
Effects of Exercise on Dynamic Balance in People with Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis of Randomized Controlled Trials

 , and
, and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Search Strategy
2.3. Eligibility Criteria
2.4. Data Extraction
2.5. Methodological Quality Assessment
2.6. Statistical Analysis
3. Results
3.1. Study Selection
3.2. Characteristics of the Included Studies
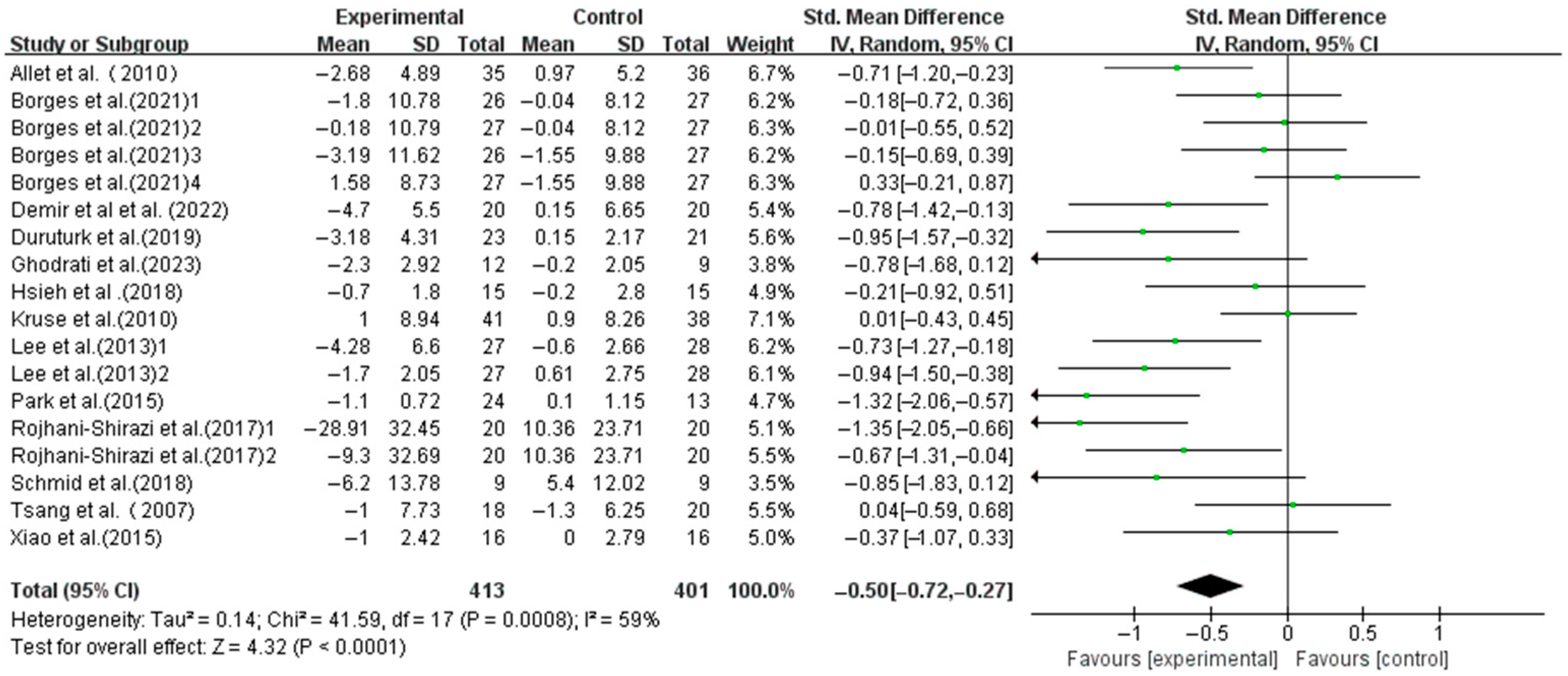
3.3. Main Effect
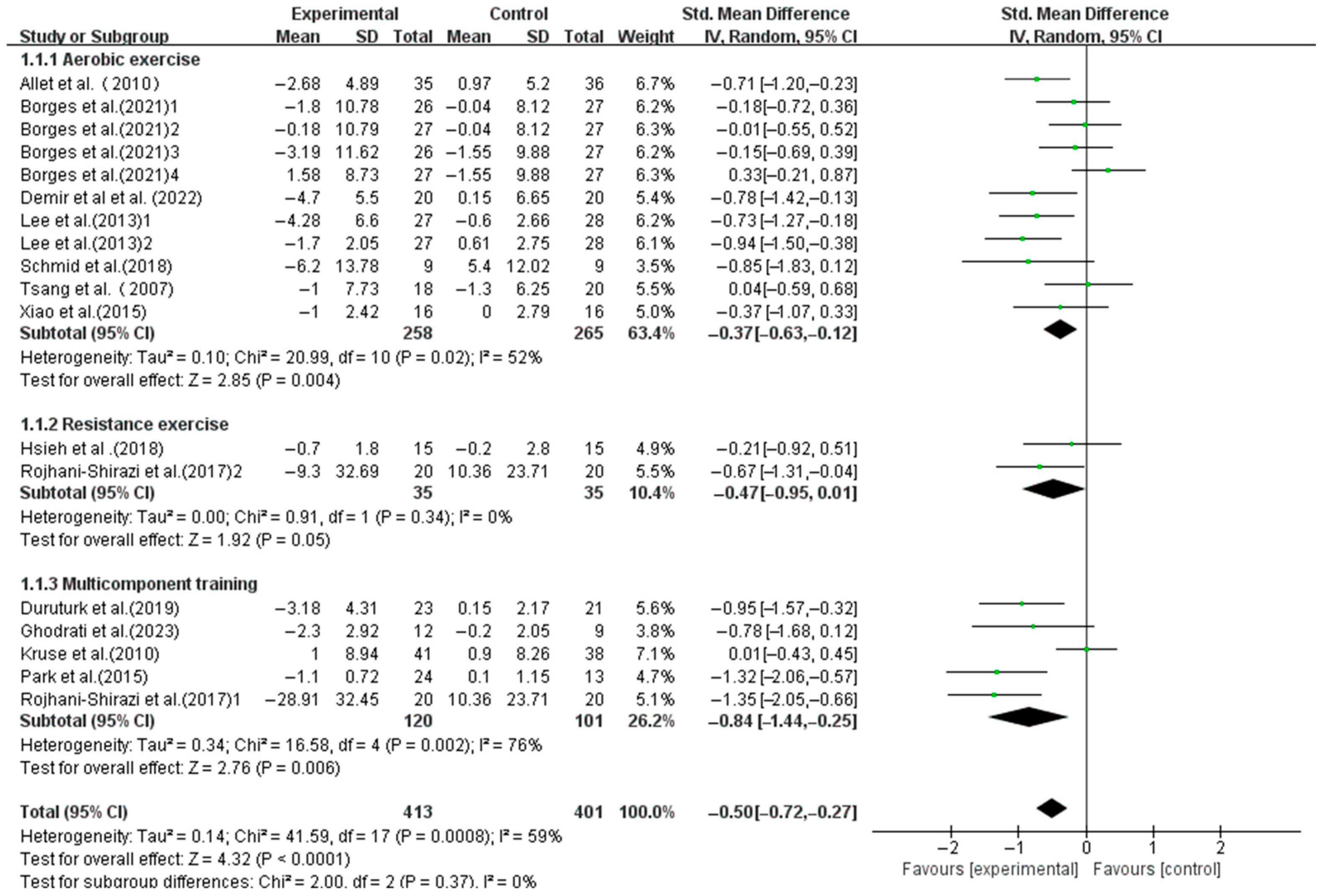
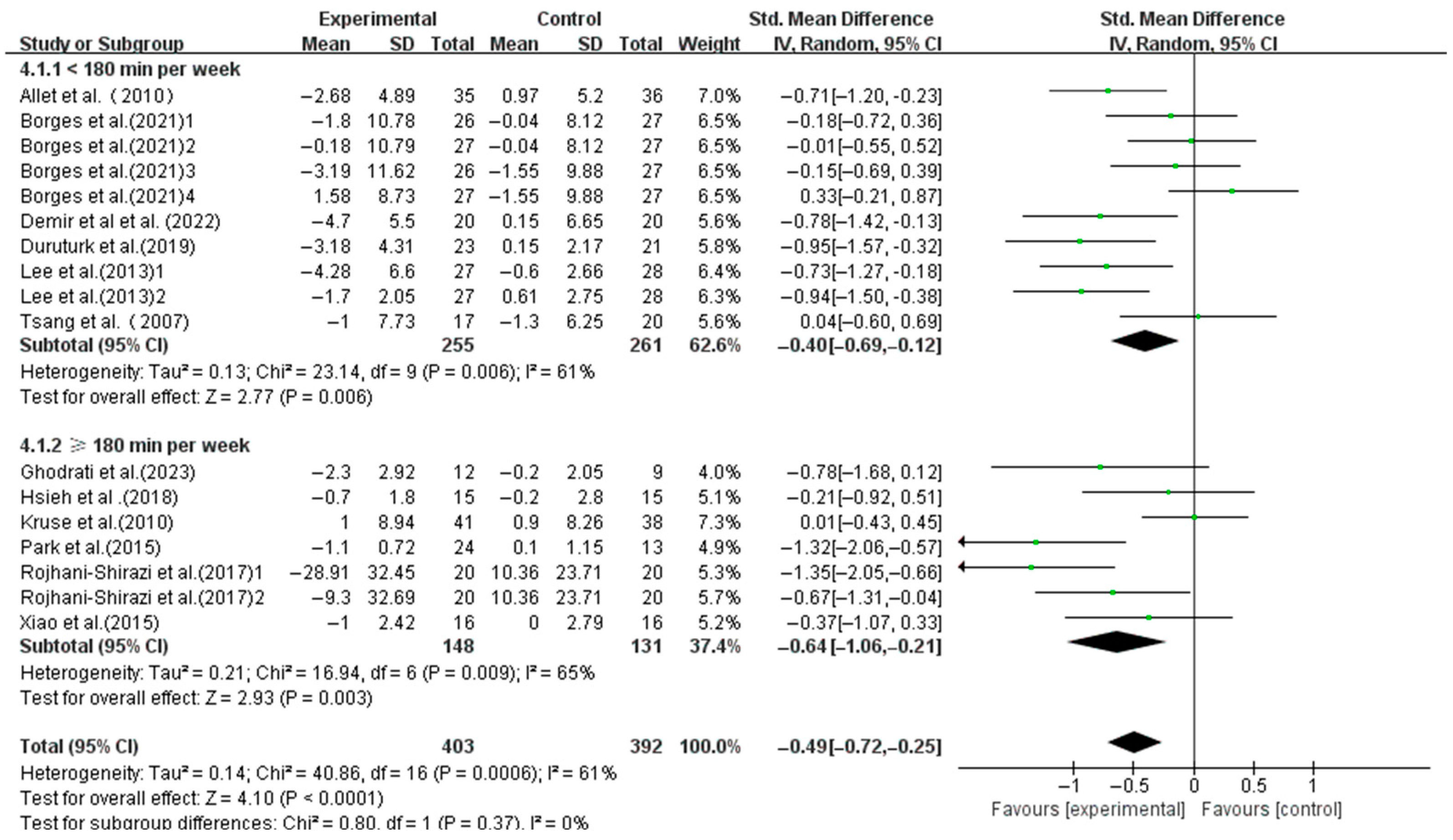
3.4. Subgroup Analysis
3.5. Meta-Regression
3.6. Risk of Bias
3.7. Publication Bias
3.8. Sensitivity Analysis
4. Discussion
4.1. Effects of Exercise on Dynamic Balance in T2DM Patients
4.2. Effects of Different Exercise Modalities on Dynamic Balance in T2DM Patients
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sun, H.; Saeedi, P.; Karuranga, S.; Pinkepank, M.; Ogurtsova, K.; Duncan, B.B.; Stein, C.; Basit, A.; Chan, J.C.N.; Mbanya, J.C.; et al. IDF Diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res. Clin. Pract. 2022, 183, 109119. [Google Scholar] [CrossRef] [PubMed]
- Cho, N.H.; Shaw, J.E.; Karuranga, S.; Huang, Y.; da Rocha Fernandes, J.D.; Ohlrogge, A.W.; Malanda, B. IDF Diabetes Atlas: Global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res. Clin. Pract. 2018, 138, 271–281. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.; Ley, S.H.; Hu, F.B. Global aetiology and epidemiology of type 2 diabetes mellitus and its complications. Nat. Rev. Endocrinol. 2018, 14, 88–98. [Google Scholar] [CrossRef]
- García-Chapa, E.G.; Leal-Ugarte, E.; Peralta-Leal, V.; Durán-González, J.; Meza-Espinoza, J.P. Genetic epidemiology of type 2 diabetes in mexican mestizos. Biomed. Res. Int. 2017, 39, 3937893. [Google Scholar] [CrossRef]
- Cole, J.B.; Florez, J.C. Genetics of diabetes mellitus and diabetes complications. Nat. Rev. Nephrol. 2020, 16, 377–390. [Google Scholar] [CrossRef]
- Feldman, E.L.; Callaghan, B.C.; Pop-Busui, R.; Zochodne, D.W.; Wright, D.E.; Bennett, D.L.; Bril, V.; Russell, J.W.; Viswanathan, V. Diabetic neuropathy. Nat. Rev. Dis. Primers. 2019, 5, 41. [Google Scholar] [CrossRef] [PubMed]
- Brognara, L.; Mazzotti, A.; Di Martino, A.; Faldini, C.; Cauli, O. Wearable Sensor for Assessing Gait and Postural Alterations in Patients with Diabetes: A Scoping Review. Medicina 2021, 57, 1145. [Google Scholar] [CrossRef]
- Kukidome, D.; Nishikawa, T.; Sato, M.; Nishi, Y.; Shimamura, R.; Kawashima, J.; Shimoda, S.; Mizuta, H.; Araki, E. Impaired balance is related to the progression of diabetic complications in both young and older adults. J. Diabetes Complicat. 2017, 31, 1275–1282. [Google Scholar] [CrossRef]
- Komalasari, D.R.; Vongsirinavarat, M.; Hiengkaew, V.; Nualnim, N. Balance performance, falls-efficacy and social participation in patients with type 2 diabetes mellitus with and without vestibular dysfunction. PeerJ 2024, 12, e17287. [Google Scholar] [CrossRef]
- Brognara, L.; Sempere-Bigorra, M.; Mazzotti, A.; Artioli, E.; Julián-Rochina, I.; Cauli, O. Wearable sensors-based postural analysis and fall risk assessment among patients with diabetic foot neuropathy. J. Tissue Viability 2023, 32, 516–526. [Google Scholar] [CrossRef]
- Freire, L.B.; Brasil-Neto, J.P.; da Silva, M.L.; Miranda, M.G.C.; de Mattos Cruz, L.; Martins, W.R.; da Silva Paz, L.P. Risk factors for falls in older adults with diabetes mellitus: Systematic review and meta-analysis. BMC Geriatr. 2024, 24, 201. [Google Scholar] [CrossRef]
- Sousa, L.M.; Marques-Vieira, C.M.; Caldevilla, M.N.; Henriques, C.M.; Severino, S.S.; Caldeira, S.M. Risk for falls among community-dwelling older people: Systematic literature review. Rev. Gaucha Enferm. 2017, 37, e55030. [Google Scholar] [PubMed]
- Blanco-Blanco, J.; Albornos-Muñoz, L.; Costa-Menen, M.À.; García-Martínez, E.; Rubinat-Arnaldo, E.; Martínez-Soldevila, J.; Moreno-Casbas, M.T.; Bays-Moneo, A.B.; Gea-Sánchez, M.; Otago Project Working Group. Prevalence of falls in noninstitutionalized people aged 65-80 and associations with sex and functional tests: A multicenter observational study. Res. Nurs. Health 2022, 45, 433–445. [Google Scholar] [CrossRef]
- Zidrou, C.; Kleisiaris, C.; Adamakidou, T. Associations between Disability in Activities of Daily Living and Social Capital aspects among older adults: A scoping review. J. Frailty Sarcopenia Falls 2021, 6, 119–130. [Google Scholar] [CrossRef]
- Sherrington, C.; Fairhall, N.J.; Wallbank, G.K.; Tiedemann, A.; Michaleff, Z.A.; Howard, K.; Clemson, L.; Hopewell, S.; Lamb, S.E. Exercise for preventing falls in older people living in the community. Cochrane Database Syst. Rev. 2019, 1, CD012424. [Google Scholar] [CrossRef] [PubMed]
- Meyer, C.; Chapman, A.; Klattenhoff Reyes, K.; Joe, A. Profiling the risk factors associated with falls in older people with diabetes receiving at-home nursing care: Retrospective analysis of an Australian aged care provider database. Health Soc. Care Community 2022, 30, 762–775. [Google Scholar] [CrossRef] [PubMed]
- Bettariga, F.; Maestroni, L.; Martorelli, L.; Jarvis, P.; Turner, A.; Bishop, C. The Effects of a Unilateral Strength and Power Training Intervention on Inter-Limb Asymmetry and Physical Performance in Male Amateur Soccer Players. J. Sci. Sport Exerc. 2023, 5, 328–339. [Google Scholar] [CrossRef]
- Huang, D.; Ke, X.; Jiang, C.; Song, W.; Feng, J.; Zhou, H.; Zhang, R.; Zhang, A.; Lan, F. Effects of 12 weeks of Tai Chi on neuromuscular responses and postural control in elderly patients with sarcopenia: A randomized controlled trial. Front. Neurol. 2023, 14, 1167957. [Google Scholar] [CrossRef]
- Chen, W.; Li, M.; Li, H.; Lin, Y.; Feng, Z. Tai Chi for fall prevention and balance improvement in older adults: A systematic review and meta-analysis of randomized controlled trials. Front. Public Health 2023, 11, 1236050. [Google Scholar] [CrossRef]
- Zhong, D.; Xiao, Q.; Xiao, X.; Li, Y.; Ye, J.; Xia, L.; Zhang, C.; Li, J.; Zheng, H.; Jin, R. Tai Chi for improving balance and reducing falls: An overview of 14 systematic reviews. Ann. Phys. Rehabil. Med. 2020, 63, 505–517. [Google Scholar] [CrossRef]
- Mansano Pletsch, A.H.; de Souza Borges, N.C.; Villar, D.M.; Franzini Sutilo, A.L.; de Oliveira Guirro, E.C.; de Paula, F.J.A.; de Jesus Guirro, R.R. Does sensorimotor training influence neuromuscular responses, balance, and quality of life in diabetics without a history of diabetic distal polyneuropathy? J. Bodyw. Mov. Ther. 2021, 27, 14856. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Kang, Y.; Peng, Z. Effects of resistance on blood glucose control and activity in elderly patients with type 2 diabetes mellitus with sarcopenia. Pract. Geriatr. 2024, 38, 1097100. [Google Scholar]
- Rojhani-Shirazi, Z.; Barzintaj, F.; Salimifard, M.R. Comparison the effects of two types of therapeutic exercises Frenkele vs. Swiss ball on the clinical balance measures in patients with type II diabetic neuropathy. Diabetes Metab. Syndr. 2017, 11, S29–S32. [Google Scholar] [CrossRef]
- Cross, K.; Vetter, S.W.; Alam, Y.; Hasan, M.Z.; Nath, A.D.; Leclerc, E. Role of the Receptor for Advanced Glycation End Products (RAGE) and Its Ligands in Inflammatory Responses. Biomolecules 2024, 14, 1550. [Google Scholar] [CrossRef] [PubMed]
- Sadier, N.S.; El Hajjar, F.; Al Sabouri, A.A.K.; Abou-Abbas, L.; Siomava, N.; Almutary, A.G.; Tambuwala, M.M. Irisin: An unveiled bridge between physical exercise and a healthy brain. Life Sci. 2024, 339, 122393. [Google Scholar] [CrossRef]
- DeFronzo, R.A.; Ferrannini, E.; Groop, L.; Henry, R.R.; Herman, W.H.; Holst, J.J.; Hu, F.B.; Kahn, C.R.; Raz, I.; Shulman, G.I.; et al. Type 2 diabetes mellitus. Nat. Rev. Dis. Primers 2015, 1, 15019. [Google Scholar] [CrossRef]
- Ahsan, M.; Garneau, L.; Aguer, C. The bidirectional relationship between AMPK pathway activation and myokine secretion in skeletal muscle: How it affects energy metabolism. Front. Physiol. 2022, 13, 1040809. [Google Scholar] [CrossRef]
- Han, R.; Liu, Z.; Sun, N.; Liu, S.; Li, L.; Shen, Y.; Xiu, J.; Xu, Q. BDNF Alleviates Neuroinflammation in the Hippocampus of Type 1 Diabetic Mice via Blocking the Aberrant HMGB1/RAGE/NF-κB Pathway. Aging Dis. 2019, 10, 611–625. [Google Scholar] [CrossRef]
- Wang, J.; Wang, J.; Sun, J.; Li, C.; Tong, S.; Hong, X. The effects of pre-cue posterior alpha on post-cue alpha activity and target processing in visual spatial attention tasks with instructional and probabilistic cues. Cereb. Cortex 2023, 33, 4056–4069. [Google Scholar] [CrossRef]
- Gu, Y.; Han, F.; Sainburg, L.E.; Schade, M.M.; Buxton, O.M.; Duyn, J.H.; Liu, X. An orderly sequence of autonomic and neural events at transient arousal changes. NeuroImage 2022, 264, 119720. [Google Scholar] [CrossRef]
- Wibowo, R.A.; Nurámalia, R.; Nurrahma, H.A.; Oktariani, E.; Setiawan, J.; Icanervilia, A.V.; Agustiningsih, D. The Effect of Yoga on Health-Related Fitness among Patients with Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 4199. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA Statement. Open Med. 2009, 6, e1000097. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. Declaración PRISMA 2020: Una guía actualizada para la publicación de revisiones sistemáticas. Rev. Esp. Cardiol. 2021, 74, 79099. [Google Scholar] [CrossRef]
- Li, G.; Tao, X.; Lei, B.; Hou, X.; Yang, X.; Wang, L.; Zhang, S.; Lv, Y.; Wang, T.; Yu, L. Effects of exercise on post-stroke cognitive function: A systematic review and meta-analysis of randomized controlled trials. Top. Stroke Rehabil. 2024, 31, 645–666. [Google Scholar] [CrossRef]
- Du, L.; Xi, H.; Zhang, S.; Zhou, Y.; Tao, X.; Lv, Y.; Hou, X.; Yu, L. Effects of exercise in people with multiple sclerosis: A systematic review and meta-analysis. Front. Public Health 2024, 12, 1387658. [Google Scholar] [CrossRef]
- Qiu, B.; Zhou, Y.; Tao, X.; Hou, X.; Du, L.; Lv, Y.; Yu, L. The effect of exercise on flow-mediated dilation in people with type 2 diabetes mellitus: A systematic review and meta-analysis of randomized controlled trials. Front. Endocrinol. 2024, 15, 1347399. [Google Scholar] [CrossRef]
- Zhou, Y.; Ren, H.; Hou, X.; Dong, X.; Zhang, S.; Lv, Y.; Li, C.; Yu, L. The effect of exercise on balance function in stroke patients: A systematic review and meta-analysis of randomized controlled trials. J. Neurol. 2024, 271, 4751–4768. [Google Scholar] [CrossRef] [PubMed]
- Allet, L.; Armand, S.; de Bie, R.A.; Golay, A.; Monnin, D.; Aminian, K.; Staal, J.B.; de Bruin, E.D. The gait and balance of patients with diabetes can be improved: A randomised controlled trial. Diabetologia 2010, 53, 458–466. [Google Scholar] [CrossRef]
- Borges, N.C.S.; Pletsch, A.H.M.; Buzato, M.B.; Terada, N.A.Y.; Cruz, F.; Guirro, R.R.J. The effect of proprioceptive training on postural control in people with diabetes: A randomized clinical trial comparing delivery at home, under supervision, or no training. Clin. Rehabil. 2021, 35, 988–998. [Google Scholar] [CrossRef]
- Demir, F.; Şahin, M.; Ergezen, G. Effectiveness of Proprioceptive Exercise on Balance and Sensory Function in Nursing Home Geriatric Individuals with Diabetes: Randomized Controlled Trial. TKJ Med. Sci. 2022, 42, 27–34. [Google Scholar]
- Duruturk, N.; Özköslü, M.A. Effect of tele-rehabilitation on glucose control, exercise capacity, physical fitness, muscle strength and psychosocial status in patients with type 2 diabetes: A double blind randomized controlled trial. Prim. Care Diabetes 2019, 13, 542–548. [Google Scholar] [CrossRef] [PubMed]
- Ghodrati, N.; Haghighi, A.H.; Kakhak, S.A.H.; Abbasian, S.; Goldfield, G.S. Effect of Combined Exercise Training on Physical and Cognitive Function in Women with Type 2 Diabetes. Can. J. Diabetes 2023, 47, 162–170. [Google Scholar] [CrossRef]
- Hsieh, P.-L.; Tseng, C.-H.; Tseng, Y.J.; Yang, W.-S. Resistance Training Improves Muscle Function and Cardiometabolic Risks But Not Quality of Life in Older People with Type 2 Diabetes Mellitus: A Randomized Controlled Trial. J. Geriatr. Phys. Ther. 2018, 41, 65–76. [Google Scholar] [CrossRef]
- Kruse, R.L.L.J.; Madsen, R.W. Fall and balance outcomes after an intervention to promote leg strength, balance, and walking in people with diabetic peripheral neu ropathy: “feet first” randomized controlled trial. Phys. Ther. 2010, 90, 156879. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Shin, S. Effectiveness of Virtual Reality Using Video Gaming Technology in Elderly Adults with Diabetes Mellitus. Diabetes Technol. Ther. 2013, 15, 489–496. [Google Scholar] [CrossRef] [PubMed]
- Park, S.Y.; Lee, I.H. Effects on training and detraining on physical function, control of diabetes and anthropometrics in type 2 diabetes; a randomized controlled trial. Physiother. Theory Pract. 2015, 31, 8388. [Google Scholar] [CrossRef]
- Schmid, A.A.; Atler, K.E.; Malcolm, M.P.; Grimm, L.A.; Klinedinst, T.C.; Marchant, D.R.; Marchant, T.P.; Portz, J.D. Yoga improves quality of life and fall risk-factors in a sample of people with chronic pain and Type 2 Diabetes. Complement. Ther. Clin. Pract. 2018, 31, 369–373. [Google Scholar] [CrossRef]
- Tsang, T.; Orr, R.; Lam, P.; Comino, E.J.; Singh, M.F. Health benefits of Tai Chi for older patients with type 2 diabetes: The “Move It for Diabetes study”—A randomized controlled trial. Clin. Interv. Aging 2007, 2, 42939. [Google Scholar]
- Xiao, C.M.; Zhuang, Y.C. Effects of Tai Chi ball on balance and physical function in older adults with type 2 diabetes mellitus. J. Am. Geriatr. Soc. 2015, 63, 176–177. [Google Scholar] [CrossRef]
- Ahn, S.; Song, R. Effects of Tai Chi Exercise on Glucose Control, Neuropathy Scores, Balance, and Quality of Life in Patients with Type 2 Diabetes and Neuropathy. J. Altern. Complement. Med. 2012, 18, 1172–1178. [Google Scholar] [CrossRef]
- Ng, T.K.-W.; Kwan, R.L.C.; Lo, S.K.; Cheing, G.L.-Y. A tailor-made exercise program for improving balance and mobility in older adults with type 2 diabetes. J. Gerontol. Nurs. 2018, 44, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Venkataraman, K.; Tai, B.C.; Khoo, E.Y.H.; Tavintharan, S.; Chandran, K.; Hwang, S.W.; Phua, M.S.L.A.; Wee, H.L.; Koh, G.C.H.; Tai, E.S. Short-term strength and balance training does not improve quality of life but improves functional status in individuals with diabetic peripheral neuropathy: A randomised controlled trial. Diabetologia 2019, 62, 2200–2210. [Google Scholar] [CrossRef]
- Sienko, K.H.; Seidler, R.D.; Carender, W.J.; Goodworth, A.D.; Whitney, S.L.; Peterka, R.J. Potential Mechanisms of Sensory Augmentation Systems on Human Balance Control. Front. Neurol. 2018, 9, 944. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Song, Y.; Dai, B. A Systematic Review of in Vivo Anterior Cruciate Ligament Loading During Static, Slow-Speed and Athletic Tasks. J. Sci. Sport. Exerc. 2024, 6, 1–13. [Google Scholar] [CrossRef]
- Lephart, S.M.; Pincivero, D.M.; Giraldo, J.L.; Fu, F.H. The role of proprioception in the management and rehabilitation of athletic injuries. Am. J. Sports Med. 1997, 25, 130–137. [Google Scholar] [CrossRef]
- Yu, A.P.; Tam, B.T.; Lai, C.W.; Yu, D.S.; Woo, J.; Chung, K.-F.; Hui, S.S.; Liu, J.Y.; Wei, G.X.; Siu, P.M. Revealing the Neural Mechanisms Underlying the Beneficial Effects of Tai Chi: A Neuroimaging Perspective. Am. J. Chin. Med. 2018, 46, 231–259. [Google Scholar] [CrossRef] [PubMed]
- Wei, G.-X.; Dong, H.-M.; Yang, Z.; Luo, J.; Zuo, X.-N. Tai Chi Chuan optimizes the functional organization of the intrinsic human brain architecture in older adults. Front. Aging Neurosci. 2014, 6, 74. [Google Scholar] [CrossRef]
- Wei, W.; Cheng, K.; Yang, Y. Effect of whole body vibration therapy on proprioception and balance function of lower limbs in patients with hemiplegia after stroke. Chin. J. Rehabil. 2021, 36, 20003. [Google Scholar]
- Dixit, S.; Maiya, A.G.; Shastry, B.A. Effect of aerobic exercise on peripheral nerve functions of population with diabetic peripheral neuropathy in type 2 diabetes: A single blind, parallel group randomized controlled trial. J. Diabetes Complications 2014, 28, 3329. [Google Scholar] [CrossRef]
- Orr, R.; Tsang, T.; Lam, P.; Comino, E.; Singh, M.F. Mobility impairment in type 2 diabetes: Association with muscle power and effect of Tai Chi intervention. Diabetes Care 2006, 29, 21202. [Google Scholar] [CrossRef]
- Singleton, J.R.; Marcus, R.L.; Jackson, J.E.; Lessard, M.K.; Graham, T.E.; Smith, A.G. Exercise increases cutaneous nerve density in diabetic patients without neuropathy. Ann. Clin. Transl. Neurol. 2014, 1, 844–849. [Google Scholar] [CrossRef] [PubMed]
- Tan, S.; Li, W.; Wang, J. Effects of six months of combined aerobic and resistance training for elderly patients with a long history of type 2 diabetes. J. Sports Sci. Med. 2012, 11, 495–501. [Google Scholar] [PubMed]
- Morrison, S.; Colberg, S.R.; Parson, H.K.; Vinik, A.I. Exercise improves gait, reaction time and postural stability in older adults with type 2 diabetes and neuropathy. J. Diabetes Complicat. 2014, 28, 715–722. [Google Scholar] [CrossRef] [PubMed]
- Cosentino, F.; Grant, P.J.; Aboyans, V.; Bailey, C.J.; Ceriello, A.; Delgado, V.; Federici, M.; Filippatos, G.; Grobbee, D.E.; Hansen, T.B.; et al. 2019 ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD. Eur. Heart J. 2020, 41, 255–323. [Google Scholar] [CrossRef]
- Kanaley, J.A.; Colberg, S.R.; Corcoran, M.H.; Malin, S.K.; Rodriguez, N.R.; Crespo, C.J.; Kirwan, J.P.; Zierath, J.R. Exercise/Physical Activity in Individuals with Type 2 Diabetes: A Consensus Statement from the American College of Sports Medicine. Med. Sci. Sports Exerc. 2022, 54, 353–368. [Google Scholar] [CrossRef]
- Hansen, D.; Peeters, S.; Zwaenepoel, B.; Verleyen, D.; Wittebrood, C.; Timmerman, N.; Schotte, M. Exercise assessment and prescription in patients with type 2 diabetes in the private and home care setting: Clinical recommendations from AXXON (Belgian Physical Therapy Association). Phys. Ther. 2013, 93, 597–610. [Google Scholar] [CrossRef]
- Hordern, M.D.; Dunstan, D.W.; Prins, J.B.; Baker, M.K.; Singh, M.A.F.; Coombes, J.S. Exercise prescription for patients with type 2 diabetes and pre-diabetes: A position statement from Exercise and Sport Science Australia. J. Sci. Med. Sport 2012, 15, 25–31. [Google Scholar] [CrossRef]
- Colberg, S.R.; Sigal, R.J.; Fernhall, B.; Regensteiner, J.G.; Blissmer, B.J.; Rubin, R.R.; Chasan-Taber, L.; Albright, A.L.; Braun, B.; American College of Sports Medicine; et al. Exercise and type 2 diabetes: The American College of Sports Medicine and the American Diabetes Association: Joint position statement. Diabetes Care 2010, 33, e147–e167. [Google Scholar] [CrossRef]
- Izquierdo, M.; Merchant, R.A.; Morley, J.E.; Anker, S.D.; Aprahamian, I.; Arai, H.; Aubertin-Leheudre, M.; Bernabei, R.; Cadore, E.L.; Cesari, M.; et al. International Exercise Recommendations in Older Adults (ICFSR): Expert Consensus Guidelines. J. Nutr. Health Aging 2021, 25, 824–853. [Google Scholar] [CrossRef]
- Thuany, M.; Hill, L.; Alvero-Cruz, J.R.; Knechtle, B.; Gomes, T.N. The Relationship Between Training Volume and BMI in the Expression of Running Performance in Runners: A Mediation Model. J. Sci. Sport. Exerc. 2023, 5, 142–148. [Google Scholar] [CrossRef]
- Abdelaal, A.; El-Shamy, S. Effects of Antigravity Treadmill Training on Gait and Balance in Patients with Diabetic Polyneuropathy: A Randomized Controlled Trial. F1000Research 2022, 11, 52. [Google Scholar] [CrossRef] [PubMed]
- Lesinski, M.; Hortobágyi, T.; Muehlbauer, T.; Gollhofer, A.; Granacher, U. Erratum to: Effects of Balance Training on Balance Performance in Healthy Older Adults: A Systematic Review and Meta-analysis. Sports Med. 2016, 46, 457. [Google Scholar] [CrossRef]
- Zhidong, C.; Wang, X.; Yin, J.; Song, D.; Chen, Z. Effects of physical exercise on working memory in older adults: A systematic and meta-analytic review. Eur. Rev. Aging Phys. Act. 2021, 18, 18. [Google Scholar] [CrossRef]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 145162. [Google Scholar] [CrossRef] [PubMed]
- Tan, S.; Zhang, D.; Li, W. Research on the effects of rehabilitation exercises on physical fitness of elder patients with type 2-diabetes mellitus. Chin. J. Rehabil. Med. 2009, 24, 71922. [Google Scholar]
- Collins, B.E.G.; Hartmann, T.E.; Marino, F.E.; Skein, M. The Effect of a 12 Week Mixed-Modality Training Intervention on the Cardio-Metabolic Health of Rotational Shift Workers. J. Sci. Sport Exerc. 2024, 6, 120–130. [Google Scholar] [CrossRef]
- Rishiraj, N.; Niven, B.; Prasad, N. Changes over 70 Weeks in Body Weight and Performance Variables in College-Aged Women 15s Rugby Players Using In-Person- and Online-Training Supervision. J. Sci. Sport Exerc. 2024, 6, 110–119. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zheng, W.; Su, H.; Han, B.; Chen, Z.; Liu, X.; Lv, Y.; Yu, L. Effects of Exercise on Dynamic Balance in People with Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Life 2025, 15, 913. https://doi.org/10.3390/life15060913
Zheng W, Su H, Han B, Chen Z, Liu X, Lv Y, Yu L. Effects of Exercise on Dynamic Balance in People with Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Life. 2025; 15(6):913. https://doi.org/10.3390/life15060913
Chicago/Turabian StyleZheng, Wenda, Hao Su, Bing Han, Zhuying Chen, Xiaojie Liu, Yuanyuan Lv, and Laikang Yu. 2025. "Effects of Exercise on Dynamic Balance in People with Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis of Randomized Controlled Trials" Life 15, no. 6: 913. https://doi.org/10.3390/life15060913
APA StyleZheng, W., Su, H., Han, B., Chen, Z., Liu, X., Lv, Y., & Yu, L. (2025). Effects of Exercise on Dynamic Balance in People with Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Life, 15(6), 913. https://doi.org/10.3390/life15060913