
High Risk of Heart Tumors after COVID-19

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
6. Limitation of the Study
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Abbasi, J. The COVID Heart—One Year After SARS-CoV-2 Infection, Patients Have an Array of Increased Cardiovascular Risks. JAMA 2022, 327, 1113–1114. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.; Xu, E.; Bowe, B.; Al-Aly, Z. Long-term cardiovascular outcomes of COVID-19. Nat. Med. 2022, 28, 583–590. [Google Scholar] [CrossRef] [PubMed]
- Sato, K.; Sinclair, J.E.; Sadeghirad, H.; Fraser, J.F.; Short, K.R.; Kulasinghe, A. Cardiovascular disease in SARS-CoV-2 infection. Clin. Transl. Immunol. 2021, 10, e1343. [Google Scholar] [CrossRef]
- Makarov, I.; Mayrina, S.; Makarova, T.; Karonova, T.; Starshinova, A.; Kudlay, D.; Mitrofanova, L. Morphological Changes in the Myocardium of Patients with Post-Acute Coronavirus Syndrome: A Study of Endomyocardial Biopsies. Diagnostics 2023, 13, 2212. [Google Scholar] [CrossRef] [PubMed]
- Mitrofanova, L.B.; Makarov, I.A.; Gorshkov, A.N.; Runov, A.L.; Vonsky, M.S.; Pisareva, M.M.; Komissarov, A.B.; Makarova, T.A.; Li, Q.; Karonova, T.L.; et al. Comparative Study of the Myocardium of Patients from Four COVID-19 Waves. Diagnostics 2023, 13, 1645. [Google Scholar] [CrossRef] [PubMed]
- Zheng, H.Y.; Zhang, M.; Yang, C.X.; Zhang, N.; Wang, X.C.; Yang, X.P.; Dong, X.Q.; Zheng, Y.T. Elevated exhaustion levels and reduced functional diversity of T cells in peripheral blood may predict severe progression in COVID-19 patients. Cell. Mol. Immunol. 2020, 17, 541–543. [Google Scholar] [CrossRef]
- Starshinova, A.; Kudryavtsev, I.; Rubinstein, A.; Malkova, A.; Dovgaluk, I.; Kudlay, D. Tuberculosis and COVID-19 Dually Affect Human Th17 Cell Immune Response. Biomedicines 2023, 11, 2123. [Google Scholar] [CrossRef]
- Chen, J.; Lau, Y.F.; Lamirande, E.W.; Paddock, C.D.; Bartlett, J.H.; Zaki, S.R.; Subbarao, K. Cellular Immune Responses to Severe Acute Respiratory Syndrome Coronavirus (SARS-CoV) Infection in Senescent BALB/c Mice: CD4+T Cells Are Important in Control of SARS-CoV Infection. J. Virol. 2010, 84, 1289–1301. [Google Scholar] [CrossRef]
- Kozlov, V.A.; Tikhonova, E.P.; Savchenko, A.A.; Kudryavtsev, I.V.; Andronova, N.V.; Anisimova, E.N.; Golovkin, A.S.; Demina, D.V.; Zdzitovetsky, D.E.; Kalinina, Y.S.; et al. Clinical Immunology. A Practical Guide for Infectious Disease Specialists; Krasnoyarsk: Polikor, Russia, 2021; 563p. (In Russian) [Google Scholar] [CrossRef]
- Roberts, A.; Deming, D.; Paddock, C.D.; Cheng, A.; Yount, B.; Vogel, L.; Herman, B.D.; Sheahan, T.; Heise, M.; Genrich, G.L.; et al. A Mouse-Adapted SARS-Coronavirus Causes Disease and Mortality in BALB/c Mice. PLOS Pathog. 2007, 3, e5. [Google Scholar] [CrossRef]
- Kudlay, D.; Kofiadi, I.; Khaitov, M. Peculiarities of the T Cell Immune Response in COVID-19. Vaccines 2022, 10, 242. [Google Scholar] [CrossRef]
- Vasichkina, E.; Alekseeva, D.; Karev, V.; Podyacheva, E.; Kudryavtsev, I.; Glushkova, A.; Starshinova, A.Y.; Kudlay, D.; Starshinova, A. Cardiac Involvement in Children Affected by COVID-19: Clinical Features and Diagnosis. Diagnostics 2023, 13, 120. [Google Scholar] [CrossRef] [PubMed]
- Callegari, A.; Klingel, K.; Kelly-Geyer, J.; Berger, C.; Geiger, J.; Knirsch, W. Difficulties in diagnosis of SARS-CoV-2 myocarditis in an adolescent. Swiss Med. Wkly. 2022, 152, w30214. [Google Scholar] [CrossRef] [PubMed]
- Costanzo, M.; De Giglio, M.A.R.; Roviello, G.N. Deciphering the Relationship between SARS-CoV-2 and Cancer. Int. J. Mol. Sci. 2023, 24, 7803. [Google Scholar] [CrossRef] [PubMed]
- Rapti, V.; Tsaganos, T.; Vathiotis, I.A.; Syrigos, N.K.; Li, P.; Poulakou, G. New Insights into SARS-CoV-2 and Cancer Cross-Talk: Does a Novel Oncogenesis Driver Emerge? Vaccines 2022, 10, 1607. [Google Scholar] [CrossRef] [PubMed]
- Tutuncuoglu, B.; Cakir, M.; Batra, J.; Bouhaddou, M.; Eckhardt, M.; Gordon, D.E.; Krogan, N.J. The Landscape of Human Cancer Proteins Targeted by SARS-CoV-2. Cancer Discov. 2020, 10, 916–921. [Google Scholar] [CrossRef] [PubMed]
- Lara, O.D.; Smith, M.J.; Wang, Y.; O’cearbhaill, R.; Blank, S.V.; Kolev, V.; Carr, C.; Knisely, A.; McEachron, J.; Gabor, L.; et al. Racial disparities in patients with coronavirus disease 2019 infection and gynecologic malignancy. Cancer 2021, 127, 1057–1067. [Google Scholar] [CrossRef]
- Saini, G.; Aneja, R. Cancer as a prospective sequela of long COVID-19. BioEssays 2021, 43, e2000331. [Google Scholar] [CrossRef]
- Li, J.; Bai, H.; Qiao, H.; Du, C.; Yao, P.; Zhang, Y.; Cai, Y.; Jia, Y.; Wei, X.; Li, C.; et al. Causal effects of COVID-19 on cancer risk: A Mendelian randomization study. J. Med. Virol. 2023, 95, e28722. [Google Scholar] [CrossRef]
- Del Valle, D.M.; Kim-Schulze, S.; Huang, H.H.; Beckmann, N.D.; Nirenberg, S.; Wang, B.; Lavin, Y.; Swartz, T.H.; Madduri, D.; Stock, A.; et al. An inflammatory cytokine signature predicts COVID-19 severity and survival. Nat. Med. 2020, 26, 1636–1643. [Google Scholar] [CrossRef]
- Li, G.; Fan, Y.; Lai, Y.; Han, T.; Li, Z.; Zhou, P.; Pan, P.; Wang, W.; Hu, D.; Liu, X.; et al. Coronavirus infections and immune responses. J. Med. Virol. 2020, 92, 424–432. [Google Scholar] [CrossRef]
- Greten, F.R.; Grivennikov, S.I. Inflammation and Cancer: Triggers, Mechanisms, and Consequences. Immunity 2019, 51, 27–41. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; van Gent, D.C.; Incrocci, L.; van Weerden, W.M.; Nonnekens, J. Role of the DNA damage response in prostate cancer formation, progression and treatment. Prostate Cancer Prostatic Dis. 2020, 23, 24–37, Erratum in Prostate Cancer Prostatic Dis. 2019. [Google Scholar] [CrossRef] [PubMed]
- Kiwerska, K.; Szyfter, K. DNA repair in cancer initiation, progression, and therapy-a double-edged sword. J. Appl. Genet. 2019, 60, 329–334. [Google Scholar] [CrossRef] [PubMed]
- Mokhtari, T.; Hassani, F.; Ghaffari, N.; Ebrahimi, B.; Yarahmadi, A.; Hassanzadeh, G. COVID-19 and multiorgan failure: A narrative review on potential mechanisms. J. Mol. Histol. 2020, 51, 613–628. [Google Scholar] [CrossRef]
- Ma-Lauer, Y.; Carbajo-Lozoya, J.; Hein, M.Y.; Müller, M.A.; Deng, W.; Lei, J.; Meyer, B.; Kusov, Y.; von Brunn, B.; Bairad, D.R.; et al. p53 down-regulates SARS coronavirus replication and is targeted by the SARS-unique domain and PLpro via E3 ubiquitin ligase RCHY1. Proc. Natl. Acad. Sci. USA 2016, 113, E5192–E5201. [Google Scholar] [CrossRef]
- Singh, N.; Bharara Singh, A. S2 subunit of SARS-nCoV-2 interacts with tumor suppressor protein p53 and BRCA: An in silico study. Transl. Oncol. 2020, 13, 100814. [Google Scholar] [CrossRef]
- Mantovani, F.; Collavin, L.; Del Sal, G. Mutant p53 as a guardian of the cancer cell. Cell Death Differ. 2019, 26, 199–212. [Google Scholar] [CrossRef]
- Ozaki, T.; Nakagawara, A. Role of p53 in Cell Death and Human Cancers. Cancers 2011, 3, 994–1013. [Google Scholar] [CrossRef]
- Gorodetska, I.; Kozeretska, I.; Dubrovska, A. BRCA Genes: The Role in Genome Stability, Cancer Stemness and Therapy Resistance. J. Cancer 2019, 10, 2109–2127. [Google Scholar] [CrossRef]
- Hotchkiss, R.S.; Moldawer, L.L. Parallels between Cancer and Infectious Disease. N. Engl. J. Med. 2014, 371, 380–383. [Google Scholar] [CrossRef]
- Ye, M.; Song, Y.; Pan, S.; Chu, M.; Wang, Z.-W.; Zhu, X. Evolving roles of lysyl oxidase family in tumorigenesis and cancer therapy. Pharmacol. Ther. 2020, 215, 107633. [Google Scholar] [CrossRef] [PubMed]
- Bouhaddou, M.; Memon, D.; Meyer, B.; White, K.M.; Rezelj, V.V.; Correa Marrero, M.; Polacco, B.J.; Melnyk, J.E.; Ulferts, S.; Kaake, R.M.; et al. The Global Phosphorylation Landscape of SARS-CoV-2 Infection. Cell 2020, 182, 685–712.e19. [Google Scholar] [PubMed]
- Dai, M.; Liu, D.; Liu, M.; Zhou, F.; Li, G.; Chen, Z.; Zhang, Z.; You, H.; Wu, M.; Zheng, Q.; et al. Patients with Cancer Appear More Vulnerable to SARS-CoV-2: A Multicenter Study during the COVID-19 Outbreak. Cancer Discov. 2020, 10, 783–791. [Google Scholar] [CrossRef]
- Zhang, L.; Richards, A.; Barrasa, M.I.; Hughes, S.H.; Young, R.A.; Jaenisch, R. Reverse-transcribed SARS-CoV-2 RNA can integrate into the genome of cultured human cells and can be expressed in patient-derived tissues. Proc. Natl. Acad. Sci. USA 2021, 118, e2105968118. [Google Scholar] [CrossRef] [PubMed]
- Briggs, E.; Ward, W.; Rey, S.; Law, D.; Nelson, K.; Bois, M.; Ostrov, N.; Lee, H.H.; Laurent, J.M.; Mita, P. Assessment of potential SARS-CoV-2 virus integration into human genome reveals no significant impact on RT-qPCR COVID-19 testing. Proc. Natl. Acad. Sci. USA 2021, 118, e2113065118. [Google Scholar] [CrossRef]
- Kazachenka, A.; Kassiotis, G. SARS-CoV-2-Host Chimeric RNA-Sequencing Reads Do Not Necessarily Arise From Virus Integration Into the Host DNA. Front Microbiol. 2021, 12, 676693. [Google Scholar] [CrossRef]
- Parry, R.; Gifford, R.J.; Lytras, S.; Ray, S.C.; Coin, L.J.M. No evidence of SARS-CoV-2 reverse transcription and integration as the origin of chimeric transcripts in patient tissues. Proc. Natl. Acad. Sci. USA 2021, 118, e2109066118. [Google Scholar] [CrossRef]
- Yau, J.W.; Teoh, H.; Verma, S. Endothelial cell control of thrombosis. BMC Cardiovasc. Disord. 2015, 15, 130. [Google Scholar] [CrossRef]
- Islam, A.K.M.M. Cardiac myxomas: A narrative review. World J. Cardiol. 2022, 14, 206–219. [Google Scholar] [CrossRef]
- Makarov, I.A.; Mitrofanova, L.B.; Antonova, I.B.; Danilova, I.A.; Khazratov, A.O.; Sidorin, V.S. Myxofibrosarcoma of the heart: Case series. J. Arrhythmology 2022, 29, 50–57. [Google Scholar] [CrossRef]
- Zhang, G.; Chen, X.; Guo, L.; Feng, Q.; Ni, Y. Primary Cardiac Chondrosarcoma. J. Card. Surg. 2012, 27, 186–188. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.J.; Wi, J.H.; Kim, Y.; Lee, S.; Joo, H.C.; Youn, Y.N. Chondrosarcoma of the Heart. Korean J. Thorac. Cardiovasc. Surg. 2015, 48, 199–201. [Google Scholar] [CrossRef]
- Parmar, C.; Jojo, A.; Vachhani, K.C.; Vijayan, S.N. Primary chondrosarcoma of the heart. Eur. J. Cardiothorac. Surg. 2008, 33, 513–515. [Google Scholar] [CrossRef] [PubMed]
- Passi, R.; Brittan, M.; Baker, A.H. The role of the endothelium in severe acute respiratory syndrome coronavirus 2 infection and pathogenesis. Curr. Opin. Physiol. 2023, 34, 100670. [Google Scholar] [CrossRef] [PubMed]
- Nappi, F.; Avtaar Singh, S.S. Endothelial Dysfunction in SARS-CoV-2 Infection. Biomedicines 2022, 10, 654. [Google Scholar] [CrossRef]
- Nalbandian, A.; Sehgal, K.; Gupta, A.; Madhavan, M.V.; McGroder, C.; Stevens, J.S.; Cook, J.R.; Nordvig, A.S.; Shalev, D.; Sehrawat, T.S.; et al. Post-acute COVID-19 syndrome. Nat. Med. 2021, 27, 601–615. [Google Scholar] [CrossRef] [PubMed]
- de Rooij, L.P.M.H.; Becker, L.M.; Carmeliet, P. A Role for the Vascular Endothelium in Post-Acute COVID-19? Circulation 2022, 145, 1503–1505. [Google Scholar] [CrossRef]
- Bearse, M.; Hung, Y.P.; Krauson, A.J.; Bonanno, L.; Boyraz, B.; Harris, C.K.; Helland, T.L.; Hilburn, C.F.; Hutchison, B.; Jobbagy, S.; et al. Factors associated with myocardial SARS-CoV-2 infection, myocarditis, and cardiac inflammation in patients with COVID-19. Mod. Pathol. 2021, 34, 1345–1357. [Google Scholar] [CrossRef]
- Mitrofanova, L.; Makarov, I.; Gorshkov, A.; Vorobeva, O.; Simonenko, M.; Starshinova, A.; Kudlay, D.; Karonova, T. New Scenarios in Heart Transplantation and Persistency of SARS-CoV-2 (Case Report). Life 2023, 13, 1551. [Google Scholar] [CrossRef]
- Patterson, B.K.; Francisco, E.B.; Yogendra, R.; Long, E.; Pise, A.; Rodrigues, H.; Hall, E.; Herrera, M.; Parikh, P.; Guevara-Coto, J.; et al. Persistence of SARS CoV-2 S1 Protein in CD16+ Monocytes in Post-Acute Sequelae of COVID-19 (PASC) up to 15 Months Post-Infection. Front. Immunol. 2022, 12, 746021. [Google Scholar] [CrossRef]
- Schultheiß, C.; Willscher, E.; Paschold, L.; Gottschick, C.; Klee, B.; Bosurgi, L.; Dutzmann, J.; Sedding, D.; Frese, T.; Girndt, M.; et al. Liquid biomarkers of macrophage dysregulation and circulating spike protein illustrate the biological heterogeneity in patients with post-acute sequelae of COVID-19. J. Med. Virol. 2023, 95, e28364. [Google Scholar] [CrossRef]
- Jahankhani, K.; Ahangari, F.; Adcock, I.M.; Mortaz, E. Possible cancer-causing capacity of COVID-19: Is SARS-CoV-2 an oncogenic agent? Biochimie 2023, 213, 130–138. [Google Scholar] [CrossRef]
- Randall, R.E.; Griffin, D.E. Within host RNA virus persistence: Mechanisms and consequences. Curr. Opin. Virol. 2017, 23, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Tempera, I.; Lieberman, P.M. Oncogenic Viruses as Entropic Drivers of Cancer Evolution. Front Virol. 2021, 1, 753366. [Google Scholar] [CrossRef]
- Gaspar-Rodríguez, A.; Padilla-González, A.; Rivera-Toledo, E. Coronavirus persistence in human respiratory tract and cell culture: An overview. Braz. J. Infect. Dis. 2021, 25, 101632. [Google Scholar] [CrossRef]
- Li, F.; Fu, L.; Liu, X.; Liu, X.-A.; Liang, Y.; Lv, Y.; Yang, Z.; Guo, A.; Chen, Z.; Li, W.; et al. Serum metabolomic abnormalities in survivors of non-severe COVID-19. Heliyon 2022, 8, e10473. [Google Scholar] [CrossRef]
- Rudiansyah, M.; Jasim, S.A.; Mohammad Pour, Z.G.; Athar, S.S.; Jeda, A.S.; Doewes, R.I.; Jalil, A.T.; Bokov, D.O.; Mustafa, Y.F.; Noroozbeygi, M.; et al. Coronavirus disease 2019 (COVID-19) update: From metabolic reprogramming to immunometabolism. J. Med. Virol. 2022, 94, 4611–4627. [Google Scholar] [CrossRef] [PubMed]
- Shen, T.; Wang, T. Metabolic Reprogramming in COVID-19. Int. J. Mol. Sci. 2021, 22, 11475. [Google Scholar] [CrossRef]
- Li, Y.S.; Ren, H.C.; Cao, J.H. Correlation of SARS-CoV-2 to cancer: Carcinogenic or anticancer? (Review). Int. J. Oncol. 2022, 60, 42. [Google Scholar] [CrossRef] [PubMed]
- Goubran, H.; Stakiw, J.; Seghatchian, J.; Ragab, G.; Burnouf, T. SARS-CoV-2 and cancer: The intriguing and informative cross-talk. Transfus. Apher. Sci. 2022, 61, 103488. [Google Scholar] [CrossRef] [PubMed]
- De Winter, F.H.R.; Hotterbeekx, A.; Huizing, M.T.; Konnova, A.; Fransen, E.; Jongers, B.; Jairam, R.K.; Van Averbeke, V.; Moons, P.; Roelant, E.; et al. Blood Cytokine Analysis Suggests That SARS-CoV-2 Infection Results in a Sustained Tumour Promoting Environment in Cancer Patients. Cancers 2021, 13, 5718. [Google Scholar] [CrossRef] [PubMed]
- Percivalle, E.; Sammartino, J.C.; Cassaniti, I.; Arbustini, E.; Urtis, M.; Smirnova, A.; Concardi, M.; Belgiovine, C.; Ferrari, A.; Lilleri, D.; et al. Macrophages and Monocytes: “Trojan Horses” in COVID-19. Viruses 2021, 13, 2178. [Google Scholar] [CrossRef] [PubMed]
- Sutanto, H.; Soegiarto, G. Risk of Thrombosis during and after a SARS-CoV-2 Infection: Pathogenesis, Diagnostic Approach, and Management. Hematol. Rep. 2023, 15, 225–243. [Google Scholar] [CrossRef] [PubMed]
- Alrifae, G.M.H.; Almuquddami, A.A.S.; Etaleb, K.M.; Abdelhamid, M.H.M. Post-Acute COVID-19 syndrome (PACS) right atrioventricular and vena cava thrombus on top of a myxoma. A Case report. J. Cardiothorac. Surg. 2022, 17, 261. [Google Scholar] [CrossRef] [PubMed]
- Moss, D.E.; Kumar, D.; Mehta, A.; Patel, P.P. Atrial Myxoma Presenting as an Atypical Stroke in a Young Patient with a Recent COVID-19 Infection. Cureus 2022, 14, e26407. [Google Scholar] [CrossRef]
- Korompoki, E.; Gavriatopoulou, M.; Fotiou, D.; Ntanasis-Stathopoulos, I.; Dimopoulos, M.A.; Terpos, E. Late-onset hematological complications post COVID-19: An emerging medical problem for the hematologist. Am. J. Hematol. 2022, 97, 119–128. [Google Scholar] [CrossRef]
- Kell, D.B.; Laubscher, G.J.; Pretorius, E. A central role for amyloid fibrin microclots in long COVID/PASC: Origins and therapeutic implications. Biochem. J. 2022, 479, 537–559. [Google Scholar] [CrossRef]
- Zoroufian, A.; Mohseni-Badalabadi, R.; Mahalleh, M.; Ghorashi, S.M.; Momtahen, S.; Omidi, N. A potential misdiagnosis in the COVID-19 pandemic era: A case report of superimposed thrombosis or tumor recurrence. J. Cardiothorac. Surg. 2021, 16, 316. [Google Scholar] [CrossRef]
- Rahimmanesh, I.; Shariati, L.; Dana, N.; Esmaeili, Y.; Vaseghi, G.; Haghjooy Javanmard, S. Cancer Occurrence as the Upcoming Complications of COVID-19. Front. Mol. Biosci. 2022, 8, 813175. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
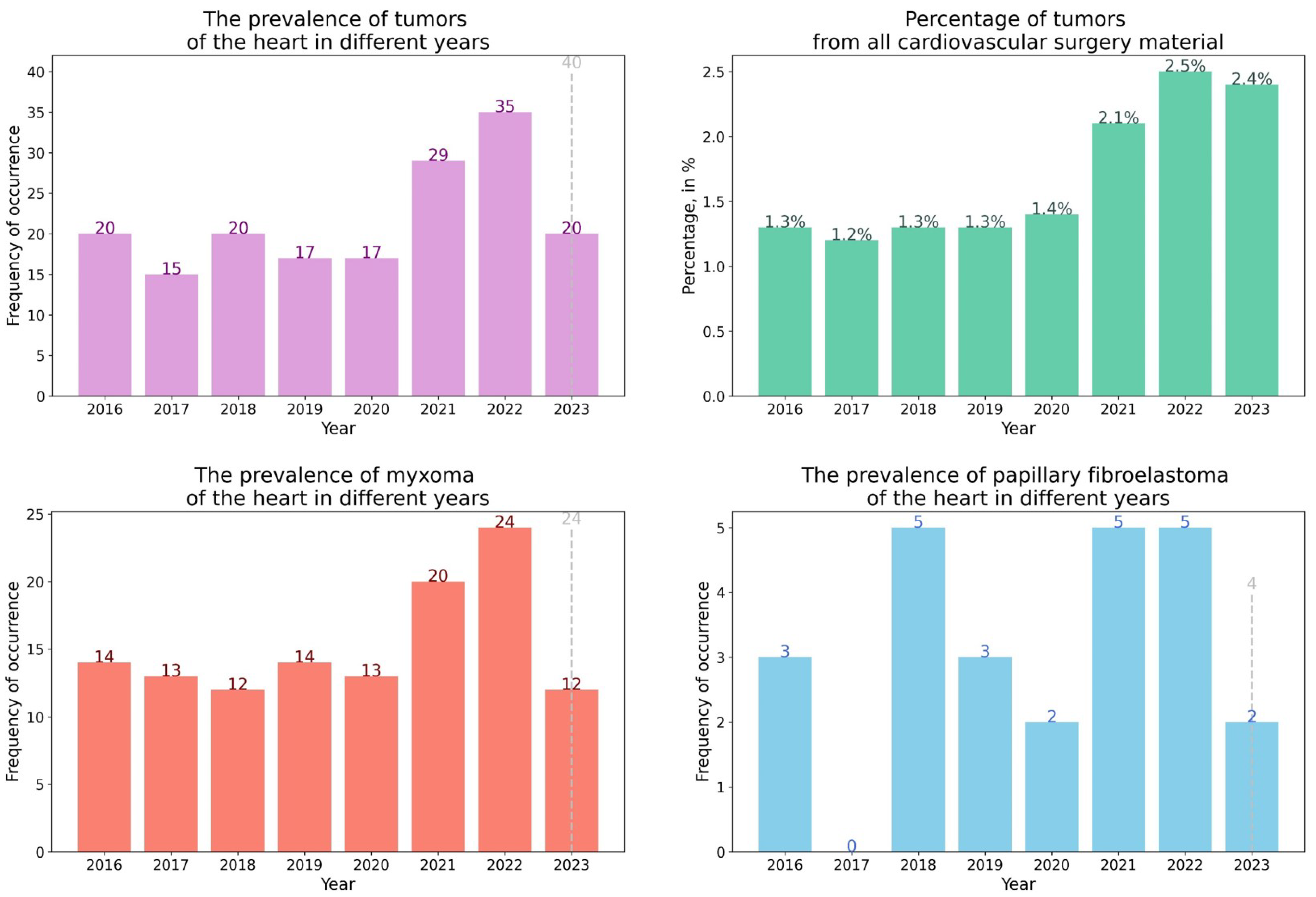
| Year of the Study | The Total Number of Surgical Material Morphological Examinations (n) | Number of Heart Tumors Detections (n/%) | Characteristics of Heart Tumors |
|---|---|---|---|
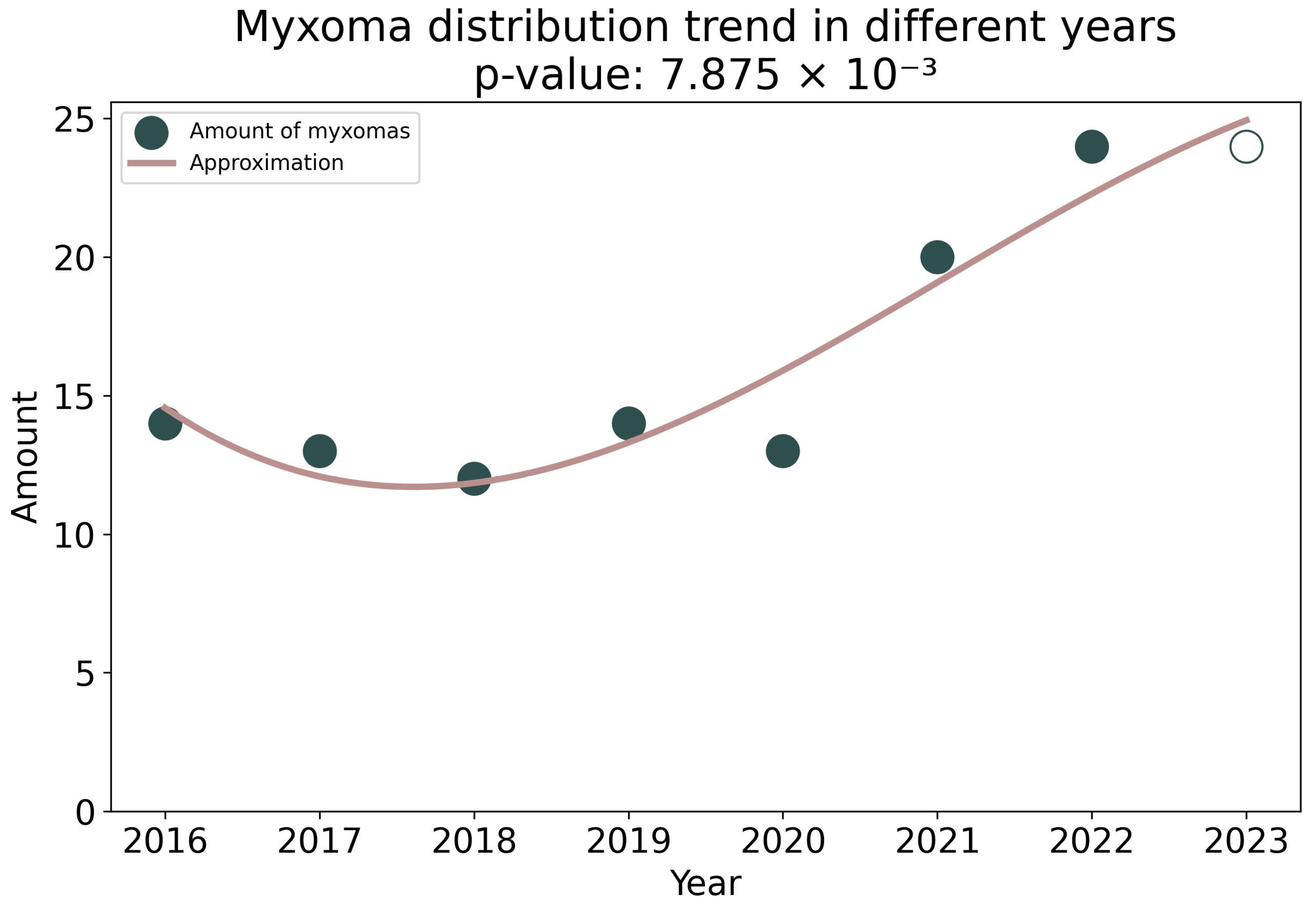
| 2016 | 8333 | 17 (0.20) | 14 cardiac myxomas and 3 papillary fibroelastomas |
| 2017 | 8235 | 14 (0.17) | 13 cardiac myxomas and 1 lipoma |
| 2018 | 10,526 | 20 (0.19) | 12 cardiac myxomas, 5 papillary fibroelastomas, 1 sclerosing epithelioid fibrosarcoma of the right atrium, 1 epithelioid cell malignant mesothelioma, 1 melanoma metastasis. |
| 2019 | 10,011 | 17 (0.17) | 14 cardiac myxomas and 3 papillary fibroelastomas |
| 2020 | 9411 | 16 (0.17) | 13 cardiac myxomas, 2 papillary fibroelastomas, 1 leiomyoma |
| 2021 | 12,707 | 28 (0.22) | 20 cardiac myxomas, 5 papillary fibroelastomas, 1 cavernous hemangioma, 1 fibrolipoma, 1 fibroepithelial polyp |
| 2022 | 12,918 | 31 (0.24) | 24 cardiac myxomas, 5 papillary fibroelastomas, 1 cavernous hemangioma, 1 lipoma |
| Year | 2016 | 2017 | 2018 | 2019 | 2020 | 2021 | 2022 | 2023 |
|---|---|---|---|---|---|---|---|---|
| Tumors | Angiosarcoma—2 Infiltrating lipoma | Myxofibrosarcoma | None | None | Lipoma | Myxofibrosarcoma | Myxofibrosarcoma B-large cell primary lymphoma Lipoma Rhabdomyoma | Myxofibrosarcoma B-large cell secondary lymphoma |
| Total: | 3 | 1 | 0 | 0 | 1 | 1 | 4 | 2 |
| № | Year | Diagnosis | Percentage of Tumor Cells Expressing SARS-CoV-2 Spike Protein | Percentage of Cells in a Tumor Expressing CD68 |
|---|---|---|---|---|
| 1 | 2022 | Papillary fibroelastoma | 95 | 30 |
| 2 | 2022 | Papillary fibroelastoma | 98 | 48 |
| 3 | 2023 | Papillary fibroelastoma | 98 | 7 |
| 4 | 2022 | Cardic Myxoma | 98 | 48 |
| 5 | 2022 | Cardic Myxoma | 0 | 75 |
| 6 | 2022 | Cardic Myxoma | 93 | 38 |
| 7 | 2023 | Cardic Myxoma | 42 | 49 |
| 8 | 2023 | Proliferating myxoma | 72 | 77 |
| 9 | 2023 | Chondrosarcoma | 87 | 61 |
| 10 | 2022 | Myxofibrosarcoma | 87 | 32 |
| 11 | 2022 | Myxofibrosarcoma by EMB | 7 | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mitrofanova, L.; Makarov, I.; Goncharova, E.; Makarova, T.; Starshinova, A.; Kudlay, D.; Shlaykhto, E. High Risk of Heart Tumors after COVID-19. Life 2023, 13, 2087. https://doi.org/10.3390/life13102087
Mitrofanova L, Makarov I, Goncharova E, Makarova T, Starshinova A, Kudlay D, Shlaykhto E. High Risk of Heart Tumors after COVID-19. Life. 2023; 13(10):2087. https://doi.org/10.3390/life13102087
Chicago/Turabian StyleMitrofanova, Lubov, Igor Makarov, Ekaterina Goncharova, Taiana Makarova, Anna Starshinova, Dmitry Kudlay, and Evgeny Shlaykhto. 2023. "High Risk of Heart Tumors after COVID-19" Life 13, no. 10: 2087. https://doi.org/10.3390/life13102087
APA StyleMitrofanova, L., Makarov, I., Goncharova, E., Makarova, T., Starshinova, A., Kudlay, D., & Shlaykhto, E. (2023). High Risk of Heart Tumors after COVID-19. Life, 13(10), 2087. https://doi.org/10.3390/life13102087