

COVID-19 and Laboratory Markers from Romanian Patients—A Narrative Review

 ,
,  , , and
, , and
Abstract
:1. Introduction
1.1. Background Information on COVID-19 and Its Impact in Romania
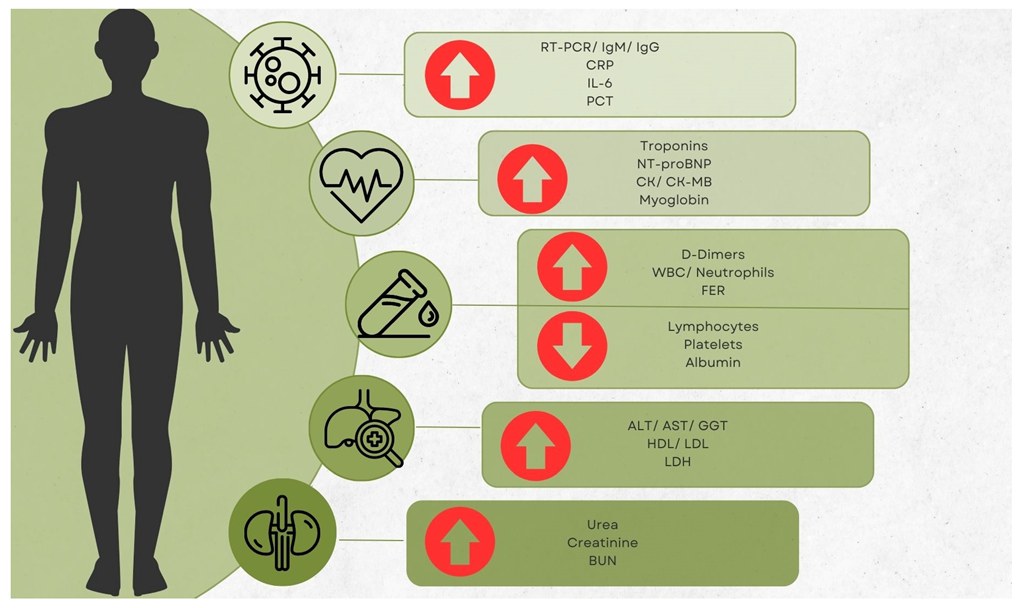
1.2. Importance of Laboratory Findings in Understanding and Managing the Disease and Purpose of the Study
2. Materials and Methods
2.1. Study Design, Sample Selection and Data Collection
2.2. Limitations
3. Results
3.1. PCR Testing
3.2. C-Reactive Protein (CRP)
3.3. Cytokines and Other Proinflammatory Markers
3.4. Lactate Dehydrogenase (LDH)
3.5. Creatine-Kinase (CK) and Its Isoforms
3.6. Troponins (TN’S) and Other Cardiac Markers
3.7. Ferritin (FER) and Other Iron Markers
3.8. High- and Low-Density Lipoprotein Cholesterol Markers (HDL and LDL), Triglycerides
3.9. Transaminase Levels and Other Hepatic Markers
3.10. Vitamin D (25-OHD)
3.11. Procalcitonin (PCT)
3.12. D-Dimers
3.13. Fibrinogen and Other Clotting Markers
3.14. Blood Urea Nitrogen (BUN) and Other Renal Markers
3.15. Complete Blood Counts (CBC) and Other Blood Test Markers
3.16. Microbiological Cultures and Assessments
3.17. Other Markers: Thyroid, Antibodies and Ablumin
4. Discussions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dascalu, S. The Successes and Failures of the Initial COVID-19 Pandemic Response in Romania. Front. Public Health 2020, 8, 344. [Google Scholar] [CrossRef]
- Leretter, M.; Vulcanescu, D.; Horhat, F.; Matichescu, A.; Rivis, M.; Rusu, L.-C.; Roi, A.; Racea, R.; Badea, I.; Dehelean, C.; et al. COVID-19: Main findings after a year and half of unease and the proper scientific progress (Review). Exp. Ther. Med. 2022, 23, 424. [Google Scholar] [CrossRef]
- Mitrică, B.; Mocanu, I.; Grigorescu, I.; Dumitraşcu, M.; Pistol, A.; Damian, N.; Şerban, P. Population Vulnerability to the SARS-CoV-2 Virus Infection. A County-Level Geographical-Methodological Approach in Romania. GeoHealth 2021, 5, e2021GH000461. [Google Scholar] [CrossRef]
- Enciu, B.G.; Tănase, A.A.; Drăgănescu, A.C.; Aramă, V.; Pițigoi, D.; Crăciun, M.-D. The COVID-19 Pandemic in Romania: A Comparative Description with Its Border Countries. Healthcare 2022, 10, 1223. [Google Scholar] [CrossRef]
- Stănculescu, E. Fear of COVID-19 in Romania: Validation of the Romanian Version of the Fear of COVID-19 Scale Using Graded Response Model Analysis. Int. J. Ment. Health Addict. 2021, 20, 1094–1109. [Google Scholar] [CrossRef]
- Stulea, R.; Goian, C.; Vlaicu, F. The Impact of the COVID-19 Pandemic on the Social Life of the Staff and Beneficiaries of the Gătaia Psychiatric Hospital, in Timiș County. Bull. Transilv. Univ. Braşov Ser. VII Soc. Sci. Law 2021, 14, 373–380. [Google Scholar] [CrossRef]
- Goian, C.; Vlaicu, L.; Moţăţeanu, G.; Bălăuţă, D.S.; Popovici, C. The Effects of the COVID-19 Pandemic on Children with Special Educational Needs in Rural Areas from Mehedinţi County. Soc. Work Rev. Rev. De Asistenta Soc. 2022, 1, 95–103. [Google Scholar]
- Bîrsanu, S.-E.; Plaiasu, M.C.; Nanu, C.A. Informed Consent in Mass Vaccination against COVID-19 in Romania: Implications of Bad Management. Vaccines 2022, 10, 1871. [Google Scholar] [CrossRef]
- Bogdan, I.; Gadela, T.; Bratosin, F.; Dumitru, C.; Popescu, A.; Horhat, F.G.; Negrean, R.A.; Horhat, R.M.; Mot, I.C.; Bota, A.V.; et al. The Assessment of Multiplex PCR in Identifying Bacterial Infections in Patients Hospitalized with SARS-CoV-2 Infection: A Systematic Review. Antibiotics 2023, 12, 465. [Google Scholar]
- Cruceriu, D.; Baldasici, O.; Balacescu, L.; Gligor-Popa, S.; Flonta, M.; Man, M.A.; Visan, S.; Vlad, C.; Trifa, A.P.; Balacescu, O.; et al. Critical Aspects Concerning the Development of a Pooling Approach for SARS-CoV-2 Diagnosis Using Large-Scale PCR Testing. Viruses 2021, 13, 902. [Google Scholar] [CrossRef]
- Charlton, C.; Kanji, J.; Tran, V.; Kus, J.; Gubbay, J.; Osiowy, C.; Robinson, J.; Sekirov, I.; Drebot, M.; Hatchette, T.; et al. Practical guidance for clinical laboratories for SARS-CoV-2 serology testing. Can. Commun. Dis. Rep. 2021, 47, 171–183. [Google Scholar] [CrossRef]
- Falzone, L.; Gattuso, G.; Tsatsakis, A.; Spandidos, D.; Libra, M. Current and innovative methods for the diagnosis of COVID-19 infection (Review). Int. J. Mol. Med. 2021, 47, 100. [Google Scholar] [CrossRef]
- Petrovan, V.; Vrajmasu, V.; Bucur, A.C.; Soare, D.S.; Radu, E.; Dimon, P.; Zaulet, M. Evaluation of Commercial qPCR Kits for Detection of SARS-CoV-2 in Pooled Samples. Diagnostics 2020, 10, 472. [Google Scholar] [CrossRef]
- Motoc, N.S.; Ruta, V.-M.; Man, M.A.; Ungur, R.A.; Ciortea, V.M.; Irsay, L.; Nicola, A.; Valean, D.; Usatiuc, L.O.; Matei, I.R.; et al. Factors Associated with Prolonged RT-PCR SARS-CoV-2 Positive Testing in Patients with Mild and Moderate Forms of COVID-19: A Retrospective Study. Medicina 2022, 58, 707. [Google Scholar] [CrossRef]
- Cismaru, C.A.; Chira, S.; Cismaru, G.L.; Nutu, A.M.; Netea, M.G.; Berindan-Neagoe, I. Assessment of the frequency of coughing and sneezing triggered by nasopharyngeal swabbing in the pandemic setting. Sci. Rep. 2022, 12, 10874. [Google Scholar] [CrossRef]
- Simbar, M.; Nazarpour, S.; Sheidaei, A. Evaluation of pregnancy outcomes in mothers with COVID-19 infection: A systematic review and meta-analysis. J. Obstet. Gynaecol. 2023, 43, 2162867. [Google Scholar] [CrossRef] [PubMed]
- Citu, C.; Neamtu, R.; Sorop, V.-B.; Horhat, D.I.; Gorun, F.; Tudorache, E.; Gorun, O.M.; Boarta, A.; Tuta-Sas, I.; Citu, I.M. Assessing SARS-CoV-2 Vertical Transmission and Neonatal Complications. J. Clin. Med. 2021, 10, 5253. [Google Scholar] [CrossRef]
- Marnell, L.; Mold, C.; Du Clos, T.W. C-reactive protein: Ligands, receptors and role in inflammation. Clin. Immunol. 2005, 117, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Pepys, M.B.; Hirschfield, G.M. C-reactive protein: A critical update. J. Clin. Investig. 2003, 111, 1805–1812. [Google Scholar] [CrossRef]
- Gao, Y.; Li, T.; Han, M.; Li, X.; Wu, D.; Xu, Y.; Zhu, Y.; Liu, Y.; Wang, X.; Wang, L. Diagnostic utility of clinical laboratory data determinations for patients with the severe COVID-19. J. Med. Virol. 2020, 92, 791–796. [Google Scholar] [CrossRef] [PubMed]
- Drăgănescu, A.C.; Săndulescu, O.; Bilașco, A.; Kouris, C.; Streinu-Cercel, A.; Luminos, M.; Streinu-Cercel, A. Transient immune hepatitis as post-coronavirus disease complication: A case report. World J. Clin. Cases 2021, 9, 4032–4039. [Google Scholar] [CrossRef] [PubMed]
- Gavriliu, L.-C.; Murariu, C.; Potop, V.; Spătaru, R. Characteristics of the pediatric patients diagnosed with SARS-CoV-2 infection in a Romanian children’s hospital: A retrospective study. PeerJ 2021, 9, e11560. [Google Scholar] [PubMed]
- Mărginean, C.O.; Meliţ, L.E.; Săsăran, M.O. Pediatric Obesity—A Potential Risk Factor for Systemic Inflammatory Syndrome Associated to COVID-19, a Case Report. Front. Pediatr. 2021, 9, 681626. [Google Scholar] [CrossRef]
- Marza, A.M.; Petrica, A.; Buleu, F.N.; Mederle, O.A. Case Report: Massive Spontaneous Pneumothorax—A Rare Form of Presentation for Severe COVID-19 Pneumonia. Medicina 2021, 57, 82. [Google Scholar] [CrossRef]
- Bîrluțiu, V.; Șofariu, C.R. Association of hiccup and SARS-CoV-2 infection with the administration of dexamethasone: A case report. Germs 2022, 12, 107–111. [Google Scholar] [CrossRef]
- Cocoş, R.; Mahler, B.; Turcu-Stiolica, A.; Stoichiță, A.; Ghinet, A.; Shelby, E.-S.; Bohîlțea, L.C. Risk of Death in Comorbidity Subgroups of Hospitalized COVID-19 Patients Inferred by Routine Laboratory Markers of Systemic Inflammation on Admission: A Retrospective Study. Viruses 2022, 14, 1201. [Google Scholar] [CrossRef]
- Cut, T.G.; Ciocan, V.; Novacescu, D.; Voicu, A.; Marinescu, A.R.; Lazureanu, V.E.; Muresan, C.O.; Enache, A.; Dumache, R. Autopsy Findings and Inflammatory Markers in SARS-CoV-2: A Single-Center Experience. Int. J. Gen. Med. 2022, 15, 8743–8753. [Google Scholar] [PubMed]
- Filip, F.; Terteliu Baitan, M.; Avramia, R.; Filip, R. Acute Appendicitis in COVID-19-Positive Children: Report of 4 Cases from an Endemic Area in Northeastern Romania. Int. J. Environ. Res. Public Health 2022, 20, 706. [Google Scholar] [CrossRef]
- Huțanu, A.; Georgescu, A.M.; Voidăzan, S.; Andrejkovits, A.V.; Negrea, V.; Dobreanu, M. Low Serum Vitamin D in COVID-19 Patients Is Not Related to Inflammatory Markers and Patients’ Outcomes—A Single-Center Experience and a Brief Review of the Literature. Nutrients 2022, 14, 1998. [Google Scholar] [CrossRef]
- Marinescu, A.R.; Lazureanu, V.E.; Musta, V.F.; Nicolescu, N.D.; Mocanu, A.; Cut, T.G.; Muresan, C.O.; Tudoran, C.; Licker, M.; Laza, R. Severe Thrombocytopenic Purpura Associated with COVID-19 in a Pediatric Patient. Infect. Drug Resist. 2022, 15, 3405–3415. [Google Scholar] [CrossRef]
- Nistor, C.-E.; Pantile, D.; Stanciu-Gavan, C.; Ciuche, A.; Moldovan, H. Diagnostic and Therapeutic Characteristics in Patients with Pneumotorax Associated with COVID-19 versus Non-COVID-19 Pneumotorax. Medicina 2022, 58, 1242. [Google Scholar] [CrossRef] [PubMed]
- Novacescu, A.N.; Buzzi, B.; Bedreag, O.; Papurica, M.; Rogobete, A.F.; Sandesc, D.; Sorescu, T.; Baditoiu, L.; Musuroi, C.; Vlad, D.; et al. Bacterial and Fungal Superinfections in COVID-19 Patients Hospitalized in an Intensive Care Unit from Timișoara, Romania. Infect. Drug Resist. 2022, 15, 7001–7014. [Google Scholar] [CrossRef]
- Pilut, C.N.; Citu, C.; Gorun, F.; Bratosin, F.; Gorun, O.M.; Burlea, B.; Citu, I.M.; Grigoras, M.L.; Manolescu, D.; Gluhovschi, A. The Utility of Laboratory Parameters for Cardiac Inflammation in Heart Failure Patients Hospitalized with SARS-CoV-2 Infection. Diagnostics 2022, 12, 824. [Google Scholar] [CrossRef] [PubMed]
- Rădulescu, A.; Lupse, M.; Istrate, A.; Calin, M.; Topan, A.; Kormos, N.F.; Macicasan, R.V.; Briciu, V. External Validation of Mortality Scores among High-Risk COVID-19 Patients: A Romanian Retrospective Study in the First Pandemic Year. J. Clin. Med. 2022, 11, 5630. [Google Scholar] [CrossRef] [PubMed]
- Roman, A.; Moldovan, S.; Stoian, M.; Tilea, B.; Dobru, D. SARS-CoV-2 associated liver injury: A six-month follow-up analysis of liver function recovery. Med. Pharm. Rep. 2022, 95, 393–399. [Google Scholar] [CrossRef]
- Todor, S.-B.; Bîrluțiu, V.; Topîrcean, D.; Mihăilă, R.-G. Role of biological markers and CT severity score in predicting mortality in patients with COVID-19: An observational retrospective study. Exp. Ther. Med. 2022, 24, 698. [Google Scholar] [CrossRef]
- Ungureanu, R.; Cobilinschi, C.; Cotae, A.-M.; Darie, R.; Tincu, R.; Constantinescu, S.; Avram, O.; Moldovan, H.; Grintescu, I.M.; Mirea, L. Hemorrhagic Cardiac Tamponade—An Unusual Threat in the COVID-19 Recovery Phase. Medicina 2022, 59, 3. [Google Scholar] [CrossRef]
- Voiosu, A.; Roman, A.; Pop, R.; Boeriu, A.; Popp, C.; Zurac, S.; Voiosu, T.; Dobru, D.; Mateescu, B. Characteristics and outcomes of patients with COVID-19 and liver injury: A retrospective analysis and a multicenter experience. Rom. J. Intern. Med. 2022, 60, 49–55. [Google Scholar] [CrossRef]
- Merticariu, C.I.; Merticariu, M.; Cobzariu, C.; Mihai, M.M.; Dragomir, M.S. Pediatric inflammatory multisystem syndrome induced Panuveitis associated with SARS-CoV-2 infection: What the Ophthalmologists need to know. Rom. J. Ophthalmol. 2022, 66, 198–208. [Google Scholar]
- Cut, T.G.; Mavrea, A.; Cumpanas, A.A.; Novacescu, D.; Oancea, C.I.; Bratosin, F.; Marinescu, A.R.; Laza, R.; Mocanu, A.; Pescariu, A.S.; et al. A Retrospective Assessment of Sputum Samples and Antimicrobial Resistance in COVID-19 Patients. Pathogens 2023, 12, 620. [Google Scholar] [CrossRef]
- Mihai, C.M.; Chisnoiu, T.; Balasa, A.L.; Frecus, C.E.; Mihai, L.; Pantazi, A.C.; Stuparu, A.Z.; Axelerad, A. Clinical Characteristics and Laboratory Findings in Children with Multisystem Inflammatory Syndrome (MIS-C)—A Retrospective Study of a Tertiary Care Center from Constanta, Romania. Healthcare 2023, 11, 544. [Google Scholar] [CrossRef] [PubMed]
- Muntean, I.A.; Pintea, I.; Bocsan, I.C.; Dobrican, C.T.; Deleanu, D. COVID-19 Disease Leading to Chronic Spontaneous Urticaria Exacerbation: A Romanian Retrospective Study. Healthcare 2021, 9, 1144. [Google Scholar] [CrossRef] [PubMed]
- Laza, R.; Musta, V.F.; Nicolescu, N.D.; Marinescu, A.R.; Mocanu, A.; Vilceanu, L.; Paczeyka, R.; Cut, T.G.; Lazureanu, V.E. Cutaneous Manifestations in SARS-CoV-2 Infection—A Series of Cases from the Largest Infectious Diseases Hospital in Western Romania. Healthcare 2021, 9, 800. [Google Scholar] [CrossRef]
- Cerbu, B.; Grigoras, M.L.; Bratosin, F.; Bogdan, I.; Citu, C.; Bota, A.V.; Timircan, M.; Bratu, M.L.; Levai, M.C.; Marincu, I. Laboratory Profile of COVID-19 Patients with Hepatitis C-Related Liver Cirrhosis. J. Clin. Med. 2022, 11, 652. [Google Scholar] [CrossRef]
- Tudoran, M.; Tudoran, C.; Lazureanu, V.; Marinescu, A.; Pop, G.; Pescariu, A.; Enache, A.; Cut, T. Alterations of Left Ventricular Function Persisting during Post-Acute COVID-19 in Subjects without Previously Diagnosed Cardiovascular Pathology. J. Pers. Med. 2021, 11, 225. [Google Scholar] [CrossRef]
- Tudoran, C.; Bende, F.; Bende, R.; Giurgi-Oncu, C.; Dumache, R.; Tudoran, M. Correspondence between Aortic and Arterial Stiffness, and Diastolic Dysfunction in Apparently Healthy Female Patients with Post-Acute COVID-19 Syndrome. Biomedicines 2023, 11, 492. [Google Scholar] [CrossRef]
- Dima, A.; Popescu, D.N.; Moroti, R.; Stoica, E.; State, G.; Negoi, F.; Berza, I.A.; Parvu, M. Antiphospholipid Antibodies Occurrence in Acute SARS-CoV-2 Infection without Overt Thrombosis. Biomedicines 2023, 11, 1241. [Google Scholar] [CrossRef]
- Reștea, P.-A.; Mureșan, M.; Voicu, A.; Jurca, T.; Pallag, A.; Marian, E.; Vicaș, L.G.; Jeican, I.I.; Crivii, C.-B. Antidiabetic Treatment before Hospitalization and Admission Parameters in Patients with Type 2 Diabetes, Obesity, and SARS-CoV-2 Viral Infection. J. Pers. Med. 2023, 13, 392. [Google Scholar] [CrossRef]
- Gradisteanu Pircalabioru, G.; Grigore, G.A.; Czobor Barbu, I.; Chifiriuc, M.-C.; Savu, O. Impact of COVID-19 on the Microbiome and Inflammatory Status of Type 2 Diabetes Patients. Biomedicines 2023, 11, 179. [Google Scholar] [CrossRef] [PubMed]
- Citu, C.; Gorun, O.M.; Motoc, A.; Citu, I.M.; Gorun, F.; Malita, D. Correlation of Lung Damage on CT Scan with Laboratory Inflammatory Markers in COVID-19 Patients: A Single-Center Study from Romania. J. Clin. Med. 2022, 11, 4299. [Google Scholar] [CrossRef] [PubMed]
- Bende, F.; Tudoran, C.; Sporea, I.; Fofiu, R.; Bâldea, V.; Cotrău, R.; Popescu, A.; Sirli, R.; Ungureanu, B.S.; Tudoran, M. A Multidisciplinary Approach to Evaluate the Presence of Hepatic and Cardiac Abnormalities in Patients with Post-Acute COVID-19 Syndrome—A Pilot Study. J. Clin. Med. 2021, 10, 2507. [Google Scholar] [CrossRef]
- Miftode, R.-S.; Costache, I.-I.; Cianga, P.; Petris, A.O.; Cianga, C.-M.; Maranduca, M.-A.; Miftode, I.-L.; Constantinescu, D.; Timpau, A.-S.; Crisan, A.; et al. The Influence of Socioeconomic Status on the Prognosis and Profile of Patients Admitted for Acute Heart Failure during COVID-19 Pandemic: Overestimated Aspects or a Multifaceted Hydra of Cardiovascular Risk Factors? Healthcare 2021, 9, 1700. [Google Scholar] [CrossRef]
- Mocanu, A.; Lazureanu, V.E.; Marinescu, A.R.; Cut, T.G.; Laza, R.; Rusu, L.-C.; Marza, A.M.; Nelson-Twakor, A.; Negrean, R.A.; Popescu, I.-M.; et al. A Retrospective Assessment of Laboratory Findings and Cytokine Markers in Severe SARS-CoV-2 Infection among Patients of Roma Population. J. Clin. Med. 2022, 11, 6777. [Google Scholar] [CrossRef]
- Mocanu, A.; Lazureanu, V.E.; Laza, R.; Marinescu, A.R.; Cut, T.G.; Sincaru, S.-V.; Marza, A.M.; Popescu, I.-M.; Herlo, L.-F.; Nelson-Twakor, A.; et al. Laboratory Findings and Clinical Outcomes of ICU-admitted COVID-19 Patients: A Retrospective Assessment of Particularities Identified among Romanian Minorities. J. Pers. Med. 2023, 13, 195. [Google Scholar] [CrossRef] [PubMed]
- Pavel-Tanasa, M.; Constantinescu, D.; Cianga, C.M.; Anisie, E.; Mereuta, A.I.; Tuchilus, C.G.; Cianga, P. Adipokines, and not vitamin D, associate with antibody immune responses following dual BNT162b2 vaccination within individuals younger than 60 years. Front. Immunol. 2022, 13, 1000006. [Google Scholar] [CrossRef] [PubMed]
- Totan, M.; Gligor, F.G.; Duică, L.; Grigore, N.; Silișteanu, S.; Maniu, I.; Antonescu, E. A Single-Center (Sibiu, Romania), Retrospective Study (March–November 2020) of COVID-19 Clinical and Epidemiological Features in Children. J. Clin. Med. 2021, 10, 3517. [Google Scholar] [CrossRef]
- Bagiu, I.C.; Scurtu, I.L.; Horhat, D.I.; Mot, I.C.; Horhat, R.M.; Bagiu, R.V.; Capraru, I.D.; Diaconu, M.M.; Adam, O.; Ciornei, B.; et al. COVID-19 Inflammatory Markers and Vitamin D Relationship in Pediatric Patients. Life 2022, 13, 91. [Google Scholar] [CrossRef] [PubMed]
- Capraru, I.D.; Vulcanescu, D.D.; Bagiu, I.C.; Horhat, F.G.; Popescu, I.M.; Baditoiu, L.M.; Muntean, D.; Licker, M.; Radulescu, M.; Mot, I.C.; et al. COVID-19 Biomarkers Comparison: Children, Adults and Elders. Medicina 2023, 59, 877. [Google Scholar] [CrossRef]
- Pál, K.; Molnar, A.A.; Huțanu, A.; Szederjesi, J.; Branea, I.; Timár, Á.; Dobreanu, M. Inflammatory Biomarkers Associated with In-Hospital Mortality in Critical COVID-19 Patients. Int. J. Mol. Sci. 2022, 23, 10423. [Google Scholar] [CrossRef]
- Timpau, A.-S.; Miftode, R.-S.; Petris, A.O.; Costache, I.-I.; Miftode, I.-L.; Rosu, F.M.; Anton-Paduraru, D.-T.; Leca, D.; Miftode, E.G. Mortality Predictors in Severe COVID-19 Patients from an East European Tertiary Center: A Never-Ending Challenge for a No Happy Ending Pandemic. J. Clin. Med. 2021, 11, 58. [Google Scholar] [CrossRef] [PubMed]
- Paranga, T.G.; Pavel-Tanasa, M.; Constantinescu, D.; Plesca, C.E.; Petrovici, C.; Miftode, I.-L.; Moscalu, M.; Cianga, P.; Miftode, E.G. Comparison of C-reactive protein with distinct hyperinflammatory biomarkers in association with COVID-19 severity, mortality and SARS-CoV-2 variants. Front. Immunol. 2023, 14, 1213246. [Google Scholar] [CrossRef]
- Davidescu, E.I.; Odajiu, I.; Tulbǎ, D.; Sandu, C.D.; Bunea, T.; Sandu, G.; Mureşanu, D.F.; Bǎlǎnescu, P.; Popescu, B.O. Prognostic Factors in COVID-19 Patients with New Neurological Manifestations: A Retrospective Cohort Study in a Romanian Neurology Department. Front. Aging Neurosci. 2021, 13, 645611. [Google Scholar] [CrossRef]
- Mihai, C.; Chisnoiu, T.; Cambrea, C.; Frecus, C.; Mihai, L.; Balasa, A.; Stroe, A.; Gogu, A.; Axelerad, A. Neurological manifestations found in children with multisystem inflammatory syndrome. Exp. Ther. Med. 2022, 23, 261. [Google Scholar] [CrossRef] [PubMed]
- Iacob, D.; Enatescu, I.; Dima, M.; Bernad, E.; Pantea, M.; Bozgan, D.; Bernad, S.; Craina, M. First Neonates with Vertical Transmission of SARS-CoV-2 Infection in Late Pregnancy in West Part of Romania: Case Series. Diagnostics 2022, 12, 1668. [Google Scholar] [CrossRef]
- To, K.K.W.; Hung, I.F.N.; Li, I.W.S.; Lee, K.; Koo, C.; Yan, W.; Liu, R.; Ho, K.; Chu, K.; Watt, C.; et al. Delayed Clearance of Viral Load and Marked Cytokine Activation in Severe Cases of Pandemic H1N1 2009 Influenza Virus Infection. Clin. Infect. Dis. 2010, 50, 850–859. [Google Scholar] [CrossRef] [PubMed]
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersall, R.S.; Manson, J.J. COVID-19: Consider cytokine storm syndromes and immunosuppression. Lancet 2020, 395, 1033–1034. [Google Scholar] [CrossRef] [PubMed]
- Marc, F.; Moldovan, C.M.; Hoza, A.; Magheru, S.; Ciavoi, G.; Farcas, D.M.; Sachelarie, L.; Calin, G.; Romila, L.; Damir, D.; et al. Comparative Study of Cytokine Storm Treatment in Patients with COVID-19 Pneumonia Using Immunomodulators. J. Clin. Med. 2022, 11, 2945. [Google Scholar] [CrossRef] [PubMed]
- Novacescu, A.; Duma, G.; Buzzi, B.; Baditoiu, L.; Bedreag, O.; Papurica, M.; Sandesc, D.; Sorescu, T.; Vlad, D.; Licker, M. Therapeutic plasma exchange followed by convalescent plasma transfusion in severe and critically ill COVID-19 patients: A single centre non-randomized controlled trial. Exp. Ther. Med. 2021, 23, 76. [Google Scholar] [CrossRef]
- Tirnea, L.; Bratosin, F.; Vidican, I.; Cerbu, B.; Turaiche, M.; Timircan, M.; Margan, M.-M.; Marincu, I. The Efficacy of Convalescent Plasma Use in Critically Ill COVID-19 Patients. Medicina 2021, 57, 257. [Google Scholar] [CrossRef]
- Radulescu, A.; Istrate, A.; Muntean, M. Treatment with Tocilizumab in Adult Patients with Moderate to Critical COVID-19 Pneumonia: A Single-Center Retrospective Study. Int. J. Infect. Dis. 2022, 117, 1–7. [Google Scholar] [CrossRef]
- Hasanvand, A. COVID-19 and the role of cytokines in this disease. Inflammopharmacology 2022, 30, 789–798. [Google Scholar] [CrossRef] [PubMed]
- Cut, T.G.; Tudoran, C.; Lazureanu, V.E.; Marinescu, A.R.; Dumache, R.; Tudoran, M. Spontaneous Pneumomediastinum, Pneumothorax, Pneumopericardium and Subcutaneous Emphysema—Not So Uncommon Complications in Patients with COVID-19 Pulmonary Infection—A Series of Cases. J. Clin. Med. 2021, 10, 1346. [Google Scholar] [CrossRef]
- Tudoran, C.; Tudoran, M.; Lazureanu, V.E.; Marinescu, A.R.; Pop, G.N.; Pescariu, A.S.; Enache, A.; Cut, T.G. Evidence of Pulmonary Hypertension after SARS-CoV-2 Infection in Subjects without Previous Significant Cardiovascular Pathology. J. Clin. Med. 2021, 10, 199. [Google Scholar] [CrossRef]
- Szabo, R.; Petrisor, C.; Bodolea, C.; Simon, R.; Maries, I.; Tranca, S.; Mocan, T. Hyperferritinemia, Low Circulating Iron and Elevated Hepcidin May Negatively Impact Outcome in COVID-19 Patients: A Pilot Study. Antioxidants 2022, 11, 1364. [Google Scholar] [CrossRef]
- Huțanu, A.; Manu, D.; Gabor, M.R.; Văsieșiu, A.M.; Andrejkovits, A.V.; Dobreanu, M. Dynamic Evaluation of Natural Killer Cells Subpopulations in COVID-19 Patients. Int. J. Mol. Sci. 2022, 23, 11875. [Google Scholar] [CrossRef]
- Trofin, F.; Dorneanu, O.S.; Constantinescu, D.; Nastase, E.V.; Luncă, C.; Iancu, L.S.; Andrioaie, I.-M.; Duhaniuc, A.; Cianga, C.M.; Pavel-Tanasa, M.; et al. Cytokines and Chemokines in Breastmilk of SARS-CoV-2 Infected or COVID-19 Vaccinated Mothers. Vaccines 2022, 10, 2001. [Google Scholar] [CrossRef] [PubMed]
- Szarpak, L.; Ruetzler, K.; Safiejko, K.; Hampel, M.; Pruc, M.; Kanczuga-Koda, L.; Filipiak, K.J.; Jaguszewski, M.J. Lactate dehydrogenase level as a COVID-19 severity marker. Am. J. Emerg. Med. 2021, 45, 638–639. [Google Scholar] [CrossRef] [PubMed]
- Drent, M.; Cobben, N.; Henderson, R.; Wouters, E.; van Dieijen-Visser, M. Usefulness of lactate dehydrogenase and its isoenzymes as indicators of lung damage or inflammation. Eur. Respir. J. 1996, 9, 1736–1742. [Google Scholar] [CrossRef]
- Craina, M.; Iacob, D.; Dima, M.; Bernad, S.; Silaghi, C.; Moza, A.; Pantea, M.; Gluhovschi, A.; Bernad, E. Clinical, Laboratory, and Imaging Findings of Pregnant Women with Possible Vertical Transmission of SARS-CoV-2—Case Series. Int. J. Environ. Res. Public Health 2022, 19, 10916. [Google Scholar] [CrossRef] [PubMed]
- Pinte, L.; Sorohan, B.M.; Prohászka, Z.; Gherghiceanu, M.; Băicuş, C. COVID-19: A trigger for severe thrombotic microangiopathy in a patient with complement gene variant. Rom. J. Intern. Med. 2022, 60, 138–142. [Google Scholar] [CrossRef]
- Hannah, J.R.; Ali, S.S.; Nagra, D.; Adas, M.A.; Buazon, A.D.; Galloway, J.B.; Gordon, P.A. Skeletal muscles and COVID-19: A systematic review of rhabdomyolysis and myositis in SARS-CoV-2 infection. Clin. Exp. Rheumatol. 2022, 40, 329–338. [Google Scholar] [CrossRef] [PubMed]
- Zaharie, G.; Hasmasanu, M.; Muresan, D.; Kovacs, T.; Matyas, M. Diagnostic challenges, management, and outcome of infants born to mothers with COVID 19 during the first wave of the pandemic. Exp. Ther. Med. 2022, 23, 102. [Google Scholar] [CrossRef] [PubMed]
- Meliț, L.E.; Mărginean, C.O.; Fleșeriu, T.; Văsieșiu, A.M.; Ghiga, D.V.; Koller, A.-M.R. COVID-19 and PIMS—Two Different Entities, but the Same Trigger. Children 2022, 9, 1348. [Google Scholar] [CrossRef]
- Kim, C.W.; Aronow, W.S. COVID-19, cardiovascular diseases and cardiac troponins. Future Cardiol. 2022, 18, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Bielecka-Dabrowa, A.; Cichocka-Radwan, A.; Lewek, J.; Pawliczak, F.; Maciejewski, M.; Banach, M. Cardiac manifestations of COVID-19. Rev. Cardiovasc. Med. 2021, 22, 365. [Google Scholar] [CrossRef]
- Haliga, R.E.; Sorodoc, V.; Lionte, C.; Petris, O.R.; Bologa, C.; Coman, A.E.; Vata, L.G.; Puha, G.; Dumitrescu, G.; Sirbu, O.; et al. Acute Clinical Syndromes and Suspicion of SARS-CoV-2 Infection: The Experience of a Single Romanian Center in the Early Pandemic Period. Medicina 2021, 57, 121. [Google Scholar] [CrossRef]
- Suriawinata, E.; Mehta, K.J. Iron and iron-related proteins in COVID-19. Clin. Exp. Med. 2023, 23, 969–991. [Google Scholar] [CrossRef]
- Uta, M.; Neamtu, R.; Bernad, E.; Mocanu, A.G.; Gluhovschi, A.; Popescu, A.; Dahma, G.; Dumitru, C.; Stelea, L.; Citu, C.; et al. The Influence of Nutritional Supplementation for Iron Deficiency Anemia on Pregnancies Associated with SARS-CoV-2 Infection. Nutrients 2022, 14, 836. [Google Scholar] [CrossRef] [PubMed]
- Iancu, G.M.; Solomon, A.; Birlutiu, V. Viral exanthema as manifestation of SARS-CoV-2 infection. Medicine 2020, 99, e21810. [Google Scholar] [CrossRef]
- Szabo, R.; Petrișor, C.; Bodolea, C.; Dobre, V.; Tranca, S.; Clichici, S.; Szabo, I.; Melinte, R.M.; Mocan, T. Effects of Tocilizumab on Inflammation and Iron Metabolism in Critically Ill Patients with COVID-19. Pharmaceutics 2023, 15, 646. [Google Scholar] [CrossRef]
- Kočar, E.; Režen, T.; Rozman, D. Cholesterol, lipoproteins, and COVID-19: Basic concepts and clinical applications. Biochim. Biophys. Acta (BBA)–Mol. Cell Biol. Lipids 2021, 1866, 158849. [Google Scholar] [CrossRef]
- Julius, U.; Schatz, U.; Tselmin, S.; Morawietz, H. COVID-19 and Lipid Disorders. Horm. Metab. Res. 2022, 54, 514–521. [Google Scholar] [CrossRef]
- Tudoran, C.; Bende, R.; Bende, F.; Giurgi-Oncu, C.; Enache, A.; Dumache, R.; Tudoran, M. Connections between Diabetes Mellitus and Metabolic Syndrome and the Outcome of Cardiac Dysfunctions Diagnosed during the Recovery from COVID-19 in Patients without a Previous History of Cardiovascular Diseases. Biology 2023, 12, 370. [Google Scholar] [CrossRef]
- Făgărășan, I.; Rusu, A.; Cristea, M.; Bala, C.G.; Vulturar, D.M.; Cristea, C.; Todea, D.A. Predictors of New-Onset Diabetes in Hospitalized Patients with SARS-CoV-2 Infection. Int. J. Environ. Res. Public Health 2022, 19, 13230. [Google Scholar] [CrossRef]
- Tian, W.; Jiang, W.; Yao, J.; Nicholson, C.J.; Li, R.H.; Sigurslid, H.H.; Wooster, L.; Rotter, J.I.; Guo, X.; Malhotra, R. Predictors of mortality in hospitalized COVID-19 patients: A systematic review and meta-analysis. J. Med. Virol. 2020, 92, 1875–1883. [Google Scholar] [CrossRef] [PubMed]
- Wijarnpreecha, K.; Ungprasert, P.; Panjawatanan, P.; Harnois, D.M.; Zaver, H.B.; Ahmed, A.; Kim, D. COVID-19 and liver injury: A meta-analysis. Eur. J. Gastroenterol. Hepatol. 2020, 33, 990–995. [Google Scholar] [CrossRef]
- Cristea, A.M.; Zaharia, D.C.; Leu, S.; Bogdan, M.A. Complications during Hospitalization in Patients with SARS-CoV-2 Pneumonia in a Romanian Pulmonary Center. Cureus 2023, 15, e33882. [Google Scholar] [CrossRef] [PubMed]
- Jugulete, G.; Luminos, M.; Pavelescu, C.; Merișescu, M.M. Remdesivir Efficacy and Tolerability in Children with COVID-19-Associated Allergic Comorbidities such as Asthma, Allergic Rhinitis, and Atopic Dermatitis. Children 2023, 10, 810. [Google Scholar] [CrossRef] [PubMed]
- Yılmaz, K.; Şen, V. Is vitamin D deficiency a risk factor for COVID-19 in children? Pediatr. Pulmonol. 2020, 55, 3595–3601. [Google Scholar] [CrossRef]
- Subramanian, S.; Griffin, G.; Hewison, M.; Hopkin, J.; Kenny, R.A.; Laird, E.; Quinton, R.; Thickett, D.; Rhodes, J.M. Vitamin D and COVID-19—Revisited. J. Intern. Med. 2022, 292, 604–626. [Google Scholar] [CrossRef]
- Topan, A.; Lupse, M.; Calin, M.; Jianu, C.; Leucuta, D.-C.; Briciu, V. 25 Hydroxyvitamin D Serum Concentration and COVID-19 Severity and Outcome—A Retrospective Survey in a Romanian Hospital. Nutrients 2023, 15, 1227. [Google Scholar] [CrossRef] [PubMed]
- Dumache, R.; Enache, A.; Cut, T.; Paul, C.; Mihailescu, A.; Ionescu, A.; Novacescu, D.; Marinescu, A.; Ciocan, V.; Muresan, C.; et al. Deficiency of Vitamin D, a Major Risk Factor for SARS-CoV-2 Severity. Clin. Lab. 2022, 68. [Google Scholar] [CrossRef] [PubMed]
- Hu, R.; Han, C.; Pei, S.; Yin, M.; Chen, X. Procalcitonin levels in COVID-19 patients. Int. J. Antimicrob. Agents 2020, 56, 106051. [Google Scholar] [CrossRef]
- Eljilany, I.; Elzouki, A.-N. D-Dimer, Fibrinogen, and IL-6 in COVID-19 Patients with Suspected Venous Thromboembolism: A Narrative Review. Vasc. Health Risk Manag. 2020, 16, 455–462. [Google Scholar] [CrossRef]
- Dumache, R.; Daescu, E.; Ciocan, V.; Mureşan, C.; Talida, C.; Gavrilita, D.; Enache, A. Molecular Testing of SARS-CoV-2 Infection from Blood Samples in Disseminated Intravascular Coagulation (DIC) and Elevated D-Dimer Levels. Clin. Lab. 2021, 67. [Google Scholar] [CrossRef] [PubMed]
- Lo, M.W.; Kemper, C.; Woodruff, T.M. COVID-19: Complement, Coagulation, and Collateral Damage. J. Immunol. 2020, 205, 1488–1495. [Google Scholar] [CrossRef]
- Afzali, B.; Noris, M.; Lambrecht, B.N.; Kemper, C. The state of complement in COVID-19. Nat. Rev. Immunol. 2021, 22, 77–84. [Google Scholar] [CrossRef]
- Tjendra, Y.; Al Mana, A.F.; Espejo, A.P.; Akgun, Y.; Millan, N.C.; Gomez-Fernandez, C.; Cray, C. Predicting Disease Severity and Outcome in COVID-19 Patients: A Review of Multiple Biomarkers. Arch. Pathol. Lab. Med. 2020, 144, 1465–1474. [Google Scholar] [CrossRef]
- Ponti, G.; Maccaferri, M.; Ruini, C.; Tomasi, A.; Ozben, T. Biomarkers associated with COVID-19 disease progression. Crit. Rev. Clin. Lab. Sci. 2020, 57, 389–399. [Google Scholar] [CrossRef]
- Palladino, M. Complete blood count alterations in COVID-19 patients. Biochem. Medica 2021, 31, 403–415. [Google Scholar] [CrossRef]
- Citu, C.; Gorun, F.; Motoc, A.; Sas, I.; Gorun, O.M.; Burlea, B.; Tuta-Sas, I.; Tomescu, L.; Neamtu, R.; Malita, D.; et al. The Predictive Role of NLR, d-NLR, MLR, and SIRI in COVID-19 Mortality. Diagnostics 2022, 12, 122. [Google Scholar] [CrossRef] [PubMed]
- Sava, C.N.; Bodog, T.M.; Niulas, L.R.; Iuhas, A.R.; Marinau, C.P.; Negrut, N.; Balmos, A.B.; Pasca, B.; Roman, N.A.; Delia Nistor-Cseppento, C. Biomarker Changes in Pediatric Patients with COVID-19: A Retrospective Study from a Single Center Database. In Vivo 2022, 36, 2813–2822. [Google Scholar] [CrossRef] [PubMed]
- Westblade, L.F.; Simon, M.S.; Satlin, M.J. Bacterial Coinfections in Coronavirus Disease 2019. Trends Microbiol. 2021, 29, 930–941. [Google Scholar] [CrossRef]
- Wu, H.-Y.; Chang, P.-H.; Chen, K.-Y.; Lin, I.-F.; Hsih, W.-H.; Tsai, W.-L.; Chen, J.-A.; Lee, S.S.-J. Coronavirus disease 2019 (COVID-19) associated bacterial coinfection: Incidence, diagnosis and treatment. J. Microbiol. Immunol. Infect. 2022, 55, 985–992. [Google Scholar] [CrossRef] [PubMed]
- Dumitru, I.; Dumitrascu, M.; Vlad, N.; Cernat, R.; Ilie-Serban, C.; Hangan, A.; Slujitoru, R.; Gherghina, A.; Mitroi-Maxim, C.; Curtali, L.; et al. Carbapenem-Resistant Klebsiella pneumoniae Associated with COVID-19. Antibiotics 2021, 10, 561. [Google Scholar] [CrossRef]
- Susan, M.; Susan, R.; Lazar, V.; Bagiu, I.-C.; Mihu, A.; Bagiu, R.; Ionescu, A.; Iana, A.; Dehelean, C.; Lighezan, D.; et al. COVID-19 association with multidrug-resistant bacteria superinfections: Lessons for future challenges. Exp. Ther. Med. 2023, 25, 254. [Google Scholar] [CrossRef]
- Cristinel Badiu, D.; Popescu, G.C.; Zgura, A.; Mercan Stanciu, A.; Dodot, M.D.; Mehedintu, C.; Toma, L.; Razvan, S.; Bacinschi, X.; Haineala, B. A Prospective Observational Study of 42 Patients with COVID-19 infection and a History of Hepatitis C Virus Infection and Thyroid Disease with Follow-Up Thyroid Function and Autoantibody Testing. Med. Sci. Monit. 2021, 27, e935075. [Google Scholar] [CrossRef]
- Anka, A.U.; Tahir, M.I.; Abubakar, S.D.; Alsabbagh, M.; Zian, Z.; Hamedifar, H.; Sabzevari, A.; Azizi, G. Coronavirus disease 2019 (COVID-19): An overview of the immunopathology, serological diagnosis and management. Scand. J. Immunol. 2020, 93, e12998. [Google Scholar] [CrossRef]
- Filchakova, O.; Dossym, D.; Ilyas, A.; Kuanysheva, T.; Abdizhamil, A.; Bukasov, R. Review of COVID-19 testing and diagnostic methods. Talanta 2022, 244, 123409. [Google Scholar] [CrossRef]
- Manolea, C.; Capitanescu, A.; Borș, R.; Rugescu, I.; Bechir, M.; Mehedintu, C.; Varlas, V. The prevalence of SARS-CoV-2 antibodies in triage-negative patients and staff of a fertility setting from lockdown release throughout 2020. Hum. Reprod. Open 2021, 2021, hoab028. [Google Scholar] [CrossRef]
- Radulescu, A.; Istrate, A.; Flonta, M.; Lupse, M. Antibody and viral RNA kinetics in SARS-CoV2 infected patients admitted to a Romanian University Hospital of Infectious Diseases. Int. J. Infect. Dis. 2021, 107, 205–211. [Google Scholar] [CrossRef]
- Maruntelu, I.; Caragea, A.M.; Tizu, M.; Constantinescu, I. SARS-CoV-2 diagnosis: A single-centre experience. J. Med. Life 2021, 14, 257–261. [Google Scholar] [CrossRef]
- Olariu, T.R.; Ursoniu, S.; Marincu, I.; Lupu, M.A. Dynamics of Antibody Response to BNT162b2 mRNA COVID-19 Vaccine: A 7-Month Follow-Up Study. Medicina 2021, 57, 1330. [Google Scholar] [CrossRef]
- Ionita, C.; Marcelli, D.; Nita, C.; Anton, C.; Berca, S.; Vacar, S.; Schiller, O.; Gheorghiu, C.; Barth, C. Comparison of antibody response to two different mRNA COVID-19 vaccines in patients on hemodialysis. J. Nephrol. 2022, 35, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Korodi, M.; Horváth, I.; Rákosi, K.; Jenei, Z.; Hudák, G.; Kákes, M.; Dallos-Fejér, K.; Simai, E.; Páll, O.; Staver, N.; et al. Longitudinal determination of BNT162b2 vaccine induced strongly binding SARS-CoV-2 IgG antibodies in a cohort of Romanian healthcare workers. Vaccine 2022, 40, 5445–5451. [Google Scholar] [CrossRef] [PubMed]
- Nedelcu, I.; Jipa, R.; Vasilescu, R.; Băicuș, C.; Popescu, C.-I.; Manea, E.; Stoichițoiu, L.E.; Pinte, L.; Damalan, A.; Simulescu, O.; et al. Long-Term Longitudinal Evaluation of Six Commercial Immunoassays for the Detection of IgM and IgG Antibodies against SARS CoV-2. Viruses 2021, 13, 1244. [Google Scholar] [CrossRef] [PubMed]
- Vâţă, A.; Anita, A.; Manciuc, C.; Savuta, G.; Luca, C.; Roșu, F.; Mihai, I.; Anita, D. Clinical significance of early IgA anti-SARS-CoV-2 antibody detection in patients from a Romanian referral COVID-19 hospital. Exp. Ther. Med. 2022, 23, 391. [Google Scholar] [CrossRef]
- Howard-Jones, A.R.; Burgner, D.P.; Crawford, N.W.; Goeman, E.; Gray, P.E.; Hsu, P.; Kuek, S.; McMullan, B.J.; Tosif, S.; Wurzel, D.; et al. COVID-19 in children. II: Pathogenesis, disease spectrum and management. J. Paediatr. Child Health 2022, 58, 46–53. [Google Scholar] [CrossRef]
- Filippatos, F.; Tatsi, E.B.; Michos, A. Immunology of Multisystem Inflammatory Syndrome after COVID-19 in Children: A Review of the Current Evidence. Int. J. Mol. Sci. 2023, 24, 5711. [Google Scholar] [CrossRef] [PubMed]
- Gottlieb, M.; Bridwell, R.; Ravera, J.; Long, B. Multisystem inflammatory syndrome in children with COVID-19. Am. J. Emerg. Med. 2021, 49, 148–152. [Google Scholar] [CrossRef]
- Williams, V.; Dash, N.; Suthar, R.; Mohandoss, V.; Jaiswal, N.; Kavitha, T.K.; Nallasamy, K.; Angurana, S.K. Clinicolaboratory Profile, Treatment, Intensive Care Needs, and Outcome of Pediatric Inflammatory Multisystem Syndrome Temporally Associated with SARS-CoV-2: A Systematic Review and Meta-analysis. J. Pediatr. Intensive Care 2020, 11, 1–12. [Google Scholar] [CrossRef]
- Lechuga, G.C.; Morel, C.M.; De-Simone, S.G. Hematological alterations associated with long COVID-19. Front. Physiol. 2023, 14, 1203472. [Google Scholar] [CrossRef] [PubMed]
- Goetzl, E.J.; Yao, P.J.; Kapogiannis, D. Prediction of Post-Acute-Sequelae of COVID-19 by Cargo Protein Biomarkers of Blood Total Extracellular Vesicles in Acute COVID-19. Am. J. Med. 2023, 136, 824–829. [Google Scholar] [CrossRef] [PubMed]
- Cismaru, C.; Elec, A.D.; Muntean, A.; Moisoiu, T.; Lupșe, M.; Antal, O.; Elec, F.I. Favipiravir in Kidney Transplant Recipients with COVID-19: A Romanian Case Series. Transplant. Proc. 2022, 54, 1489–1493. [Google Scholar] [CrossRef]
- Koureas, M.; Speletas, M.; Bogogiannidou, Z.; Babalis, D.; Pinakas, V.; Pinaka, O.; Komnos, A.; Tsoutsa, S.; Papadamou, G.; Kyritsi, M.A.; et al. Transmission Dynamics of SARS-CoV-2 during an Outbreak in a Roma Community in Thessaly, Greece-Control Measures and Lessons Learned. Int. J. Environ. Res. Public Health 2021, 18, 2878. [Google Scholar] [CrossRef]
- Cronin, A.; Ibrahim, N. A scoping review of literature exploring factors affecting vaccine uptake within Roma communities across Europe. Expert Rev. Vaccines 2022, 21, 1429–1442. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Assessment | General Role | Most Frequent Modification | Studied Populations | Predictive Ability (Ref.) | Clinical Associations (Ref.) |
|---|---|---|---|---|---|
| RT-PCR | Early detection; diagnosis | Positive | General | - | - |
| Antigen levels—IgM, IgG | Diagnosis; post-vaccination monitoring | Elevated | General | - | - |
| CRP | Disease severity assessment; monitoring progression; therapeutic guidance | Elevated | Adults, children, infants, elders, Roma | Yes, even more so in Roma [53,54,58,59,60,61,62,70] | Diabetes [48,94] Antiphospholipid syndrome [47] Hypertension [27] Cardiac dysfunction [46,73,93] Overweight/metabolic syndrome [27,54,93] Lung involvement [50,57] PIMS [83] Chronic Spontaneous Urticaria Exacerbation [42] Pneumothorax/pneumomediastinum [31,72] Liver failure [44] Multiple organ dysfunction [60] |
| LDH | Disease severity assessment; monitoring progression; therapeutic guidance | Elevated | General | Yes [57,58,61] | Lung involvement [57] Chronic Spontaneous Urticaria Exacerbation [42] |
| FER | Disease severity assessment | Elevated | Adults, children, elders | Yes [58,60,70] | Pneumothorax/pneumomediastinum [31,72] |
| HDL | Disease severity assessment | Elevated | Adults, children, elders | Yes [46,58,93] | - |
| Vitamin D | Disease severity assessment | Decreased | Adults, children, elders | Yes [57,58,102,103] No [55] | More comorbidities [29,101] Lung involvement [57] |
| PCT | Disease severity assessment; evaluation of complications | Elevated | Adults | Yes [36] | Diabetes [48] Co-/supra-infections [40,115,116] |
| D-dimers | Disease severity assessment; monitoring progression; evaluation of complications | Elevated | Adults, elders | Yes [26,36,60,105] | Hypertension, overweight [27] Cardiac dysfunction [73] Liver failure [44] PIMS [83] Pneumothorax/pneumomediastinum [31,72] Liver failure [44] Multiple organ dysfunction [60] |
| BUN | Disease severity assessment | Elevated | Adults | - | - |
| Neutrophils | Disease severity assessment; monitoring progression | Increased | General | - | - |
| Lymphocytes | Disease severity assessment; monitoring progression | Decreased | General | - | - |
| Platelets | Disease severity assessment; monitoring progression | Decreased | General | - | - |
| NLR | Disease severity assessment; monitoring progression; therapeutic guidance | Increased | General | Yes [26,29,36,48,111] | Lung involvement [50] |
| ESR | Evaluation of complications | Increased | Children | - | - |
| Cytokines—IL-1, IL-6, IL-8, IL-1β, IFN-γ, TNF-α, TGF- β | Monitoring progression; therapeutic guidance | Elevated | Adults, children, elders, Roma, pregnant and lactating women | Yes; IL-6, especially in Roma [36,53,59,60] | IL-6: hypertension, overweight [27,54]; lung involvement [50,72]; cardiac dysfunction [73]; multiple organ dysfunction [74]; liver failure [44] IL1β, IL-8: bacterial infection [49] |
| Tn’s | Monitoring progression | Elevated | Adults | Yes [33] No [21,86] | Cardiac dysfunction [33] |
| BNP | Monitoring progression | Elevated | Adults, children | Yes [33] No [21,86] | Cardiac dysfunction [33] |
| AST and ALT | Therapeutic guidance | Elevated | Remdesivir side-effects in children | - | |
| Fibrinogen | Evaluation of complications | Elevated | Adults, children | Yes [33,41,62] No [29,61,79] | PIMS [41] Cardiac dysfunction [33] |
| Creatinine | Evaluation of complications | Elevated | Children, elders, Roma | Yes [53,59,62,83] | PIMS [83] Renal dysfunction [41,59] |
| Albumin | Evaluation of complications | Decreased | Children | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Musat, O.; Sorop, V.B.; Sorop, M.I.; Lazar, V.; Marti, D.T.; Susan, M.; Avram, C.R.; Oprisoni, A.; Vulcanescu, D.D.; Horhat, F.G.; et al. COVID-19 and Laboratory Markers from Romanian Patients—A Narrative Review. Life 2023, 13, 1837. https://doi.org/10.3390/life13091837
Musat O, Sorop VB, Sorop MI, Lazar V, Marti DT, Susan M, Avram CR, Oprisoni A, Vulcanescu DD, Horhat FG, et al. COVID-19 and Laboratory Markers from Romanian Patients—A Narrative Review. Life. 2023; 13(9):1837. https://doi.org/10.3390/life13091837
Chicago/Turabian StyleMusat, Ovidiu, Virgiliu Bogdan Sorop, Madalina Ioana Sorop, Viorica Lazar, Daniela Teodora Marti, Monica Susan, Cecilia Roberta Avram, Andrada Oprisoni, Dan Dumitru Vulcanescu, Florin George Horhat, and et al. 2023. "COVID-19 and Laboratory Markers from Romanian Patients—A Narrative Review" Life 13, no. 9: 1837. https://doi.org/10.3390/life13091837
APA StyleMusat, O., Sorop, V. B., Sorop, M. I., Lazar, V., Marti, D. T., Susan, M., Avram, C. R., Oprisoni, A., Vulcanescu, D. D., Horhat, F. G., Bagiu, I. C., Horhat, D. I., & Diaconu, M. M. (2023). COVID-19 and Laboratory Markers from Romanian Patients—A Narrative Review. Life, 13(9), 1837. https://doi.org/10.3390/life13091837