

Focused Ultrasound, an Emerging Tool for Atherosclerosis Treatment: A Comprehensive Review

 , , ,
, , ,
Abstract
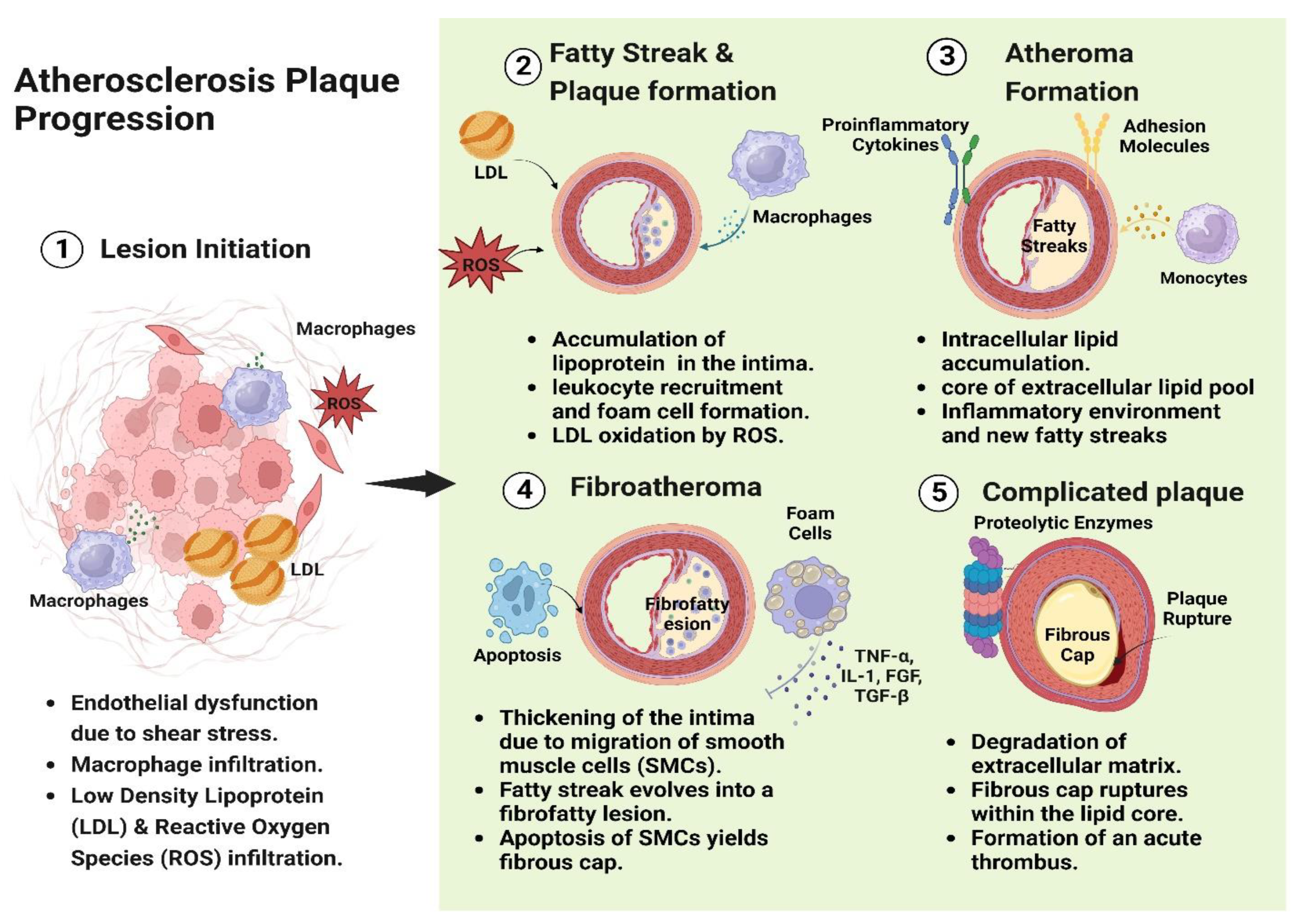
1. Introduction
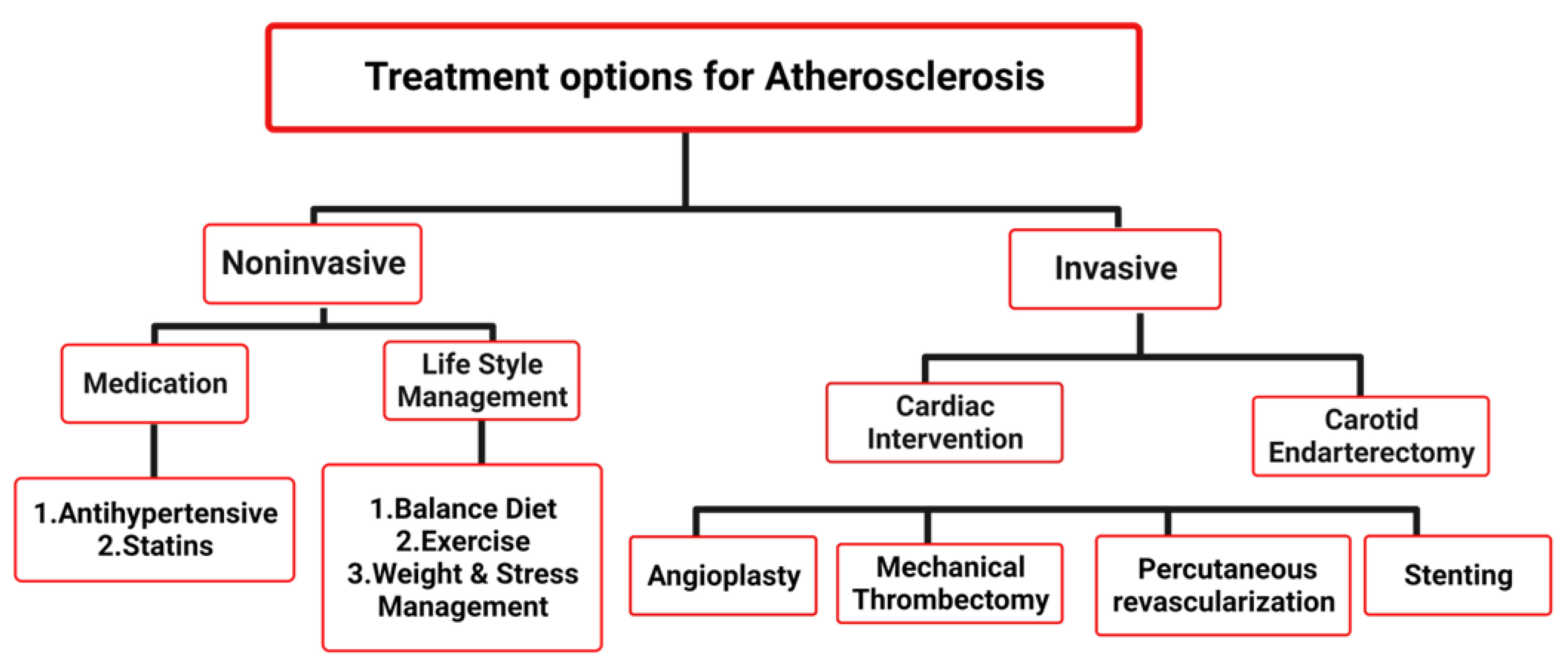
2. Current Treatment Options for Atherosclerosis
3. Comparison of Invasive and Noninvasive Treatment Options for Atherosclerosis
4. Focused Ultrasound as an Emerging Tool for Atherosclerosis Treatment
5. Overview of FUS Parameters for Achieving Sono Thrombolysis in Atherosclerosis Treatment
- a.
- Intensity:
- b.
- Frequency:
- c.
- Duration of exposure:
- d.
- Spatial targeting:
6. Mechanisms of Focused Ultrasound Thrombolysis and Clinical Outcomes
7. Comparison of FUS with Traditional Treatment Methods
8. Merits of FUS in Atherosclerosis Treatment
9. Limitations and Future Perspectives
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhang, Y.; Dong, H.; Xu, Y.; Shi, R.; Gu, J.; Lang, H.; Gao, J.; Zhang, W.W. External ultrasound for carotid atherosclerotic plaque treatment. J. Ultrasound Med. 2015, 34, 451–459. [Google Scholar] [CrossRef] [PubMed]
- Conte, M.S.; Pomposelli, F.B.; Clair, D.G.; Geraghty, P.J.; McKinsey, J.F.; Mills, J.L.; Moneta, G.L.; Murad, M.H.; Powell, R.J.; Reed, A.B. Society for Vascular Surgery practice guidelines for atherosclerotic occlusive disease of the lower extremities: Management of asymptomatic disease and claudication. J. Vasc. Surg. 2015, 61, 2S–41S.e41. [Google Scholar] [CrossRef] [PubMed]
- Criqui, M.H.; Aboyans, V. Epidemiology of peripheral artery disease. Circ. Res. 2015, 116, 1509–1526. [Google Scholar] [CrossRef]
- Secemsky, E.A.; Schermerhorn, M.; Carroll, B.J.; Kennedy, K.F.; Shen, C.; Valsdottir, L.R.; Landon, B.; Yeh, R.W. Readmissions after revascularization procedures for peripheral arterial disease: A nationwide cohort study. Ann. Intern. Med. 2018, 168, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.-A.; Farooqi, H.M.U.; Paeng, D.-G. Axial shear rate: A hemorheological factor for erythrocyte aggregation under Womersley flow in an elastic vessel based on numerical simulation. Comput. Biol. Med. 2023, 157, 106767. [Google Scholar] [CrossRef]
- Lee, C.-A.; Kong, Q.; Paeng, D.-G. Depletion-model-based numerical simulation of the kinetics of red blood cell aggregation under sinusoidal pulsatile flow. Biorheology 2018, 55, 1–14. [Google Scholar] [CrossRef]
- Lee, C.-A.; Paeng, D.-G. Numerical simulation of spatiotemporal red blood cell aggregation under sinusoidal pulsatile flow. Sci. Rep. 2021, 11, 9977. [Google Scholar] [CrossRef]
- Rosenschein, U.; Bernstein, J.J.; DiSegni, E.; Kaplinsky, E.; Bernheim, J.; Rozenzsajn, L.A. Experimental ultrasonic angioplasty: Disruption of atherosclerotic plaques and thrombi in vitro and arterial recanalization in vivo. J. Am. Coll. Cardiol. 1990, 15, 711–717. [Google Scholar] [CrossRef]
- Fowkes, F.G.R.; Rudan, D.; Rudan, I.; Aboyans, V.; Denenberg, J.O.; McDermott, M.M.; Norman, P.E.; Sampson, U.K.; Williams, L.J.; Mensah, G.A. Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010: A systematic review and analysis. Lancet 2013, 382, 1329–1340. [Google Scholar] [CrossRef]
- Hirsch, A.T.; Hartman, L.; Town, R.J.; Virnig, B.A. National health care costs of peripheral arterial disease in the Medicare population. Vasc. Med. 2008, 13, 209–215. [Google Scholar] [CrossRef]
- Achim, A.; Kákonyi, K.; Nagy, F.; Jambrik, Z.; Varga, A.; Nemes, A.; Chan, J.S.K.; Toth, G.G.; Ruzsa, Z. Radial Artery Calcification in Predicting Coronary Calcification and Atherosclerosis Burden. Cardiol. Res. Pract. 2022, 2022, 5108389. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.-A.; Paeng, D.-G. Numerical study of local parabolic rouleaux formation analyzed by axial and radial shear rates. In Biorheology; IOS Press: Amsterdam, The Netherlands, 2021; Volume 58, p. 124. [Google Scholar]
- Kim, Y.-S.; Rhim, H.; Choi, M.J.; Lim, H.K.; Choi, D. High-intensity focused ultrasound therapy: An overview for radiologists. Korean J. Radiol. 2008, 9, 291–302. [Google Scholar] [CrossRef] [PubMed]
- Yao, J.; Zhao, X.; Tan, F.; Cao, X.; Guo, S.; Li, X.; Huang, Z.; Diabakte, K.; Wang, L.; Liu, M. Early modulation of macrophage ROS-PPARγ-NF-κB signalling by sonodynamic therapy attenuates neointimal hyperplasia in rabbits. Sci. Rep. 2020, 10, 11638. [Google Scholar] [CrossRef] [PubMed]
- Williams, A.; Chater, B.; Allen, K.; Sherwood, M.; Sanderson, J. Release of β-Thromboglobulin from Human Platelets by Therapeutic Intensities of Ultrasound. Br. J. Haematol. 1978, 40, 133–142. [Google Scholar] [CrossRef]
- Wu, J. Shear stress in cells generated by ultrasound. Prog. Biophys. Mol. Biol. 2007, 93, 363–373. [Google Scholar] [CrossRef]
- Adams, G.; Shammas, N.; Mangalmurti, S.; Bernardo, N.L.; Miller, W.E.; Soukas, P.A.; Parikh, S.A.; Armstrong, E.J.; Tepe, G.; Lansky, A. Intravascular lithotripsy for treatment of calcified lower extremity arterial stenosis: Initial analysis of the disrupt PAD III study. J. Endovasc. Ther. 2020, 27, 473–480. [Google Scholar] [CrossRef]
- Chater, B.; Williams, A. Platelet aggregation induced in vitro by therapeutic ultrasound. Thromb. Haemost. 1977, 38, 640–651. [Google Scholar] [CrossRef]
- Achim, A.; Lackó, D.; Hüttl, A.; Csobay-Novák, C.; Csavajda, Á.; Sótonyi, P.; Merkely, B.; Nemes, B.; Ruzsa, Z. Impact of Diabetes Mellitus on Early Clinical Outcome and Stent Restenosis after Carotid Artery Stenting. J. Diabetes Res. 2022, 2022, 4196195. [Google Scholar] [CrossRef]
- Zorob, T.; Farooqi, M.A.; Ahsan, A.; Zaki, A.; Rathore, M.A.; Farooqi, H.M.U. Prevalence and Trends in Hepatitis B & C Virus among Blood Donors in Pakistan: A Regional Transfusion Center Study. Livers 2023, 3, 271–281. [Google Scholar]
- Amjad, R.; Lee, C.-A.; Farooqi, H.M.U.; Khan, H.; Paeng, D.-G. Choroidal thickness in different patterns of diabetic macular edema. J. Clin. Med. 2022, 11, 6169. [Google Scholar] [CrossRef]
- Farooqi, H.M.U.; Kim, K.-H.; Kausar, F.; Muhammad, J.; Bukhari, H.; Choi, K.-H. Frequency and molecular characterization of Staphylococcus aureus from placenta of mothers with term and preterm deliveries. Life 2022, 12, 257. [Google Scholar] [CrossRef] [PubMed]
- Elhelf, I.S.; Albahar, H.; Shah, U.; Oto, A.; Cressman, E.; Almekkawy, M. High intensity focused ultrasound: The fundamentals, clinical applications and research trends. Diagn. Interv. Imaging 2018, 99, 349–359. [Google Scholar] [CrossRef] [PubMed]
- Gandini, R.; Del Giudice, C. Local ultrasound to enhance paclitaxel delivery after femoral-popliteal treatment in critical limb ischemia: The PACUS Trial. Cardiovasc. Interv. 2016, 9, 2147–2153. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.J.; Gaines, P.; Crew, J.R.; CumberlandM, D.C. Clinical trial of percutaneous peripheral ultrasound angiopalsty. J. Am. Coll. Cardiol. 1993, 22, 480–488. [Google Scholar] [CrossRef]
- Alexandrov, A.V.; Grotta, J.C. Arterial reocclusion in stroke patients treated with intravenous tissue plasminogen activator. Neurology 2002, 59, 862–867. [Google Scholar] [CrossRef]
- Rubiera, M.; Ribo, M.; Delgado-Mederos, R.; Santamarina, E.; Maisterra, O.; Delgado, P.; Montaner, J.; Alvarez-Sabín, J.; Molina, C.A. Do bubble characteristics affect recanalization in stroke patients treated with microbubble-enhanced sonothrombolysis? Ultrasound Med. Biol. 2008, 34, 1573–1577. [Google Scholar] [CrossRef]
- Damianou, C.; Hadjisavvas, V.; Mylonas, N.; Couppis, A.; Ioannides, K. MRI-guided sonothrombolysis of rabbit carotid artery. J. Stroke Cerebrovasc. Dis. 2014, 23, e113–e121. [Google Scholar] [CrossRef]
- Steffen, W.; Cumberland, D.; Gaines, P.; Luo, H.; Nita, H.; Maurer, G.; Fishbein, M.; Siegel, R. Chrome congestive heart failure: Catheter-delivered high intensity, low frequency ultrasound induces vasodilation in vivo. Eur. Heart J. 1994, 15, 369–376. [Google Scholar] [CrossRef]
- Steffen, W.; Fishbein, M.C.; Luo, H.; Lee, D.-Y.; Nitams, H.; Cumberland, D.C.; Tabak, S.W.; Carbonne, M.; Maurer, G.; Siegel, R.J. High intensity, low frequency catheter-delivered ultrasound dissolution of occlusive coronary artery thrombi: An in vitro and in vivo study. J. Am. Coll. Cardiol. 1994, 24, 1571–1579. [Google Scholar] [CrossRef]
- Wang, Y.; Wang, W.; Xu, H.; Sun, Y.; Sun, J.; Jiang, Y.; Yao, J.; Tian, Y. Non-lethal sonodynamic therapy inhibits atherosclerotic plaque progression in ApoE−/−mice and attenuates ox-LDL-mediated macrophage impairment by inducing heme oxygenase-1. Cell. Physiol. Biochem. 2017, 41, 2432–2446. [Google Scholar] [CrossRef]
- Zahid, A.S.; Farooqi, H.M.U.; Ahsan, A.; Farooqi, M.A.; Kausar, F.; Muhammad, J.; Ahmad, A. Comparative analysis of antigenic strength and in vivo serum antibodies concentration of tetanus toxoid vaccine adsorbed in Pakistan. Saudi J. Biol. Sci. 2022, 29, 103337. [Google Scholar] [CrossRef] [PubMed]
- Farooqi, M.A.; Ahsan, A.; Yousuf, S.; Shakoor, N.; Farooqi, H.M.U. Seroprevalence of Hepatitis E Virus Antibodies (IgG) in the Community of Rawalpindi. Livers 2022, 2, 108–115. [Google Scholar] [CrossRef]
- Vaezy, S.; Martin, R.; Kaczkowski, P.; Keilman, G.; Goldman, B.; Yaziji, H.; Carter, S.; Caps, M.; Crum, L. Use of high-intensity focused ultrasound to control bleeding. J. Vasc. Surg. 1999, 29, 533–542. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Shehata, I.A.; Ballard, J.R.; Casper, A.J.; Liu, D.; Mitchell, T.; Ebbini, E.S. Feasibility of targeting atherosclerotic plaques by high-intensity–focused ultrasound: An in vivo study. J. Vasc. Interv. Radiol. 2013, 24, 1880–1887.e1882. [Google Scholar] [CrossRef] [PubMed]
- Shehata, I.A. Treatment with high intensity focused ultrasound: Secrets revealed. Eur. J. Radiol. 2012, 81, 534–541. [Google Scholar] [CrossRef]
- Sun, X.; Guo, S.; Yao, J.; Wang, H.; Peng, C.; Li, B.; Wang, Y.; Jiang, Y.; Wang, T.; Yang, Y. Rapid inhibition of atherosclerotic plaque progression by sonodynamic therapy. Cardiovasc. Res. 2019, 115, 190–203. [Google Scholar] [CrossRef]
- Mason, O.R.; Davidson, B.P.; Sheeran, P.; Muller, M.; Hodovan, J.M.; Sutton, J.; Powers, J.; Lindner, J.R. Augmentation of Tissue Perfusion in Patients With Peripheral Artery Disease Using Microbubble Cavitation. JACC Cardiovasc. Imaging 2019, 13, 641–651. [Google Scholar] [CrossRef]
- Cintas, P.; Le Traon, A.P.; Larrue, V. High rate of recanalization of middle cerebral artery occlusion during 2-MHz transcranial color-coded Doppler continuous monitoring without thrombolytic drug. Stroke 2002, 33, 626–628. [Google Scholar] [CrossRef][Green Version]
- Chen, J.; Yang, Y.; Li, Y.; Xu, L.; Zhao, C.; Chen, Q.; Lu, Y. Targeted microbubbles combined with low-power focused ultrasound promote the thrombolysis of acute deep vein thrombosis. Front. Bioeng. Biotechnol. 2023, 11, 1163405. [Google Scholar] [CrossRef]
- Blana, A.; Walter, B.; Rogenhofer, S.; Wieland, W.F. High-intensity focused ultrasound for the treatment of localized prostate cancer: 5-year experience. Urology 2004, 63, 297–300. [Google Scholar] [CrossRef]
- Brodmann, M.; Werner, M.; Brinton, T.J.; Illindala, U.; Lansky, A.; Jaff, M.R.; Holden, A. Safety and performance of lithoplasty for treatment of calcified peripheral artery lesions. J. Am. Coll. Cardiol. 2017, 70, 908–910. [Google Scholar] [CrossRef] [PubMed]
- Casper, A.J.; Liu, D.; Ballard, J.R.; Ebbini, E.S. Real-time implementation of a dual-mode ultrasound array system: In vivo results. IEEE Trans. Biomed. Eng. 2013, 60, 2751–2759. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Brayman, A.A.; Kreider, W.; Bailey, M.R.; Matula, T.J. Observations of translation and jetting of ultrasound-activated microbubbles in mesenteric microvessels. Ultrasound Med. Biol. 2011, 37, 2139–2148. [Google Scholar] [CrossRef]
- Chaar, C.I.O.; Gholitabar, N.; Goodney, P.; Dardik, A.; Abougergi, M.S. One-Year readmission after open and endovascular revascularization for critical limb ischemia. Ann. Vasc. Surg. 2019, 61, 25–32.e2. [Google Scholar] [CrossRef]
- Birnbaum, Y. Augmentation of Ultrasound-Induced Clot Disruption by Nongas-Filled Microparticles. Echocardiography 2001, 18, 265–268. [Google Scholar] [CrossRef] [PubMed]
- Zderic, V.; Brayman, A.A.; Sharar, S.R.; Crum, L.A.; Vaezy, S. Microbubble-enhanced hemorrhage control using high intensity focused ultrasound. Ultrasonics 2006, 45, 113–120. [Google Scholar] [CrossRef]
- Zhang, B.; Wu, H.; Kim, H.; Welch, P.J.; Cornett, A.; Stocker, G.; Nogueira, R.G.; Kim, J.; Owens, G.; Dayton, P.A. A Model of High-Speed Endovascular Sonothrombolysis with Vortex Ultrasound-Induced Shear Stress to Treat Cerebral Venous Sinus Thrombosis. Research 2023, 6, 0048. [Google Scholar] [CrossRef]
- Arora, D.; Cooley, D.; Perry, T.; Skliar, M.; Roemer, R.B. Direct thermal dose control of constrained focused ultrasound treatments: Phantom and in vivo evaluation. Phys. Med. Biol. 2005, 50, 1919. [Google Scholar] [CrossRef]
- Xiong, L.; Yu, J.; Shao, D.; Zhu, H.; Wu, X. Noninvasive thermometer for HIFU and its scaling. Ultrasonics 2006, 44, e31–e35. [Google Scholar]
- Farooqi, H.M.U.; Khalid, M.A.U.; Kim, K.H.; Lee, S.R.; Choi, K.H. Real-time physiological sensor-based liver-on-chip device for monitoring drug toxicity. J. Micromech. Microeng. 2020, 30, 115013. [Google Scholar] [CrossRef]
- Farooqi, H.M.U.; Kang, B.; Khalid, M.A.U.; Salih, A.R.C.; Hyun, K.; Park, S.H.; Huh, D.; Choi, K.H. Real-time monitoring of liver fibrosis through embedded sensors in a microphysiological system. Nano Converg. 2021, 8, 3. [Google Scholar] [CrossRef] [PubMed]
- Piazza, G.; Hohlfelder, B.; Jaff, M.R.; Ouriel, K.; Engelhardt, T.C.; Sterling, K.M.; Jones, N.J.; Gurley, J.C.; Bhatheja, R.; Kennedy, R.J. A prospective, single-arm, multicenter trial of ultrasound-facilitated, catheter-directed, low-dose fibrinolysis for acute massive and submassive pulmonary embolism: The SEATTLE II study. Cardiovasc. Interv. 2015, 8, 1382–1392. [Google Scholar] [CrossRef] [PubMed]
- Alonso, A.; Della Martina, A.; Stroick, M.; Fatar, M.; Griebe, M.; Pochon, S.; Schneider, M.; Hennerici, M.; Allémann, E.; Meairs, S. Molecular imaging of human thrombus with novel abciximab immunobubbles and ultrasound. Stroke 2007, 38, 1508–1514. [Google Scholar] [CrossRef] [PubMed]
- Barlinn, K.; Tsivgoulis, G.; Barreto, A.D.; Alleman, J.; Molina, C.A.; Mikulik, R.; Saqqur, M.; Demchuk, A.M.; Schellinger, P.D.; Howard, G. Outcomes following sonothrombolysis in severe acute ischemic stroke: Subgroup analysis of the CLOTBUST trial. Int. J. Stroke 2014, 9, 1006–1010. [Google Scholar] [CrossRef]
- Chen, H.; Kreider, W.; Brayman, A.A.; Bailey, M.R.; Matula, T.J. Blood vessel deformations on microsecond time scales by ultrasonic cavitation. Phys. Rev. Lett. 2011, 106, 034301. [Google Scholar] [CrossRef]
- Del Giudice, C.; Gandini, R. CRT-200.04 Ultrasound plasty to improve outcome of percutaneous angioplasty in below-the-knee lesions: 24 months results of the ULYSSE Registry. Cardiovasc. Interv. 2020, 13 (Suppl. S4), S30. [Google Scholar] [CrossRef]
- DeRubertis, B.G.; Pierce, M.; Chaer, R.A.; Rhee, S.J.; Benjeloun, R.; Ryer, E.J.; Kent, C.; Faries, P.L. Lesion severity and treatment complexity are associated with outcome after percutaneous infra-inguinal intervention. J. Vasc. Surg. 2007, 46, 709–716. [Google Scholar] [CrossRef][Green Version]
- Francis, C.W.; Blinc, A.; Lee, S.; Cox, C. Ultrasound accelerates transport of recombinant tissue plasminogen activator into clots. Ultrasound Med. Biol. 1995, 21, 419–424. [Google Scholar] [CrossRef]
- Barreto, A.D.; Alexandrov, A.V.; Shen, L.; Sisson, A.; Bursaw, A.W.; Sahota, P.; Peng, H.; Ardjomand-Hessabi, M.; Pandurengan, R.; Rahbar, M.H. CLOTBUST-Hands Free: Pilot safety study of a novel operator-independent ultrasound device in patients with acute ischemic stroke. Stroke 2013, 44, 3376–3381. [Google Scholar] [CrossRef]
- Duc, N.M.; Keserci, B. Emerging clinical applications of high-intensity focused ultrasound. Diagn. Interv. Radiol. 2019, 25, 398. [Google Scholar] [CrossRef]
- Farber, A.; Eberhardt, R.T. The current state of critical limb ischemia: A systematic review. JAMA Surg. 2016, 151, 1070–1077. [Google Scholar] [CrossRef] [PubMed]
- Fry, W.; Fry, F. Fundamental neurological research and human neurosurgery using intense ultrasound. IRE Trans. Med. Electron. 1960, ME-7, 166–181. [Google Scholar] [CrossRef]
- Hölscher, T.; Fisher, D.J.; Ahadi, G.; Voie, A. Introduction of a rabbit carotid artery model for sonothrombolysis research. Transl. Stroke Res. 2012, 3, 397–407. [Google Scholar] [CrossRef] [PubMed]
- Hughes, C.B.; Nigmet, Y.; Villanueva, F.S.; Chen, X.; Demetris, A.J.; Stolz, D.B.; Pacella, J.J.; Humar, A. Ultrasound-Targeted Microbubble Cavitation During Machine Perfusion Reduces Microvascular Thrombi and Graft Injury in a Rat Liver Model of Donation After Circulatory Death. In Transplantation Proceedings; Elsevier: Amsterdam, The Netherlands, 2023; Volume 55, pp. 485–495. [Google Scholar]
- Jiang, N.; Wang, Z.; Deng, Q.; Zhou, Y.; Cao, S.; Zhou, Q.; Chen, J.; Guo, R.; Hu, B. Low-intensity focused ultrasound guided dodecafluoropentane-loaded acoustic phase-change nanoparticles for treatment of porcine coronary microthromboembolism. Int. J. Cardiol. 2023, 371, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.I.; Schneider, P.A. New innovations and devices in the management of chronic limb-threatening ischemia. J. Endovasc. Ther. 2020, 27, 524–539. [Google Scholar] [CrossRef] [PubMed]
- Laird, J.R.; Schneider, P.A.; Tepe, G.; Brodmann, M.; Zeller, T.; Metzger, C.; Krishnan, P.; Scheinert, D.; Micari, A.; Cohen, D.J. Durability of treatment effect using a drug-coated balloon for femoropopliteal lesions: 24-month results of IN. PACT SFA. J. Am. Coll. Cardiol. 2015, 66, 2329–2338. [Google Scholar] [CrossRef]
- Wright, C.; Hynynen, K.; Goertz, D. In vitro and in vivo high intensity focused ultrasound thrombolysis. Investig. Radiol. 2012, 47, 217. [Google Scholar] [CrossRef]
- Zderic, V.; Keshavarzi, A.; Noble, M.L.; Paun, M.; Sharar, S.R.; Crum, L.A.; Martin, R.W.; Vaezy, S. Hemorrhage control in arteries using high-intensity focused ultrasound: A survival study. Ultrasonics 2006, 44, 46–53. [Google Scholar] [CrossRef]
- Lei, W.; Hu, J.; Liu, Y.; Liu, W.; Chen, X. Numerical evaluation of high-intensity focused ultrasound-induced thermal lesions in atherosclerotic plaques. Math. Biosci. Eng 2021, 18, 1154–1168. [Google Scholar] [CrossRef]
- Gollmann-Tepeköylü, C.; Lobenwein, D.; Theurl, M.; Primessnig, U.; Lener, D.; Kirchmair, E.; Mathes, W.; Graber, M.; Pölzl, L.; An, A. Shock wave therapy improves cardiac function in a model of chronic ischemic heart failure: Evidence for a mechanism involving VEGF signaling and the extracellular matrix. J. Am. Heart Assoc. 2018, 7, e010025. [Google Scholar] [CrossRef]
- Groen, M.H.A.; Slieker, F.J.B.; Vink, A.; de Borst, G.J.; Simons, M.V.; Ebbini, E.S.; Doevendans, P.A.; Hazenberg, C.E.V.B.; van Es, R. Safety and feasibility of arterial wall targeting with robot-assisted high intensity focused ultrasound: A preclinical study. Int. J. Hyperth. 2020, 37, 903–912. [Google Scholar] [CrossRef] [PubMed]
- Razuvaev, A.; Lund, K.; Roy, J.; Hedin, U.; Caidahl, K. Noninvasive real-time imaging of intima thickness after rat carotid artery balloon injury using ultrasound biomicroscopy. Atherosclerosis 2008, 199, 310–316. [Google Scholar] [CrossRef] [PubMed]
- Dick, F.; Diehm, N.; Galimanis, A.; Husmann, M.; Schmidli, J.; Baumgartner, I. Surgical or endovascular revascularization in patients with critical limb ischemia: Influence of diabetes mellitus on clinical outcome. J. Vasc. Surg. 2007, 45, 751–761. [Google Scholar] [CrossRef] [PubMed]
- Lynn, J.G.; Zwemer, R.L.; Chick, A.J.; Miller, A.E. A new method for the generation and use of focused ultrasound in experimental biology. J. Gen. Physiol. 1942, 26, 179. [Google Scholar] [CrossRef] [PubMed]
- Miller, D.L.; Smith, N.B.; Bailey, M.R.; Czarnota, G.J.; Hynynen, K.; Makin, I.R.S.; Bioeffects Committee of the American Institute of Ultrasound in Medicin. Overview of therapeutic ultrasound applications and safety considerations. J. Ultrasound Med. 2012, 31, 623–634. [Google Scholar] [CrossRef]
- Fereydooni, A.; Gorecka, J.; Dardik, A. Using the epidemiology of critical limb ischemia to estimate the number of patients amenable to endovascular therapy. Vasc. Med. 2020, 25, 78–87. [Google Scholar] [CrossRef]
- Goodney, P.P.; Holman, K.; Henke, P.K.; Travis, L.L.; Dimick, J.B.; Stukel, T.A.; Fisher, E.S.; Birkmeyer, J.D. Regional intensity of vascular care and lower extremity amputation rates. J. Vasc. Surg. 2013, 57, 1471–1480.e3. [Google Scholar] [CrossRef]
- Poliachik, S.L.; Chandler, W.L.; Mourad, P.D.; Bailey, M.R.; Bloch, S.; Cleveland, R.O.; Kaczkowski, P.; Keilman, G.; Porter, T.; Crum, L.A. Effect of high-intensity focused ultrasound on whole blood with and without microbubble contrast agent. Ultrasound Med. Biol. 1999, 25, 991–998. [Google Scholar] [CrossRef]
- Raabe, R.D. Ultrasound-accelerated thrombolysis in arterial and venous peripheral occlusions: Fibrinogen level effects. J. Vasc. Interv. Radiol. 2010, 21, 1165–1172. [Google Scholar] [CrossRef]
- Raza, A.; Harwood, A.; Totty, J.; Smith, G.; Chetter, I. Extracorporeal shockwave therapy for peripheral arterial disease: A review of the potential mechanisms of action. Ann. Vasc. Surg. 2017, 45, 294–298. [Google Scholar] [CrossRef]
- Park, S.; Pham, N.T.; Huynh, H.-T.; Kang, H.W. Development of temperature controller-integrated portable HIFU driver for thermal coagulation. BioMed. Eng. OnLine 2019, 18, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Min, S.; Byeon, Y.; Kim, M.; Lee, Y.; Lee, S.-H.; Lee, Y.; Farooqi, H.M.U.; Lee, H.-K.; Paeng, D.-G. Production enhancement of human adipose-derived mesenchymal stem cells by low-intensity ultrasound stimulation. Sci. Rep. 2022, 12, 22041. [Google Scholar] [CrossRef] [PubMed]
- Kucher, N.; Boekstegers, P.; Müller, O.J.; Kupatt, C.; Beyer-Westendorf, J.; Heitzer, T.; Tebbe, U.; Horstkotte, J.; Müller, R.; Blessing, E. Randomized, controlled trial of ultrasound-assisted catheter-directed thrombolysis for acute intermediate-risk pulmonary embolism. Circulation 2014, 129, 479–486. [Google Scholar] [CrossRef] [PubMed]
- Steffen, M.W.; Undavalli, C.; Asi, N.; Wang, Z.; Elamin, M.B.; Conte, M.S.; Murad, M.H. The natural history of untreated severe or critical limb ischemia. J. Vasc. Surg. 2015, 62, 1642–1651.e3. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Setup | Study Pattern | Principle | Intensity (W/cm2) | Frequency | Clinical Relevance | Results | Reference |
|---|---|---|---|---|---|---|---|
| Ultrasound Angioplasty Ablation System | Invasive | Biomechanical | 115 | 19.5 kHz | 86% of lesions recanalized with ultrasound | Decreased arterial sclerosis | [25] |
| Dedicated ultrasound device | Noninvasive | Biomechanical | Individually calculated | 1 MHz | Atorvastatin and Son dynamic therapy decreased diameter stenosis in PAD. lesions after four weeks | Decreased induration of the arteries | [37] |
| Sonos 5500 | Noninvasive | Biomechanical | NA | 1.3 MHz | Continuous The ultrasound did not affect perfusion in limbs, but ultrasound in PAD patients, it showed. microbubble cavitation increased perfusion | Lower the contradictory effects of ultrasound | [38] |
| CardioProlific Genesis System | Invasive | Biomechanical | NA | 20 kHz | The treatment group has shown improvement. primary patency rates at six and 12 months | Improved efficacy of Sono thrombolysis | [24] |
| 500M Transcranial Doppler System | Noninvasive | Biomechanical | 128 | 2 MHz | Complete recanalization is achieved. in 36% of patients; clinical recovery achieved in 20% of patients | Peripheral arterial vasodilation | [26] |
| ATL Ultramark 9 HDI | Noninvasive | Biomechanical | 415 | 2 MHz | Improved efficacy of Sono thrombolysis | [39] | |
| PMD 100 | Noninvasive | Biomechanical | 750 | 2 MHz | Ultrasound and tPA administration resulted in complete recanalization clinical recovery from acute ischemic stroke | Increased arterial blood flow | [27] |
| TCD 100M | Noninvasive | Biomechanical | 385 | 2 MHz | The type of microbubbles did not affect recanalization rates, clinical improvement, bleeding, in-hospital mortality, or long-term outcome | Decreased Contradictory effects | [1] |
| Dedicated cervical orthotic device. | Noninvasive | Biomechanical | 0.75–1 | 800 kHz | Decreased thickness and area of carotid plaques | Decreased plaques | [1] |
| Model | Study Design | Duration of Exposure | Frequency | Duration of Exposure | Results | Ref. |
|---|---|---|---|---|---|---|
| Rabbit | Custom device with amplifier | 10–40 | 1 MHz | Biomechanical | Decrease in carotid artery atherosclerosis through decreased neointima formation, macrophage | [37] |
| Adult human | Custom apparatus made with piezoelectric transducer | 1 | 1 MHz | Biomechanical | Enhanced Sonothrombolysis via increased uptake of tPA | [15] |
| Adult human | Sonic Concepts | 560–2360 | 1.1 MHz | Biomechanical | Cavitation and hemolysis is greater in samples with contrast agent treated with ultrasound | [34] |
| Adult human | Sonicator model XL 2020 | NA | 20 kHz | Biomechanical | Ultrasound and nongas-filled particles (HAEMACCEL and HAES) decreased clot burden | [46] |
| Rabbit | ExAblate 4000 | 66–200 | 220 kHz | Biomechanical | Mild recanalization in carotid artery stroke thrombosis model, dependent on platelet-activation and cavitation | [64] |
| Rabbit | Custom using function generator | 300 | 1.51 MHz | Biomechanical | Increased sonothrombolysis and partial blood flow restoration in femoral artery | [69] |
| Rabbit | Custom device with amplifier | 10–40 | 1 MHz | Biomechanical | Enhanced sonothrombolysis in rabbit carotid model via increased uptake of tPA | [28] |
| Adult human | Sonacell Multiphone | NA | 0.75, 1.5., 3.0 MHz | Biomechanical | Release of bthromboglobulin in platelets is mediated by ultrasound induced cavitation | [15] |
| Swine | Sonic Concepts | 2500–3100 | 3.5 MHz | Thermal | Control of arterial hemorrhage | [34] |
| Rabbit | Custom made. 111F-U applicator with piezoelectric discs | 3000–6100 | 3.5 MHz | Thermal | Control of arterial hemorrhage | [70] |
| In vitro | Pulsed Doppler US | NA | 5.7 MHz | Biomechanical | tPA and US-induced clot dissolution | [65] |
| DVT rabbit model | Low-Power Focused Ultrasound Device | 2.0 | 0.7 MHz | Thermal | Low-power focused ultrasound reduces inflammation and promotes FUS-mediated plaque dissolution | [40] |
| N/A | Mathematical model | NA | 1.1 MHz | Thermal | To predict the damage of plaque ablation based on wall thickness; | [71] |
| Swine | Imasonic Dual- Mode US Array | 4100–5600 | 3.5 MHz | Thermal | Disruption of atherosclerosis in swine PAD model, accompanied by aggregates of lipid laden macrophages with necrosis. | [35] |
| (PAD) Sprague Dawley rat | Duolith SD1 | 0.1 | 1.054 MHz | Biomechanical | Increase in angiogenesis in hindlimb ischemia model for PAD | [46] |
| C57BL./6J mice (diabetic) | Custom transducer | 0.3 | 1 MHz | Biomechanical | Increased perfusion in hindlimb ischemia model for PAD accompanied by increased angiogenic factors, | [72] |
| Mice (ApoEee) | Custom transducer | 0.3 | 1 MHz | Biomechanical | Inhibition of atherosclerosis via reduction of LDL oxidation | [31] |
| Mice (ApoEee), Rabbit | Custom transducer | 0.1–0.4 | 1 MHz | Biomechanical | Decrease in atherosclerosis in femoral arteries through decrease in macrophages and lipids | [26] |
| Swine | HIFU Synthesizer, International Cardio Corporation | 1.5 | 1 MHz | Thermal | Targeting the dorsal wall of the external femoral artery without endothelial damage | [73] |
| Mice (C57BL6) | EPIQ 7 | NA | 3.5 MHz | Biomechanical | Increased perfusion in hindlimb ischemia model for PAD | [38] |
| Porcine model | XL2020, Sonic | 6.0 | 1 MHz | Thermal | LIFU irradiation for coronarySono thrombolysis | [66] |
| (3D) Phantom flow model | vortex ultrasound transducer array | NA | 1.8 MHz | Biomechanical | In vitro vortex sonothrombolysis in cerebral venous sinus thrombosis | [48] |
| (PAD) Sprague-Dawley rat | SONOS 7500, Philips | NA | 1.3 MHz | Biomechanical | Decreases in hepatic arterial and portal venous flow resistance | [74] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Imtiaz, C.; Farooqi, M.A.; Bhatti, T.; Lee, J.; Moin, R.; Kang, C.U.; Farooqi, H.M.U. Focused Ultrasound, an Emerging Tool for Atherosclerosis Treatment: A Comprehensive Review. Life 2023, 13, 1783. https://doi.org/10.3390/life13081783
Imtiaz C, Farooqi MA, Bhatti T, Lee J, Moin R, Kang CU, Farooqi HMU. Focused Ultrasound, an Emerging Tool for Atherosclerosis Treatment: A Comprehensive Review. Life. 2023; 13(8):1783. https://doi.org/10.3390/life13081783
Chicago/Turabian StyleImtiaz, Cynthia, Muhammad Awais Farooqi, Theophilus Bhatti, Jooho Lee, Ramsha Moin, Chul Ung Kang, and Hafiz Muhammad Umer Farooqi. 2023. "Focused Ultrasound, an Emerging Tool for Atherosclerosis Treatment: A Comprehensive Review" Life 13, no. 8: 1783. https://doi.org/10.3390/life13081783
APA StyleImtiaz, C., Farooqi, M. A., Bhatti, T., Lee, J., Moin, R., Kang, C. U., & Farooqi, H. M. U. (2023). Focused Ultrasound, an Emerging Tool for Atherosclerosis Treatment: A Comprehensive Review. Life, 13(8), 1783. https://doi.org/10.3390/life13081783