.18 | 0.04 | 0.04 | 1.13 | 1.1 | 1.27 | 1.3 | 0.980 | 0.92 | 0.969 | 0.22 |
| SS_openF | 15 | 15 | 0.43 | 0.77 | 0.02 | 0.12 | 0.4 | 0.6 | 0.46 | 1 | 0.901 | 0.90 | 0.099 | 0.08 | ||
| SS_closedI | 15 | 15 | 1.25 | 0.43 | 1.22 | 0.20 | 0.03 | 0.03 | 1.19 | 1.17 | 1.29 | 1.28 | 0.92 | 0.95 | 0.180 | 0.49 |
| SS_closedF | 15 | 15 | 0.82 | 1.02 | 0.02 | 0.06 | 0.8 | 0.9 | 0.85 | 1.1 | 0.919 | 0.89 | 0.183 | 0.06 | ||
| USS_openI | 15 | 15 | 1.23 | 0.42 | 1.26 | 0.21 | 0.05 | 0.03 | 1.16 | 1.2 | 1.3 | 1.3 | 0.923 | 0.92 | 0.214 | 0.16 |
| USS_openF | 15 | 15 | 0.81 | 1.05 | 0.02 | 0.04 | 0.79 | 1 | 0.84 | 1.1 | 0.924 | 0.82 | 0.223 | 0.01 | ||
| USS_closedI | 15 | 15 | 3.07 | 0.66 | 3.06 | 0.02 | 0.04 | 0.03 | 3 | 3 | 3.15 | 3.1 | 0.98 | 0.92 | 0.972 | 0.18 |
| USS_closedF | 15 | 15 | 2.41 | 3.04 | 0.01 | 0.06 | 2.39 | 3 | 2.43 | 3.2 | 0.877 | 0.8 | 0.042 | 0.00 | ||
| Statistic | df | p | Mean diff. | SE diff. | Significant Difference | Effect Size (Cohen’s d) | ||
|---|---|---|---|---|---|---|---|---|
| Age | Student’s t | 0.525 | 28 | 0.604 | 0.60 | 1.14 | 0.19 | |
| Welch’s t | 0.525 | 27.7 | 0.604 | 0.60 | 1.14 | 0.19 | ||
| SS_openI | Student’s t | 1.424 | 28 | 0.166 | 0.02 | 0.02 | 0.52 | |
| Welch’s t | 1.424 | 28 | 0.166 | 0.02 | 0.02 | 0.52 | ||
| SS_SS_openF | Student’s t | −10.98 | 28 | <0.001 | −0.34 | 0.03 | −4.01 | |
| Welch’s t | −10.98 | 14.9 | <0.001 | −0.34 | 0.03 | Yes | −4.01 | |
| SS_closedI | Student’s t | 2.681 | 28 | 0.012 | 0.03 | 0.01 | Yes | 0.98 |
| Welch’s t | 2.681 | 27.5 | 0.012 | 0.03 | 0.01 | 0.98 | ||
| SS_SS_closedF | Student’s t | −12.505 | 28 | <0.001 | −0.20 | 0.02 | −4.57 | |
| Welch’s t | −12.505 | 16.2 | <0.001 | −0.20 | 0.02 | Yes | −4.57 | |
| USS_openI | Student’s t | −1.914 | 28 | 0.066 | −0.03 | 0.01 | −0.70 | |
| Welch’s t | −1.914 | 23 | 0.068 | −0.03 | 0.01 | −0.70 | ||
| USS_SS_openF | Student’s t | −20.42 | 28 | <0.001 | −0.23 | 0.01 | −7.46 | |
| Welch’s t | −20.42 | 18.3 | <0.001 | −0.23 | 0.01 | Yes | −7.46 | |
| USS_closedI | Student’s t | 0.587 | 28 | 0.562 | 0.01 | 0.01 | 0.21 | |
| Welch’s t | 0.587 | 25.2 | 0.563 | 0.01 | 0.01 | 0.21 | ||
| USS_SS_closedF | Student’s t | −39.028 | 28 | <0.001 | −0.63 | 0.02 | −14.25 | |
| Welch’s t | −39.028 | 15.4 | <0.001 | −0.63 | 0.02 | Yes | −14.25 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xhardo, K.; Xhardo, E.; Bratu, M.; Pandea, A.; Cordun, M.; Vasiliu, A.-M.; Costin, D.-E.; Iacob, G.S.; Mihajlov, M.; Onu, I.; et al. The Impact of Biodex Balance on Improving Coordination and Static Balance in Patients with Diabetic Peripheral Neuropathy. Life 2025, 15, 1030. https://doi.org/10.3390/life15071030
Xhardo K, Xhardo E, Bratu M, Pandea A, Cordun M, Vasiliu A-M, Costin D-E, Iacob GS, Mihajlov M, Onu I, et al. The Impact of Biodex Balance on Improving Coordination and Static Balance in Patients with Diabetic Peripheral Neuropathy. Life. 2025; 15(7):1030. https://doi.org/10.3390/life15071030
Chicago/Turabian StyleXhardo, Kristo, Elona Xhardo, Mircea Bratu, Alin Pandea, Mariana Cordun, Ana-Maria Vasiliu, Dan-Eugen Costin, George Sebastian Iacob, Marjan Mihajlov, Ilie Onu, and et al. 2025. "The Impact of Biodex Balance on Improving Coordination and Static Balance in Patients with Diabetic Peripheral Neuropathy" Life 15, no. 7: 1030. https://doi.org/10.3390/life15071030
APA StyleXhardo, K., Xhardo, E., Bratu, M., Pandea, A., Cordun, M., Vasiliu, A.-M., Costin, D.-E., Iacob, G. S., Mihajlov, M., Onu, I., & Iordan, D.-A. (2025). The Impact of Biodex Balance on Improving Coordination and Static Balance in Patients with Diabetic Peripheral Neuropathy. Life, 15(7), 1030. https://doi.org/10.3390/life15071030