
Oral Health and Dietary Habits Before and After COVID-19 Restrictions in a Portuguese Adult Population: An Observational Study

 ,
,  ,
,  ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Setting and Participants
2.2. Dependent Variables
2.3. Independent Variables
2.4. Statistical Analysis
3. Results
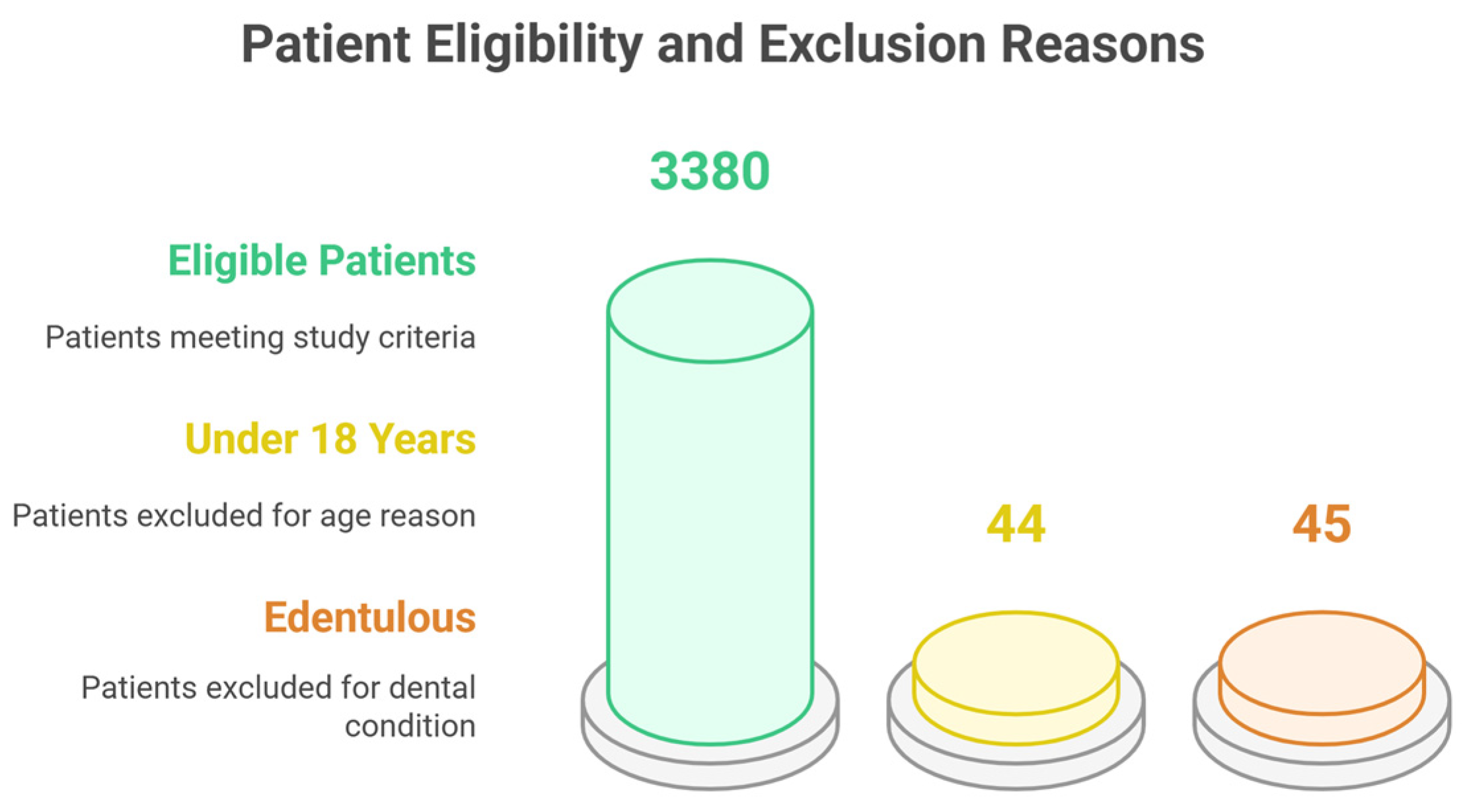
Participants’ Inclusion and Characteristics
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cucinotta, D.; Vanelli, M. WHO Declares COVID-19 a Pandemic. Acta Biomed. 2020, 91, 157–160. [Google Scholar] [CrossRef] [PubMed]
- Al-Halabi, M.; Salami, A.; Alnuaimi, E.; Kowash, M.; Hussein, I. Assessment of paediatric dental guidelines and caries management alternatives in the post COVID-19 period. A critical review and clinical recommendations. Eur. Arch. Paediatr. Dent. 2020, 21, 543–556. [Google Scholar] [CrossRef] [PubMed]
- Souza, T.F.d.; Martins, M.L.; Jural, L.A.; Maciel, I.P.; Magno, M.B.; Coqueiro, R.d.S.; Pithon, M.M.; Leal, S.C.; Fonseca-Gonçalves, A.; Maia, L.C. Did the Use of Minimum Interventions for Caries Management Change during the COVID-19 Pandemic? A Cross-Sectional Study. Caries Res. 2023, 57, 459–469. [Google Scholar] [CrossRef] [PubMed]
- Bekes, K.; Ritschl, V.; Stamm, T. COVID-19 pandemic and its impact on pediatric dentistry in Austria: Knowledge, perception and attitude among pediatric dentists in a cross-sectional survey. J. Multidiscip. Healthc. 2021, 14, 161–169. [Google Scholar] [CrossRef]
- Cărămidă, M.; Dumitrache, M.A.; Țâncu, A.M.C.; Ilici, R.R.; Ilinca, R.; Sfeatcu, R. Oral Habits during the Lockdown from the SARS-CoV-2 Pandemic in the Romanian Population. Medicina 2022, 58, 387. [Google Scholar] [CrossRef]
- Guerreiro, E.; Botelho, J.; Machado, V.; Proença, L.; Mendes, J.J.; Manso, A.C. Caries Experience before and after COVID-19 Restrictions: An Observational Study. J. Clin. Med. 2024, 13, 1164. [Google Scholar] [CrossRef]
- Wdowiak-Szymanik, A.; Wdowiak, A.; Szymanik, P.; Grocholewicz, K. Pandemic COVID-19 influence on adult’s oral hygiene, dietary habits and caries disease—Literature review. Int. J. Environ. Res. Public Health 2022, 19, 12744. [Google Scholar] [CrossRef]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef]
- Ng, D.M.; Jeffery, R.W. Relationships between perceived stress and health behaviors in a sample of working adults. Health Psychol. 2003, 22, 638. [Google Scholar] [CrossRef]
- Nichter, M.; Nichter, M.; Carkoglu, A.; Tobacco Etiology Research. Reconsidering stress and smoking: A qualitative study among college students. Tob. Control 2007, 16, 211–214. [Google Scholar] [CrossRef]
- Fidler, J.A.; West, R. Self-perceived smoking motives and their correlates in a general population sample. Nicotine Tob. Res. 2009, 11, 1182–1188. [Google Scholar] [CrossRef] [PubMed]
- Evers, C.; Dingemans, A.; Junghans, A.F.; Boevé, A. Feeling bad or feeling good, does emotion affect your consumption of food? A meta-analysis of the experimental evidence. Neurosci. Biobehav. Rev. 2018, 92, 195–208. [Google Scholar] [CrossRef]
- Yılmaz, C.; Gökmen, V. Neuroactive compounds in foods: Occurrence, mechanism and potential health effects. Food Res. Int. 2020, 128, 108744. [Google Scholar] [CrossRef]
- Rodríguez-Martín, B.C.; Meule, A. Food craving: New contributions on its assessment, moderators, and consequences. Front. Media SA 2015, 6, 21. [Google Scholar] [CrossRef]
- Havermans, R.C.; Vancleef, L.; Kalamatianos, A.; Nederkoorn, C. Eating and inflicting pain out of boredom. Appetite 2015, 85, 52–57. [Google Scholar] [CrossRef] [PubMed]
- Matsuyama, Y.; Isumi, A.; Fujiwara, T. Impacts of the COVID-19 pandemic exposure on child dental caries: Difference-in-differences analysis. Caries Res. 2022, 56, 546–554. [Google Scholar] [CrossRef]
- Cuschieri, S. The STROBE guidelines. Saudi J. Anaesth. 2019, 13, S31–S34. [Google Scholar] [CrossRef] [PubMed]
- Biazevic, M.G.H.; Frias, A.C. Levantamentos em Saúde Bucal: Métodos Básicos, 5th ed.; Faculdade de Odontologia da Universidade de São Paulo (FOUSP): São Paulo, Brazil, 2017. [Google Scholar]
- Guerreiro, E.; Botelho, J.; Machado, V.; Proença, L.; Mendes, J.J.; Manso, A.C. Caries experience and risk indicators in a Portuguese Population: A cross-sectional study. Int. J. Environ. Res. Public Health 2023, 20, 2511. [Google Scholar] [CrossRef]
- Mendes, J.J.; Viana, J.; Cruz, F.; Garrido, L.; Jessen, I.; Rodrigues, J.; Proença, L.; Delgado, A.S.; Machado, V.; Botelho, J. Radiographically screened periodontitis is associated with deteriorated oral-health quality of life: A cross-sectional study. PLoS ONE 2022, 17, e0269934. [Google Scholar] [CrossRef]
- Schneider, S.L. The international standard classification of education 2011. In Class and Stratification Analysis; Emerald Group Publishing Limited: Leeds, UK, 2013; Volume 30, pp. 365–379. [Google Scholar]
- Khamees, A.; Awadi, S.; Rawashdeh, S.; Talafha, M.; Alzoubi, M.; Almdallal, W.; Al-Eitan, S.; Saeed, A.; Al-Zoubi, R.M.; Al-Zoubi, M.S. The impact of COVID-19 pandemic lockdown on smoking habits and lifestyle: A cross-sectional study. Health Sci. Rep. 2023, 6, e1392. [Google Scholar] [CrossRef]
- Ferrante, G.; Camussi, E.; Piccinelli, C.; Senore, C.; Armaroli, P.; Ortale, A.; Garena, F.; Giordano, L. Did social isolation during the SARS-CoV-2 epidemic have an impact on the lifestyles of citizens? Epidemiol. Prev. 2020, 44, 353–362. [Google Scholar] [CrossRef] [PubMed]
- Bakaloudi, D.R.; Evripidou, K.; Siargkas, A.; Breda, J.; Chourdakis, M. Impact of COVID-19 lockdown on smoking and vaping: Systematic review and meta-analysis. Public. Health 2023, 218, 160–172. [Google Scholar] [CrossRef]
- Fernandes, A.; Ferreira, S.; Moreira, P.; Machado-Sousa, M.; Couto, B.; Raposo-Lima, C.; Costa, P.; Morgado, P.; Picó-Pérez, M. Stress, anxiety, and depression trajectories during the “first wave” of the COVID-19 pandemic: What drives resilient, adaptive and maladaptive responses in the Portuguese population? Front. Public. Health 2024, 12, 1333997. [Google Scholar] [CrossRef]
- Murmura, F.; Liberatore, L.; Musso, F.; Bravi, L.; Pierli, G. Organic Honey—Comparison of Generational Behaviour and Consumption Trends After COVID-19. J. Food Prod. Mark. 2024, 30, 67–88. [Google Scholar] [CrossRef]
- Sedik, P.; Hudecova, M.; Predanocyova, K. Exploring Consumers’ Preferences and Attitudes to Honey: Generation Approach in Slovakia. Foods 2023, 12, 1941. [Google Scholar] [CrossRef] [PubMed]
- Attia, Y.A.; Giorgio, G.M.; Addeo, N.F.; Asiry, K.A.; Piccolo, G.; Nizza, A.; Di Meo, C.; Alanazi, N.A.; Al-Qurashi, A.D.; El-Hack, M.E.A.; et al. COVID-19 pandemic: Impacts on bees, beekeeping, and potential role of bee products as antiviral agents and immune enhancers. Environ. Sci. Pollut. Res. Int. 2022, 29, 9592–9605. [Google Scholar] [CrossRef]
- Castellana, F.; De Nucci, S.; De Pergola, G.; Di Chito, M.; Lisco, G.; Triggiani, V.; Sardone, R.; Zupo, R. Trends in Coffee and Tea Consumption during the COVID-19 Pandemic. Foods 2021, 10, 2458. [Google Scholar] [CrossRef]
- Cummings, J.R.; Ackerman, J.M.; Wolfson, J.A.; Gearhardt, A.N. COVID-19 stress and eating and drinking behaviors in the United States during the early stages of the pandemic. Appetite 2021, 162, 105163. [Google Scholar] [CrossRef] [PubMed]
- Thubsang, A.; Thiwongwiang, C.; Wisetdee, C.; Chompoonuch, J.; Anson, M.; Phalamat, S.; Arreeras, T. COVID-19 pandemic affected on coffee beverage decision and consumers’ behavior. In Proceedings of the 2022 International Conference on Decision Aid Sciences and Applications (DASA), Chiang Rai, Thailand, 23–25 March 2022; pp. 976–980. [Google Scholar]
- Fernandes, S.; Sosa-Napolskij, M.; Lobo, G.; Silva, I. Impact of the COVID-19 pandemic in the Portuguese population: Consumption of alcohol, stimulant drinks, illegal substances, and pharmaceuticals. PLoS ONE 2021, 16, e0260322. [Google Scholar] [CrossRef]
- Costa, A.L.; Pereira, J.L.; Franco, L.; Guinot, F. COVID-19 lockdown: Impact on oral health-related behaviors and practices of Portuguese and Spanish children. Int. J. Environ. Res. Public. Health 2022, 19, 16004. [Google Scholar] [CrossRef]
- Paszynska, E.; Cofta, S.; Hernik, A.; Otulakowska-Skrzynska, J.; Springer, D.; Roszak, M.; Sidor, A.; Rzymski, P. Self-Reported Dietary Choices and Oral Health Care Needs during COVID-19 Quarantine: A Cross-Sectional Study. Nutrients 2022, 14, 313. [Google Scholar] [CrossRef]
- Skotnicka, M.; Karwowska, K.; Kłobukowski, F.; Wasilewska, E.; Małgorzewicz, S. Dietary Habits before and during the COVID-19 Epidemic in Selected European Countries. Nutrients 2021, 13, 1690. [Google Scholar] [CrossRef]
- Maestre, A.; Sospedra, I.; Martínez-Sanz, J.M.; Gutierrez-Hervas, A.; Fernández-Saez, J.; Hurtado-Sánchez, J.A.; Norte, A. Assessment of Spanish food consumption patterns during COVID-19 home confinement. Nutrients 2021, 13, 4122. [Google Scholar] [CrossRef] [PubMed]
- Immordino, G.; Jappelli, T.; Oliviero, T.; Zazzaro, A. Fear of COVID-19 contagion and consumption: Evidence from a survey of Italian households. Health Econ. 2022, 31, 496–507. [Google Scholar] [CrossRef] [PubMed]
- Caroppo, E.; Mazza, M.; Sannella, A.; Marano, G.; Avallone, C.; Claro, A.E.; Janiri, D.; Moccia, L.; Janiri, L.; Sani, G. Will Nothing Be the Same Again?: Changes in Lifestyle during COVID-19 Pandemic and Consequences on Mental Health. Int. J. Environ. Res. Public. Health 2021, 18, 8433. [Google Scholar] [CrossRef] [PubMed]
- Rusu, L.C.; Ardelean, L.C.; Tigmeanu, C.V.; Matichescu, A.; Sauciur, I.; Bratu, E.A. COVID-19 and Its Repercussions on Oral Health: A Review. Med. 2021, 57, 1189. [Google Scholar] [CrossRef]
- Abdelrahman, H.; Atteya, S.; Ihab, M.; Nyan, M.; Maharani, D.A.; Rahardjo, A.; Shaath, M.; Aboalshamat, K.; Butool, S.; Shamala, A.; et al. Dental practice closure during the first wave of COVID-19 and associated professional, practice and structural determinants: A multi-country survey. BMC Oral Health 2021, 21, 243. [Google Scholar] [CrossRef]
- Faria, S.F.S.; Costa, F.O.; Pereira, A.G.; Cota, L.O.M. Self-perceived and self-reported breath odour and the wearing of face masks during the COVID-19 pandemic. Oral Dis. 2022, 28, 2406–2416. [Google Scholar] [CrossRef]
- Sari, A.; Bilmez, Z.Y. Effects of Coronavirus (COVID-19) Fear on Oral Health Status. Oral Health Prev. Dent. 2021, 19, 411–423. [Google Scholar] [CrossRef]
- Pietrobelli, A.; Pecoraro, L.; Ferruzzi, A.; Heo, M.; Faith, M.; Zoller, T.; Antoniazzi, F.; Piacentini, G.; Fearnbach, S.N.; Heymsfield, S.B. Effects of COVID-19 Lockdown on Lifestyle Behaviors in Children with Obesity Living in Verona, Italy: A Longitudinal Study. Obesity 2020, 28, 1382–1385. [Google Scholar] [CrossRef]
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; Gotzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M.; Initiative, S. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. Epidemiology 2007, 18, 805–835. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P.; Initiative, S. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Variable | Total (n = 3380) | Pre-Lockdown (n = 2278) | Post-Lockdown (n = 1102) |
|---|---|---|---|
| Sex, % (n) | |||
| Female | 59.4 (2007) | 60.1 (1369) | 56.8 (476) |
| Male | 40.6 (1373) | 39.9 (909) | 43.2 (362) |
| Age, mean | 43.21 | 43.36 | 42.90 |
| Age interval (years), % (n) | |||
| 18–24 | 21.3 (719) | 21.2 (484) | 21.3 (235) |
| 25–44 | 32.4 (1094) | 32.3 (736) | 32.5 (358) |
| 45–64 | 32.2 (1088) | 31.9 (727) | 32.8 (361) |
| ≥65 | 14.2 (479) | 14.5 (331) | 13.4 (148) |
| Education, % (n) | |||
| No studies | 22.4 (756) | 24.1 (550) | 18.7 (206) |
| Elementary | 37.4 (1265) | 37.7 (859) | 36.8 (406) |
| Middle | 26.9 (1247) | 37.4 (853) | 35.8 (394) |
| Higher | 3.3 (112) | 0.7 (16) | 8.7 (96) |
| BMI (Kg/m2) % (n) | |||
| <18.5 | 3.6 (120) | 3.8 (86) | 3.1 (34) |
| 18.5–24.9 | 46.1 (1558) | 44.5 (1013) | 49.5 (545) |
| 25.0–29.9 | 34.1 (1153) | 34.4 (784) | 33.5 (369) |
| ≥30.0 | 16.2 (549) | 17.3 (35) | 14.0 (154) |
| Active Smoker % (n) | |||
| No | 79.2 (2678) | 82.0 (1869) | 73.4 (809) |
| Yes | 20.8 (702) | 18.0 (409) | 26.6 (293) |
| Variable | Total (n = 3380) | Pre-Lockdown (n = 2278) | Post-Lockdown (n = 1102) |
|---|---|---|---|
| Type of toothbrush, % (n) | |||
| Manual | |||
| Yes | 88.6 (2993) | 88.5 (2017) | 88.6 (976) |
| No | 11.4 (387) | 11.5 (261) | 11.4 (126) |
| Electric | |||
| Yes | 10.9 (368) | 10.8 (246) | 11.1 (122) |
| No | 89.1 (3012) | 89.2 (2032) | 88.9 (980) |
| Toothbrush frequency % (n) | |||
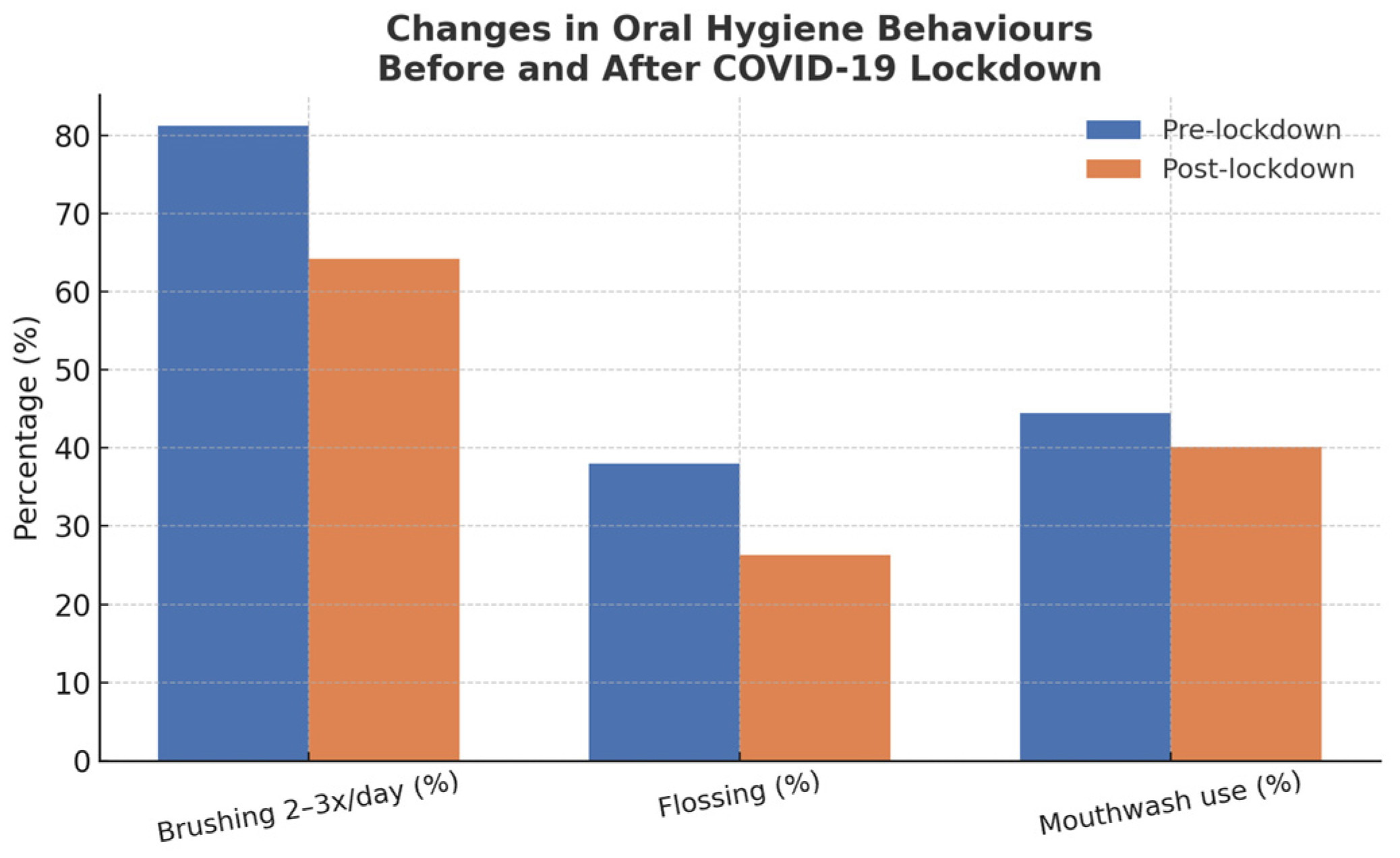
| 2–3 times/daily | 75.6 (2555) | 81.2 (1847) | 64.2 (708) |
| 1 time/daily | 15.0 (507) | 15.5 (352) | 14.1 (155) |
| 2–6 times/weekly | 7.3 (248) | 1.9 (44) | 18.5 (204) |
| Never | 2.1 (70) | 1.5 (35) | 3.2 (35) |
| Dental Floss usage, % (n) | |||
| No | 65.8 (2225) | 62.0 (1413) | 73.7 (812) |
| Yes | 34.2 (1155) | 38.0 (865) | 26.3 (290) |
| Mouth wash usage, % (n) | |||
| No | 56.9 (1924) | 55.5 (1264) | 59.9 (660) |
| Yes | 43.1 (1456) | 44.5 (1014) | 40.1 (442) |
| Variable | Total (n = 3380) | Pre-Lockdown (n = 2278) | Post-Lockdown (n = 1102) |
|---|---|---|---|
| Fresh fruit % (n) | |||
| Several times a day | 44.7 (1512) | 43.8 (997) | 46.7 (515) |
| Every day | 30.5 (1031) | 30.4 (693) | 30.7 (338) |
| Once a week | 18.3 (618) | 19.1 (435) | 16.6 (183) |
| Several times a month | 2.7 (90) | 2.7 (61) | 2.6 (29) |
| Seldom/never | 3.8 (129) | 4.0 (92) | 3.4 (37) |
| Biscuits and cakes % (n) | |||
| Not know/not answer | 0.1 (3) | 0 (0) | 0.3 (3) |
| Several times a day | 6.3 (213) | 5.9 (134) | 7.2 (79) |
| Every day | 17.8 (600) | 18.8 (428) | 15.6 (172) |
| Once a week | 44.1 (1490) | 44.2 (1007) | 43.8 (483) |
| Several times a month | 4.0 (135) | 4.3 (97) | 3.4 (38) |
| Seldom/never | 27.8 (939) | 26.9 (612) | 29.7 (327) |
| Jam or Honey % (n) | |||
| Not know/not answer | 0.1 (3) | 0 (0) | 0.3 (3) |
| Several times a day | 1.1 (37) | 1.2 (28) | 0.8 (9) |
| Every day | 7.7 (260) | 7.0 (160) | 9.1 (100) |
| Once a week | 19.9 (673) | 19.4 (441) | 21.1 (232) |
| Several times a month | 2.0 (67) | 2.0 (46) | 1.9 (21) |
| Seldom/never | 69.2 (2340) | 70.4 (1603) | 66.9 (737) |
| Sweets/candies, % (n) | |||
| Not know/not answer | 0.1 (2) | 0 (0) | 0.2 (2) |
| Several times a day | 5.6 (190) | 5.4 (122) | 6.2 (68) |
| Every day | 12.9 (436) | 13.2 (300) | 12.3 (136) |
| Once a week | 44.1 (1490) | 43.4 (988) | 45.6 (502) |
| Several times a month | 3.6 (123) | 3.5 (79) | 4.0 (44) |
| Seldom/never | 33.7 (1139) | 34.6 (789) | 31.8 (350) |
| Lemonade or soft drinks, % (n) | |||
| Not know/not answer | 0.1 (3) | 0 (0) | 0.3 (3) |
| Several times a day | 6.4 (216) | 6.2 (141) | 6.8 (75) |
| Every day | 9.7 (327) | 10.2 (233) | 8.5 (94) |
| Once a week | 26.0 (878) | 25.9 (591) | 26.0 (287) |
| Several times a month | 3.3 (111) | 3.3 (75) | 3.3 (36) |
| Seldom/never | 54.6 (1845) | 54.3 (1238) | 55.1 (607) |
| Tea with sugar, % (n) | |||
| Not know/not answer | 0.2 (6) | 0 (0) | 0.35 (6) |
| Several times a day | 2.8 (95) | 2.8 (64) | 2.8 (31) |
| Every day | 7.0 (237) | 7.1 (161) | 6.9 (76) |
| Once a week | 10.4 (352) | 10.7 (244) | 9.8 (108) |
| Several times a month | 1.5 (51) | 1.2 (27) | 2.2 (24) |
| Seldom/never | 78.1 (2639) | 78.2 (1782) | 77.8 (857) |
| Coffee with sugar, % (n) | |||
| Not know/not answer | 5.3 (178) | 0 (0) | 16.2 (178) |
| Several times a day | 21.0 (711) | 22.5 (512) | 18.1 (199) |
| Every day | 15.2 (513) | 16.3 (372) | 12.8 (141) |
| Once a week | 5.3 (180) | 6.0 (136) | 4.0 (44) |
| Several times a month | 1.3 (43) | 1.3 (29) | 1.3 (14) |
| Seldom/never | 51.9 (1755) | 54.0 (1229) | 47.7 (526) |
| Variable | Mean (Pre-Lockdown) | Mean (Post-Lockdown) | p-Value |
|---|---|---|---|
| BMI | 1.65 | 1.58 | 0.007 * |
| Active smoker | 0.18 | 0.27 | <0.001 * |
| Fresh fruit consumption | 2.32 | 2.24 | 0.076 |
| Biscuits | 3.90 | 4.01 | 0.152 |
| Honey/Jam | 5.19 | 5.06 | 0.013 * |
| Candy chewing | 5.39 | 5.46 | 0.199 |
| Sweets | 4.23 | 4.17 | 0.199 |
| Soft drinks | 4.69 | 4.73 | 0.247 |
| Tea with sugar | 5.31 | 5.29 | 0.772 |
| Coffee with sugar | 4.15 | 3.58 | <0.001 * |
| Manual toothbrush | 0.89 | 0.89 | 0.984 |
| Electric toothbrush | 0.11 | 0.11 | 0.406 |
| Dental floss usage | 0.38 | 0.26 | <0.001 * |
| Mouthwash usage | 0.45 | 0.40 | 0.015 * |
| Tooth brushing frequency | 0.24 | 0.62 | <0.001 * |
| Variable | Spearman’s ρ | p-Value |
|---|---|---|
| Education—BMI | −0.22 | <0.001 |
| Education—Smoking status | +0.04 | 0.023 |
| Age—Honey consumption | −0.12 | <0.001 |
| Gender—Smoking status | −0.11 | <0.001 |
| Age—BMI | +0.36 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guerreiro, E.; Cachinho, R.; Dionísio, T.; Nobre, M.; Júdice, A.; Simões, C.; Mendes, J.J. Oral Health and Dietary Habits Before and After COVID-19 Restrictions in a Portuguese Adult Population: An Observational Study. Life 2025, 15, 746. https://doi.org/10.3390/life15050746
Guerreiro E, Cachinho R, Dionísio T, Nobre M, Júdice A, Simões C, Mendes JJ. Oral Health and Dietary Habits Before and After COVID-19 Restrictions in a Portuguese Adult Population: An Observational Study. Life. 2025; 15(5):746. https://doi.org/10.3390/life15050746
Chicago/Turabian StyleGuerreiro, Eduardo, Ricardo Cachinho, Tiago Dionísio, Manuel Nobre, André Júdice, Cátia Simões, and José João Mendes. 2025. "Oral Health and Dietary Habits Before and After COVID-19 Restrictions in a Portuguese Adult Population: An Observational Study" Life 15, no. 5: 746. https://doi.org/10.3390/life15050746
APA StyleGuerreiro, E., Cachinho, R., Dionísio, T., Nobre, M., Júdice, A., Simões, C., & Mendes, J. J. (2025). Oral Health and Dietary Habits Before and After COVID-19 Restrictions in a Portuguese Adult Population: An Observational Study. Life, 15(5), 746. https://doi.org/10.3390/life15050746