
Prognostic Impact of COVID-19 Inflammation Score Response: A Sub-Group Analysis on Critically Ill Patients of the RuxCoFlam Trial

 , , , and
, , , and
Abstract

1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
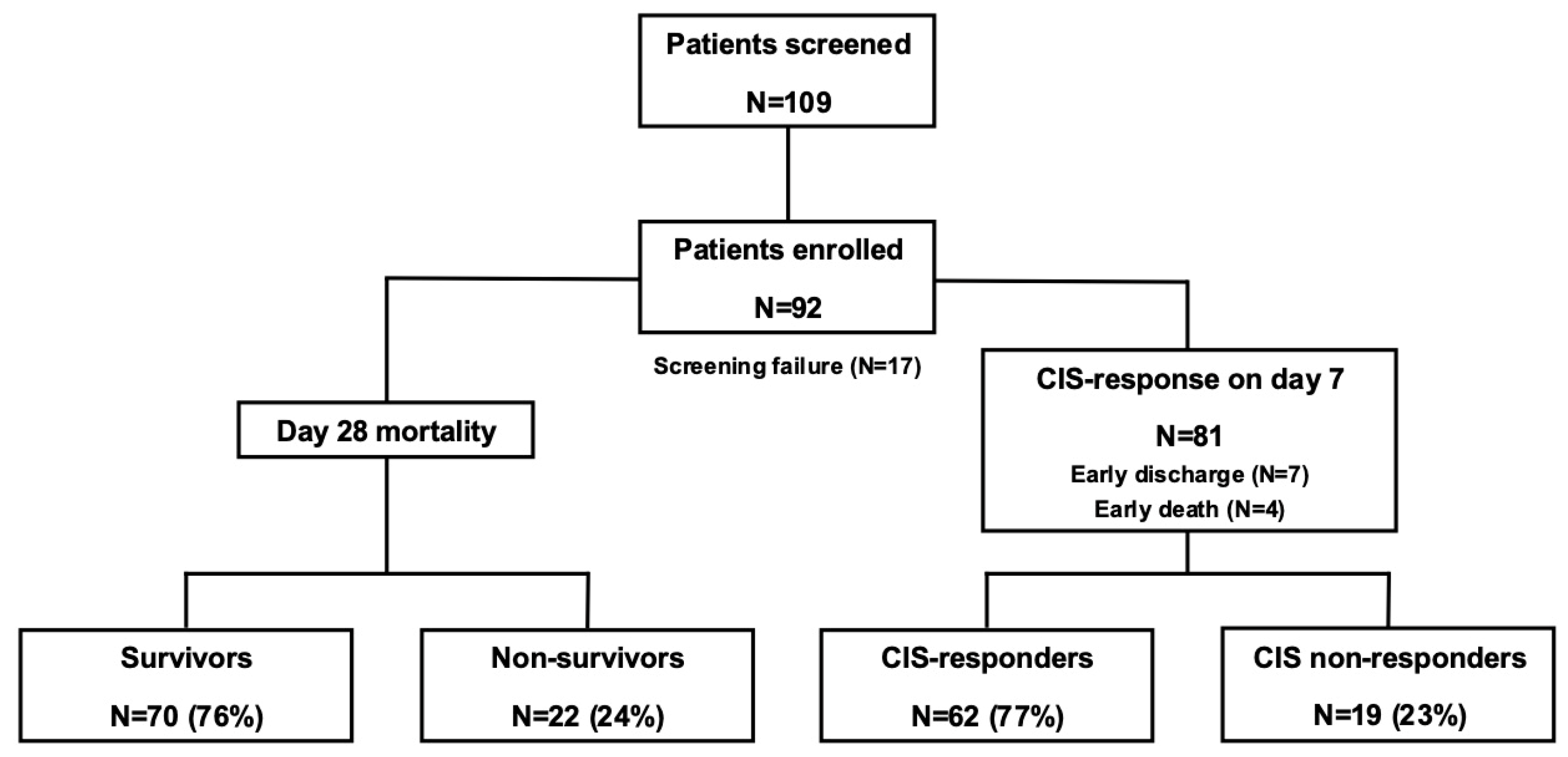
3.1. Patient Disposition and Rux Treatment
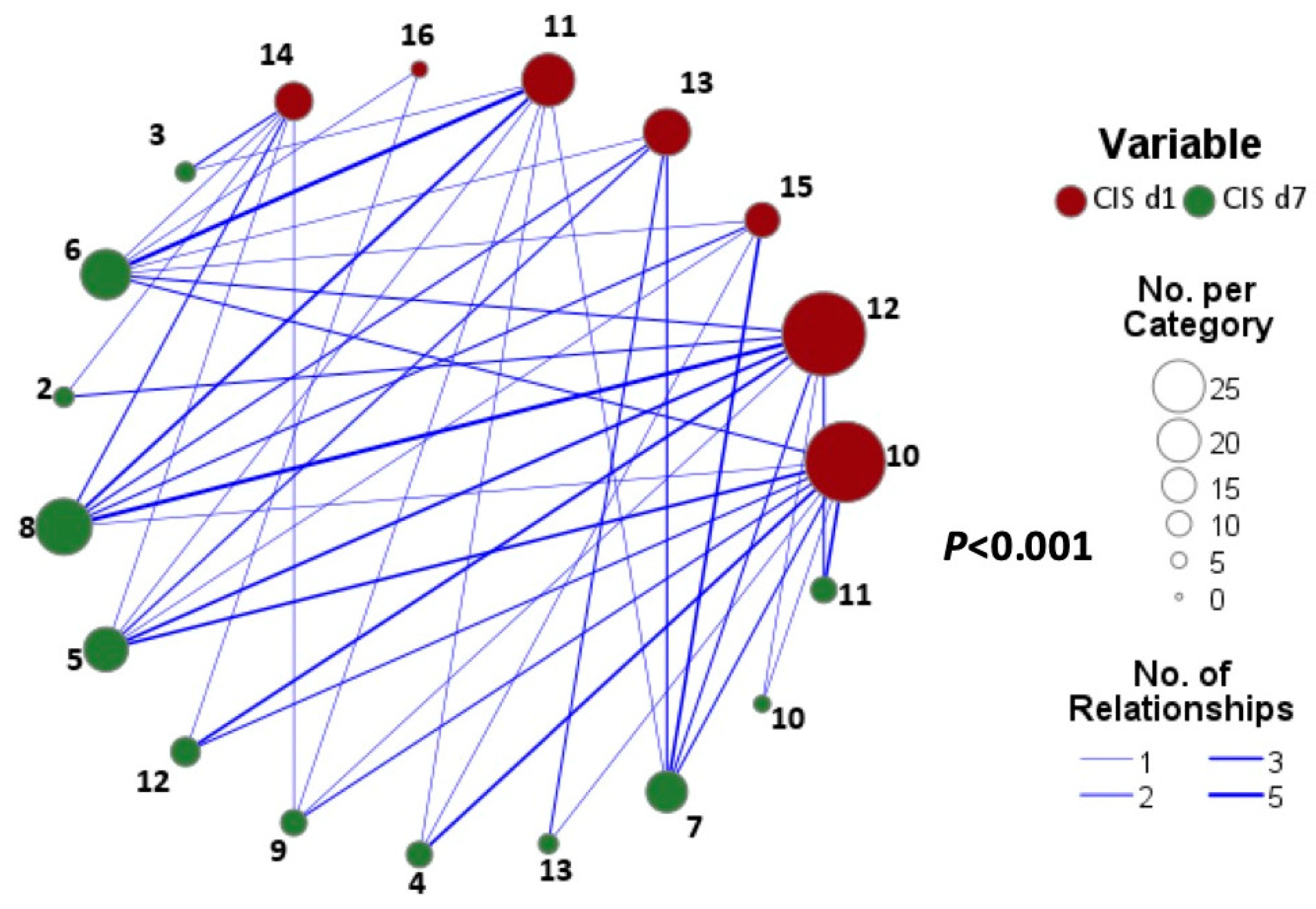
3.2. CIS Repsonose on Day 7
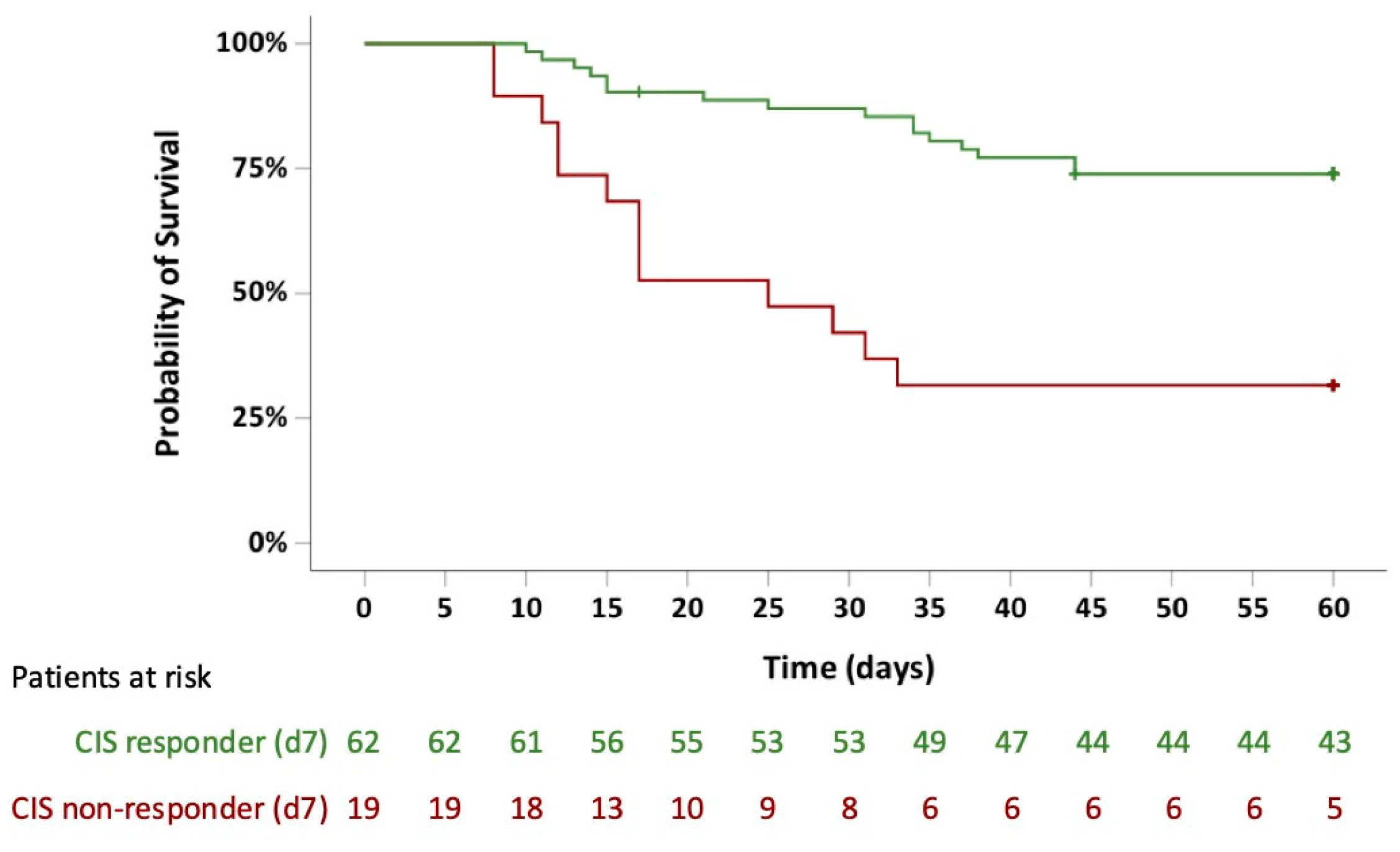
3.3. Survival Probabilities
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| aPTT | Activated partial thromboplastin time |
| BID | Twice daily |
| BMI | Body mass index |
| °C | Degree Celsius |
| CI | Confidence interval |
| CIS | COVID-19 inflammation score |
| CoV-2 | Coronavirus type 2 |
| COVID-19 | Coronavirus disease 2019 |
| CRP | C-reactive protein |
| Ct | Cycle threshold |
| CT | Computed tomography |
| ECMO | Extracorporeal membrane oxygenation |
| FDA | Food and Drug Administration |
| G/L | Giga/liter |
| HR | Hazard ratio |
| ICU | Intensive care unit |
| IFN-γ | Interferon-γ, |
| IL-6 | Interleukin-6 |
| JAK | Janus kinase |
| mg/L | Milligram/liter |
| MPN | Myeloproliferative neoplasm |
| OR | Odds ratio |
| Pts | Patients |
| RRT | Renal replacement therapy |
| Rux | Ruxolitinib |
| SAPS II | Simplified Acute Physiology Score II |
| SOFA | Sequential Organ Failure Assessment |
| SpO2 | Peripheral arterial oxygen saturation |
| ULN | Upper limit of normal |
| US | United states |
| WBC | White blood cell |
| WHO | World Health Organization |
References
- Goker Bagca, B.; Biray Avci, C. The potential of JAK/STAT pathway inhibition by ruxolitinib in the treatment of COVID-19. Cytokine Growth Factor. Rev. 2020, 54, 51–62. [Google Scholar] [CrossRef] [PubMed]
- Han, M.K.; Antila, M.; Ficker, J.H.; Gordeev, I.; Guerreros, A.; Bernus, A.L.; Roquilly, A.; Sifuentes-Osornio, J.; Tabak, F.; Teijeiro, R.; et al. Ruxolitinib in addition to standard of care for the treatment of patients admitted to hospital with COVID-19 (RUXCOVID): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Rheumatol. 2022, 4, e351–e361. [Google Scholar] [CrossRef] [PubMed]
- Botta, C.; Indrieri, A.; Garofalo, E.; Biamonte, F.; Bruni, A.; Pasqua, P.; Cesario, F.; Costanzo, F.S.; Longhini, F.; Mendicino, F. COVID-19: High-JAKing of the Inflammatory “Flight” by Ruxolitinib to Avoid the Cytokine Storm. Front. Oncol. 2020, 10, 599502. [Google Scholar] [CrossRef] [PubMed]
- Neubauer, A.; Wiesmann, T.; Vogelmeier, C.F.; Mack, E.; Skevaki, C.; Gaik, C.; Keller, C.; Figiel, J.; Sohlbach, K.; Rolfes, C.; et al. Ruxolitinib for the treatment of SARS-CoV-2 induced acute respiratory distress syndrome (ARDS). Leukemia 2020, 34, 2276–2278. [Google Scholar] [CrossRef]
- Neubauer, A.; Johow, J.; Mack, E.; Burchert, A.; Meyn, D.; Kadlubiec, A.; Torje, I.; Wulf, H.; Vogelmeier, C.F.; Hoyer, J.; et al. The janus-kinase inhibitor ruxolitinib in SARS-CoV-2 induced acute respiratory distress syndrome (ARDS). Leukemia 2021, 35, 2917–2923. [Google Scholar] [CrossRef]
- Mortara, A.; Mazzetti, S.; Margonato, D.; Delfino, P.; Bersano, C.; Catagnano, F.; Lauriola, M.; Grosso, P.; Perseghin, G.; Ippoliti, G. Compassionate use of ruxolitinib in patients with SARS-CoV-2 infection not on mechanical ventilation: Short-term effects on inflammation and ventilation. Clin. Transl. Sci. 2021, 14, 1062–1068. [Google Scholar] [CrossRef]
- Ovilla-Martinez, R.; Cota-Rangel, X.; De La Pena-Celaya, J.; Alvarado-Zepeda, M.A.; Jimenez Sastre, A.; Azuara Forcelledo, H.; Ordonez Rodriguez, B.; Pulido Broca, J.; Molina Jaimes, A.; Muniz-Carvajal, A.; et al. Ruxolitinib as a treatment strategy for SARS-CoV-2 pneumonia: Clinical experience in a real-world setting. J. Infect. Dev. Ctries. 2022, 16, 63–72. [Google Scholar] [CrossRef]
- Rein, L.; Calero, K.; Shah, R.; Ojielo, C.; Hudock, K.M.; Lodhi, S.; Sadaka, F.; Bellam, S.; Palma, C.; Hager, D.N.; et al. Randomized Phase 3 Trial of Ruxolitinib for COVID-19-Associated Acute Respiratory Distress Syndrome. Crit. Care Med. 2022, 50, 1701–1713. [Google Scholar] [CrossRef]
- Hammersen, J.; Birndt, S.; Dohner, K.; Reuken, P.; Stallmach, A.; Sauerbrey, P.; La Rosee, F.; Pfirrmann, M.; Fabisch, C.; Weiss, M.; et al. The JAK1/2 inhibitor ruxolitinib in patients with COVID-19 triggered hyperinflammation: The RuxCoFlam trial. Leukemia 2023, 37, 1879–1886. [Google Scholar] [CrossRef]
- La Rosee, F.; Bremer, H.C.; Gehrke, I.; Kehr, A.; Hochhaus, A.; Birndt, S.; Fellhauer, M.; Henkes, M.; Kumle, B.; Russo, S.G.; et al. The Janus kinase 1/2 inhibitor ruxolitinib in COVID-19 with severe systemic hyperinflammation. Leukemia 2020, 34, 1805–1815. [Google Scholar] [CrossRef]
- Feng, C.; Hua, Z.; He, L.; Yao, S.; Zou, H.; Zhu, Y.; Wang, Z.; Wang, Y. A convenient and practical index for predicting the induction response in adult patients with hemophagocytic lymphohistiocytosis: Ferritin/platelet ratio. Ann. Hematol. 2024, 103, 715–723. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef] [PubMed]
- Monk, M.; Torres, J.; Vickery, K.; Jayaraman, G.; Sarva, S.T.; Kesavan, R. A Comparison of ICU Mortality Scoring Systems Applied to COVID-19. Cureus 2023, 15, e35423. [Google Scholar] [CrossRef] [PubMed]
- Allyn, J.; Ferdynus, C.; Bohrer, M.; Dalban, C.; Valance, D.; Allou, N. Simplified Acute Physiology Score II as Predictor of Mortality in Intensive Care Units: A Decision Curve Analysis. PLoS ONE 2016, 11, e0164828. [Google Scholar] [CrossRef]
- Le-Gall, J.R.; Lemeshow, S.; Saulnier, F. A new Simplified Acute Physiology Score (SAPS II) based on a European/North American multicenter study. JAMA 1993, 270, 2957–2963. [Google Scholar] [CrossRef]
- Vincent, J.L.; de Mendonca, A.; Cantraine, F.; Moreno, R.; Takala, J.; Suter, P.M.; Sprung, C.L.; Colardyn, F.; Blecher, S. Use of the SOFA score to assess the incidence of organ dysfunction/failure in intensive care units: Results of a multicenter, prospective study. Working group on “sepsis-related problems” of the European Society of Intensive Care Medicine. Crit. Care Med. 1998, 26, 1793–1800. [Google Scholar] [CrossRef]
- Rubio-Rivas, M.; Mora-Lujan, J.M.; Formiga, F.; Arevalo-Canas, C.; Lebron Ramos, J.M.; Villalba Garcia, M.V.; Fonseca Aizpuru, E.M.; Diez-Manglano, J.; Arnalich Fernandez, F.; Romero Cabrera, J.L.; et al. WHO Ordinal Scale and Inflammation Risk Categories in COVID-19. Comparative Study of the Severity Scales. J. Gen. Intern. Med. 2022, 37, 1980–1987. [Google Scholar] [CrossRef]
- Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; Elmahi, E.; et al. Recovery Collaborative Group. Dexamethasone in Hospitalized Patients with COVID-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar] [CrossRef]
- Catanzaro, M.; Fagiani, F.; Racchi, M.; Corsini, E.; Govoni, S.; Lanni, C. Immune response in COVID-19: Addressing a pharmacological challenge by targeting pathways triggered by SARS-CoV-2. Signal Transduct. Target. Ther. 2020, 5, 84. [Google Scholar] [CrossRef]
- Chandel, A.; Leazer, S.; Alcover, K.C.; Farley, J.; Berk, J.; Jayne, C.; McNutt, R.; Olsen, M.; Allard, R.; Yang, J.; et al. Intensive Care and Organ Support Related Mortality in Patients With COVID-19: A Systematic Review and Meta-Analysis. Crit. Care Explor. 2023, 5, e0876. [Google Scholar] [CrossRef]
- Bos, L.D.J.; Ware, L.B. Acute respiratory distress syndrome: Causes, pathophysiology, and phenotypes. Lancet 2022, 400, 1145–1156. [Google Scholar] [CrossRef]
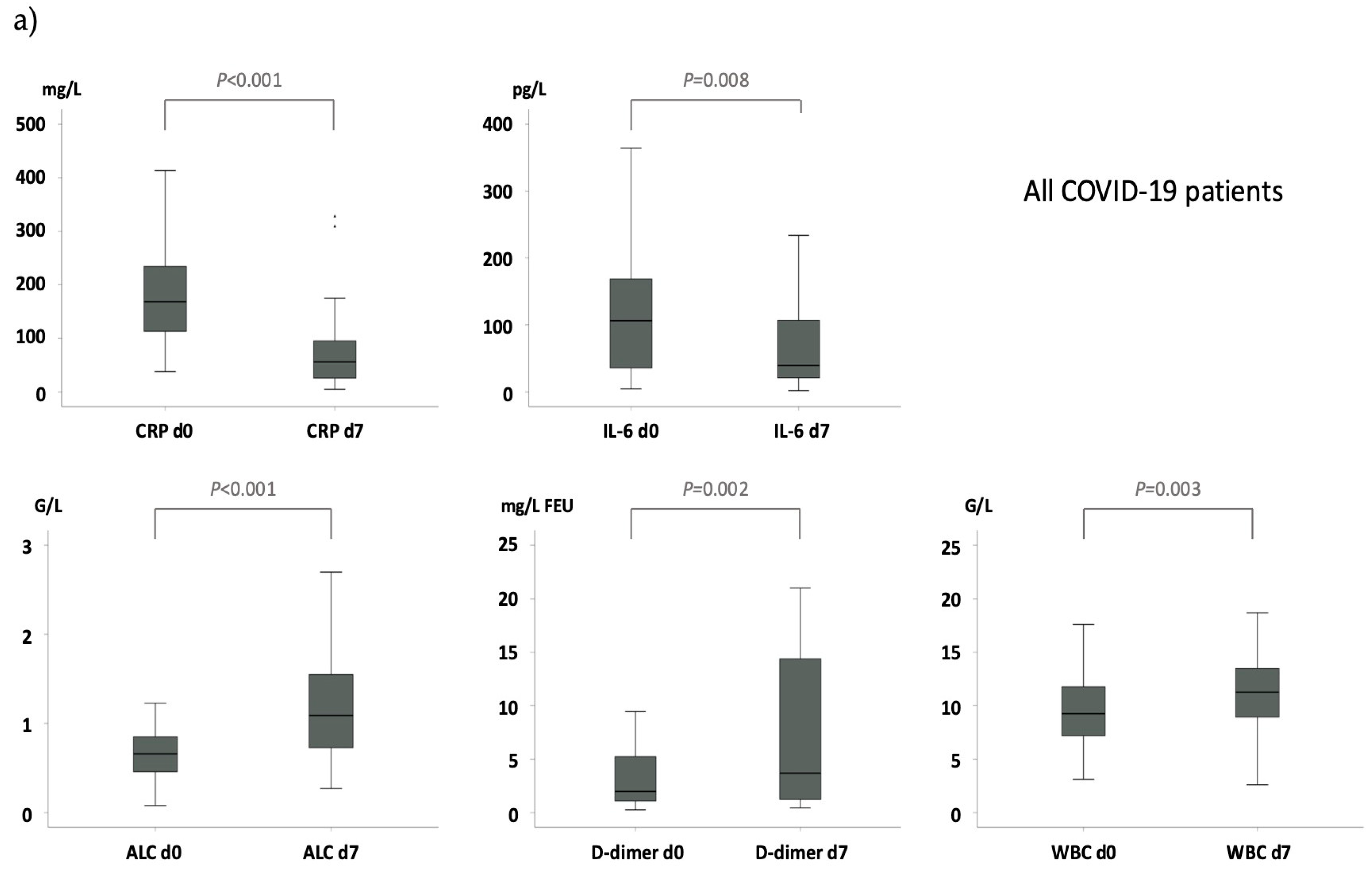
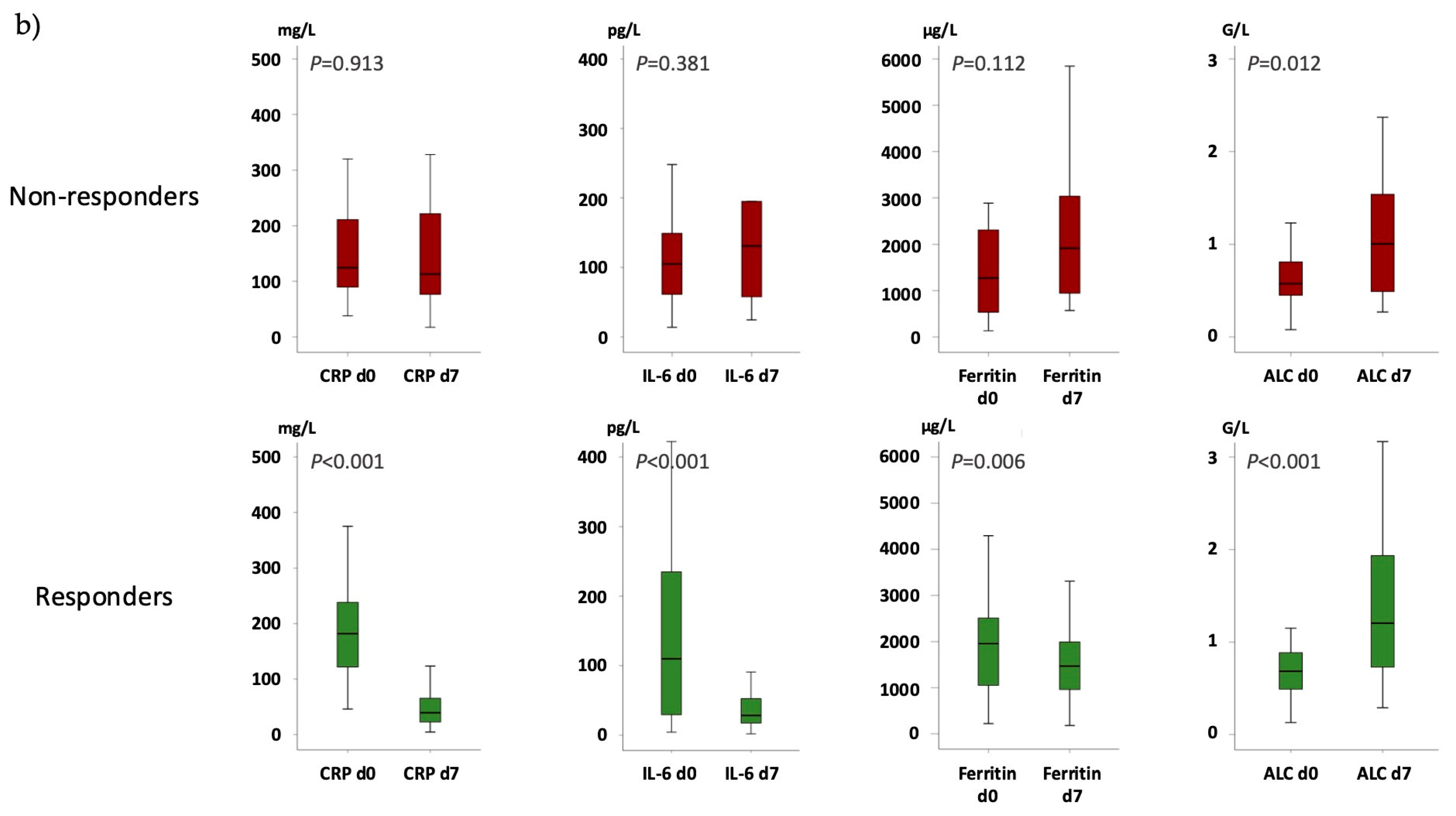
 indicates no difference in the delta (Δ) from day 7 to day 0.
indicates no difference in the delta (Δ) from day 7 to day 0.
indicates no difference in the delta (Δ) from day 7 to day 0.
indicates no difference in the delta (Δ) from day 7 to day 0.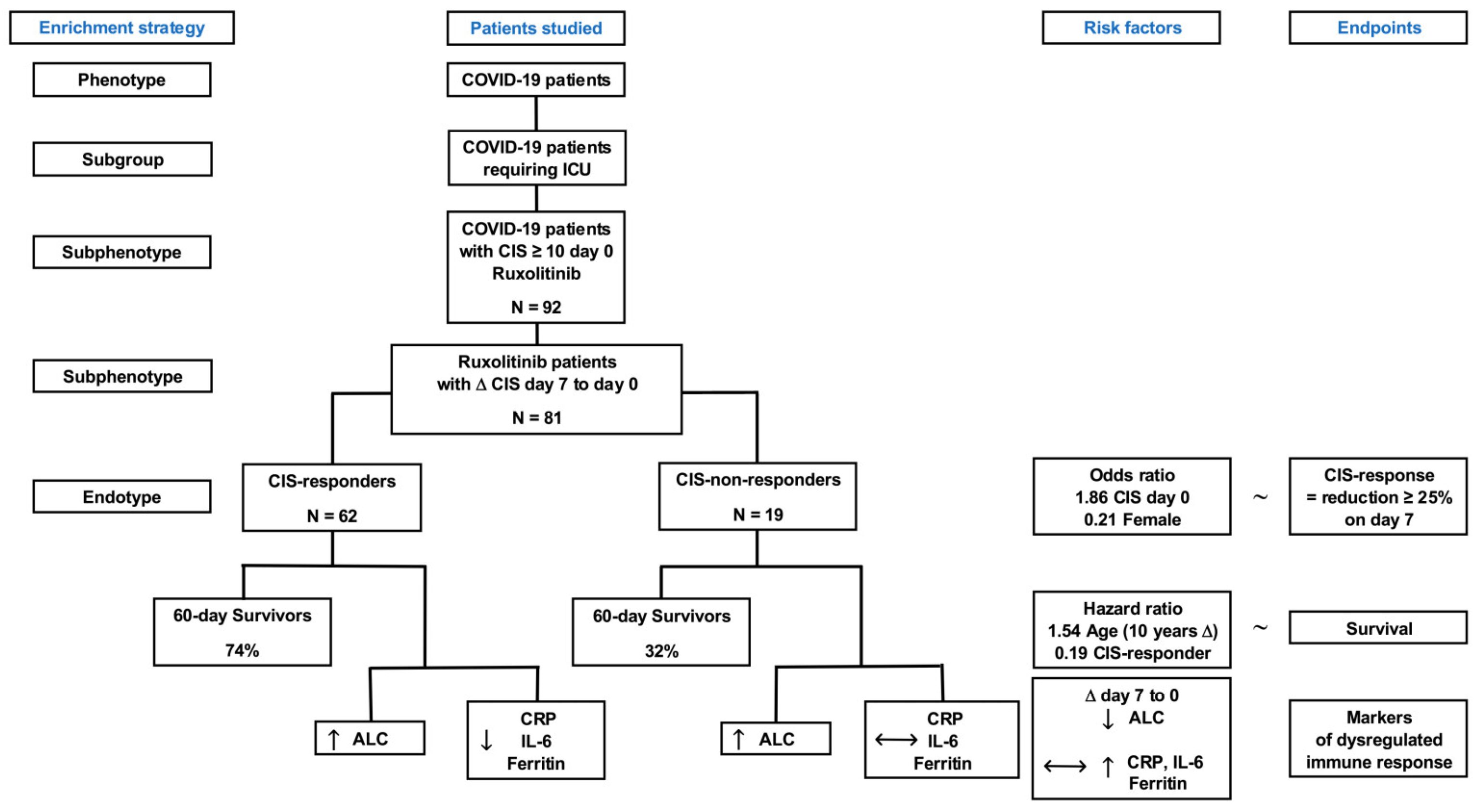

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | Cases n (%) | Mean (SD) | Median (Min–Max) |
|---|---|---|---|
| Total | 92 (100) | ||
| Age (years) | 92 | 58.3 (±12.2) | 58 (25–85) |
| Gender | 92 | ||
| Female | 22 (23.9) | ||
| Male | 70 (76.1) | ||
| BMI (kg/m2) | 89 | 33.2 (±14.0) | 29 (20–52) |
| Blood group | 92 | ||
| O | 25 (27.8) | ||
| B | 11 (12.2) | ||
| AB | 8 (8.9) | ||
| A | 46 (51.1) | ||
| n. a. | 2 (2.2) | ||
| SARS-CoV-2 | 92 | ||
| ct-value | 90 | 27.0 (±6.3) | 27 (15–40) |
| Days of symptoms | 85 | 9.9 (±5.2) | 10 (1–24) |
| CIS on day 0 | 92 | 12.0 (±1.7) | 12 (10–16) |
| Severity of disease | 92 | ||
| SAPSII | 92 | 34.4 (±9.0) | 32 (15–63) |
| SOFA | 91 | 5.4 (±2.2) | 5 (2–12) |
| WHO scale | 92 | 6.1 (±1.0) | 6 (5–7) |
| Comorbidities * | 92 | ||
| Arterial hypertension | 49 (53.3) | ||
| Cardiovascular disease | 32 (34.8) | ||
| Diabetes mellitus | 23 (25.0) | ||
| Hyperlipoproteinemia | 13 (14.1) | ||
| COPD/Asthma bronchiale | 18 (19.6) | ||
| Metabolic syndrome | 9 (9.8) | ||
| Arthritis | 4 (4.3) | ||
| Treatments * | 92 | ||
| Corticosteroids | 91 (98.9) | ||
| Remdesivir | 48 (52.2) | ||
| Corticosteroids and remdesivir | 47 (51.1) | ||
| Catecholamines | 62 (67.4) | ||
| Renal replacement | 8 (8.7) | ||
| ECMO | 23 (25.0) | ||
| Maximum ruxolitinib dose | 92 | ||
| 10 mg | 40 (43.5) | ||
| 15 mg | 24 (26.1) | ||
| 20 mg | 28 (30.4) | ||
| ICU length of stay (days) | 92 | 18.7 (±14.2) | 15 (2–73) |
| Complications * | 92 | ||
| Bacterial superinfection | 65 (70.7) | ||
| Bacteremia | 41 (44.6) | ||
| Viral superinfection/reactivation | 6 (6.5) | ||
| Fungal superinfection | 33 (35.9) | ||
| Fungemia | 3 (3.3) | ||
| Thrombosis/PAE | 13 (14.1) | ||
| Bleedings | 30 (32.6) |
| (A) CIS Response ~ | Variable | Reference Group | Odds Ratio | 95% CI | p-Value |
|---|---|---|---|---|---|
| Age (10 y difference) | continuous | 0.88 | [0.56–1.38] | 0.567 | |
| Blood group A | categorial | All other | 1.73 | [0.61–4.91] | 0.302 |
| BMI (kg/m2) | continuous | 0.99 | [0.96–1.02] | 0.415 | |
| CIS d0 | continuous | 1.86 | [1.21–2.84] | 0.005 | |
| ct-value | continuous | 1.04 | [0.96–1.14] | 0.346 | |
| Gender female | categorial | male | 0.21 | [0.07–0.66] | 0.007 |
| SAPSII | continuous | 0.99 | [0.94–1.06] | 0.814 | |
| SOFA | continuous | 0.91 | [0.72–1.15] | 0.435 | |
| Days symptom onset | continuous | 0.96 | [0.86–1.06] | 0.387 | |
| WHO scale 5 | categorial | 6 and 7 | 1.01 | [0.35–2.93] | 0.984 |
| (B) CIS Response ~ | Variable | Reference Group | Odds Ratio | 95% CI | p-Value |
| Age (10 y difference) | continuous | 0.66 | [0.38–1.14] | 0.134 | |
| Blood group A | categorial | All other | 2.65 | [0.70–10.02] | 0.151 |
| BMI (kg/m2) | continuous | 0.98 | [0.92–1.05] | 0.524 | |
| CIS d0 | continuous | 1.56 | [1.01–2.41] | 0.046 | |
| ct-value | continuous | 1.03 | [0.93–1.15] | 0.576 | |
| Gender female | categorial | male | 0.21 | [0.06–0.82] | 0.024 |
| SAPSII | continuous | 0.99 | [0.90–1.10] | 0.886 | |
| SOFA | continuous | 0.83 | [0.58–1.20] | 0.315 | |
| Days symptom onset | continuous | 1.00 | [0.86–1.16] | 0.975 | |
| WHO scale 5 | categorial | 6 and 7 | 0.56 | [0.12–2.67] | 0.467 |
| (C) Survival (d60) ~ | Variable | Reference Group | Hazard Ratio | 95% CI | p-Value |
| Age (10 y difference) | continuous | 1.76 | [1.29–2.40] | <0.001 | |
| Blood group A | categorial | All other | 0.83 | [0.42–1.64] | 0.593 |
| BMI (kg/m2) | continuous | 0.99 | [0.96–1.02] | 0.502 | |
| CIS d0 | continuous | 0.95 | [0.77–1.17] | 0.613 | |
| CIS response | categorial | 0.24 | [0.11–0.50] | <0.001 | |
| ct-value | continuous | 1.01 | [0.96–1.07] | 0.631 | |
| Gender female | categorial | male | 1.50 | [0.70–3.23] | 0.301 |
| SAPSII | continuous | 1.06 | [1.03–1.10] | <0.001 | |
| SOFA | continuous | 1.07 | [0.92–1.23] | 0.394 | |
| Days symptom onset | continuous | 1.02 | [0.95–1.09] | 0.561 | |
| WHO scale 5 | categorial | 6 and 7 | 0.81 | [0.41–1.64] | 0.562 |
| (D) Survival (d60) ~ | Variable | Reference Group | Hazard Ratio | 95% CI | p-Value |
| Age (10 y difference) | continuous | 1.54 | [1.10–2.17] | 0.012 | |
| Blood group A | categorial | All other | 0.80 | [0.34–1.88] | 0.605 |
| BMI (kg/m2) | continuous | 0.99 | [0.95–1.02] | 0.439 | |
| CIS d0 | continuous | 0.96 | [0.72–1.26] | 0.752 | |
| CIS response | categorial | 0.19 | [0.08–0.45] | <0.001 | |
| ct-value | continuous | 1.06 | [1.00–1.12] | 0.071 | |
| Gender female | categorial | male | 0.80 | [0.27–2.37] | 0.684 |
| SAPSII | continuous | 1.03 | [0.98–1.09] | 0.280 | |
| SOFA | continuous | 1.01 | [0.79–1.29] | 0.936 | |
| Days symptom onset | continuous | 1.03 | [0.94–1.12] | 0.577 | |
| WHO scale 5 | categorial | 6 and 7 | 0.68 | [0.29–1.58] | 0.370 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Weiss, M.; Hammersen, J.; Rudolphi, S.; Formann, I.; Träger, K.; Rücker, F.G.; Grüner, B.; Allgöwer, A.; Birndt, S.; Fabisch, C.; et al. Prognostic Impact of COVID-19 Inflammation Score Response: A Sub-Group Analysis on Critically Ill Patients of the RuxCoFlam Trial. Life 2025, 15, 781. https://doi.org/10.3390/life15050781
Weiss M, Hammersen J, Rudolphi S, Formann I, Träger K, Rücker FG, Grüner B, Allgöwer A, Birndt S, Fabisch C, et al. Prognostic Impact of COVID-19 Inflammation Score Response: A Sub-Group Analysis on Critically Ill Patients of the RuxCoFlam Trial. Life. 2025; 15(5):781. https://doi.org/10.3390/life15050781
Chicago/Turabian StyleWeiss, Manfred, Jakob Hammersen, Sebastian Rudolphi, Isabell Formann, Karl Träger, Frank G. Rücker, Beate Grüner, Andreas Allgöwer, Sebastian Birndt, Christian Fabisch, and et al. 2025. "Prognostic Impact of COVID-19 Inflammation Score Response: A Sub-Group Analysis on Critically Ill Patients of the RuxCoFlam Trial" Life 15, no. 5: 781. https://doi.org/10.3390/life15050781
APA StyleWeiss, M., Hammersen, J., Rudolphi, S., Formann, I., Träger, K., Rücker, F. G., Grüner, B., Allgöwer, A., Birndt, S., Fabisch, C., Hochhaus, A., Döhner, K., Rosée, P. L., & Stegelmann, F. (2025). Prognostic Impact of COVID-19 Inflammation Score Response: A Sub-Group Analysis on Critically Ill Patients of the RuxCoFlam Trial. Life, 15(5), 781. https://doi.org/10.3390/life15050781