

Which Positions Optimize Pelvic Floor Activation in Female Athletes?

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
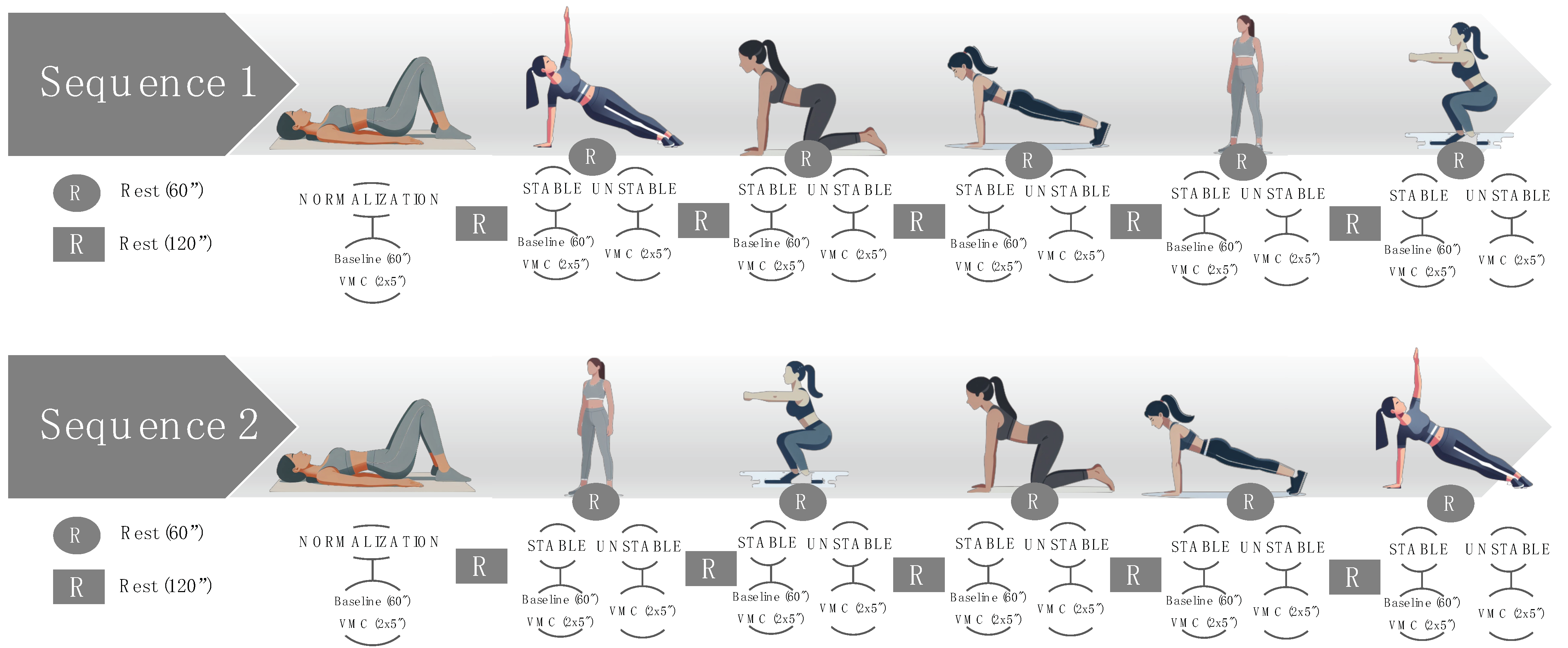
2.2. Instrumentation and Data Collection
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fitz, F.F.; Paladini, L.M.; Ferreira, L.d.A.; Gimenez, M.M.; Bortolini, M.A.T.; Castro, R.A. Ability to Contract the Pelvic Floor Muscles and Association with Muscle Function in Incontinent Women. Int. Urogynecol. J. 2020, 31, 2337–2344. [Google Scholar] [CrossRef] [PubMed]
- Joy, E.A.; Van Hala, S.; Cooper, L. Health-Related Concerns of the Female Athlete: A Lifespan Approach. Am. Fam. Physician 2009, 79, 489–495. [Google Scholar]
- Brown, N.; Williams, G.K.R.; Stodter, A.; McNarry, M.A.; Roldan-Reoyo, O.; Mackintosh, K.A.; Moore, I.S.; Williams, E.M.P. A Global Women’s Rugby Union Web-Based Survey. Int. J. Environ. Res. Public Health 2023, 20, 5475. [Google Scholar] [CrossRef] [PubMed]
- Joseph, C.; Srivastava, K.; Ochuba, O.; Ruo, S.W.; Alkayyali, T.; Sandhu, J.K.; Waqar, A.; Jain, A.; Poudel, S. Stress Urinary Incontinence Among Young Nulliparous Female Athletes. Cureus 2021, 13, e17986. [Google Scholar] [CrossRef]
- Fukuda, F.S.; Arbieto, E.R.M.; Da Roza, T.; Luz, S.C.T. Da Pelvic Floor Muscle Training in Women Practicing High-Impact Sports: A Systematic Review. Int. J. Sports Med. 2022, 44, 397–405. [Google Scholar] [PubMed]
- Dumoulin, C.; Hay-Smith, J. Pelvic Floor Muscle Training versus No Treatment, or Inactive Control Treatments, for Urinary Incontinence in Women. Cochrane Database Syst. Rev. 2010, 10, CD005654. [Google Scholar] [CrossRef]
- Díaz-Mohedo, E.; Odriozola Aguirre, I.; Molina García, E.; Infantes-Rosales, M.A.; Hita-Contreras, F. Functional Exercise Versus Specific Pelvic Floor Exercise: Observational Pilot Study in Female University Students. Healthcare 2023, 11, 561. [Google Scholar] [CrossRef]
- Bø, K.; Finckenhagen, H.B. Is There Any Difference in Measurement of Pelvic Floor Muscle Strength in Supine and Standing Position? Acta Obstet. Gynecol. Scand 2003, 82, 1120–1124. [Google Scholar] [CrossRef]
- Betsch, M.; Wild, M.; Große, B.; Rapp, W.; Horstmann, T. The Effect of Simulating Leg Length Inequality on Spinal Posture and Pelvic Position: A Dynamic Rasterstereographic Analysis. Eur. Spine J. 2012, 21, 691–697. [Google Scholar] [CrossRef] [PubMed]
- Navarro Brazález, B.; Torres Lacomba, M.; de la Villa, P.; Sánchez Sánchez, B.; Prieto Gómez, V.; Asúnsolo del Barco, Á.; McLean, L. The Evaluation of Pelvic Floor Muscle Strength in Women with Pelvic Floor Dysfunction: A Reliability and Correlation Study. Neurourol. Urodyn. 2018, 37, 269–277. [Google Scholar] [CrossRef] [PubMed]
- Molina-Molina, A.; Ruiz-Malagón, E.J.; Carrillo-Pérez, F.; Roche-Seruendo, L.E.; Damas, M.; Banos, O.; García-Pinillos, F. Validation of MDurance, A Wearable Surface Electromyography System for Muscle Activity Assessment. Front. Physiol. 2020, 11, 606287. [Google Scholar] [CrossRef] [PubMed]
- Carrillo-Perez, F.; Diaz-Reyes, I.; Damas, M.; Banos, O.; Soto-Hermoso, V.M.; Molina-Molina, A. A Novel Automated Algorithm for Computing Lumbar Flexion Test Ratios Enhancing Athletes Objective Assessment of Low Back Pain. In Proceedings of the icSPORTS 2018—Proceedings of the 6th International Congress on Sport Sciences Research and Technology Support 2018, Seville, Spain, 20–21 September 2018; pp. 34–39. [Google Scholar] [CrossRef]
- Luginbuehl, H.; Naeff, R.; Zahnd, A.; Baeyens, J.-P.; Kuhn, A.; Radlinger, L. Pelvic Floor Muscle Electromyography during Different Running Speeds: An Exploratory and Reliability Study. Arch. Gynecol. Obstet. 2016, 293, 117–124. [Google Scholar] [CrossRef] [PubMed]
- Bussey, M.D.; Aldabe, D.; Adhia, D.; Mani, R. Reliability of Surface Electromyography Activity of Gluteal and Hamstring Muscles during Sub-Maximal and Maximal Voluntary Isometric Contractions. Musculoskelet. Sci. Pract. 2018, 34, 103–107. [Google Scholar] [CrossRef]
- Filter, A.; Olivares-Jabalera, J.; Santalla, A.; Morente-Sánchez, J.; Robles-Rodríguez, J.; Requena, B.; Loturco, I. Curve Sprinting in Soccer: Kinematic and Neuromuscular Analysis. Int. J. Sports Med. 2020, 41, 744–750. [Google Scholar] [CrossRef]
- Koenig, I.; Eichelberger, P.; Leitner, M.; Moser, H.; Kuhn, A.; Taeymans, J.; Radlinger, L. Pelvic Floor Muscle Activity Patterns in Women with and without Stress Urinary Incontinence While Running. Ann. Phys. Rehabil. Med. 2020, 63, 495–499. [Google Scholar] [CrossRef]
- Dietz, H.P.; Wilson, P.D.; Clarke, B. The Use of Perineal Ultrasound to Quantify Levator Activity and Teach Pelvic Floor Muscle Exercises. Int. Urogynecol. J. 2001, 12, 166–169. [Google Scholar] [CrossRef] [PubMed]
- Ben Ami, N.; Dar, G. What Is the Most Effective Verbal Instruction for Correctly Contracting the Pelvic Floor Muscles? Neurourol. Urodyn. 2018, 37, 2904–2910. [Google Scholar] [CrossRef]
- Merletti, R.; Hermens, H. Introduction to the Special Issue on the SENIAM European Concerted Action. J. Electromyogr. Kinesiol. 2000, 10, 283–286. [Google Scholar] [CrossRef] [PubMed]
- Oleksy, Ł.; Wojciechowska, M.; Mika, A.; Antos, E.; Bylina, D.; Kielnar, R.; Pruszczyński, B.; Stolarczyk, A. Normative Values for Glazer Protocol in the Evaluation of Pelvic Floor Muscle Bioelectrical Activity. Medicine 2020, 99, e19060. [Google Scholar] [CrossRef]
- Ballmer, C.; Eichelberger, P.; Leitner, M.; Moser, H.; Luginbuehl, H.; Kuhn, A.; Radlinger, L. Electromyography of Pelvic Floor Muscles with True Differential versus Faux Differential Electrode Configuration. Int. Urogynecol. J. 2020, 31, 2051–2059. [Google Scholar] [CrossRef] [PubMed]
- Leitner, M.; Moser, H.; Eichelberger, P.; Kuhn, A.; Radlinger, L. Evaluation of Pelvic Floor Muscle Activity during Running in Continent and Incontinent Women: An Exploratory Study. Neurourol. Urodyn. 2017, 36, 1570–1576. [Google Scholar] [CrossRef]
- Gimenez, M.M.; Fitz, F.F.; de Azevedo Ferreira, L.; Bortolini, M.A.T.; Lordêlo, P.V.S.; Castro, R.A. Pelvic Floor Muscle Function Differs between Supine and Standing Positions in Women with Stress Urinary Incontinence: An Experimental Crossover Study. J. Physiother. 2022, 68, 51–60. [Google Scholar] [CrossRef] [PubMed]
- Mastwyk, S.; McClelland, J.; Cooper, M.M.; Frawley, H.C. Pelvic Floor Muscle Function in the Standing Position in Women with Pelvic Floor Dysfunction. Int. Urogynecol. J. 2022, 33, 2435–2444. [Google Scholar] [CrossRef]
- Griffin, C.; Dougherty, M.C.; Yarandi, H. Pelvic Muscles during Rest: Responses to Pelvic Muscle Exercise. Nurs. Res. 1994, 43, 164–167. [Google Scholar] [CrossRef] [PubMed]
- Madill, S.J.; McLean, L. Quantification of Abdominal and Pelvic Floor Muscle Synergies in Response to Voluntary Pelvic Floor Muscle Contractions. J. Electromyogr. Kinesiol. 2008, 18, 955–964. [Google Scholar] [CrossRef] [PubMed]
- Johnson, V.Y. How the Principles of Exercise Physiology Influence Pelvic Floor Muscle Training. J. Wound Ostomy Cont. Nurs. 2001, 28, 150–155. [Google Scholar] [CrossRef]
- Chmielewska, D.; Stania, M.; Sobota, G.; Kwaśna, K.; Błaszczak, E.; Taradaj, J.; Juras, G. Impact of Different Body Positions on Bioelectrical Activity of the Pelvic Floor Muscles in Nulliparous Continent Women. Biomed. Res. Int. 2015, 2015, 905897. [Google Scholar] [CrossRef]
- Chmielewska, D.; Stania, M.; Kucab–Klich, K.; Błaszczak, E.; Kwaśna, K.; Smykla, A.; Hudziak, D.; Dolibog, P. Electromyographic Characteristics of Pelvic Floor Muscles in Women with Stress Urinary Incontinence Following SEMG-Assisted Biofeedback Training and Pilates Exercises. PLoS ONE 2019, 14, e0225647. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Mias, N.L.; Subramaniam, N.; Friedman, T.; Shek, K.L.; Dietz, H.P. Prolapse assessment supine and standing: Do we need different cutoffs for “significant prolapse”? Int. Urogynecol. J. 2018, 29, 685–689. [Google Scholar] [CrossRef] [PubMed]
- Miller, J.M.; Perucchini, D.; Carchidi, L.T.; Delancey, J.O.L.; Ashton-Miller, J. Pelvic Floor Muscle Contraction During a Cough and Decreased Vesical Neck Mobility. Obstet. Gynecol. 2001, 97, 255–260. [Google Scholar]
- Sapsford, R.R.; Richardson, C.A.; Stanton, W.R. Sitting Posture Affects Pelvic Floor Muscle Activity in Parous Women: An Observational Study. Aust. J. Physiother. 2006, 52, 219–222. [Google Scholar] [CrossRef]
- Kannan, P.; Winser, S.; Goonetilleke, R.; Cheing, G. Ankle Positions Potentially Facilitating Greater Maximal Contraction of Pelvic Floor Muscles: A Systematic Review and Meta-Analysis. Disabil. Rehabil. 2019, 41, 2483–2491. [Google Scholar] [CrossRef] [PubMed]
- Lee, K. Investigation of Electromyographic Activity of Pelvic Floor Muscles in Different Body Positions to Prevent Urinary Incontinence. Med. Sci. Monit. 2019, 25, 9357–9363. [Google Scholar] [CrossRef] [PubMed]
- Dayican, D.K.; Keser, I.; Yavuz, O.; Tosun, G.; Kurt, S.; Tosun, O.C. Can Pelvic Floor Muscle Training Positions Be Selected According to the Functional Status of Pelvic Floor Muscles? Niger. J. Clin. Pract. 2023, 26, 1309–1318. [Google Scholar] [CrossRef]
- Nightingale, G.; Chandrakumaran, K.; Phillips, C. The Effect of Modified Pilates-Based Positions on Pelvic Floor Electromyographic (EMG) Activity; a Pilot Study. Int. Urogynecol. J. 2021, 32, 287–292. [Google Scholar] [CrossRef] [PubMed]
- Medrano Sánchez, E.M.; Serrano, C.M.S.; De La, M.; Almeida, C.; Mohedo, E.D.; Chilló N Martínez, R. Spanish Version of the Broome Pelvic Muscle Self-Efficacy Scale: Validity and Reliability. Phys. Ther. 2013, 93, 1696–1706. [Google Scholar] [CrossRef] [PubMed]
- Bø, K.; Kvarstein, B.; Nygaard, I. Lower Urinary Tract Symptoms and Pelvic Floor Muscle Exercise Adherence after 15 Years. Obstet. Gynecol. 2005, 105, 999–1005. [Google Scholar] [CrossRef]
- Bø, K.; Talseth, T.; Holme, I. Single Blind, Randomised Controlled Trial of Pelvic Floor Exercises, Electrical Stimulation, Vaginal Cones, and No Treatment in Management of Genuine Stress Incontinence in Women. BMJ 1999, 318, 487–493. [Google Scholar] [CrossRef]
- Pires, T.F.; Pires, P.M.; Moreira, M.H.; Gabriel, R.E.C.D.; João, P.V.; Viana, S.A.; Viana, R.A. Pelvic Floor Muscle Training in Female Athletes: A Randomized Controlled Pilot Study. Int. J. Sports Med. 2020, 41, 264–270. [Google Scholar] [CrossRef] [PubMed]
- Dessole, F.; Adrián Curillo-Aguirre, C.; Gea-Izquierdo, E. Effectiveness of Pelvic Floor Muscle Training on Quality of Life in Women with Urinary Incontinence: A Systematic Review and Meta-Analysis. Medicina 2023, 59, 1004. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Position | Condition | Exercise | Peak Amplitude (in μV) | Peak Amplitude (in %) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | 95% CI | p Value * | Mean | SD | 95% CI | p-Value * | |||||
| Supine (Normalization) | Stable | Supine | 23.42 | 9.31 | 15.34 | 25.09 | <0.001 | 16.23 | 12.11 | 11.67 | 24.27 | <0.001 |
| Standing | Stable | Standing with support | 39.27 | 13.35 | 33.75 | 44.78 | 28.46 | 20.11 | 20.16 | 36.76 | ||
| Unstable | Standing | 42.48 | 19.52 | 34.42 | 50.54 | 30.15 | 19.67 | 22.03 | 38.27 | |||
| Side-lying | Stable | Side-lying position | 26.84 | 16.42 | 20.06 | 33.62 | 22.03 | 24.44 | 11.94 | 32.12 | ||
| Unstable | Side plank | 31.69 | 17.92 | 24.29 | 39.09 | 24.69 | 22.42 | 15.44 | 33.95 | |||
| Quadruped | Stable | Quadruped hold | 40.39 | 14.83 | 34.27 | 46.51 | 29.64 | 21.18 | 20.89 | 38.38 | ||
| Unstable | Off-knees quadruped hold | 56.72 | 60.75 | 31.65 | 81.80 | 37.59 | 30.73 | 24.91 | 50.27 | |||
| Plank | Stable | Plank on knee | 57.06 | 26.73 | 46.03 | 68.09 | 39.49 | 24.41 | 29.41 | 49.56 | ||
| Unstable | Full plank | 52.11 | 23.29 | 42.50 | 61.72 | 35.71 | 20.26 | 27.35 | 44.07 | |||
| Squat | Stable | Wall squat | 47.52 | 25.89 | 36.84 | 58.21 | 38.13 | 41.86 | 20.85 | 55.41 | ||
| Unstable | Parallel plank | 53.53 | 19.69 | 45.40 | 61.66 | 40.69 | 33.68 | 26.78 | 54.59 | |||
| Peak Amplitude (in μV) | Peak Amplitude (in %) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | 95% CI | p Value * | Mean | SD | 95% CI | p-Value * | |||
| Supine (Normalization) | 169.08 | 72.12 | 139.31 | 198.85 | 0.001 | 0.001 | ||||
| Standing | 169.13 | 80.34 | 135.97 | 202.29 | 104.00 | 32.40 | 90.63 | 117.38 | ||
| Side plank | 163.93 | 74.55 | 133.15 | 194.70 | 102.49 | 30.15 | 90.04 | 114.93 | ||
| Quadruped hold | 192.96 | 79.99 | 159.95 | 225.98 | 121.58 | 30.81 | 108.86 | 134.29 | ||
| Full plank | 193.56 | 82.35 | 159.57 | 227.56 | 121.97 | 41.79 | 104.73 | 139.22 | ||
| Parallel squat | 208.10 | 70.30 | 179.08 | 237.12 | 151.40 | 109.4 | 106.24 | 196.56 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodríguez-López, E.S.; Martín-Márquez, L.M.; Acevedo-Gómez, M.B.; López-Illescas, Á.; Benito-de-Pedro, M.; Ojedo-Martín, C. Which Positions Optimize Pelvic Floor Activation in Female Athletes? Life 2025, 15, 58. https://doi.org/10.3390/life15010058
Rodríguez-López ES, Martín-Márquez LM, Acevedo-Gómez MB, López-Illescas Á, Benito-de-Pedro M, Ojedo-Martín C. Which Positions Optimize Pelvic Floor Activation in Female Athletes? Life. 2025; 15(1):58. https://doi.org/10.3390/life15010058
Chicago/Turabian StyleRodríguez-López, Elena Sonsoles, Luz María Martín-Márquez, María Barbaño Acevedo-Gómez, África López-Illescas, María Benito-de-Pedro, and Cristina Ojedo-Martín. 2025. "Which Positions Optimize Pelvic Floor Activation in Female Athletes?" Life 15, no. 1: 58. https://doi.org/10.3390/life15010058
APA StyleRodríguez-López, E. S., Martín-Márquez, L. M., Acevedo-Gómez, M. B., López-Illescas, Á., Benito-de-Pedro, M., & Ojedo-Martín, C. (2025). Which Positions Optimize Pelvic Floor Activation in Female Athletes? Life, 15(1), 58. https://doi.org/10.3390/life15010058