
Psoriasiform Dermatitis: From Pathogenesis to New Therapeutic Opportunities

 , , ,
, , ,  and
and
Abstract
1. Introduction
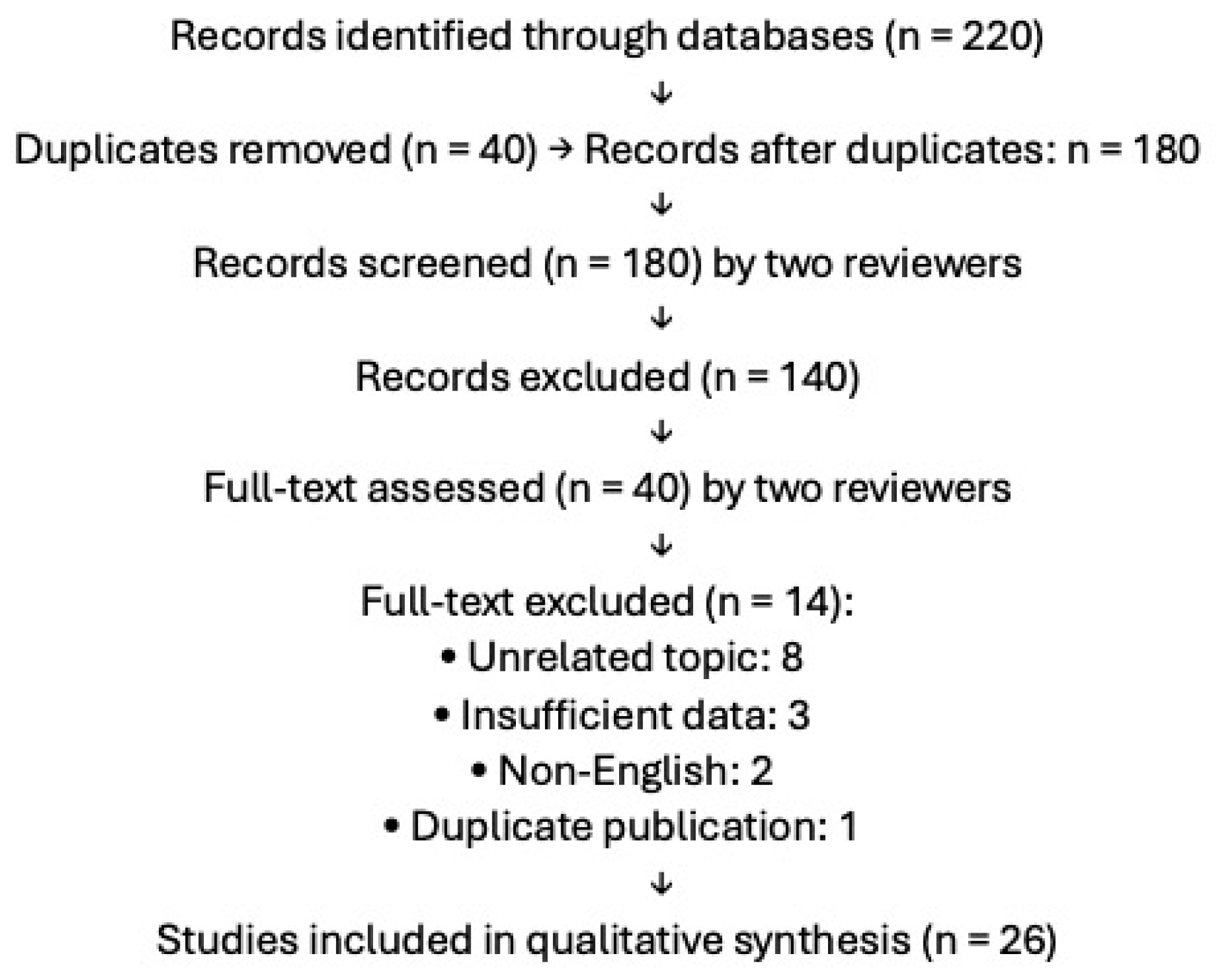
2. Methods
3. Pathogenesis
4. Clinical Features
5. Diagnosis
6. Histopathology
7. Advanced Imaging
8. Treatment Approaches
8.1. Topical Therapies
8.2. Experimental and Non-Conventional Agents
8.3. JAK Inhibitors
8.4. PDE4 Inhibitors (Apremilast)
8.5. Anti-IL-17
8.6. Anti-IL-23
8.7. Anti-IL-4/IL-13
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Wick, M.R. Psoriasiform dermatitides: A brief review. Semin. Diagn. Pathol. 2017, 34, 220–225. [Google Scholar] [CrossRef] [PubMed]
- Ali, K.; Wu, L.; Qiu, Y.; Li, M. Case report: Clinical and histopathological characteristics of psoriasiform erythema and de novo IL-17A cytokines expression on lesioned skin in atopic dermatitis children treated with dupilumab. Front. Med. 2022, 9, 932766. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Liu, T.; Li, S.; Ying, S.; Tang, S.; Ding, Y.; Li, Y.; Qiao, J.; Fang, H. The IL-23/IL-17 Pathway in Inflammatory Skin Diseases: From Bench to Bedside. Front. Immunol. 2020, 11, 594735. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zhu, H.; Jiang, J.; Yang, M.; Zhao, M.; He, Z.; Tang, C.; Song, C.; Akbar, A.N.; Reddy, V.; Pan, W.; et al. Topical application of a BCL-2 inhibitor ameliorates imiquimod-induced psoriasiform dermatitis by eliminating senescent cells. J. Dermatol. Sci. 2024, 115, 54–63. [Google Scholar] [CrossRef] [PubMed]
- George, L.A.; Gadani, A.; Cross, R.K.; Jambaulikar, G.; Ghazi, L.J. Psoriasiform Skin Lesions Are Caused by Anti-TNF Agents Used for the Treatment of Inflammatory Bowel Disease. Dig. Dis. Sci. 2015, 60, 3424–3430. [Google Scholar] [CrossRef] [PubMed]
- Gambardella, A.; Calabrese, G.; Di Brizzi, E.V.; Alfano, R.; Argenziano, G. A case of Atopic dermatitis and Hidradenitis Suppurativa successfully treated with Dupilumab. J. Eur. Acad. Dermatol. Venereol. 2020, 34, e284–e286. [Google Scholar] [CrossRef] [PubMed]
- Ferrucci, S.; Tavecchio, S.; Maronese, C.A.; Balato, A.; Di Brizzi, E.V.; Ortoncelli, M.; Ribero, S.; Girolomoni, G.; Maurelli, M.; Fortina, A.B.; et al. Short-, mid- and long-term efficacy of dupilumab in moderate-to-severe atopic dermatitis: A real-world multicentre Italian study of 2576 patients. Clin. Exp. Dermatol. 2024, 49, 1561–1572. [Google Scholar] [CrossRef] [PubMed]
- Napolitano, M.; Foggia, L.; Patruno, C.; Gallo, L.; Tommasino, N.; Cecere, D.; Megna, M. Efficacy of Janus kinase inhibitors in the treatment of psoriasiform atopic dermatitis. Clin. Exp. Dermatol. 2024, 49, 1232–1234. [Google Scholar] [CrossRef] [PubMed]
- Salvi, I.; Parodi, A.; Cozzani, E.; Burlando, M. Case report: Psoriasiform eczema with immune-mediated comorbidities treated with upadacitinib. Front. Immunol. 2024, 15, 1432233. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Tortola, L.; Rosenwald, E.; Abel, B.; Blumberg, H.; Schäfer, M.; Coyle, A.J.; Renauld, J.-C.; Werner, S.; Kisielow, J.; Kopf, M. Psoriasiform dermatitis is driven by IL-36-mediated DC-keratinocyte crosstalk. J. Clin. Investig. 2012, 122, 3965–3976. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Huang, Y.; Wang, Y.; Zhen, Y.; Liu, W.; Wang, Y.; Wang, R.; Wang, N.; Huang, S.; Yan, J.; Sun, Q. LPCAT1 Facilitates Keratinocyte Hyperproliferation and Skin Inflammation in Psoriasis by Regulating GLUT3. J. Investig. Dermatol. 2024, 144, 1479–1490.e14. [Google Scholar] [CrossRef] [PubMed]
- Blanchard, G.; Bisig, B.; de Leval, L.; Hohl, D.; Guenova, E. Cytokine-pathway blockers worsen mycosis fungoides masquerading as psoriasis. JAAD Case Rep. 2024, 48, 98–102. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Liu, J.; Qiu, C.; Zhou, Z.; Li, J.; Zhen, Y.; Wang, R.; Zhuang, Y.; Zhang, F. Pentraxin 3 exacerbates psoriasiform dermatitis through regulation of macrophage polarization. Int. Immunopharmacol. 2024, 130, 111805. [Google Scholar] [CrossRef] [PubMed]
- Popa, L.G.; Giurcaneanu, C.; Portelli, M.G.; Mihai, M.M.; Beiu, C.; Orzan, O.A.; Ion, A.; Anghel, T.H. Perspectives on Psoriasiform Adverse Events from Immune Checkpoint Inhibitors: Lessons Learned from Our Practice. Medicina 2024, 60, 373. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bezdek, S.; Leng, L.; Busch, H.; Mousavi, S.; Rades, D.; Dahlke, M.; Zillikens, D.; Bucala, R.; Sadik, C.D. Macrophage Migration Inhibitory Factor (MIF) Drives Murine Psoriasiform Dermatitis. Front. Immunol. 2018, 9, 2262. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Billi, A.C.; Ludwig, J.E.; Fritz, Y.; Rozic, R.; Swindell, W.R.; Tsoi, L.C.; Gruzska, D.; Abdollahi-Roodsaz, S.; Xing, X.; Diaconu, D.; et al. KLK6 expression in skin induces PAR1-mediated psoriasiform dermatitis and inflammatory joint disease. J. Clin. Investig. 2020, 130, 3151–3157. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Diaz-Perez, J.A.; Killeen, M.E.; Yang, Y.; Carey, C.D.; Falo, L.D.; Mathers, A.R. Extracellular ATP and IL-23 Form a Local Inflammatory Circuit Leading to the Development of a Neutrophil-Dependent Psoriasiform Dermatitis. J. Investig. Dermatol. 2018, 138, 2595–2605. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Stingeni, L.; Bianchi, L.; Antonelli, E.; Caroppo, E.S.; Ferrucci, S.M.; Gurioli, C.; Ortoncelli, M.; Fabbrocini, G.; Nettis, E.; Schena, D.; et al. A 52-week update of a multicentre Italian real-world experience on effectiveness and safety of dupilumab in adolescents with moderate-to-severe atopic dermatitis. J. Eur. Acad. Dermatol. Venereol. 2023, 37, e384–e388. [Google Scholar] [CrossRef] [PubMed]
- Parker, J.J.; Sugarman, J.L.; Silverberg, N.B.; Gonzalez, M.E.; Ramien, M.L.; Teng, J.M.C.; Paller, A.S. Psoriasiform dermatitis during dupilumab treatment for moderate-to-severe atopic dermatitis in children. Pediatr. Dermatol. 2021, 38, 1500–1505. [Google Scholar] [CrossRef] [PubMed]
- Patruno, C.; Fabbrocini, G.; De Lucia, M.; Picone, V.; Genco, L.; Napolitano, M. Psoriasiform dermatitis induced by dupilumab successfully treated with upadacitinib. Dermatol. Ther. 2022, 35, e15788. [Google Scholar] [CrossRef] [PubMed]
- Bieber, K.; Bezdek, S.; Gupta, Y.; Vorobyev, A.; Sezin, T.; Gross, N.; Prüssmann, J.; Sayegh, J.; Becker, M.; Mousavi, S.; et al. Forward genetics and functional analysis highlight Itga11 as a modulator of murine psoriasiform dermatitis. J. Pathol. 2023, 261, 184–197. [Google Scholar] [CrossRef] [PubMed]
- Tian, S.; Chen, S.; Feng, Y.; Li, Y. The Interactions of Small Proline-Rich Proteins with Late Cornified Envelope Proteins are Involved in the Pathogenesis of Psoriasis. Clin. Cosmet. Investig. Dermatol. 2021, 14, 1355–1365. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mehta, S.; Singal, A.; Singh, N.; Bhattacharya, S.N. A study of clinicohistopathological correlation in patients of psoriasis and psoriasiform dermatitis. Indian. J. Dermatol. Venereol. Leprol. 2009, 75, 100. [Google Scholar] [CrossRef] [PubMed]
- Di Brizzi, E.V.; Buononato, D.; Benvenuto, P.; Argenziano, G.; De Pasquale, R.; Fiorella, C.S.; Gioffrè, C.; Musumeci, M.L.; Palazzo, G.; Zichichi, L.; et al. Effectiveness and Safety After a Switch to Tildrakizumab: A Real World Multicenter Italian Study in Psoriasis. Dermatol. Pract. Concept. 2023, 13, e2023215. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Gargiulo, L.; Ibba, L.; Ingurgio, R.C.; Malagoli, P.; Amoruso, F.; Balato, A.; Bardazzi, F.; Brianti, P.; Brunasso, G.; Burlando, M.; et al. Comparative effectiveness of tildrakizumab 200 mg versus tildrakizumab 100 mg in psoriatic patients with high disease burden or above 90 kg of body weight: A 16-week multicenter retrospective study-IL PSO (Italian landscape psoriasis). J. Dermatol. Treat. 2024, 35, 2350760. [Google Scholar] [CrossRef] [PubMed]
- Barr, R.J.; Young, E.M., Jr. Psoriasiform and related papulosquamous disorders. J. Cutan. Pathol. 1985, 12, 412–425. [Google Scholar] [CrossRef] [PubMed]
- Patrizi, A.; Bardazzi, F.; Neri, I.; Fanti, P.A. Psoriasiform acral dermatitis: A peculiar clinical presentation of psoriasis in children. Pediatr. Dermatol. 1999, 16, 439–443. [Google Scholar] [CrossRef] [PubMed]
- Tosti, A.; Fanti, P.A.; Morelli, R.; Bardazzi, F. Psoriasiform acral dermatitis. Report of three cases. Acta Derm. Venereol. 1992, 72, 206–207. [Google Scholar] [CrossRef] [PubMed]
- Lallas, A.; Zalaudek, I.; Argenziano, G.; Longo, C.; Moscarella, E.; Di Lernia, V.; Al Jalbout, S.; Apalla, Z. Dermoscopy in general dermatology. Dermatol. Clin. 2013, 31, 679–694. [Google Scholar] [CrossRef] [PubMed]
- Di Brizzi, E.V.; Moscarella, E.; Piana, S.; Longo, C.; Franco, R.; Alfano, R.; Argenziano, G. Clinical and dermoscopic features of pleomorphic dermal sarcoma. Australas. J. Dermatol. 2019, 60, e153–e154. [Google Scholar] [CrossRef] [PubMed]
- Corneli, P.; Moscarella, E.; Di Brizzi, E.V.; Ronchi, A.; Zalaudek, I.; Alfano, R.; Argenziano, G. Pigmented Squamous Cell Carcinoma: Is the Reported Prevalence Real? Dermatol. Pract. Concept. 2019, 9, 150–151. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sutarjono, B.; Lebovitch, H. Psoriasiform spongiotic dermatitis. BMJ Case Rep. 2019, 12, e228690. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Scharf, C.; Di Brizzi, E.V.; Licata, G.; Piccolo, V.; Argenziano, G.; Moscarella, E. Reflectance confocal microscopy in paediatric patients: Applications and limits. Exp. Dermatol. 2023, 32, 210–213. [Google Scholar] [CrossRef] [PubMed]
- Benvenuto, P.; Tancredi, V.; Ronchi, A.; Scharf, C.; Fulgione, E.; Moscarella, E. In Vivo Characterization of the Inflammatory Infiltrate in Discoid Lupus Erythematosus (DLE) by Line-Field Confocal Optical Coherence Tomography (LC-OCT). Dermatol. Pract. Concept. 2025, 15, 5089. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mao, J.; Du, N.; Jia, Y.; Mao, Q.; Yang, J.; Zhang, Y.; Li, Y.; Cao, L.; Min, W. Case report: Treatment of psoriasiform dermatitis in patients with malignancy. Front. Med. 2024, 11, 1363405. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kurihara, K.; Fujiyama, T.; Tokura, Y.; Honda, T. Two cases of psoriasiform dermatitis arising during dupilumab therapy and successfully treated with delgocitinib ointment. Eur. J. Dermatol. 2021, 31, 658–660. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Lu, S.; Lai, Y.; Wang, L. Topical histone deacetylase 1 inhibitor Entinostat ameliorates psoriasiform dermatitis through suppression of IL-17A response. J. Dermatol. Sci. 2023, 110, 89–98. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Killeen, M.E.; Sumpter, T.L.; Ferris, L.K.; Falo, L.D.; Freeman, B.A.; Schopfer, F.J.; Mathers, A.R. Electrophilic nitro-fatty acids suppress psoriasiform dermatitis: STAT3 inhibition as a contributory mechanism. Redox Biol. 2021, 43, 101987. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Okura, I.; Kamata, M.; Asano, Y.; Mitsui, A.; Shimizu, T.; Sato, S.; Tada, Y. Fingolimod ameliorates imiquimod-induced psoriasiform dermatitis by sequestrating interleukin-17-producing ?d T cells in secondary lymph nodes. J. Dermatol. Sci. 2021, 102, 116–125. [Google Scholar] [CrossRef] [PubMed]
- Chan, T.C.; Lee, M.-S.; Huang, W.-C.; Chang, W.-Y.; Krueger, J.G.; Tsai, T.-F. Capsaicin attenuates imiquimod-induced epidermal hyperplasia and cutaneous inflammation in a murine model of psoriasis. Biomed. Pharmacother. 2021, 141, 111950. [Google Scholar] [CrossRef] [PubMed]
- Miot, H.A.; Criado, P.R.; de Castro, C.C.S.; Ianhez, M.; Talhari, C.; Ramos, P.M. JAK-STAT pathway inhibitors in dermatology. An. Bras. Dermatol. 2023, 98, 656–677. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Tancredi, V.; Buononato, D.; Caccavale, S.; Di Brizzi, E.V.; Di Caprio, R.; Argenziano, G.; Balato, A. New Perspectives in the Management of Chronic Hand Eczema: Lessons from Pathogenesis. Int. J. Mol. Sci. 2023, 25, 362. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Samuel, C.; Cornman, H.; Kambala, A.; Kwatra, S.G. A Review on the Safety of Using JAK Inhibitors in Dermatology: Clinical and Laboratory Monitoring. Dermatol. Ther. 2023, 13, 729–749. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Shahriari, N.; Strober, B.; Shahriari, M. Upadacitinib for the treatment of psoriasiform and spongiotic dermatitis: A multicenter case series. JAAD Case Rep. 2024, 49, 106–109. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Cirone, K.D.; Lovegrove, F.E. Dupilumab-induced psoriasis in a patient with atopic dermatitis successfully treated with Upadacitinib: A case report. SAGE Open Med. Case Rep. 2025, 13, 2050313X251317811. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Foggia, L.; Potestio, L.; Patruno, C.; di Vico, F.; Napolitano, M. Reply to: Upadacitinib for the management of overlapping psoriasis and atopic dermatitis: A case series. Int. J. Dermatol. 2025, 64, 218. [Google Scholar] [CrossRef] [PubMed]
- Zhong, L.; Luo, N.; Wang, Q.; Li, T.; Hao, P. Tofacitinib for the Treatment of Psoriasiform Dermatitis Caused by IL-17 Inhibitors: A Case Report. J. Inflamm. Res. 2023, 16, 2167–2172. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Tegtmeyer, K.; Zhao, J.; Maloney, N.J.; Atassi, G.; Beestrum, M.; Lio, P.A. Off-label studies on tofacitinib in dermatology: A review. J. Dermatol. Treat. 2021, 32, 399–409. [Google Scholar] [CrossRef] [PubMed]
- Zerilli, T.; Ocheretyaner, E. Apremilast (Otezla): A New Oral Treatment for Adults With Psoriasis and Psoriatic Arthritis. Pharm. Ther. 2015, 40, 495–500. [Google Scholar] [PubMed] [PubMed Central]
- Uchida, H.; Kamata, M.; Shimizu, T.; Egawa, S.; Ito, M.; Takeshima, R.; Mizukawa, I.; Watanabe, A.; Tada, Y. Apremilast downregulates interleukin-17 production and induces splenic regulatory B cells and regulatory T cells in imiquimod-induced psoriasiform dermatitis. J. Dermatol. Sci. 2021, 104, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Orsini, D.; Megna, M.; Assorgi, C.; Balato, A.; Balestri, R.; Bernardini, N.; Bettacchi, A.; Bianchelli, T.; Bianchi, L.; Buggiani, G.; et al. Efficacy and Safety of bimekizumab in elderly patients: Real-world multicenter retrospective study-IL PSO (Italian Landscape Psoriasis). J. Dermatol. Treat. 2024, 35, 2393376. [Google Scholar] [CrossRef] [PubMed]
- Chiricozzi, A.; Coscarella, G.; Puig, L.; Vender, R.; Yeung, J.; Carrascosa, J.; Piaserico, S.; Gisondi, P.; Lynde, C.; Ferreira, P.; et al. Age affects drug survival rates of interleukin (IL)-17 and IL-23 inhibitors in patients with plaque psoriasis: Results from a retrospective, multicentric, multi-country, cohort study. J. Eur. Acad. Dermatol. Venereol. 2024, 38, 2175–2185. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Yu, S.; Zhang, G.; Xie, Y.; Wei, J.C. Interleukin-17 Monoclonal Antibody Successfully Treated Psoriasiform Drug Eruption Induced by Immune Checkpoint Inhibitors: A Case Report and Review of Literature. Dermatitis 2024, 35, 410–412. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Li, X.; Li, W.; Fan, R.; Ma, Q.; Luo, X.; Jian, H.; Chen, X.; Cao, C.; Zheng, W. Development of IL-17A inhibitor-induced atopic dermatitis-like rash in psoriasis patients: Insights into immune shift. Exp. Dermatol. 2024, 33, e14958. [Google Scholar] [CrossRef] [PubMed]
- Tan, T.L.; Taglia, L.; Yazdan, P. Drug-induced psoriasiform alopecia associated with interleukin-17 inhibitor therapy. J. Cutan. Pathol. 2021, 48, 771–774. [Google Scholar] [CrossRef] [PubMed]
- Caldarola, G.; Pirro, F.; Di Stefani, A.; Talamonti, M.; Galluzzo, M.; D’aDamio, S.; Magnano, M.; Bernardini, N.; Malagoli, P.; Bardazzi, F.; et al. Clinical and histopathological characterization of eczematous eruptions occurring in course of anti IL-17 treatment: A case series and review of the literature. Expert Opin. Biol. Ther. 2020, 20, 665–672. [Google Scholar] [CrossRef] [PubMed]
- Megna, M.; Balato, A.; Caccavale, S.; Cacciapuoti, S.; Calabrese, G.; Di Brizzi, E.V.; Di Costanzo, L.; Manzo, R.; Marino, V.; Puca, R.V.; et al. Real-Life Effectiveness and Safety of Guselkumab in Patients with Psoriasis Who Have an Inadequate Response to Ustekinumab: A 3-Year Multicenter Study. J. Clin. Med. 2024, 13, 2552. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zhou, L.; Wang, Y.; Wan, Q.; Wu, F.; Barbon, J.; Dunstan, R.; Gauld, S.; Konrad, M.; Leys, L.; McCarthy, R.; et al. A non-clinical comparative study of IL-23 antibodies in psoriasis. MAbs 2021, 13, 1964420. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Shimizu, T.; Kamata, M.; Fukaya, S.; Hayashi, K.; Fukuyasu, A.; Tanaka, T.; Ishikawa, T.; Ohnishi, T.; Tada, Y. Anti-IL-17A and IL-23p19 antibodies but not anti-TNFα antibody induce expansion of regulatory T cells and restoration of their suppressive function in imiquimod-induced psoriasiform dermatitis. J. Dermatol. Sci. 2019, 95, 90–98. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Wu, Z.; Wu, M.; Qiu, X.; Wu, Y.; Kuang, Z.; Wang, L.; Sun, T.; Liu, Y.; Yi, S.; et al. IBI112, a selective anti-IL23p19 monoclonal antibody, displays high efficacy in IL-23-induced psoriasiform dermatitis. Int. Immunopharmacol. 2020, 89 (Pt B), 107008. [Google Scholar] [CrossRef] [PubMed]
- Strecker, M.; Wlotzka, K.; Strassheimer, F.; Roller, B.; Ludmirski, G.; König, S.; Röder, J.; Opitz, C.; Alekseeva, T.; Reul, J.; et al. AAV-mediated gene transfer of a checkpoint inhibitor in combination with HER2-targeted CAR-NK cells as experimental therapy for glioblastoma. Oncoimmunology 2022, 11, 2127508. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Peña, A.; DeJongh, B.; Haas, M.; Harms, M. Overcoming barriers to monitoring patients taking second-generation antipsychotics. Ment. Health Clin. 2018, 8, 49–55. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]

{kind=link}
| Class | Agents |
|---|---|
| Topical therapies | Corticosteroids, Vitamin D analogs (Calcipotriol), Retinoids, Calcineurin inhibitors (Tacrolimus, Pimecrolimus) |
| JAK/STAT inhibitors | Delgocitinib (topical), Upadacitinib, Baricitinib, Abrocitinib, Tofacitinib, Gusacitinib |
| IL-4/IL-13 blockade | Dupilumab (IL-4/IL-13), Tralokinumab (IL-13) |
| PDE4 inhibitors | Apremilast, AFX5931 |
| Retinoids (systemic) | Alitretinoin |
| IL-17 inhibitors | Secukinumab, Ixekizumab, Brodalumab, Bimekizumab |
| IL-23 inhibitors | Guselkumab, Risankizumab, Tildrakizumab |
| Experimental agents | NO2-FAs, Fingolimod, Capsaicin |
| Systemic steroids | Prednisone, Methylprednisolone |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Brizzi, E.V.; Caccavale, S.; Giorgio, C.M.; Argenziano, G.; Balato, A. Psoriasiform Dermatitis: From Pathogenesis to New Therapeutic Opportunities. Life 2025, 15, 1026. https://doi.org/10.3390/life15071026
Di Brizzi EV, Caccavale S, Giorgio CM, Argenziano G, Balato A. Psoriasiform Dermatitis: From Pathogenesis to New Therapeutic Opportunities. Life. 2025; 15(7):1026. https://doi.org/10.3390/life15071026
Chicago/Turabian StyleDi Brizzi, Eugenia Veronica, Stefano Caccavale, Caterina Mariarosaria Giorgio, Giuseppe Argenziano, and Anna Balato. 2025. "Psoriasiform Dermatitis: From Pathogenesis to New Therapeutic Opportunities" Life 15, no. 7: 1026. https://doi.org/10.3390/life15071026
APA StyleDi Brizzi, E. V., Caccavale, S., Giorgio, C. M., Argenziano, G., & Balato, A. (2025). Psoriasiform Dermatitis: From Pathogenesis to New Therapeutic Opportunities. Life, 15(7), 1026. https://doi.org/10.3390/life15071026