

The Effects of Abdominal Draw-In Maneuvers Combined with Blood Flow Restriction on the Transverse Abdominis in University Students with Sedentary Lifestyles


Abstract
1. Introduction
2. Materials and Methods
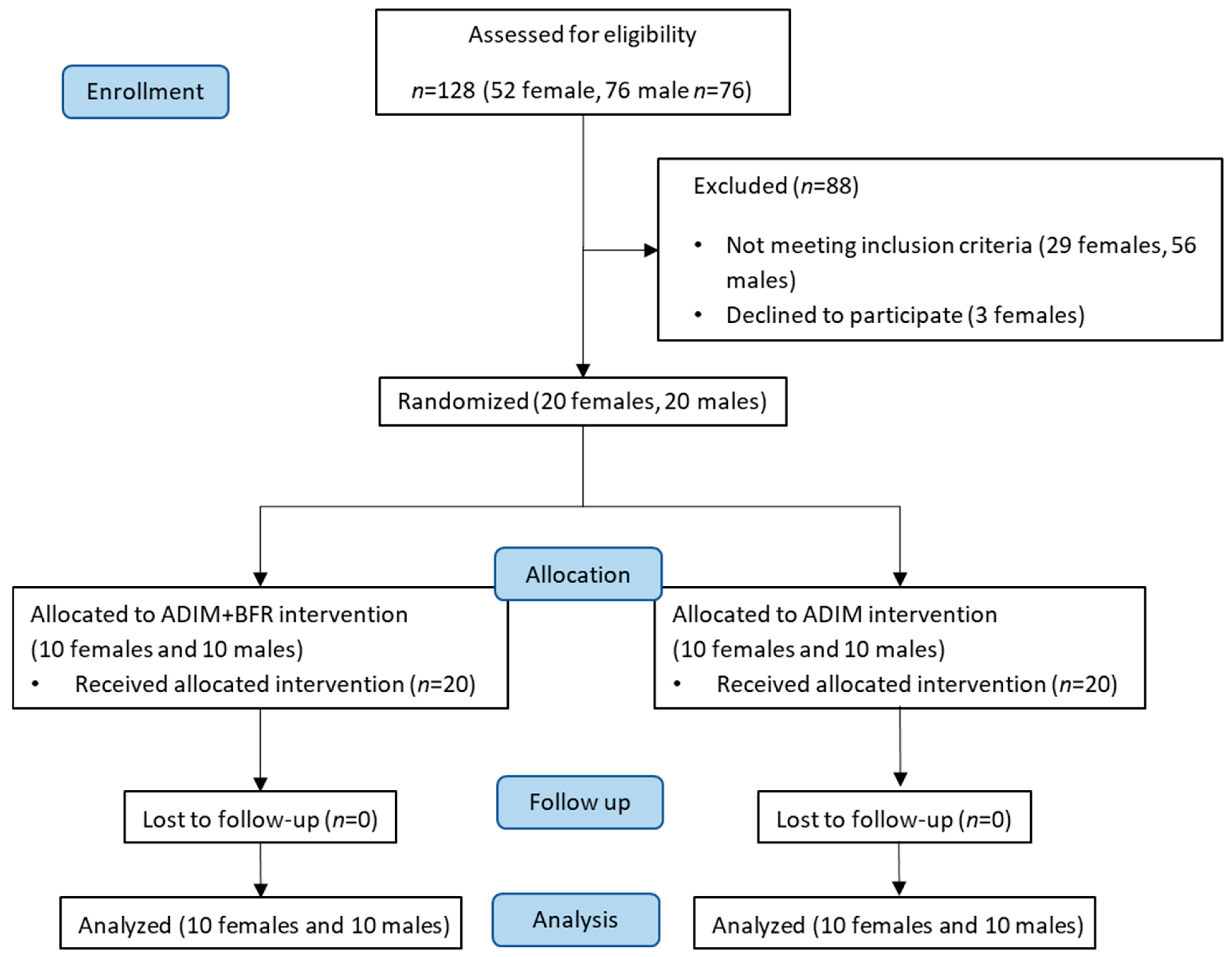
2.1. Participants and Study Design
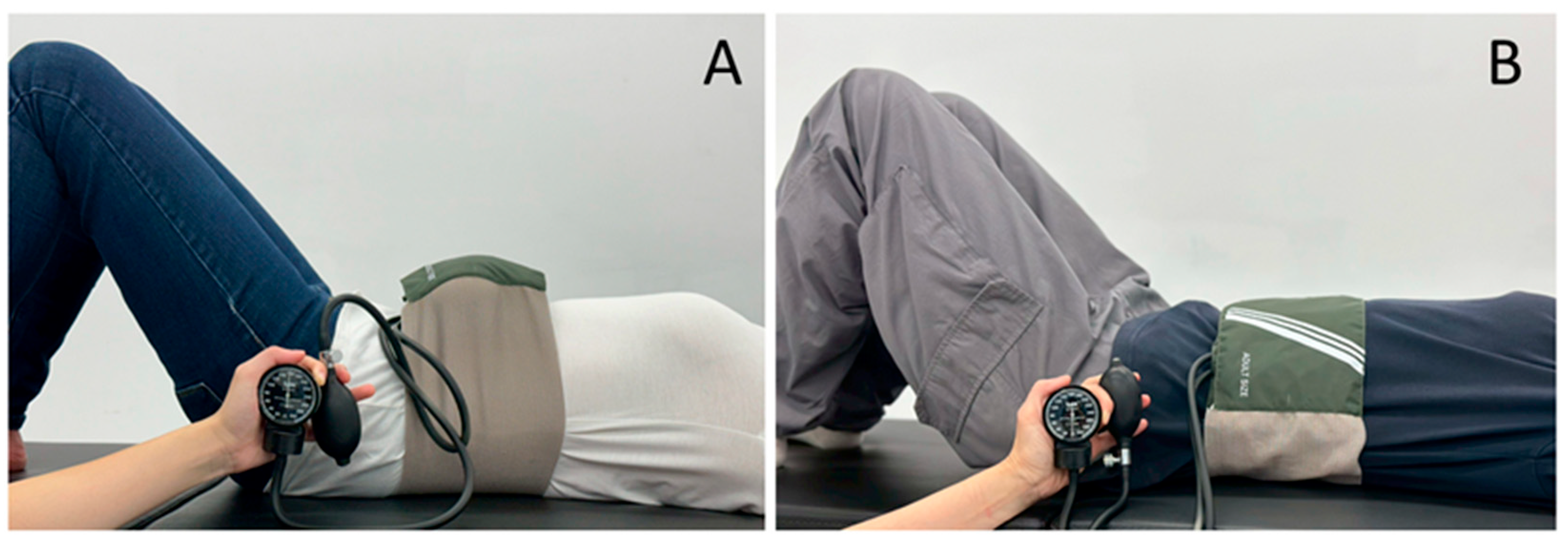
2.2. Intervention
2.2.1. Abdominal Drawing-In Maneuver
2.2.2. Combined Abdominal Drawing-In Maneuver and Blood Flow Restriction Training
2.3. Outcome Measurements
2.3.1. Demographics
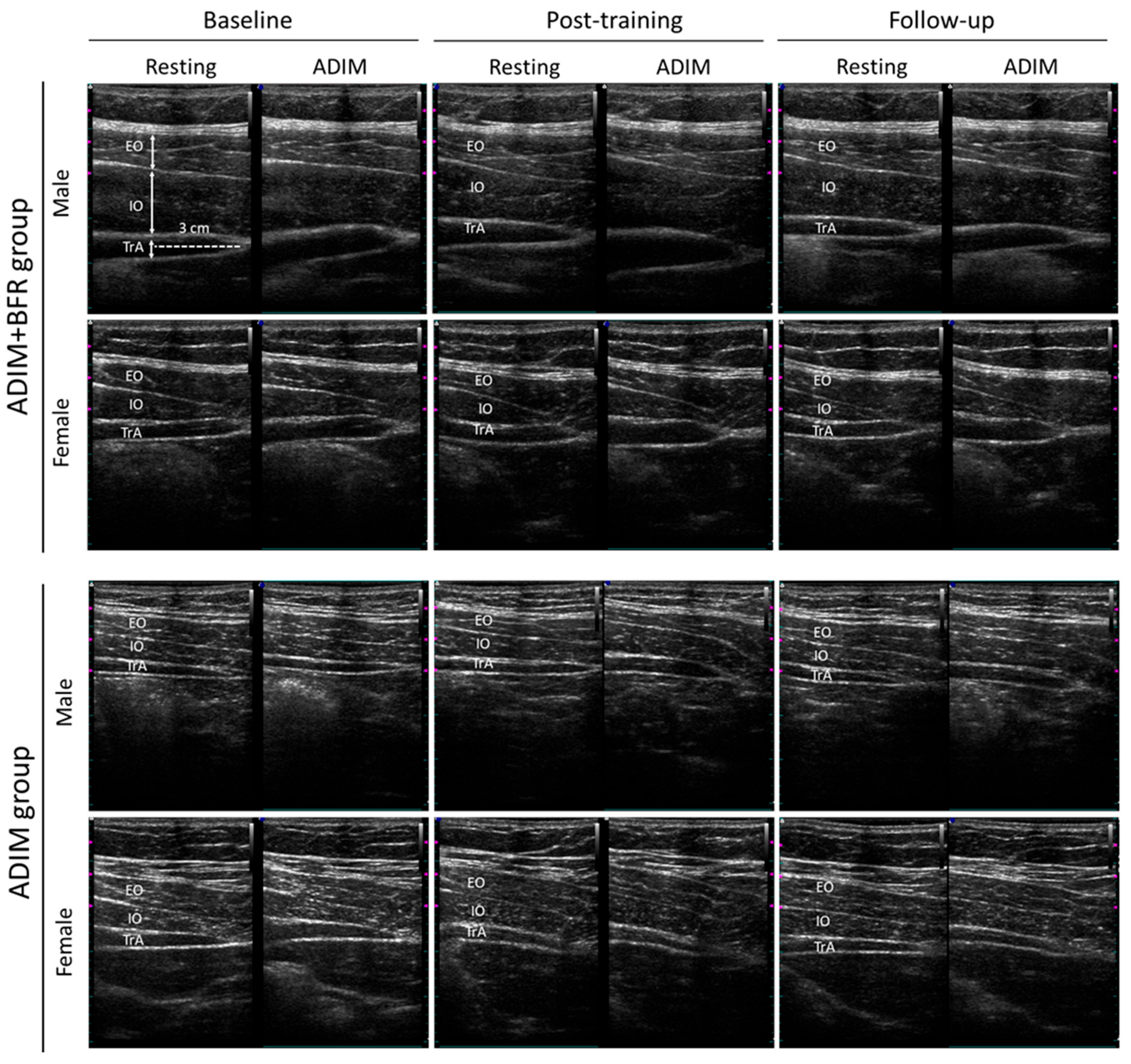
2.3.2. Ultrasound Image Analysis
2.3.3. Abdominal Muscle Performance Assessments
- Double Leg Lowering Test
- Abdominal Muscle Strength Test
- Abdominal Endurance Test
- Statistical Analysis
3. Results
3.1. Demographic Characteristics
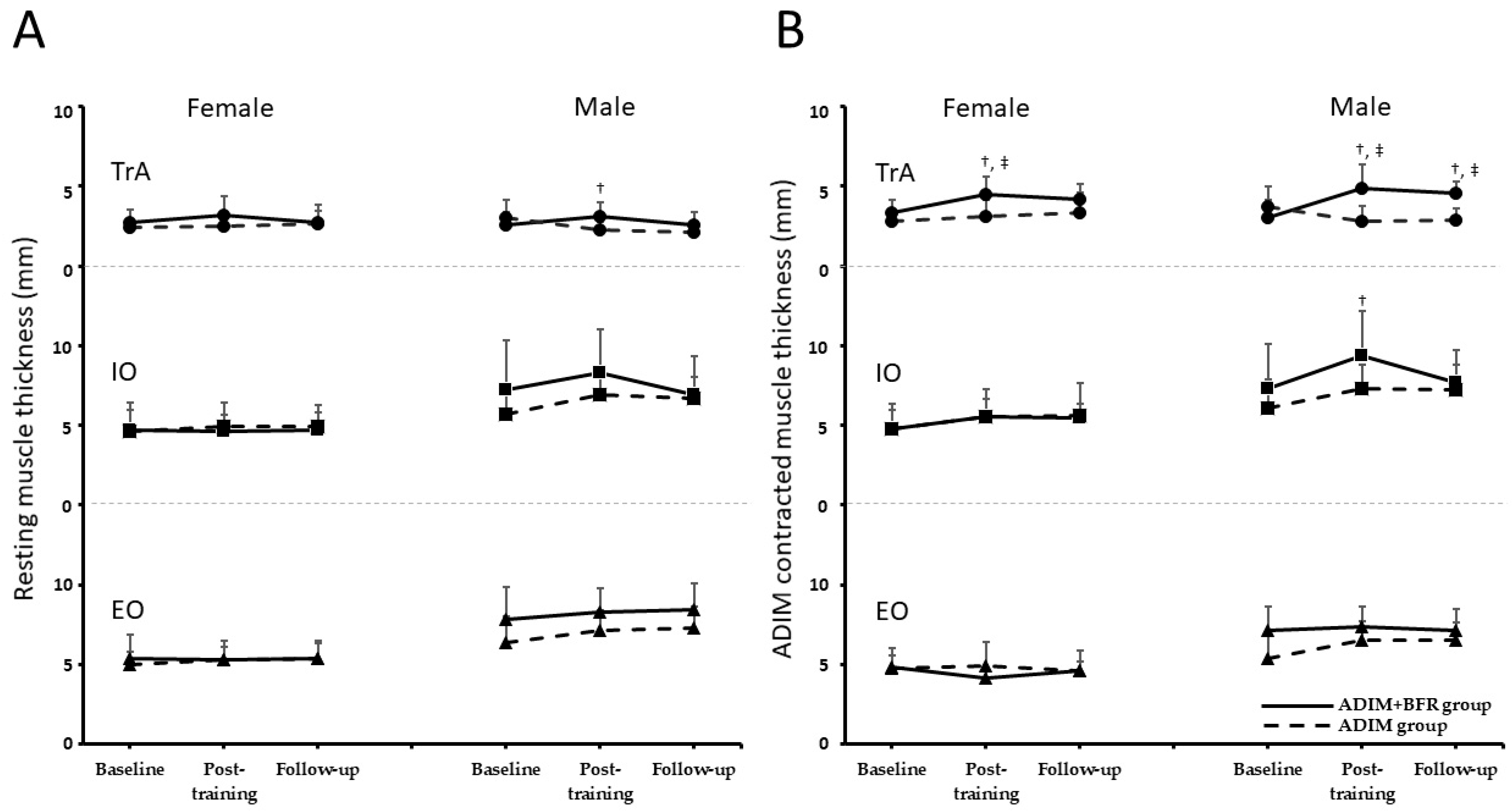
3.2. Alternations in Muscle Thickness at Baseline, Post-Training, and at Follow-Up
3.3. Contraction Ratio, Contraction Difference, and Preferential Activation Ratio
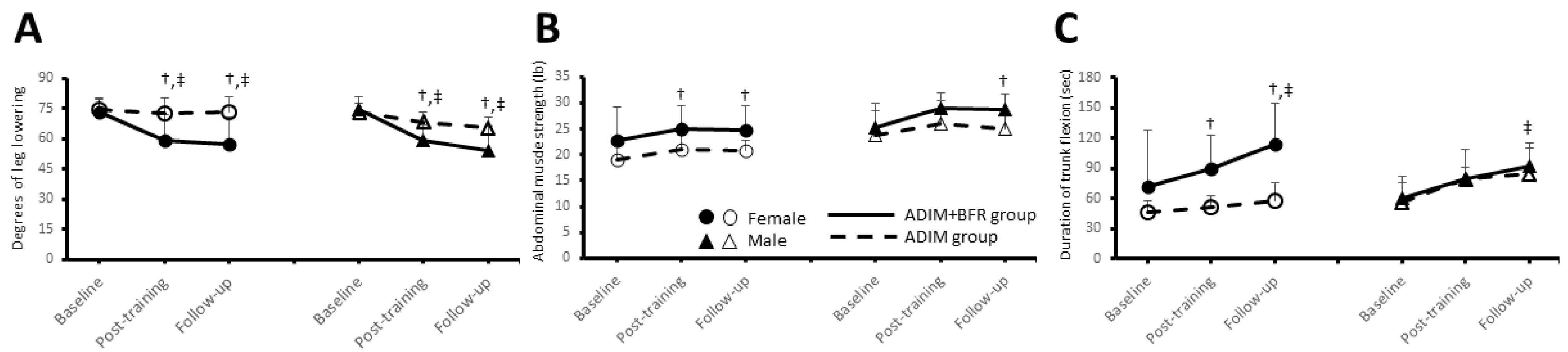
3.4. Abdominal Muscle Performances
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ADIM | abdominal drawing-in maneuver |
| AET | abdominal endurance test |
| AMST | abdominal muscle strength test |
| BFR | blood flow restriction |
| CR | contraction ratio |
| Diff | difference in contraction thickness |
| DLLT | double leg lowering test |
| EO | external oblique |
| ICC | intraclass correlation coefficient |
| IO | internal oblique |
| PAR | preferential activation ratio |
| TrA | transversus abdominis |
References
- Rouse, P.C.; Biddle, S.J.H. An ecological momentary assessment of the physical activity and sedentary behaviour patterns of university students. Health Educ. J. 2010, 69, 116–125. [Google Scholar] [CrossRef]
- Farinola, M.; Bazan, N. Sedentary behavior and physical activity in university students: A pilot study. Rev. Argent. Cardiol. 2011, 79, 351–354. [Google Scholar]
- Carballo-Fazanes, A.; Rico-Díaz, J.; Barcala-Furelos, R.; Rey, E.; Rodríguez-Fernández, J.E.; Varela-Casal, C.; Abelairas-Gómez, C. Physical Activity Habits and Determinants, Sedentary Behaviour and Lifestyle in University Students. Int. J. Environ. Res. Public Health 2020, 17, 3272. [Google Scholar] [CrossRef] [PubMed]
- Moulin, M.S.; Irwin, J.D. An Assessment of Sedentary Time Among Undergraduate Students at a Canadian University. Int. J. Exerc. Sci. 2016, 10, 1116–1129. [Google Scholar] [CrossRef]
- Areeudomwong, P.; Puntumetakul, R.; Kaber, D.B.; Wanpen, S.; Leelayuwat, N.; Chatchawan, U. Effects of handicraft sitting postures on lower trunk muscle fatigue. Ergonomics 2012, 55, 693–703. [Google Scholar] [CrossRef]
- Saiklang, P.; Puntumetakul, R.; Chatprem, T. The Effect of Core Stabilization Exercise with the Abdominal Drawing-in Maneuver Technique on Stature Change during Prolonged Sitting in Sedentary Workers with Chronic Low Back Pain. Int. J. Environ. Res. Public Health 2022, 19, 1904. [Google Scholar] [CrossRef]
- Ghowsi, M.; Qalekhani, F.; Farzaei, M.H.; Mahmudii, F.; Yousofvand, N.; Joshi, T. Inflammation, oxidative stress, insulin resistance, and hypertension as mediators for adverse effects of obesity on the brain: A review. Biomedicine 2021, 11, 13–22. [Google Scholar] [CrossRef]
- Panjabi, M.M. Clinical spinal instability and low back pain. J. Electromyogr. Kinesiol. 2003, 13, 371–379. [Google Scholar] [CrossRef]
- Kavcic, N.; Grenier, S.; McGill, S.M. Determining the Stabilizing Role of Individual Torso Muscles During Rehabilitation Exercises. Spine 2004, 29, 1254–1265. [Google Scholar] [CrossRef]
- Tsartsapakis, I.; Pantazi, G.A.; Konstantinidou, A.; Zafeiroudi, A.; Kellis, E. Spinal Muscle Thickness and Activation during Abdominal Hollowing and Bracing in CrossFit(®) Athletes. Sports 2023, 11, 159. [Google Scholar] [CrossRef]
- Leonard, J.H.; Paungmali, A.; Sitilertpisan, P.; Pirunsan, U.; Uthaikhup, S. Changes in Transversus Abdominis Muscle Thickness after Lumbo-Pelvic Core Stabilization Training among Chronic Low Back Pain Individuals. Clin. Ter. 2015, 166, e312–e316. [Google Scholar] [PubMed]
- Lee, N.G.; You, J.S.; Kim, T.H.; Choi, B.S. Unipedal postural stability in nonathletes with core instability after intensive abdominal drawing-in maneuver. J. Athl. Train. 2015, 50, 147–155. [Google Scholar] [CrossRef] [PubMed]
- Henry, S.M.; Westervelt, K.C. The use of real-time ultrasound feedback in teaching abdominal hollowing exercises to healthy subjects. J. Orthop. Sports Phys. Ther. 2005, 35, 338–345. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.S.; Seok, C.H.; Jeon, H.S. Abdominal draw-in maneuver combined with simulated weight bearing increases transversus abdominis and internal oblique thickness. Physiother. Theory Pract. 2017, 33, 954–958. [Google Scholar] [CrossRef]
- ShahAli, S.; Shanbehzadeh, S.; ShahAli, S.; Ebrahimi Takamjani, I. Application of Ultrasonography in the Assessment of Abdominal and Lumbar Trunk Muscle Activity in Participants With and Without Low Back Pain: A Systematic Review. J. Manip. Physiol. Ther. 2019, 42, 541–550. [Google Scholar] [CrossRef]
- Slysz, J.; Stultz, J.; Burr, J.F. The efficacy of blood flow restricted exercise: A systematic review & meta-analysis. J. Sci. Med. Sport 2016, 19, 669–675. [Google Scholar]
- Scott, B.R.; Loenneke, J.P.; Slattery, K.M.; Dascombe, B.J. Exercise with blood flow restriction: An updated evidence-based approach for enhanced muscular development. Sports Med. 2015, 45, 313–325. [Google Scholar] [CrossRef]
- Lee, E.; Kim, Y. Effect of university students’ sedentary behavior on stress, anxiety, and depression. Perspect. Psychiatr. Care 2019, 55, 164–169. [Google Scholar] [CrossRef]
- Park, D.J.; Lee, S.K. What is a Suitable Pressure for the Abdominal Drawing-in Maneuver in the Supine Position Using a Pressure Biofeedback Unit? J. Phys. Ther. Sci. 2013, 25, 527–530. [Google Scholar] [CrossRef]
- Xu, C.; Fu, Z.; Wang, X. Effect of Transversus abdominis muscle training on pressure-pain threshold in patients with chronic low Back pain. BMC Sports Sci. Med. Rehabil. 2021, 13, 35. [Google Scholar] [CrossRef]
- Pulkovski, N.; Mannion, A.F.; Caporaso, F.; Toma, V.; Gubler, D.; Helbling, D.; Sprott, H. Ultrasound assessment of transversus abdominis muscle contraction ratio during abdominal hollowing: A useful tool to distinguish between patients with chronic low back pain and healthy controls? Eur. Spine J. 2012, 21 (Suppl. 6), S750–S759. [Google Scholar] [CrossRef] [PubMed]
- Teyhen, D.S.; Miltenberger, C.E.; Deiters, H.M.; Del Toro, Y.M.; Pulliam, J.N.; Childs, J.D.; Boyles, R.E.; Flynn, T.W. The use of ultrasound imaging of the abdominal drawing-in maneuver in subjects with low back pain. J. Orthop. Sports Phys. Ther. 2005, 35, 346–355. [Google Scholar] [CrossRef] [PubMed]
- Sharrock, C.; Cropper, J.; Mostad, J.; Johnson, M.; Malone, T. A pilot study of core stability and athletic performance: Is there a relationship? Int. J. Sports Phys. Ther. 2011, 6, 63–74. [Google Scholar] [PubMed]
- McGill, S.M.; Childs, A.; Liebenson, C. Endurance times for low back stabilization exercises: Clinical targets for testing and training from a normal database. Arch. Phys. Med. Rehabil. 1999, 80, 941–944. [Google Scholar] [CrossRef]
- Huxel Bliven, K.C.; Anderson, B.E. Core stability training for injury prevention. Sports Health 2013, 5, 514–522. [Google Scholar] [CrossRef]
- Urquhart, D.M.; Hodges, P.W.; Allen, T.J.; Story, I.H. Abdominal muscle recruitment during a range of voluntary exercises. Man. Ther. 2005, 10, 144–153. [Google Scholar] [CrossRef]
- Kumar, S.P. Efficacy of segmental stabilization exercise for lumbar segmental instability in patients with mechanical low back pain: A randomized placebo controlled crossover study. N. Am. J. Med. Sci. 2011, 3, 456–461. [Google Scholar] [CrossRef]
- Javadian, Y.; Behtash, H.; Akbari, M.; Taghipour-Darzi, M.; Zekavat, H. The effects of stabilizing exercises on pain and disability of patients with lumbar segmental instability. J. Back. Musculoskelet. Rehabil. 2012, 25, 149–155. [Google Scholar] [CrossRef]
- Shimizu, I.; Miaki, H.; Mizuno, K.; Azuma, N.; Nakagawa, T.; Yamazaki, T. Contributions of muscle elasticity and lateral slide of the transversus abdominis to lumbar stability. J. Sport Rehabil. 2020, 30, 582–586. [Google Scholar] [CrossRef]
- Abe, T.; Kearns, C.F.; Sato, Y. Muscle size and strength are increased following walk training with restricted venous blood flow from the leg muscle, Kaatsu-walk training. J. Appl. Physiol. 2006, 100, 1460–1466. [Google Scholar] [CrossRef]
- Pearson, S.J.; Hussain, S.R. A review on the mechanisms of blood-flow restriction resistance training-induced muscle hypertrophy. Sports Med. 2015, 45, 187–200. [Google Scholar] [CrossRef] [PubMed]
- Yasuda, T.; Ogasawara, R.; Sakamaki, M.; Ozaki, H.; Sato, Y.; Abe, T. Combined effects of low-intensity blood flow restriction training and high-intensity resistance training on muscle strength and size. Eur. J. Appl. Physiol. 2011, 111, 2525–2533. [Google Scholar] [CrossRef] [PubMed]
- Arvanitidis, M.; Jiménez-Grande, D.; Haouidji-Javaux, N.; Falla, D.; Martinez-Valdes, E. Low Back Pain-Induced Dynamic Trunk Muscle Control Impairments Are Associated with Altered Spatial EMG-Torque Relationships. Med. Sci. Sports Exerc. 2024, 56, 193–208. [Google Scholar] [CrossRef] [PubMed]
- Rivera, C.E. Core and Lumbopelvic Stabilization in Runners. Phys. Med. Rehabil. Clin. N. Am. 2016, 27, 319–337. [Google Scholar] [CrossRef]
- Panjabi, M.M. The stabilizing system of the spine. Part I. Function, dysfunction, adaptation, and enhancement. J. Spinal Disord. 1992, 5, 383–389; discussion 397. [Google Scholar] [CrossRef]
- Hodges, P.W.; Richardson, C.A. Inefficient muscular stabilization of the lumbar spine associated with low back pain. A motor control evaluation of transversus abdominis. Spine 1996, 21, 2640–2650. [Google Scholar] [CrossRef]
- Dülger, E.; Bilgin, S.; Karakaya, J.; Soylu, A.R. Comparison of two different feedback techniques for activating the transversus abdominis: An observational study. J. Back Musculoskelet. Rehabil. 2022, 35, 357–361. [Google Scholar] [CrossRef]
- Hibbs, A.E.; Thompson, K.G.; French, D.; Wrigley, A.; Spears, I. Optimizing performance by improving core stability and core strength. Sports Med. 2008, 38, 995–1008. [Google Scholar] [CrossRef]
- Comerford, M.J.; Mottram, S.L. Movement and stability dysfunction--contemporary developments. Man. Ther. 2001, 6, 15–26. [Google Scholar] [CrossRef]
- Kojić, F.; Mandić, D.; Ilić, V. Resistance training induces similar adaptations of upper and lower-body muscles between sexes. Sci. Rep. 2021, 11, 23449. [Google Scholar] [CrossRef]
- Landen, S.; Hiam, D.; Voisin, S.; Jacques, M.; Lamon, S.; Eynon, N. Physiological and molecular sex differences in human skeletal muscle in response to exercise training. J. Physiol. 2023, 601, 419–434. [Google Scholar] [CrossRef] [PubMed]
- MacGregor, K.; Ellefsen, S.; Pillon, N.J.; Hammarström, D.; Krook, A. Sex differences in skeletal muscle metabolism in exercise and type 2 diabetes mellitus. Nat. Rev. Endocrinol. 2025, 21, 166–179. [Google Scholar] [CrossRef] [PubMed]
- Nuzzo, J.L. Sex differences in skeletal muscle fiber types: A meta-analysis. Clin. Anat. 2024, 37, 81–91. [Google Scholar] [CrossRef] [PubMed]
- Otsuki, R.; Del Bel, M.J.; Benoit, D.L. Sex differences in muscle activation patterns associated with anterior cruciate ligament injury during landing and cutting tasks: A systematic review. J. Electromyogr. Kinesiol. 2021, 60, 102583. [Google Scholar] [CrossRef]
- Roberts, B.M.; Nuckols, G.; Krieger, J.W. Sex Differences in Resistance Training: A Systematic Review and Meta-Analysis. J. Strength Cond. Res. 2020, 34, 1448–1460. [Google Scholar] [CrossRef]
- Yagi, M.; Taniguchi, M.; Tateuchi, H.; Hirono, T.; Fukumoto, Y.; Yamagata, M.; Nakai, R.; Yamada, Y.; Kimura, M.; Ichihashi, N. Age-and sex-related differences of muscle cross-sectional area in iliocapsularis: A cross-sectional study. BMC Geriatr. 2022, 22, 435. [Google Scholar]
- Labarbera, K.E.; Murphy, B.G.; Laroche, D.P.; Cook, S.B. Sex differences in blood flow restricted isotonic knee extensions to fatigue. J. Sports Med. Phys. Fit. 2013, 53, 444–452. [Google Scholar]
- Spitz, R.W.; Wong, V.; Bell, Z.W.; Viana, R.B.; Chatakondi, R.N.; Abe, T.; Loenneke, J.P. Blood Flow Restricted Exercise and Discomfort: A Review. J. Strength Cond. Res. 2022, 36, 871–879. [Google Scholar] [CrossRef]
- Nakajima, T.; Kurano, M.; Iida, H.; Takano, H.; Oonuma, H.; Morita, T.; Meguro, K.; Sato, Y.; Nagata, T. Use and safety of KAATSU training: Results of a national survey. Int. J. KAATSU Train. Res. 2006, 2, 5–13. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ADIM + BFR | ADIM | |||
|---|---|---|---|---|
| Female | Male | Female | Male | |
| Number | 10 | 10 | 10 | 10 |
| Age (years) | 22.5 ± 3.5 | 22.2 ± 2.2 | 22.8 ± 3.4 | 23.8 ± 3.1 |
| Weight (kg) | 54.4 ± 13.9 | 71.5 ± 9.1 | 52.9 ± 7.5 | 72.9 ± 9.5 |
| Height (cm) | 165.8 ± 4.2 | 175.2 ± 5.3 | 163.8 ± 2.2 | 177.2 ± 7.3 |
| BMI | 22.4 ± 4.1 | 24.1 ± 2.2 | 21.4 ± 3.5 | 23.42 |
| Sedentary behavior (minutes/day) | 885.64 ± 239.84 | 871.02 ± 266.52 | 866.35 ± 271.13 | 874.92 ± 285.21 |
| Duration of regular exercise (minutes/week) | 26.00 ± 23.16 | 34.00 ± 16.27 | 29.50 ± 18.19 | 30.00 ± 19.80 |
| Within-Subjects Comparison | Between-Subjects Comparison | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Data Collection Points (Time) | Time | Time × Group | Time × Gender | Time × Group × Gender | Group | Gender | Group × Gender | |||||||
| Muscle | Action | Group | Gender | N | Baseline | Post-Training | Follow-Up | F Value | F Value | F Value | F Value | F Value | F Value | F Value |
| EO | ADIM | ADIM+BFR | F | 10 | 4.81 ± 1.23 | 4.12 ± 0.47 | 4.57 ± 0.63 | 0.79 | 2.82 | 3.35 | 1.11 | 1.58 | 43.87 * | 4.59 * |
| M | 10 | 7.10 ± 1.54 | 7.34 ± 1.27 | 7.10 ± 1.39 | ||||||||||
| ADIM | F | 10 | 4.74 ± 0.82 | 4.92 ± 1.45 | 4.64 ± 1.20 | |||||||||
| M | 10 | 6.39 ± 1.41 | 6.51 ± 1.21 | 6.52 ± 1.14 | ||||||||||
| Resting | ADIM+BFR | F | 10 | 5.35 ± 1.51 | 5.26 ± 0.86 | 5.38 ± 0.93 | 4.02 * | 0.49 | 1.68 | 0.02 | 3.07 | 35.19 * | 2.27 | |
| M | 10 | 7.19 ± 1.09 | 8.29 ± 1.48 | 8.43 ± 1.67 | ||||||||||
| ADIM | F | 10 | 5.03 ± 0.76 | 5.31 ± 1.17 | 5.37 ± 1.13 | |||||||||
| M | 10 | 6.37 ± 1.63 | 7.10 ± 1.29 | 7.31 ± 1.34 | ||||||||||
| IO | ADIM | ADIM+BFR | F | 10 | 4.75 ± 1.56 | 5.52 ± 1.14 | 5.45 ± 0.90 | 12.13 * | 1.73 | 1.98 | 1.15 | 1.26 | 19.04 * | 1.65 |
| M | 10 | 7.32 ± 1.82 | 9.35 ± 1.80 ‡ | 7.67 ± 1.01 | ||||||||||
| ADIM | F | 10 | 4.77 ± 1.21 | 5.55 ± 1.68 | 5.65 ± 1.00 | |||||||||
| M | 10 | 6.11 ± 1.80 | 7.29 ± 1.54 | 7.27 ± 1.54 | ||||||||||
| Resting | ADIM+BFR | F | 10 | 4.70 ± 1.76 | 4.60 ± 1.07 | 4.70 ± 1.08 | 3.45 * | 1.45 | 2.63 | 1.07 | 0.75 | 17.89 * | 1.41 | |
| M | 10 | 7.25 ± 1.09 | 8.34 ± 1.66 | 6.93 ± 1.41 | ||||||||||
| ADIM | F | 10 | 4.64 ± 1.35 | 4.95 ± 1.51 | 4.91 ± 1.38 | |||||||||
| M | 10 | 6.68 ± 1.93 | 7.90 ± 1.69 | 6.70 ± 1.36 | ||||||||||
| TrA | ADIM | ADIM+BFR | F | 10 | 3.37 ± 0.78 | 4.46 ± 1.16 †,‡ | 4.17 ± 0.98 | 6.96 * | 14.34 * | 0.48 | 5.82 * | 14.17 * | 0.23 | 0.05 |
| M | 10 | 3.07 ± 1.08 | 4.90 ± 1.50 †,‡ | 4.57 ± 0.71 †,‡ | ||||||||||
| ADIM | F | 10 | 2.80 ± 0.36 | 3.12 ± 1.05 | 3.33 ± 1.26 | |||||||||
| M | 10 | 2.73 ± 1.25 | 2.82 ± 0.95 | 2.91 ± 0.70 | ||||||||||
| Resting | ADIM+BFR | F | 10 | 2.76 ± 0.78 | 3.19 ± 1.16 | 2.70 ± 1.11 | 2.21 | 5.28 * | 2.66 | 3.39 * | 2.30 | 0.12 | 0.04 | |
| M | 10 | 2.59 ± 0.81 | 3.10 ± 0.88 † | 2.60 ± 0.82 | ||||||||||
| ADIM | F | 10 | 2.39 ± 0.46 | 2.51 ± 0.74 | 2.62 ± 0.86 | |||||||||
| M | 10 | 3.06 ± 1.05 | 2.24 ± 0.52 | 2.10 ± 0.55 | ||||||||||
| Within-Subjects Comparison | Between-Subjects Comparison | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Data Collection Time Points | Time | Time × Group | Time × Gender | Time × Gender × Group | Group | Gender | Group × Gender | |||||||
| Index | Muscle | Group | Gender | N | Baseline | Post-Training | Follow-Up | F Value | F Value | F Value | F Value | F Value | F Value | F Value |
| CR | EO | ADIM+BFR | F | 10 | 0.91 ± 0.11 | 0.79 ± 0.11 ‡ | 0.86 ± 0.09 | 2.28 | 2.76 | 2.76 | 2.40 | 1.03 | 0.12 | 1.27 |
| M | 10 | 0.93 ± 0.10 | 0.90 ± 0.15 | 0.85 ± 0.10 ‡ | ||||||||||
| ADIM | F | 10 | 0.95 ± 0.09 | 0.92 ± 0.15 | 0.86 ± 0.11 | |||||||||
| M | 10 | 0.85 ± 0.10 | 0.92 ± 0.06 | 0.90 ± 0.08 | ||||||||||
| IO | ADIM+BFR | F | 10 | 1.04 ± 0.18 | 1.21 ± 0.14 ‡ | 1.20 ± 0.27 ‡ | 4.46 * | 1.97 | 0.82 | 0.34 | 1.00 | 0.45 | 0.09 | |
| M | 10 | 1.03 ± 0.10 | 1.15 ± 0.23 | 1.17 ± 0.25 | ||||||||||
| ADIM | F | 10 | 1.04 ± 0.10 | 1.13 ± 0.11 | 1.14 ± 0.16 | |||||||||
| M | 10 | 1.11 ± 0.19 | 1.07 ± 0.10 | 1.09 ± 0.11 | ||||||||||
| TrA | ADIM+BFR | F | 10 | 1.24 ± 0.16 | 1.48 ± 0.42 | 1.68 ± 0.53 †,‡ | 13.54 * | 6.98 * | 0.77 | 0.45 | 12.77 * | 1.35 | 0.04 | |
| M | 10 | 1.20 ± 0.22 | 1.61 ± 0.31 †,‡ | 1.89 ± 0.53 †,‡ | ||||||||||
| ADIM | F | 10 | 1.20 ± 0.20 | 1.24 ± 0.13 | 1.26 ± 0.13 | |||||||||
| M | 10 | 1.27 ± 0.40 | 1.24 ± 0.23 | 1.39 ± 0.15 | ||||||||||
| Diff | EO | ADIM+BFR | F | 10 | 0.54 ± 0.65 | 1.14 ± 0.81 †,‡ | 0.81 ± 0.53 | 2.85 | 2.75 | 1.55 | 2.40 | 2.19 | 1.56 | 0.17 |
| M | 10 | 0.69 ± 0.76 | 0.95 ± 0.28 | 1.33 ± 0.04 ‡ | ||||||||||
| ADIM | F | 10 | 0.28 ± 0.52 | 0.39 ± 0.64 | 0.73 ± 0.59 | |||||||||
| M | 10 | 0.98 ± 0.70 | 0.58 ± 0.45 | 0.80 ± 0.71 | ||||||||||
| IO | ADIM+BFR | F | 10 | −0.05 ± 0.72 | −0.92 ± 0.59 ‡ | −0.75 ± 0.98 ‡ | 4.91 * | 1.46 | 0.23 | 0.29 | 0.37 | 0.00 | 0.03 | |
| M | 10 | −0.07 ± 0.66 | −1.01 ± 0.20 | −0.75 ± 0.33 | ||||||||||
| ADIM | F | 10 | −0.13 ± 0.49 | −0.60 ± 0.50 | −0.73 ± 0.83 | |||||||||
| M | 10 | −0.43 ± 0.83 | −0.39 ± 0.63 | −0.56 ± 0.78 | ||||||||||
| TrA | ADIM+BFR | F | 10 | −0.61 ± 0.41 | −1.27 ± 0.99 | −1.47 ± 0.92 †,‡ | 14.32 * | 8.02 * | 0.44 | 1.77 | 17.22 * | 1.72 | 0.40 | |
| M | 10 | −0.48 ± 0.66 | −1.80 ± 0.89 †,‡ | −1.97 ± 0.69 †,‡ | ||||||||||
| ADIM | F | 10 | −0.41 ± 0.40 | −0.61 ± 0.43 | −0.71 ± 0.52 | |||||||||
| M | 10 | −0.66 ± 0.60 | −0.58 ± 0.59 | −0.81 ± 0.31 | ||||||||||
| PAR | EO | ADIM+BFR | F | 10 | −0.10 ± 0.09 | −0.27 ± 0.10 †,‡ | −0.23 ± 0.10 ‡ | 11.36 * | 5.84 * | 2.52 | 1.38 | 3.87 | 0.87 | 0.92 |
| M | 10 | −0.07 ± 0.07 | −0.17 ± 0.19 ‡ | −0.22 ± 0.12 ‡ | ||||||||||
| ADIM | F | 10 | −0.08 ± 0.07 | −0.14 ± 0.10 | −0.17 ± 0.09 | |||||||||
| M | 10 | −0.15 ± 0.12 | −0.10 ± 0.07 | −0.14 ± 0.08 | ||||||||||
| IO | ADIM+BFR | F | 10 | 0.01 ± 0.15 | 0.04 ± 0.14 | 0.04 ± 0.15 | 0.98 | 1.22 | 2.40 | 1.08 | 0.12 | 0.10 | 0.28 | |
| M | 10 | 0.03 ± 0.08 | 0.05 ± 0.14 | 0.05 ± 0.14 | ||||||||||
| ADIM | F | 10 | 0.02 ± 0.07 | 0.07 ± 0.10 | 0.09 ± 0.12 | |||||||||
| M | 10 | 0.10 ± 0.16 | 0.04 ± 0.07 | 0.05 ± 0.08 | ||||||||||
| TrA | ADIM+BFR | F | 10 | 0.21 ± 0.19 | 0.37 ± 0.28 | 0.44 ± 0.30 † | 10.32 * | 5.39 * | 1.63 | 0.75 | 14.81 * | 4.70 * | 0.08 | |
| M | 10 | 0.20 ± 0.16 | 0.46 ± 0.19 †,‡ | 0.69 ± 0.28 †,‡ | ||||||||||
| ADIM | F | 10 | 0.17 ± 0.18 | 0.17 ± 0.12 | 0.21 ± 0.09 | |||||||||
| Within-Subjects Comparison | Between-Subjects Comparison | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Data Collection Time Points | Time | Time × Group | Time × Gender | Time × Gender × Group | Group | Gender | Group × Gender | ||||||
| Test | Group | Gender | N | Baseline | Post-Training | Follow-Up | F Value | F Value | F Value | F Value | F Value | F Value | F Value |
| DLLT | ADIM+BFR | F | 10 | 73.25 ± 7.36 | 59.50 ± 12.24 †,‡ | 57.50 ± 13.23 †,‡ | 36.05 * | 12.71 * | 1.84 | 0.05 | 15.52 * | 1.69 | 0.68 |
| (degree) | M | 10 | 74.25 ± 3.74 | 59.00 ± 7.75 †,‡ | 54.00 ± 12.14 †,‡ | ||||||||
| ADIM | F | 10 | 74.75 ± 4.63 | 72.50 ± 7.99 | 73.25 ± 7.46 | ||||||||
| M | 10 | 73.25 ± 7.64 | 68.25 ± 5.01 | 65.50 ± 5.50 | |||||||||
| AMST | ADIM+BFR | F | 10 | 22.81 ± 6.46 | 24.98 ± 4.61 † | 24.65 ± 4.86 † | 11.33 * | 0.55 | 0.39 | 0.35 | 8.49 * | 12.95 * | 0.22 |
| (lb) | M | 10 | 25.35 ± 4.70 | 29.04 ± 2.88 | 28.61 ± 3.14 † | ||||||||
| ADIM | F | 10 | 19.15 ± 2.88 | 21.08 ± 2.57 | 20.77 ± 2.04 | ||||||||
| M | 10 | 23.73 ± 4.81 | 26.12 ± 4.45 | 24.90 ± 3.68 | |||||||||
| AET | ADIM+BFR | F | 10 | 72.50 ± 55.08 | 89.30 ± 34.05 † | 114.00 ± 41.39 †,‡ | 31.15 * | 2.88 | 1.16 | 1.62 | 7.84 * | 0.19 | 5.17 * |
| (second) | M | 10 | 60.30 ± 21.18 | 80.00 ± 11.59 | 92.00 ± 22.79 ‡ | ||||||||
| ADIM | F | 10 | 46.30 ± 12.07 | 50.90 ± 11.99 | 58.30 ± 17.40 | ||||||||
| M | 10 | 56.30 ± 19.59 | 79.30 ± 29.96 | 84.20 ± 26.08 | |||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsieh, Y.-L.; Weng, T.-Y.; Yang, N.-P.; Lai, Y.-L.; Chien, A. The Effects of Abdominal Draw-In Maneuvers Combined with Blood Flow Restriction on the Transverse Abdominis in University Students with Sedentary Lifestyles. Life 2025, 15, 965. https://doi.org/10.3390/life15060965
Hsieh Y-L, Weng T-Y, Yang N-P, Lai Y-L, Chien A. The Effects of Abdominal Draw-In Maneuvers Combined with Blood Flow Restriction on the Transverse Abdominis in University Students with Sedentary Lifestyles. Life. 2025; 15(6):965. https://doi.org/10.3390/life15060965
Chicago/Turabian StyleHsieh, Yueh-Ling, Tzu-Yu Weng, Nian-Pu Yang, Yu-Liang Lai, and Andy Chien. 2025. "The Effects of Abdominal Draw-In Maneuvers Combined with Blood Flow Restriction on the Transverse Abdominis in University Students with Sedentary Lifestyles" Life 15, no. 6: 965. https://doi.org/10.3390/life15060965
APA StyleHsieh, Y.-L., Weng, T.-Y., Yang, N.-P., Lai, Y.-L., & Chien, A. (2025). The Effects of Abdominal Draw-In Maneuvers Combined with Blood Flow Restriction on the Transverse Abdominis in University Students with Sedentary Lifestyles. Life, 15(6), 965. https://doi.org/10.3390/life15060965