
Intravenous Magnesium Sulphate as an Adjuvant Therapy for Acute Exacerbations of Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis
 , , , , , and
, , , , , and
Abstract
1. Introduction
2. Methods
2.1. Data Sources and Searches
2.2. Eligibility Criteria
2.3. Selection Process
2.4. Data Extraction
2.5. Risk of Bias Assessment
2.6. Data Analysis
3. Results
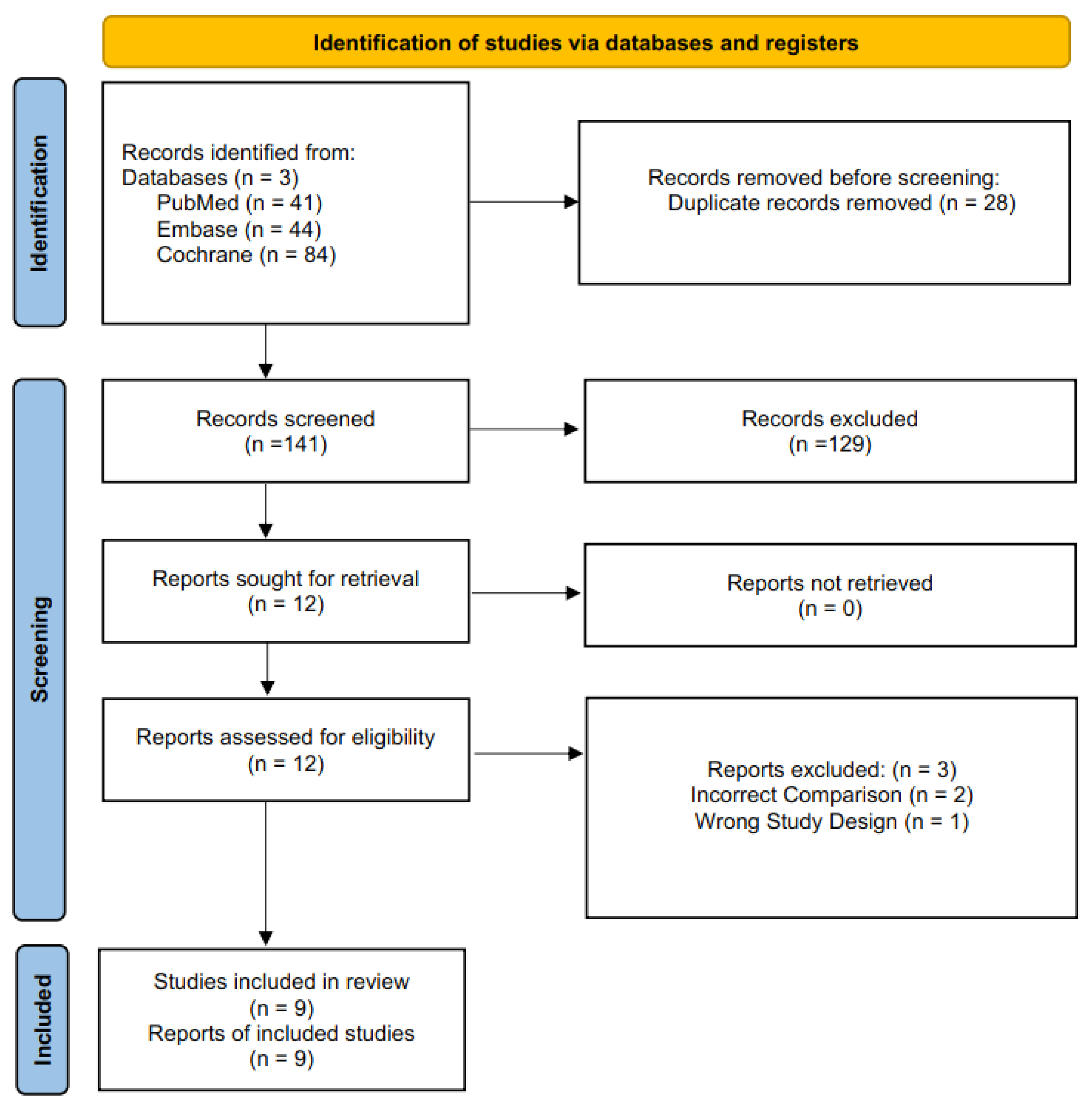
3.1. Study Selection
3.2. Study Characteristics
3.3. Primary Outcomes
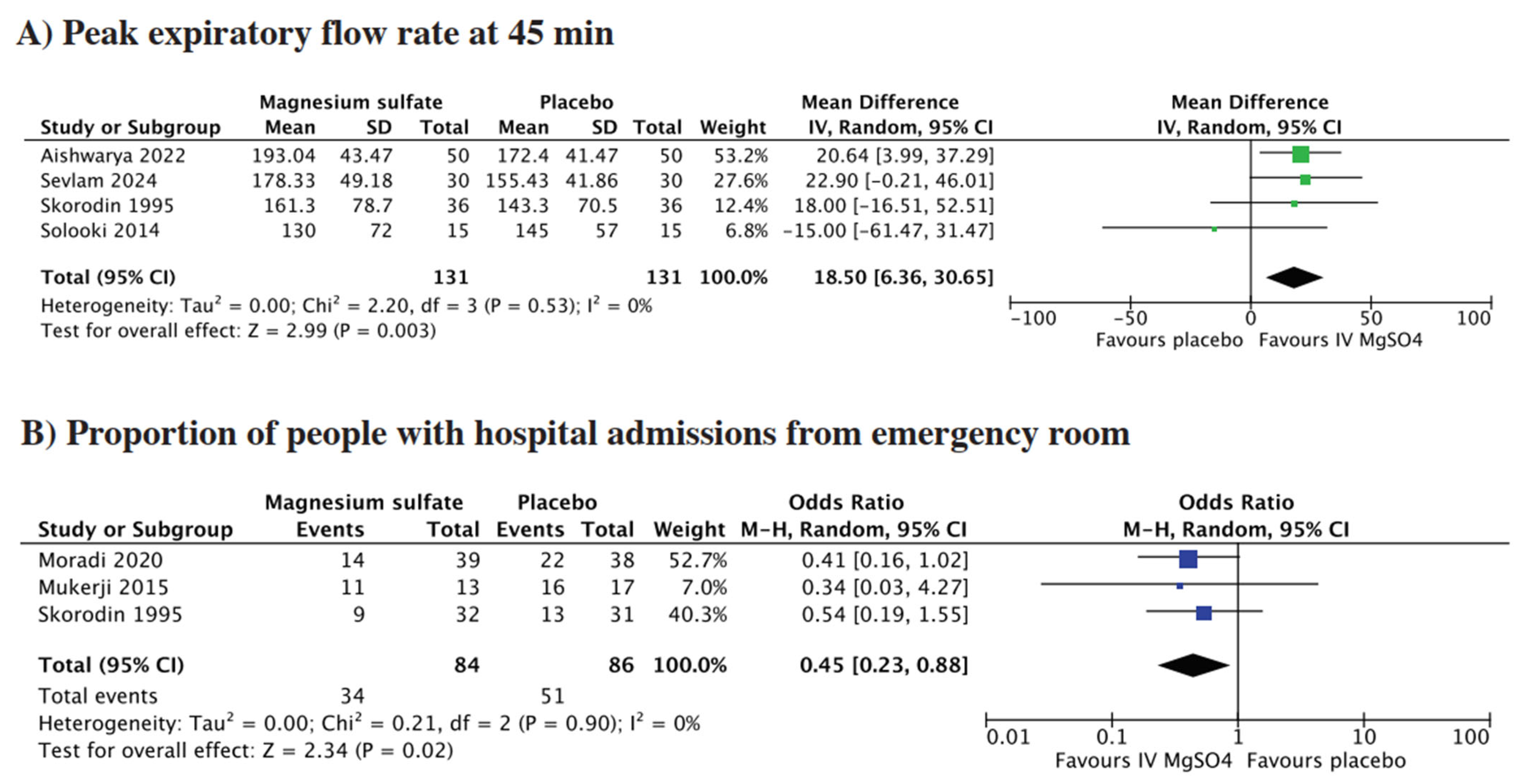
3.3.1. Peak Expiratory Flow at 45 min
3.3.2. Proportion of People with Hospital Admissions from Emergency Room
3.4. Secondary Outcomes
3.4.1. Length of Hospital Stay
3.4.2. Adverse Events
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Agustí, A.; Celli, B.R.; Criner, G.J.; Halpin, D.; Anzueto, A.; Barnes, P.; Bourbeau, J.; Han, M.K.; Martinez, F.J.; Montes de Oca, M.; et al. Global Initiative for Chronic Obstructive Lung Disease 2023 Report: GOLD Executive Summary. Am. J. Respir. Crit. Care Med. 2023, 207, 819–837. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. The Global Burden of Chronic Respiratory Diseases: Burden and Trends; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Boers, E.; Barrett, M.; Su, J.G.; Benjafield, A.V.; Sinha, S.; Kaye, L.; Zar, H.J.; Vuong, V.; Tellez, D.; Gondalia, R.; et al. Global Burden of Chronic Obstructive Pulmonary Disease Through 2050. JAMA Netw. Open 2023, 6, e2346598. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Roisin, R. COPD exacerbations · 5: Management. Thorax 2006, 61, 535–544. [Google Scholar] [CrossRef]
- Perera, P.N.; Armstrong, E.P.; Sherrill, D.L.; Skrepnek, G.H. Acute exacerbations of COPD in the United States: Inpatient burden and predictors of costs and mortality. COPD 2012, 9, 131–141. [Google Scholar] [CrossRef]
- Le Rouzic, O.; Roche, N.; Cortot, A.B.; Tillie-Leblond, I.; Masure, F.; Perez, T.; Boucot, I.; Hamouti, L.; Ostinelli, J.; Pribil, C.; et al. Defining the “Frequent Exacerbator” Phenotype in COPD: A Hypothesis-Free Approach. Chest 2018, 153, 1106–1115. [Google Scholar] [CrossRef] [PubMed]
- Cerci Neto, A.; Ferreira Filho, O.F.; Parreira, J.d.S. The relative frequency of hypomagnesemia in outpatients with chronic airflow limitation treated at a referral center in the north of the state of Paraná, Brazil. J. Bras. Pneumol. Publicacao Soc. Bras. Pneumol. E Tisilogia 2006, 32, 294–300. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Skorodin, M.; Tenholder, M.; Yetter, B.; Owen, K.; Waller, R.; Khandelwahl, S.; Maki, K.; Rohail, T.; D’Alfonso, N. Magnesium sulfate in exacerbations of chronic obstructive pulmonary disease. Arch. Intern. Med. 1995, 155, 496–500. [Google Scholar] [CrossRef]
- Solooki, M.; Miri, M.; Mokhtari, M.; Valai, M.; Sistanizad, M.; Kouchek, M. Magnesium Sulfate in Exacerbations of COPD in Patients Admitted to Internal Medicine Ward. Iran. J. Pharm. Res. 2014, 13, 1235–1239. [Google Scholar]
- Nouira, S.; Bouida, W.; Grissa, M.; Beltaief, K.; Trimech, M.; Boubaker, H.; Marghli, S.; Letaief, M.; Boukef, R. Magnesium sulfate versus ipratropium bromide in chronic obstructive pulmonary disease exacerbation: A randomized trial. Am. J. Ther. 2014, 21, 152–158. [Google Scholar] [CrossRef]
- Mukerji, S.; Shahpuri, B.; Clayton-Smith, B.; Smith, N.; Armstrong, P.; Hardy, M.; Marchant, G.; Marsh, E. Intravenous magnesium sulphate as an adjuvant therapy in acute exacerbations of chronic obstructive pulmonary disease: A single centre, randomised, double-blinded, parallel group, placebo-controlled trial: A pilot study. N. Z. Med. J. 2015, 128, 34–42. [Google Scholar] [PubMed]
- Jahanian, F.; Khatir, I.; Ahidashti, H.; Amirifard, S. The Effect of Intravenous Magnesium Sulphate as an Adjuvant in the Treatment of Acute Exacerbations of COPD in the Emergency Department: A Double-Blind Randomized Clinical Trial. Ethiop. J. Health Sci. 2021, 31, 267–274. [Google Scholar] [CrossRef] [PubMed]
- Vafadar Moradi, E.; Pishbin, E.; Habibzadeh, S.R.; Talebi Doluee, M.; Soltanifar, A. The Adjunctive Effect of Intravenous Magnesium Sulfate in Acute Exacerbation of Chronic Obstructive Pulmonary Disease: A Randomized Controlled Clinical Trial. Acad. Emerg. Med. Off. J. Soc. Acad. Emerg. Med. 2020, 28, 359–362. [Google Scholar] [CrossRef]
- Selvam, N.; Girish, K.; Priyanka, S.; Jyothi, R.; Srinivas Prabhu, N. A prospective comparative study of efficacy of intravenous magnesium sulfate infusion versus placebo, as an adjuvant to nebulized salbutamol in the management of acute exacerbations of chronic obstructive pulmonary disease. Natl. J. Physiol. Pharm. Pharmacol. 2024, 14, 2186–2191. [Google Scholar] [CrossRef]
- Aishwarya; Sharma, A.K.; Meena, A.B.; Sharma, G.; Jain, D.; Meena, V.R.; Ranjan, A.; Saxena, A. A study of role of intravenous magnesium sulfate in acute exacerbation of copd in a tertiary center. Int. J. Curr. Res. 2022. [Google Scholar] [CrossRef]
- Abreu González, J.; Hernández García, C.; Abreu González, P.; Martín García, C.; Jiménez, A. Effect of intravenous magnesium sulfate on chronic obstructive pulmonary disease exacerbations requiring hospitalization: A randomized placebo-controlled trial. Arch. Bronconeumol. 2006, 42, 384–387. [Google Scholar] [CrossRef]
- Kshirsagar, K.; Patil, V.C. Chronic obstructive pulmonary disease: Is serum magnesium level a risk factor for its acute exacerbation? Casp. J. Intern. Med. 2021, 12, 223–227. [Google Scholar] [CrossRef]
- Hughes, R.; Goldkorn, A.; Masoli, M.; Weatherall, M.; Burgess, C.; Beasley, R. Use of isotonic nebulised magnesium sulphate as an adjuvant to salbutamol in treatment of severe asthma in adults: Randomised placebo-controlled trial. Lancet Lond. Engl. 2003, 361, 2114–2117. [Google Scholar] [CrossRef]
- Gourgoulianis, K.I.; Chatziparasidis, G.; Chatziefthimiou, A.; Molyvdas, P.A. Magnesium as a relaxing factor of airway smooth muscles. J. Aerosol Med. Off. J. Int. Soc. Aerosols Med. 2001, 14, 301–307. [Google Scholar] [CrossRef]
- Ruljancic, N.; Popovic-Grle, S.; Rumenjak, V.; Sokolic, B.; Malic, A.; Mihanovic, M.; Cepelak, I. COPD: Magnesium in the plasma and polymorphonuclear cells of patients during a stable phase. COPD 2007, 4, 41–47. [Google Scholar] [CrossRef]
- Makwana, S.; Patel, A.; Sonagara, M. Correlation Between Serum Magnesium Level and Acute Exacerbation in Patients With Chronic Obstructive Pulmonary Disease (COPD). Cureus 2022, 14, e26229. [Google Scholar] [CrossRef] [PubMed]
- Rennard, S.I.; Farmer, S.G. Exacerbations and progression of disease in asthma and chronic obstructive pulmonary disease. Proc. Am. Thorac. Soc. 2004, 1, 88–92. [Google Scholar] [CrossRef] [PubMed]
- Cheuk, D.K.L.; Chau, T.C.H.; Lee, S.L. A meta-analysis on intravenous magnesium sulphate for treating acute asthma. Arch. Dis. Child. 2005, 90, 74–77. [Google Scholar] [CrossRef] [PubMed]
- Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for the Prevention, Diagnosis and Management of Chronic Obstructive Pulmonary Disease: 2024 Report. Available online: https://goldcopd.org (accessed on 10 May 2025).
- National Institute for Health and Care Excellence (NICE). Chronic Obstructive Pulmonary Disease in over 16s: Diagnosis and Management. NICE Guideline. Available online: https://www.nice.org.uk/guidance/ng115 (accessed on 10 May 2025).


{kind=link}
{kind=link}
{kind=link}
| Database | Search String | Records |
|---|---|---|
| PubMed/MEDLINE | (“Magnesium Sulfate”[Mesh] OR “magnesium sulfate”[tiab] OR “MgSO4”[tiab] OR “magnesium”) AND (“Pulmonary Disease, Chronic Obstructive”[Mesh] OR “chronic obstructive pulmonary disease”[tiab] OR “COPD”[tiab]) AND (“Acute Disease”[Mesh] OR “acute exacerbation”[tiab] OR “acute attack”[tiab] OR “exacerbation”[tiab]) | 41 |
| Cochrane | (“magnesium sulfate” OR “MgSO4” OR magnesium) AND (“chronic obstructive pulmonary disease” OR COPD) AND (“acute disease” OR “acute exacerbation” OR “acute attack” OR exacerbation) | 44 |
| Embase |
| 84 |
| Author (Year) | Sample Size | Sex | Current Smoker | Study Design | Setting | Mean Age | Patient Population | Intervention | |||
|---|---|---|---|---|---|---|---|---|---|---|---|
| MgSO4 | Placebo | Male | Female | MgSO4 | Placebo | ||||||
| Skorodin 1995 [9] | 36 | 36 | 70 | 2 | NR | NR | RCT | Emergency department | 64.7 ± 8.2 | Patients with acute COPD exacerbation with COPD duration of 11 years, smoking history of 40 years, and average initial SpO2 of 92.1% following albuterol. | IV 1.2 g of MgSO4 over 20 min plus standard care. |
| González 2006 [17] | 12 | 12 | 24 | 0 | NR | NR | RCT | Inpatient | 64 (57–78) | Patients with acute COPD exacerbation, with mean weight of 76 ± 7 kg, and height of 162 ± 13 cm. All patients underwent baseline spirometry and received standard COPD management including bronchodilators, corticosteroids, oxygen, and antibiotics. | A 20 min intravenous infusion of 1.5 g of magnesium sulfate dissolved in 100 mL of 0.9% saline solution. |
| Solooki 2014 [10] | 15 | 15 | 21 | 9 | NR | NR | RCT | Emergency department | 68.5 ± 9.06 | Patients with acute COPD exacerbation, with mean pretreatment FEV1 of 26% ± 12 in the intervention group and 35% ± 18 in the control group. | 2 g magnesium sulfate diluted in 100 mL normal saline infused over 20 min was administered |
| Nouira 2014 [11] | 62 | 62 | 95 | 29 | 58 | 52 | RCT | Emergency department | 69.06 ± 8.21 | Patients with acute COPD exacerbation. Common comorbidities included arterial hypertension, left heart failure, and diabetes. Participants had a mean COPD duration of ~10–13 years and were mostly current smokers. | 150 mg of magnesium sulfate in 4 mL of normal saline via aerosol mask (driven by pressurized air at 10 L/min), along with an intravenous bolus of 1.5 g magnesium sulfate in 10 mL. |
| Mukerji 2015 [12] | 14 | 19 | 24 | 9 | 4 | 5 | RCT | Emergency department | 74.29 ± 10.82 | Patients with acute exacerbation of COPD with mean pack years of 40 ± 27.9 years in intervention group and 38.8 ± 18.2 years in control group. | 2 g of intravenous magnesium sulfate diluted in 20 mL of 0.9% saline, administered over 15 min. |
| Jahanian 2021 [13] | 30 | 30 | 14 | 46 | 16 | 17 | RCT | Emergency department | 64.35 ± 5.61 | Patients with acute exacerbation of COPD presenting to emergency department with similar baseline FEV1 52.56 ± 6.66 in intevention group and 50.90 ± 7 incontrol group. | IV infusion of magnesium sulfate (2 gr in 100 mL of normal saline) over 30 min. |
| Moradi 2020 [14] | 39 | 38 | NR | NR | NR | NR | RCT | Emergency department | NR | Patients with acute exacerbation of COPD with no significant differences in age, sex, vital signs, PEFR, and DSS | 2.5 g of MgSO4 (5 mL of 50% solution) in 50 mL of normal saline over 15 min. |
| Aishwarya 2022 [16] | 50 | 50 | NR | NR | NR | NR | Observational | Inpatient | NR | Patients with acute exacerbation of COPD with pretreatment PEFR of 171.2 ± 44.03 in intervention group and 168 ± 40.33 in control group. | IV MgSO4 2 g in 100 mL of normal saline slowly over a period of 20–30 min. |
| Selvam 2024 [15] | 30 | 30 | 36 | 24 | 14 | 12 | Observational | Emergency department | 58.33 ± 9.66 | Patients with acute exacerbation of COPD had a mean exacerbation frequency of 1.47 ± 1.41 in the MgSO4 group and 1.37 ± 1.07 in the placebo group over the past year. | A single dose of intravenous MgSO4 infusion 2 g in 100 mL of normal saline slowly infused over a period of 20–30 min |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Farid, T.; Omar, A.S.; Kandi, S.V.; Maliyekal, S.P.; Tuen, T.Q.; Vijayan, A.T.; Pillai, L.S.; Deiab, A.T.; Sajid, M.; Mesmar, A.; et al. Intravenous Magnesium Sulphate as an Adjuvant Therapy for Acute Exacerbations of Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis. Life 2025, 15, 973. https://doi.org/10.3390/life15060973
Farid T, Omar AS, Kandi SV, Maliyekal SP, Tuen TQ, Vijayan AT, Pillai LS, Deiab AT, Sajid M, Mesmar A, et al. Intravenous Magnesium Sulphate as an Adjuvant Therapy for Acute Exacerbations of Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis. Life. 2025; 15(6):973. https://doi.org/10.3390/life15060973
Chicago/Turabian StyleFarid, Taimur, Abdousamad Said Omar, Sijah Varar Kandi, Soja Puthiyara Maliyekal, Tze Quan Tuen, Amrutha Thazhuthedath Vijayan, Lakshmi Sudhir Pillai, Ahmed Talaat Deiab, Muhammad Sajid, Ahmad Mesmar, and et al. 2025. "Intravenous Magnesium Sulphate as an Adjuvant Therapy for Acute Exacerbations of Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis" Life 15, no. 6: 973. https://doi.org/10.3390/life15060973
APA StyleFarid, T., Omar, A. S., Kandi, S. V., Maliyekal, S. P., Tuen, T. Q., Vijayan, A. T., Pillai, L. S., Deiab, A. T., Sajid, M., Mesmar, A., Hassan, E. I. E., Keethadath, R., Al Chalabi, H., Hashmi, T. M., Ahmed, M., & Ahmed, R. (2025). Intravenous Magnesium Sulphate as an Adjuvant Therapy for Acute Exacerbations of Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis. Life, 15(6), 973. https://doi.org/10.3390/life15060973