

A Review of the Potential Benefits of Herbal Medicines, Small Molecules of Natural Sources, and Supplements for Health Promotion in Lupus Conditions

 ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Ethnobotany
3.2. Purified Molecules from Natural Sources
3.2.1. Artemisinin and Its Derivatives
Toxicity and Side Effects
3.2.2. Antroquinonol
Toxicity and Side Effects
3.2.3. Baicalin
Toxicity and Side Effects
3.2.4. Curcumin
In Vivo and In Vitro Studies
Toxicity and Side Effects
3.2.5. Emodin
Toxicity and Side Effects
3.2.6. Esculetin
Toxicity and Side Effects of Esculetin
3.2.7. Mangiferin
Toxicity and Side Effects
3.2.8. Salvianolic Acid A
Toxicity and Side Effects
3.2.9. Triptolide
Toxicity and Side Effects
3.2.10. Total Glycosides of Paeony (TGP)
Toxicity and Side Effects
3.3. Fatty Acids, Vitamins, and Minerals
3.3.1. Fatty Acids
3.3.2. Vitamin A
3.3.3. Vitamin B
3.3.4. Vitamin C
3.3.5. Vitamin D
3.3.6. Vitamin E
3.3.7. Calcium
3.3.8. Iron
3.3.9. Selenium
3.3.10. Zinc
3.4. Herbal Medicines, Medicinal Plants, Mushrooms, and Fungi and Their Crude Extracts
3.4.1. Tripterygium wilfordii Hook. F.
Clinical Trials
Active Compounds and Possible Mechanisms of Efficacy
Toxicity and Side Effects
3.4.2. Ophiocordyceps sinensis (syn. Cordyceps sinensis)
Clinical Trials
Active Compounds and Possible Mechanisms of Efficacy
Toxicity and Side Effects
3.4.3. Ganoderma Lucidum and Ganoderma Tsugae
Clinical Trials
Active Compounds and Possible Mechanisms of Efficacy
Toxicity and Side Effects
3.4.4. Urtica Dioica L.
Clinical Trials
Active Compounds and Possible Mechanisms of Efficacy
Toxicity and Side Effects
3.4.5. Nelumbo nucifera Gaertn.
Toxicity and Side Effects
3.4.6. Artemisia annua Pall.
Clinical Trial
Phytochemicals and Possible Mechanisms of Action
Toxicity and Side Effects
3.4.7. Linum usitatissimum L.
Clinical Trials
Phytochemicals and Possible Mechanisms of Action
Toxicity and Side Effects
3.4.8. Rehmannia glutinosa (Gaertn.) DC.
Clinical Trial
Phytochemicals and Possible Mechanisms of Action
Toxicity and Side Effects
3.4.9. Paeonia × suffruticosa Andrews
Clinical Trials
Toxicity and Side Effects
3.4.10. Paeonia lactiflora Pall.
Clinical Trials
Phytochemicals and Possible Mechanisms of Action
Toxicity and Side Effects
3.4.11. Scutellaria baicalensis Georgi
Phytochemicals and Possible Mechanisms of Action
Toxicity and Side Effects
3.4.12. Gentiana macrophylla Pall.
Clinical Trial
Animal Studies
Toxicity and Side Effects
3.4.13. Glycyrrhiza glabra L.
Phytochemicals and Possible Mechanisms of Action
Toxicity and Side Effects
3.4.14. Antrodia camphorata
Toxicity and Side Effects
3.4.15. Astragalus propinquus Schischkin (syn. Astragalus membranaceus (Fisch.) Bunge)
Toxicity and Side Effects
3.4.16. Bryophyllum pinnatum (Lam.) Oken
Toxicity and Side Effects
3.4.17. Anemarrhenae aspheloidis
Toxicity and Side Effects
3.4.18. Camellia sinensis (L.) Kuntze
Clinical Trial
Toxicity and Side Effects
3.4.19. Curcuma longa L.
Clinical Trials
Toxicity and Side Effects
3.5. Other Plants with Lower Evidence for Lupus Conditions
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dörner, T.; Furie, R. Novel paradigms in systemic lupus erythematosus. Lancet 2019, 393, 2344–2358. [Google Scholar] [CrossRef] [PubMed]
- Veeranki, S.; Choubey, D. Systemic lupus erythematosus and increased risk to develop B cell malignancies: Role of the p200-family proteins. Immunol. Lett. 2010, 133, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Lightfoot, Y.L.; Blanco, L.P.; Kaplan, M.J. Metabolic abnormalities and oxidative stress in lupus. Curr. Opin. Rheumatol. 2017, 29, 442. [Google Scholar] [CrossRef] [PubMed]
- Bertsias, G.K.; Pamfil, C.; Fanouriakis, A.; Boumpas, D.T. Diagnostic criteria for systemic lupus erythematosus: Has the time come? Nat. Rev. Rheumatol. 2013, 9, 687–694. [Google Scholar] [CrossRef] [PubMed]
- Bootsma, H.; Spronk, P.; de Boer, G.; Limburg, P.; Kallenberg, C.; Derksen, R.; Wolters-Dicke, J.; Gmelig-Meyling, F.; Kater, L.; Hermans, J. Prevention of relapses in systemic lupus erythematosus. Lancet 1995, 345, 1595–1599. [Google Scholar] [CrossRef]
- Loram, L.C.; Culp, M.E.; Connolly-Strong, E.C.; Sturgill-Koszycki, S. Melanocortin peptides: Potential targets in systemic lupus erythematosus. Inflammation 2015, 38, 260–271. [Google Scholar] [CrossRef]
- Fanouriakis, A.; Tziolos, N.; Bertsias, G.; Boumpas, D.T. Update οn the diagnosis and management of systemic lupus erythematosus. Ann. Rheum. Dis. 2021, 80, 14–25. [Google Scholar] [CrossRef]
- Mikdashi, J.; Nived, O. Measuring disease activity in adults with systemic lupus erythematosus: The challenges of administrative burden and responsiveness to patient concerns in clinical research. Arthritis Res. Ther. 2015, 17, 1–10. [Google Scholar] [CrossRef]
- Almaani, S.; Meara, A.; Rovin, B.H. Update on lupus nephritis. Clin. J. Am. Soc. Nephrol. 2017, 12, 825–835. [Google Scholar] [CrossRef]
- Hoover, P.J.; Costenbader, K.H. Insights into the epidemiology and management of lupus nephritis from the US rheumatologist’s perspective. Kidney Int. 2016, 90, 487–492. [Google Scholar] [CrossRef]
- Wallace, D.J. The evolution of drug discovery in systemic lupus erythematosus. Nat. Rev. Rheumatol. 2015, 11, 616–620. [Google Scholar] [CrossRef] [PubMed]
- Basta, F.; Fasola, F.; Triantafyllias, K.; Schwarting, A. Systemic lupus erythematosus (SLE) therapy: The old and the new. Rheumatol. Ther. 2020, 7, 433–446. [Google Scholar] [CrossRef] [PubMed]
- Kuhn, A.; Bonsmann, G.; Anders, H.-J.; Herzer, P.; Tenbrock, K.; Schneider, M. The diagnosis and treatment of systemic lupus erythematosus. Dtsch. Ärzteblatt Int. 2015, 112, 423. [Google Scholar] [CrossRef] [PubMed]
- Gurevitz, S.; Snyder, J.; Wessel, E.; Frey, J.; Williamson, B. Systemic lupus erythematosus: A review of the disease and treatment options. Consult. Pharm. 2013, 28, 110–121. [Google Scholar] [CrossRef]
- Tanaka, Y. State-of-the-art treatment of systemic lupus erythematosus. Int. J. Rheum. Dis. 2020, 23, 465–471. [Google Scholar] [CrossRef] [PubMed]
- Liossis, S.N.; Staveri, C. What’s new in the treatment of systemic lupus erythematosus. Front. Med. 2021, 8, 655100. [Google Scholar] [CrossRef] [PubMed]
- Verdelli, A.; Corrà, A.; Mariotti, E.B.; Aimo, C.; Ruffo di Calabria, V.; Volpi, W.; Quintarelli, L.; Caproni, M. An update on the management of refractory cutaneous lupus erythematosus. Front. Med. 2022, 9, 941003. [Google Scholar] [CrossRef]
- Schwartz, N.; Stock, A.D.; Putterman, C. Neuropsychiatric lupus: New mechanistic insights and future treatment directions. Nat. Rev. Rheumatol. 2019, 15, 137–152. [Google Scholar] [CrossRef]
- Lubov, J.E.; Jamison, A.S.; Baltich Nelson, B.; Amudzi, A.A.; Haas, K.N.; Richmond, J.M. Medicinal plant extracts and natural compounds for the treatment of cutaneous lupus erythematosus: A systematic review. Front. Pharmacol. 2022, 13, 802624. [Google Scholar] [CrossRef]
- Cao, F.; Cheng, M.-H.; Hu, L.-Q.; Shen, H.-H.; Tao, J.-H.; Li, X.-M.; Pan, H.-F.; Gao, J. Natural products action on pathogenic cues in autoimmunity: Efficacy in systemic lupus erythematosus and rheumatoid arthritis as compared to classical treatments. Pharmacol. Res. 2020, 160, 105054. [Google Scholar] [CrossRef]
- Momtazi-Borojeni, A.A.; Haftcheshmeh, S.M.; Esmaeili, S.-A.; Johnston, T.P.; Abdollahi, E.; Sahebkar, A. Curcumin: A natural modulator of immune cells in systemic lupus erythematosus. Autoimmun. Rev. 2018, 17, 125–135. [Google Scholar] [CrossRef] [PubMed]
- Duarte-Garcia, A.; Myasoedova, E.; Karmacharya, P.; Hocaoğlu, M.; Murad, M.H.; Warrington, K.J.; Crowson, C.S. Effect of omega-3 fatty acids on systemic lupus erythematosus disease activity: A systematic review and meta-analysis. Autoimmun. Rev. 2020, 19, 102688. [Google Scholar] [CrossRef] [PubMed]
- Yuan, K.; Li, X.; Lu, Q.; Zhu, Q.; Jiang, H.; Wang, T.; Huang, G.; Xu, A. Application and mechanisms of triptolide in the treatment of inflammatory diseases—A review. Front. Pharmacol. 2019, 10, 1469. [Google Scholar] [CrossRef] [PubMed]
- Vahedi-Mazdabadi, Y.; Saeedi, M. Treatment of Lupus Nephritis from Iranian Traditional Medicine and Modern Medicine Points of View: A Comparative Study. Evid.-Based Complement. Altern. Med. 2021, 2021, 6645319. [Google Scholar] [CrossRef]
- Gururaja, D.; Hegde, V. Ayurvedic management of systemic lupus erythematosus overlap vasculitis. J. Ayurveda Integr. Med. 2019, 10, 294–298. [Google Scholar] [CrossRef]
- Salek, M.; Hosseini Hooshiar, S.; Salek, M.; Poorebrahimi, M.; Jafarnejad, S. Omega-3 fatty acids: Current insights into mechanisms of action in systemic lupus erythematosus. Lupus 2023, 32, 7–22. [Google Scholar] [CrossRef]
- Huerta, M.D.R.; Trujillo-Martin, M.M.; Rúa-Figueroa, Í.; Cuellar-Pompa, L.; Quiros-Lopez, R.; Serrano-Aguilar, P.; Spanish, S. Healthy lifestyle habits for patients with systemic lupus erythematosus: A systemic review. Semin. Arthritis Rheum. 2016, 45, 463–470. [Google Scholar] [CrossRef]
- Zheng, R.; Gonzalez, A.; Yue, J.; Wu, X.; Qiu, M.; Gui, L.; Zhu, S.; Huang, L. Efficacy and safety of vitamin D supplementation in patients with systemic lupus erythematosus: A meta-analysis of randomized controlled trials. Am. J. Med. Sci. 2019, 358, 104–114. [Google Scholar] [CrossRef]
- Islam, M.A.; Khandker, S.S.; Alam, S.S.; Kotyla, P.; Hassan, R. Vitamin D status in patients with systemic lupus erythematosus (SLE): A systematic review and meta-analysis. Autoimmun. Rev. 2019, 18, 102392. [Google Scholar] [CrossRef]
- Balkrishna, A.; Thakur, P.; Singh, S.; Chandra Dev, S.N.; Varshney, A. Mechanistic paradigms of natural plant metabolites as remedial candidates for systemic lupus erythromatosus. Cells 2020, 9, 1049. [Google Scholar] [CrossRef]
- Thomas, D.E. The Lupus Encyclopedia: A Comprehensive Guide for Patients and Families; JHU Press: Baltimore, MD, USA, 2014. [Google Scholar]
- Fu, S.M.; Gaskin, F. History of systemic lupus erythematosus with an emphasis on certain recent major issues. In Systemic Lupus Erythematosus; Elsevier: Amsterdam, The Netherlands, 2021; pp. 3–8. [Google Scholar]
- Tene, V.; Malagon, O.; Finzi, P.V.; Vidari, G.; Armijos, C.; Zaragoza, T. An ethnobotanical survey of medicinal plants used in Loja and Zamora-Chinchipe, Ecuador. J. Ethnopharmacol. 2007, 111, 63–81. [Google Scholar] [CrossRef] [PubMed]
- Kyaw, M.S.; Aye, M.M.; Grinnell, M.; Rabach, M. Traditional and ethnobotanical dermatology practices in Myanmar. Clin. Dermatol. 2018, 36, 320–324. [Google Scholar] [CrossRef] [PubMed]
- Magee, A.; Van Wyk, B.-E.; Van Vuuren, S. Ethnobotany and antimicrobial activity of sieketroos (Arctopus species). S. Afr. J. Bot. 2007, 73, 159–162. [Google Scholar] [CrossRef]
- Orhan, N.; Akkol, E.; Ergun, F. Evaluation of antiinflammatory and antinociceptive effects of some Juniperus species growing in Turkey. Turk. J. Biol. 2012, 36, 719–726. [Google Scholar] [CrossRef]
- Gilca, M.; Tiplica, G.S.; Salavastru, C.M. Traditional and ethnobotanical dermatology practices in Romania and other Eastern European countries. Clin. Dermatol. 2018, 36, 338–352. [Google Scholar] [CrossRef]
- Verma, R.; Singh, H.; Thakur, A.; Kohli, S. Ethnobotanical survey of medicinal and aromatic plants of Bhagalpur Region. Int. J. Appl. Sci. Biotechnol. 2020, 8, 216–222. [Google Scholar] [CrossRef]
- Sharififar, F.; Yassa, N.; Mozaffarian, V. Bioactivity of major components from the seeds of Bunium persicum (Boiss.) Fedtch. Pak. J. Pharm. Sci. 2010, 23, 300–304. [Google Scholar]
- Abou El-Soud, N.H.; El-Lithy, N.A.; El-Saeed, G.; Wahby, M.S.; Khalil, M.Y.; Morsy, F.; Shaffie, N. Renoprotective effects of caraway (Carum carvi L.) essential oil in streptozotocin induced diabetic rats. J. Appl. Pharm. Sci. 2014, 4, 027–033. [Google Scholar] [CrossRef]
- Aghili, M.H. Makhzan-al-Advia; Tehran University of Medical Sciences: Tehran, Iran, 2009; pp. 227–228. (In Persian) [Google Scholar]
- Ardakani, M.R.S.; Farjadmand, F.; Rahimi, R. Makhzan al adviyeh and pointing to the scientific names of medicinal plants for the first time in a persian book. Tradit. Integr. Med. 2018, 3, 186–195. [Google Scholar]
- Seri, A.; Khorsand, M.; Rezaei, Z.; Hamedi, A.; Takhshid, M.A. Inhibitory effect of bunium persicum hydroalcoholic extract on glucose-induced albumin glycation, oxidation, and aggregation in vitro. Iran. J. Med. Sci. 2017, 42, 369. [Google Scholar]
- Mehrabadi, M.M.; Zarshenas, M.M. A Concise Overview of Phytochemistry, Pharmacology and Clinical Aspects of Persian Cumin; Bunium persicum (Boiss.) B. Fedtsch. Curr. Drug Discov. Technol. 2021, 18, 485–491. [Google Scholar] [CrossRef] [PubMed]
- Bansal, S.; Sharma, K.; Gautam, V.; Lone, A.A.; Malhotra, E.V.; Kumar, S.; Singh, R. A comprehensive review of Bunium persicum: A valuable medicinal spice. Food Rev. Int. 2021, 39, 1184–1202. [Google Scholar] [CrossRef]
- Chang, J.-M.; Lee, Y.-R.; Hung, L.-M.; Liu, S.-Y.; Kuo, M.-T.; Wen, W.-C.; Chen, P. An extract of Antrodia camphorata mycelia attenuates the progression of nephritis in systemic lupus erythematosus-prone NZB/W F1 mice. Evid.-Based Complement. Altern. Med. 2011, 2011, 465894. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Han, C.; Sheng, Y.; Wang, J.; Li, W.; Zhou, X.; Ruan, S. Antrodia camphorata polysaccharide improves inflammatory response in liver injury via the ROS/TLR4/NF-κB signal. J. Cell. Mol. Med. 2022, 26, 2706–2716. [Google Scholar] [CrossRef]
- Kushairi, N.; Tarmizi, N.A.K.A.; Phan, C.W.; Macreadie, I.; Sabaratnam, V.; Naidu, M.; David, P. Modulation of neuroinflammatory pathways by medicinal mushrooms, with particular relevance to Alzheimer’s disease. Trends Food Sci. Technol. 2020, 104, 153–162. [Google Scholar] [CrossRef]
- Septembre-Malaterre, A.; Lalarizo Rakoto, M.; Marodon, C.; Bedoui, Y.; Nakab, J.; Simon, E.; Hoarau, L.; Savriama, S.; Strasberg, D.; Guiraud, P.; et al. Artemisia annua, a Traditional Plant Brought to Light. Int. J. Mol. Sci. 2020, 21, 4986. [Google Scholar] [CrossRef]
- Alesaeidi, S.; Miraj, S. A Systematic Review of Anti-malarial Properties, Immunosuppressive Properties, Anti-inflammatory Properties, and Anti-cancer Properties of Artemisia Annua. Electron. Physician 2016, 8, 3150–3155. [Google Scholar] [CrossRef]
- Durazzo, A.; Nazhand, A.; Lucarini, M.; Silva, A.M.; Souto, S.B.; Guerra, F.; Severino, P.; Zaccardelli, M.; Souto, E.B.; Santini, A. Astragalus (Astragalus membranaceus Bunge): Botanical, geographical, and historical aspects to pharmaceutical components and beneficial role. Rend. Lincei. Sci. Fis. Nat. 2021, 32, 625–642. [Google Scholar] [CrossRef]
- Chibli, L.A.; Rodrigues, K.C.; Gasparetto, C.M.; Pinto, N.C.; Fabri, R.L.; Scio, E.; Alves, M.S.; Del-Vechio-Vieira, G.; Sousa, O.V. Anti-inflammatory effects of Bryophyllum pinnatum (Lam.) Oken ethanol extract in acute and chronic cutaneous inflammation. J. Ethnopharmacol. 2014, 154, 330–338. [Google Scholar] [CrossRef]
- Smith, G.F.; Figueiredo, E.; van Wyk, A.E. Chapter 12—Taxonomic Treatment. In Kalanchoe (Crassulaceae) in Southern Africa; Smith, G.F., Figueiredo, E., van Wyk, A.E., Eds.; Academic Press: Cambridge, MA, USA, 2019; pp. 131–303. [Google Scholar]
- Mule, P.; Upadhye, M.; Taru, P.; Dhole, S. A Review on Bryophyllum pinnatum (Lam.) Oken. Res. J. Pharmacogn. Phytochem. 2020, 12, 111. [Google Scholar] [CrossRef]
- Sánchez, M.; González-Burgos, E.; Iglesias, I.; Lozano, R.; Gómez-Serranillos, M.P. The Pharmacological Activity of Camellia sinensis (L.) Kuntze on Metabolic and Endocrine Disorders: A Systematic Review. Biomolecules 2020, 10, 603. [Google Scholar] [CrossRef]
- Oliveira, A.; Guimarães, A.; Oliveira Junior, R.; Quintans, J.; Medeiros, F.; Barbosa Filho, J.; Quintans-Júnior, L.; Almeida, J.R. Camellia sinensis (L.) Kuntze: A Review of Chemical and Nutraceutical Properties. Nat. Prod. Res. Rev. 2016, 4, 21–62. [Google Scholar]
- Umesh, C.V. Chapter 13—Camellia sinensis. In Herbs, Spices and Their Roles in Nutraceuticals and Functional Foods; Amalraj, A., Kuttappan, S., Varma A.C, K., Matharu, A., Eds.; Academic Press: Cambridge, MA, USA, 2023; pp. 219–231. [Google Scholar]
- Sahoo, J.P.; Behera, L.; Praveena, J.; Sawant, S.; Mishra, A.; Sharma, S.S.; Ghosh, L.; Mishra, A.P.; Sahoo, A.R.; Pradhan, P. The golden spice turmeric (Curcuma longa) and its feasible benefits in prospering human health—A review. Am. J. Plant Sci. 2021, 12, 455–475. [Google Scholar] [CrossRef]
- Varma, A.C.K.; Jude, S.; Varghese, B.A.; Kuttappan, S.; Amalraj, A. Chapter 2—Curcuma longa. In Herbs, Spices and Their Roles in Nutraceuticals and Functional Foods; Amalraj, A., Kuttappan, S., Varma A.C, K., Matharu, A., Eds.; Academic Press: Cambridge, MA, USA, 2023; pp. 15–30. [Google Scholar]
- Jyotirmayee, B.; Mahalik, G. A review on selected pharmacological activities of Curcuma longa L. Int. J. Food Prop. 2022, 25, 1377–1398. [Google Scholar] [CrossRef]
- Wachtel-Galor, S.; Yuen, J.; Buswell, J.A.; Benzie, I.F.F. Ganoderma lucidum (Lingzhi or Reishi): A Medicinal Mushroom. In Herbal Medicine: Biomolecular and Clinical Aspects, 2nd ed.; CRC Press/Taylor & Francis: Boca Raton, FL, USA, 2011. [Google Scholar]
- Sanodiya, B.S.; Thakur, G.S.; Baghel, R.K.; Prasad, G.B.; Bisen, P.S. Ganoderma lucidum: A potent pharmacological macrofungus. Curr. Pharm. Biotechnol. 2009, 10, 717–742. [Google Scholar] [CrossRef]
- Ahmad, R.; Riaz, M.; Khan, A.; Aljamea, A.; Algheryafi, M.; Sewaket, D.; Alqathama, A. Ganoderma lucidum (Reishi) an edible mushroom; a comprehensive and critical review of its nutritional, cosmeceutical, mycochemical, pharmacological, clinical, and toxicological properties. Phytother. Res. PTR 2021, 35, 6030–6062. [Google Scholar] [CrossRef]
- Yu, Y.H.; Kuo, H.P.; Hsieh, H.H.; Li, J.W.; Hsu, W.H.; Chen, S.J.; Su, M.H.; Liu, S.H.; Cheng, Y.C.; Chen, C.Y.; et al. Ganoderma tsugae Induces S Phase Arrest and Apoptosis in Doxorubicin-Resistant Lung Adenocarcinoma H23/0.3 Cells via Modulation of the PI3K/Akt Signaling Pathway. Evid.-Based Complement. Altern. Med. 2012, 2012, 371286. [Google Scholar] [CrossRef] [PubMed]
- Jiang, M.; Cui, B.-W.; Wu, Y.-L.; Nan, J.-X.; Lian, L.-H. Genus Gentiana: A review on phytochemistry, pharmacology and molecular mechanism. J. Ethnopharmacol. 2021, 264, 113391. [Google Scholar] [CrossRef]
- Zhang, X.; Zhan, G.; Jin, M.; Zhang, H.; Dang, J.; Zhang, Y.; Guo, Z.; Ito, Y. Botany, traditional use, phytochemistry, pharmacology, quality control, and authentication of Radix Gentianae Macrophyllae-A traditional medicine: A review. Phytomedicine 2018, 46, 142–163. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.-Y.; Hsu, T.-C.; Kuo, W.-W.; Liou, Y.-F.; Lee, S.-D.; Ju, D.-T.; Kuo, C.-H.; Tzang, B.-S. The root extract of Gentiana macrophylla Pall. Alleviates cardiac apoptosis in lupus prone mice. PLoS ONE 2015, 10, e0127440. [Google Scholar] [CrossRef]
- Pasdaran, A.; Naychov, Z.; Batovska, D.; Kerr, P.; Favre, A.; Dimitrov, V.; Aneva, I.; Hamedi, A.; Kozuharova, E. Some European Gentiana Species Are Used Traditionally to Cure Wounds: Bioactivity and Conservation Issues. Diversity 2023, 15, 467. [Google Scholar] [CrossRef]
- Ravanfar, P.; Namazi, G.; Atigh, M.; Zafarmand, S.; Hamedi, A.; Salehi, A.; Izadi, S.; Borhani-Haghighi, A. Efficacy of whole extract of licorice in neurological improvement of patients after acute ischemic stroke. J. Herb. Med. 2016, 6, 12–17. [Google Scholar] [CrossRef]
- Petramfar, P.; Hajari, F.; Yousefi, G.; Azadi, S.; Hamedi, A. Efficacy of oral administration of licorice as an adjunct therapy on improving the symptoms of patients with Parkinson’s disease, A randomized double blinded clinical trial. J. Ethnopharmacol. 2020, 247, 112226. [Google Scholar] [CrossRef] [PubMed]
- Ayeka, P.A.; Bian, Y.; Githaiga, P.M.; Zhao, Y. The immunomodulatory activities of licorice polysaccharides (Glycyrrhiza uralensis Fisch.) in CT 26 tumor-bearing mice. BMC Complement. Altern. Med. 2017, 17, 536. [Google Scholar] [CrossRef]
- Jiang, M.; Zhao, S.; Yang, S.; Lin, X.; He, X.; Wei, X.; Song, Q.; Li, R.; Fu, C.; Zhang, J. An “essential herbal medicine”—Licorice: A review of phytochemicals and its effects in combination preparations. J. Ethnopharmacol. 2020, 249, 112439. [Google Scholar] [CrossRef]
- Ansari, R.; Zarshenas, M.M.; Dadbakhsh, A. A Review on Pharmacological and Clinical Aspects of Linum usitatissimum L. Curr. Drug Discov. Technol. 2018, 15, 148–158. [Google Scholar] [CrossRef]
- Ganguly, S.; Panjagari, N.R.; Raman, R.K. Flaxseed (Linum usitatissimum). In Oilseeds: Health Attributes and Food Applications; Springer: Berlin/Heidelberg, Germany, 2021; pp. 253–283. [Google Scholar]
- Heydarirad, G.; Tavakoli, A.; Cooley, K.; Pasalar, M. A review on medical plants advised for neuralgia from the perspective of “canon of medicine”. Adv. Integr. Med. 2021, 8, 230–235. [Google Scholar] [CrossRef]
- Mehta, N.; Patel, E.P.; Pragnesh, B.S.V.P.; Shah, B. Nelumbo nucifera (Lotus): A review on ethanobotany, phytochemistry and pharmacology. Indian J. Pharm. Biol. Res. 2013, 1, 152–167. [Google Scholar] [CrossRef]
- Sharma, B.R.; Gautam, L.N.S.; Adhikari, D.; Karki, R. A comprehensive review on chemical profiling of Nelumbo nucifera: Potential for drug development. Phytother. Res. 2017, 31, 3–26. [Google Scholar] [CrossRef] [PubMed]
- Luo, Y.; Yang, S.K.; Zhou, X.; Wang, M.; Tang, D.; Liu, F.Y.; Sun, L.; Xiao, L. Use of Ophiocordyceps sinensis (syn. Cordyceps sinensis) combined with angiotensin-converting enzyme inhibitors (ACEI)/angiotensin receptor blockers (ARB) versus ACEI/ARB alone in the treatment of diabetic kidney disease: A meta-analysis. Ren. Fail. 2015, 37, 614–634. [Google Scholar] [CrossRef]
- Lo, H.-C.; Hsieh, C.; Lin, F.-Y.; Hsu, T.-H. A systematic review of the mysterious caterpillar fungus Ophiocordyceps sinensis in DongChongXiaCao (冬蟲夏草 Dōng Chóng Xià Cǎo) and related bioactive ingredients. J. Tradit. Complement. Med. 2013, 3, 16–32. [Google Scholar] [CrossRef] [PubMed]
- He, D.Y.; Dai, S.M. Anti-inflammatory and immunomodulatory effects of paeonia lactiflora pall., a traditional chinese herbal medicine. Front. Pharmacol. 2011, 2, 10. [Google Scholar] [CrossRef]
- Wang, Z.; He, C.; Peng, Y.; Chen, F.; Xiao, P. Origins, Phytochemistry, Pharmacology, Analytical Methods and Safety of Cortex Moutan (Paeonia suffruticosa Andrew): A Systematic Review. Molecules 2017, 22, 946. [Google Scholar] [CrossRef]
- Kim, Y.G.; Komakech, R.; Jeong, D.H.; Park, Y.M.; Lee, T.K.; Kim, K.H.; Lee, A.Y.; Moon, B.C.; Kang, Y. Verification of the Field Productivity of Rehmannia glutinosa (Gaertn.) DC. Developed Through Optimized In Vitro Culture Method. Plants 2020, 9, 317. [Google Scholar] [CrossRef] [PubMed]
- Bian, Z.; Zhang, R.; Zhang, X.; Zhang, J.; Xu, L.; Zhu, L.; Ma, Y.; Liu, Y. Extraction, structure and bioactivities of polysaccharides from Rehmannia glutinosa: A review. J. Ethnopharmacol. 2023, 305, 116132. [Google Scholar] [CrossRef] [PubMed]
- Zhao, T.; Tang, H.; Xie, L.; Zheng, Y.; Ma, Z.; Sun, Q.; Li, X. Scutellaria baicalensis Georgi. (Lamiaceae): A review of its traditional uses, botany, phytochemistry, pharmacology and toxicology. J. Pharm. Pharmacol. 2019, 71, 1353–1369. [Google Scholar] [CrossRef]
- Song, J.-W.; Long, J.-Y.; Xie, L.; Zhang, L.-L.; Xie, Q.-X.; Chen, H.-J.; Deng, M.; Li, X.-F. Applications, phytochemistry, pharmacological effects, pharmacokinetics, toxicity of Scutellaria baicalensis Georgi. and its probably potential therapeutic effects on COVID-19: A review. Chin. Med. 2020, 15, 102. [Google Scholar] [CrossRef]
- Billah, M.M.; Khan, F.; Niaz, K. Chapter 3.38—Scutellaria baicalensis Georgi. In Nonvitamin and Nonmineral Nutritional Supplements; Nabavi, S.M., Silva, A.S., Eds.; Academic Press: Cambridge, MA, USA, 2019; pp. 403–408. [Google Scholar]
- Song, C.Y.; Xu, Y.G.; Lu, Y.Q. Use of Tripterygium wilfordii Hook F for immune-mediated inflammatory diseases: Progress and future prospects. J. Zhejiang Univ. Sci. B 2020, 21, 280–290. [Google Scholar] [CrossRef]
- Brinker, A.M.; Ma, J.; Lipsky, P.E.; Raskin, I. Medicinal chemistry and pharmacology of genus Tripterygium (Celastraceae). Phytochemistry 2007, 68, 732–766. [Google Scholar] [CrossRef]
- Devkota, H.P.; Paudel, K.R.; Khanal, S.; Baral, A.; Panth, N.; Adhikari-Devkota, A.; Jha, N.K.; Das, N.; Singh, S.K.; Chellappan, D.K.; et al. Stinging Nettle (Urtica dioica L.): Nutritional Composition, Bioactive Compounds, and Food Functional Properties. Molecules 2022, 27, 5219. [Google Scholar] [CrossRef]
- Hamedi, A.; Sakhteman, A.; Moheimani, S.M. An in silico approach towards investigation of possible effects of essential oils constituents on receptors involved in cardiovascular diseases (CVD) and associated risk factors (Diabetes Mellitus and Hyperlipidemia). Cardiovasc. Hematol. Agents Med. Chem. (Former. Curr. Med. Chem.-Cardiovasc. Hematol. Agents) 2021, 19, 32–42. [Google Scholar] [CrossRef]
- Ebrahimi-Najafabadi, H.; Kazemeini, S.S.; Pasdaran, A.; Hamedi, A. A novel similarity search approach for high-performance thin-layer chromatography (HPTLC) fingerprinting of medicinal plants. Phytochem. Anal. 2019, 30, 405–414. [Google Scholar] [CrossRef] [PubMed]
- Mojab, F.; Hamedi, A.; Nickavar, B.; Javidnia, K. Hydrodistilled volatile constituents of the leaves of Daucus carota L. subsp. sativus (Hoffman.) Arcang. (Apiaceae) from Iran. J. Essent. Oil Bear. Plants 2008, 11, 271–277. [Google Scholar] [CrossRef]
- Tsai, P.Y.; Ka, S.M.; Chang, J.M.; Lai, J.H.; Dai, M.S.; Jheng, H.L.; Kuo, M.T.; Chen, P.; Chen, A. Antroquinonol differentially modulates T cell activity and reduces interleukin-18 production, but enhances Nrf2 activation, in murine accelerated severe lupus nephritis. Arthritis Rheum. 2012, 64, 232–242. [Google Scholar] [CrossRef]
- Liu, C.-P.; Tsai, W.-J.; Shen, C.-C.; Lin, Y.-L.; Liao, J.-F.; Chen, C.-F.; Kuo, Y.-C. Inhibition of (S)-armepavine from Nelumbo nucifera on autoimmune disease of MRL/MpJ-lpr/lpr mice. Eur. J. Pharmacol. 2006, 531, 270–279. [Google Scholar] [CrossRef]
- Lan, L. Study on effect of Cordyceps sinensis and artemisinin in preventing recurrence of lupus nephritis. Chin. J. Integr. Tradit. West. Med. 2002, 8, 89. [Google Scholar] [CrossRef]
- Yang, L.-Y.; Chen, A.; Kuo, Y.-C.; Lin, C.-Y. Efficacy of a pure compound H1-A extracted from Cordyceps sinensis on autoimmune disease of MRL lpr/lpr mice. J. Lab. Clin. Med. 1999, 134, 492–500. [Google Scholar] [CrossRef] [PubMed]
- Hou, L.F.; He, S.J.; Li, X.; Yang, Y.; He, P.L.; Zhou, Y.; Zhu, F.H.; Yang, Y.F.; Li, Y.; Tang, W. Oral administration of artemisinin analog SM934 ameliorates lupus syndromes in MRL/lpr mice by inhibiting Th1 and Th17 cell responses. Arthritis Rheum. 2011, 63, 2445–2455. [Google Scholar] [CrossRef]
- Yang, J.; Yang, X.; Yang, J.; Li, M. Baicalin ameliorates lupus autoimmunity by inhibiting differentiation of Tfh cells and inducing expansion of Tfr cells. Cell Death Dis. 2019, 10, 140. [Google Scholar] [CrossRef]
- Chae, B.-S. Baicalin Ameliorates Dysimmunoregulation in Pristane-Induced Lupus Mice: Production of IL-6 and PGE2 and Activation of T cells. Nat. Prod. Sci. 2011, 17, 354–362. [Google Scholar]
- Handono, K.; Pratama, M.Z.; Endharti, A.T.; Kalim, H. Treatment of low doses curcumin could modulate Th17/Treg balance specifically on CD4+ T cell cultures of systemic lupus erythematosus patients. Cent. Eur. J. Immunol. 2015, 40, 461–469. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Wang, J.; Zhou, M.; Li, M.; Li, M.; Tan, H. Curcumin attenuates murine lupus via inhibiting NLRP3 inflammasome. Int. Immunopharmacol. 2019, 69, 213–216. [Google Scholar] [CrossRef] [PubMed]
- Dent, E.L.; Taylor, E.B.; Turbeville, H.R.; Ryan, M.J. Curcumin attenuates autoimmunity and renal injury in an experimental model of systemic lupus erythematosus. Physiol. Rep. 2020, 8, e14501. [Google Scholar] [CrossRef]
- Kalim, H.; Handono, K.; Khalasha, T.; Pratama, M.Z.; Dantara, T.W.I.; Wulandari, A.P.; Albinsaid, F.; Fitria, S.N.; Mahardika, M.V. Immune modulation effects of curcumin in pristane-induced lupus mice. Indian J. Rheumatol. 2017, 12, 86. [Google Scholar] [CrossRef]
- Li, W.-D.; Dong, Y.-J.; Tu, Y.-Y.; Lin, Z.-B. Dihydroarteannuin ameliorates lupus symptom of BXSB mice by inhibiting production of TNF-alpha and blocking the signaling pathway NF-kappa B translocation. Int. Immunopharmacol. 2006, 6, 1243–1250. [Google Scholar] [CrossRef]
- Zhang, T.; Zhang, Y.; Jiang, N.; Zhao, X.; Sang, X.; Yang, N.; Feng, Y.; Chen, R.; Chen, Q. Dihydroartemisinin regulates the immune system by promotion of CD8+ T lymphocytes and suppression of B cell responses. Sci. China Life Sci. 2020, 63, 737–749. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Tao, T.; Wang, W.; Yang, B.; Cha, X. Dihydroartemisinin attenuated the symptoms of mice model of systemic lupus erythematosus by restoring the Treg/Th17 balance. Clin. Exp. Pharmacol. Physiol. 2021, 48, 626–633. [Google Scholar] [CrossRef]
- Xia, Y.; Xu, S. Effect of emodin on nephritis of BXSB lupus mice and its pharmacological mechanism. Cent. China Med. J. 2003, 27, 63–64. [Google Scholar]
- Yuan, X.; Dai, B.; Yang, L.; Lin, B.; Lin, E.; Pan, Y. Emodin ameliorates renal injury in BXSB mice by modulating TNF-α/ICAM-1. Biosci. Rep. 2020, 40, BSR20202551. [Google Scholar] [CrossRef]
- Zhang, Y.; Li, Z.; Wu, H.; Wang, J.; Zhang, S. Esculetin alleviates murine lupus nephritis by inhibiting complement activation and enhancing Nrf2 signaling pathway. J. Ethnopharmacol. 2022, 288, 115004. [Google Scholar] [CrossRef] [PubMed]
- Lu, M.; Yu, S.; Xu, W.; Gao, B.; Xiong, S. HMGB1 promotes systemic lupus erythematosus by enhancing macrophage inflammatory response. J. Immunol. Res. 2015, 2015, 946748. [Google Scholar] [CrossRef]
- Garcia-Gordillo, M.A.; Collado-Mateo, D.; Hernández-Mocholi, M.A.; Pazzi, F.; Gusi, N.; Dominguez-Munoz, F.J.; Adsuar, J.C. Cost-Utility Analysis of a Six-Weeks Ganoderma Lucidum-Based Treatment for Women with Fibromyalgia: A Randomized Double-Blind, Active Placebo-Controlled Trial. Myopain 2015, 23, 188–194. [Google Scholar] [CrossRef]
- Maekawa, T.; Kosuge, S.; Karino, A.; Okano, T.; Ito, J.; Munakata, H.; Ohtsuki, K. Biochemical characterization of 60S acidic ribosomal P proteins from porcine liver and the inhibition of their immunocomplex formation with sera from systemic lupus erythematosus (SLE) patients by glycyrrhizin in vitro. Biol. Pharm. Bull. 2000, 23, 27–32. [Google Scholar] [CrossRef]
- Liang, C.-L.; Lu, W.; Zhou, J.-Y.; Chen, Y.; Zhang, Q.; Liu, H.; Qiu, F.; Dai, Z. Mangiferin attenuates murine lupus nephritis by inducing CD4+ Foxp3+ regulatory T cells via suppression of mTOR signaling. Cell. Physiol. Biochem. 2018, 50, 1560–1573. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.; Yan, Y.; Zhang, H.; Chen, Y.; He, Y.; Wang, S.; Fang, L.; Lv, Y.; Du, G. Salvianolic acid A alleviates renal injury in systemic lupus erythematosus induced by pristane in BALB/c mice. Acta Pharm. Sin. B 2017, 7, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Xiao, W.; Hou, P. Clinical study of total glucosides of paeony in patients with systemic lupus erythematosus. Zhongguo Zhong Xi Yi Jie He Za Zhi Zhongguo Zhongxiyi Jiehe Zazhi = Chin. J. Integr. Tradit. West. Med. 2011, 31, 476–479. [Google Scholar]
- Shuai, Z.-w.; Xu, J.-h.; Liu, S. Clinical study on effect of Total Glucosides of Peony in treating systemic lupus erythematosus as adjuvant treatment. Chin. J. Integr. Tradit. West. Med. 2003, 23, 188–191. [Google Scholar]
- Gong, X.; Li, H.; Guo, H.; Wu, S.; Lu, C.; Chen, Y.; Li, S. Efficacy and safety of total glucosides of paeony in the treatment of systemic lupus erythematosus: A systematic review and meta-analysis. Front. Pharmacol. 2022, 13, 932874. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Jiang, A. DNA methylation was involved in total glucosides of paeony regulating ERα for the treatment of female systemic lupus erythematosus mice. J. Pharmacol. Sci. 2019, 140, 187–192. [Google Scholar] [CrossRef]
- Ding, Z.-X.; Yang, S.-F.; Wu, Q.-F.; Lu, Y.; Chen, Y.-Y.; Nie, X.-L.; Jie, H.-Y.; Qi, J.-M.; Wang, F.-S. Therapeutic effect of total glucosides of paeony on lupus nephritis in MRL/lpr mice. J. South. Med. Univ. 2011, 31, 656–660. [Google Scholar]
- Zhao, M.; Liang, G.; Luo, S.; Lu, Q. Effect of total glucosides of peony on expression and DNA methylation status of ITGAL gene in CD4 (+) T cells of systemic lupus erythematosus. Zhong Nan Da Xue Xue Bao. Yi Xue Ban = J. Cent. South Univ. Med. Sci. 2012, 37, 463–468. [Google Scholar]
- Liu, L.; Jiao, W.; Zhang, X.; Zhang, Y.; Zhao, G.; Sun, Y.; Shuhua, L. Regulation on function and maturation of dendritic cells from systemic lupus erythematosus patients by triptolide. Chin. J. Microbiol. Immunol. 2011, 31, 824–829. [Google Scholar]
- Liu, Y.-F.; He, H.-Q.; Ding, Y.-L.; Wu, S.-Y.; Chen, D.-S.; CL, E. Effects of Triptolide on Tc and Th Cell Excursion in Peripheral Blood of Nude Mice with Systemic Lupus Erythematosus BALB/c-un. Zhongguo Shi Yan Xue Ye Xue Za Zhi 2019, 27, 1691–1695. [Google Scholar] [PubMed]
- Tao, X.; Fan, F.; Hoffmann, V.; Gao, C.Y.; Longo, N.S.; Zerfas, P.; Lipsky, P.E. Effective therapy for nephritis in (NZB × NZW) F1 mice with triptolide and tripdiolide, the principal active components of the Chinese herbal remedy Tripterygium wilfordii Hook F. Arthritis Rheum. Off. J. Am. Coll. Rheumatol. 2008, 58, 1774–1783. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.; Tang, X.; Yan, Q.; Song, H.; Li, Z.; Wang, D.; Chen, H.; Sun, L. Triptolide ameliorates lupus via the induction of miR-125a-5p mediating Treg upregulation. Int. Immunopharmacol. 2019, 71, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.-Y.; Li, H.; Wu, Y.-W.; Cheng, L.; Yan, Y.-X.; Yang, X.-Q.; Zhu, F.-H.; He, S.-J.; Tang, W.; Zuo, J.-P. (5R)-5-hydroxytriptolide ameliorates lupus nephritis in MRL/lpr mice by preventing infiltration of immune cells. Am. J. Physiol.-Ren. Physiol. 2017, 312, F769–F777. [Google Scholar] [CrossRef] [PubMed]
- Halade, G.V.; Rahman, M.M.; Bhattacharya, A.; Barnes, J.L.; Chandrasekar, B.; Fernandes, G. Docosahexaenoic acid-enriched fish oil attenuates kidney disease and prolongs median and maximal life span of autoimmune lupus-prone mice. J. Immunol. 2010, 184, 5280–5286. [Google Scholar] [CrossRef]
- Fettouh, D.S.; Saif, D.S.; El Gazzar, S.F.; Sonbol, A.A. Study the relationship between vitamin A deficiency, T helper 17, regulatory T cells, and disease activity in patients with systemic lupus erythematosus. Egypt. Rheumatol. Rehabil. 2019, 46, 244–250. [Google Scholar] [CrossRef]
- Handono, K.; Firdausi, S.N.; Pratama, M.Z.; Endharti, A.T.; Kalim, H. Vitamin A improve Th17 and Treg regulation in systemic lupus erythematosus. Clin. Rheumatol. 2016, 35, 631–638. [Google Scholar] [CrossRef] [PubMed]
- Minami, Y.; Hirabayashi, Y.; Nagata, C.; Ishii, T.; Harigae, H.; Sasaki, T. Intakes of vitamin B6 and dietary fiber and clinical course of systemic lupus erythematosus: A prospective study of Japanese female patients. J. Epidemiol. 2011, 21, 246–254. [Google Scholar] [CrossRef]
- Shah, M.; Adams-Huet, B.; Kavanaugh, A.; Coyle, Y.; Lipsky, P. Nutrient intake and diet quality in patients with systemic lupus erythematosus on a culturally sensitive cholesterol lowering dietary program. J. Rheumatol. 2004, 31, 71–75. [Google Scholar]
- Minami, Y.; Sasaki, T.; Arai, Y.; Kurisu, Y.; Hisamichi, S. Diet and systemic lupus erythematosus: A 4 year prospective study of Japanese patients. J. Rheumatol. 2003, 30, 747–754. [Google Scholar] [PubMed]
- Ben-Zvi, I.; Aranow, C.; Mackay, M.; Stanevsky, A.; Kamen, D.L.; Marinescu, L.M.; Collins, C.E.; Gilkeson, G.S.; Diamond, B.; Hardin, J.A. The impact of vitamin D on dendritic cell function in patients with systemic lupus erythematosus. PLoS ONE 2010, 5, e9193. [Google Scholar] [CrossRef] [PubMed]
- Antico, A.; Tampoia, M.; Tozzoli, R.; Bizzaro, N. Can supplementation with vitamin D reduce the risk or modify the course of autoimmune diseases? A systematic review of the literature. Autoimmun. Rev. 2012, 12, 127–136. [Google Scholar] [CrossRef] [PubMed]
- Maeshima, E.; Liang, X.-M.; Goda, M.; Otani, H.; Mune, M. The efficacy of vitamin E against oxidative damage and autoantibody production in systemic lupus erythematosus: A preliminary study. Clin. Rheumatol. 2007, 26, 401–404. [Google Scholar] [CrossRef]
- Leiter, L.M.; Reuhl, K.R.; Racis Jr, S.P.; Sherman, A.R. Iron status alters murine systemic lupus erythematosus. J. Nutr. 1995, 125, 474–484. [Google Scholar]
- O’Dell, J.R.; McGivern, J.P.; Kay, H.; Klassen, L.W. Improved survival in murine lupus as the result of selenium supplementation. Clin. Exp. Immunol. 1988, 73, 322. [Google Scholar]
- Soni, C.; Sinha, I.; Fasnacht, M.J.; Olsen, N.J.; Rahman, Z.S.; Sinha, R. Selenium supplementation suppresses immunological and serological features of lupus in B6. Sle1b mice. Autoimmunity 2019, 52, 57–68. [Google Scholar] [CrossRef]
- D’Cunha, N.M.; Peterson, G.; Baby, K.; Thomas, J. Impetigo: A need for new therapies in a world of increasing antimicrobial resistance. J. Clin. Pharm. Ther. 2017, 43, 150–153. [Google Scholar] [CrossRef]
- Corson, T.W.; Crews, C.M. Molecular understanding and modern application of traditional medicines: Triumphs and trials. Cell 2007, 130, 769–774. [Google Scholar] [CrossRef]
- Garcia, L.C. A Review of Artemisia annua L.: Its genetics, biochemical characteristics, and anti-malarial efficacy. Int. J. Sci. Technol. 2015, 5, 38–46. [Google Scholar]
- Krishna, S.; Bustamante, L.; Haynes, R.K.; Staines, H.M. Artemisinins: Their growing importance in medicine. Trends Pharmacol. Sci. 2008, 29, 520–527. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Xu, T.; Qiu, X.; Tian, B.; Bi, C.; Yao, L. Effectiveness of Bailing capsules in the treatment of lupus nephritis: A meta-analysis. Mol. Med. Rep. 2020, 22, 2132–2140. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Fortin, P.; Li, Y.; Panaritis, T.; Gans, M.; Esdaile, J. Discontinuation of antimalarial drugs in systemic lupus erythematosus. J. Rheumatol. 1999, 26, 808–815. [Google Scholar] [PubMed]
- Mu, X.; Wang, C. Artemisinins—A promising new treatment for systemic lupus erythematosus: A descriptive review. Curr. Rheumatol. Rep. 2018, 20, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Golenser, J.; Waknine, J.H.; Krugliak, M.; Hunt, N.H.; Grau, G.E. Current perspectives on the mechanism of action of artemisinins. Int. J. Parasitol. 2006, 36, 1427–1441. [Google Scholar] [CrossRef] [PubMed]
- Efferth, T.; Oesch, F. The immunosuppressive activity of artemisinin-type drugs towards inflammatory and autoimmune diseases. Med. Res. Rev. 2021, 41, 3023–3061. [Google Scholar] [CrossRef] [PubMed]
- Dang, W.-Z.; Li, H.; Jiang, B.; Nandakumar, K.S.; Liu, K.-F.; Liu, L.-X.; Yu, X.-C.; Tan, H.-J.; Zhou, C. Therapeutic effects of artesunate on lupus-prone MRL/lpr mice are dependent on T follicular helper cell differentiation and activation of JAK2–STAT3 signaling pathway. Phytomedicine 2019, 62, 152965. [Google Scholar] [CrossRef]
- Li, D.; Qi, J.; Wang, J.; Pan, Y.; Li, J.; Xia, X.; Dou, H.; Hou, Y. Protective effect of dihydroartemisinin in inhibiting senescence of myeloid-derived suppressor cells from lupus mice via Nrf2/HO-1 pathway. Free Radic. Biol. Med. 2019, 143, 260–274. [Google Scholar] [CrossRef]
- Efferth, T.; Kaina, B. Toxicity of the antimalarial artemisinin and its dervatives. Crit. Rev. Toxicol. 2010, 40, 405–421. [Google Scholar] [CrossRef]
- Yin, J.; Wang, H.; Ding, R. Artemisinin and its derivatives: Progress in toxicology. Chin. J. Pharmacol. Toxicol. 2014, 6, 309–314. [Google Scholar]
- Lee, W.-T.; Lee, T.-H.; Cheng, C.-H.; Chen, K.-C.; Chen, Y.-C.; Lin, C.-W. Antroquinonol from Antrodia Camphorata suppresses breast tumor migration/invasion through inhibiting ERK-AP-1-and AKT-NF-κB-dependent MMP-9 and epithelial-mesenchymal transition expressions. Food Chem. Toxicol. 2015, 78, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Tsai, P.-Y.; Ka, S.-M.; Chao, T.-K.; Chang, J.-M.; Lin, S.-H.; Li, C.-Y.; Kuo, M.-T.; Chen, P.; Chen, A. Antroquinonol reduces oxidative stress by enhancing the Nrf2 signaling pathway and inhibits inflammation and sclerosis in focal segmental glomerulosclerosis mice. Free Radic. Biol. Med. 2011, 50, 1503–1516. [Google Scholar] [CrossRef] [PubMed]
- Geethangili, M.; Tzeng, Y.-M. Review of pharmacological effects of Antrodia camphorata and its bioactive compounds. Evid.-Based Complement. Altern. Med. 2011, 2011, 212641. [Google Scholar] [CrossRef]
- Zhang, B.-B.; Hu, P.-F.; Huang, J.; Hu, Y.-D.; Chen, L.; Xu, G.-R. Current advances on the structure, bioactivity, synthesis, and metabolic regulation of novel ubiquinone derivatives in the edible and medicinal mushroom Antrodia cinnamomea. J. Agric. Food Chem. 2017, 65, 10395–10405. [Google Scholar] [CrossRef]
- Villaume, M.T.; Sella, E.; Saul, G.; Borzilleri, R.M.; Fargnoli, J.; Johnston, K.A.; Zhang, H.; Fereshteh, M.P.; Dhar, T.M.; Baran, P.S. Antroquinonol a: Scalable synthesis and preclinical biology of a phase 2 drug candidate. ACS Cent. Sci. 2016, 2, 27–31. [Google Scholar] [CrossRef]
- Angamuthu, V.; Shanmugavadivu, M.; Nagarajan, G.; Velmurugan, B.K. Pharmacological activities of antroquinonol-Mini review. Chem.-Biol. Interact. 2019, 297, 8–15. [Google Scholar] [CrossRef]
- Kuang, Y.; Li, B.; Wang, Z.; Qiao, X.; Ye, M. Terpenoids from the medicinal mushroom Antrodia camphorata: Chemistry and medicinal potential. Nat. Prod. Rep. 2021, 38, 83–102. [Google Scholar] [CrossRef]
- Huang, C.-Y.; Ju, D.-T.; Chang, C.-F.; Reddy, P.M.; Velmurugan, B.K. A review on the effects of current chemotherapy drugs and natural agents in treating non–small cell lung cancer. Biomedicine 2017, 7, 23. [Google Scholar] [CrossRef]
- Chang, W.-H.; Chen, M.C.; Cheng, I.H. Antroquinonol lowers brain amyloid-β levels and improves spatial learning and memory in a transgenic mouse model of Alzheimer’s disease. Sci. Rep. 2015, 5, 15067. [Google Scholar] [CrossRef]
- Chae, B.S. Effect of Baicalin on the Ex vivo Production of Cytokines in Pristane-Induced Lupus Mice. YAKHAK HOEJI 2016, 60, 21–28. [Google Scholar] [CrossRef]
- Delerue, T.; Barroso, M.F.; Dias-Teixeira, M.; Figueiredo-González, M.; Delerue-Matos, C.; Grosso, C. Interactions between Ginkgo biloba L. and Scutellaria baicalensis Georgi in multicomponent mixtures towards cholinesterase inhibition and ROS scavenging. Food Res. Int. 2021, 140, 109857. [Google Scholar] [CrossRef] [PubMed]
- Cai, Y.; Ma, W.; Xiao, Y.; Wu, B.; Li, X.; Liu, F.; Qiu, J.; Zhang, G. High doses of baicalin induces kidney injury and fibrosis through regulating TGF-β/Smad signaling pathway. Toxicol. Appl. Pharmacol. 2017, 333, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.; Liu, Y.; Zhang, C. Pharmacokinetics and bioavailability enhancement of baicalin: A review. Eur. J. Drug Metab. Pharmacokinet. 2019, 44, 159–168. [Google Scholar] [CrossRef] [PubMed]
- Salehi, B.; Stojanović-Radić, Z.; Matejić, J.; Sharifi-Rad, M.; Anil Kumar, N.V.; Martins, N.; Sharifi-Rad, J. The therapeutic potential of curcumin: A review of clinical trials. Eur. J. Med. Chem. 2019, 163, 527–545. [Google Scholar] [CrossRef] [PubMed]
- Constantin, M.M.; Nita, I.E.; Olteanu, R.; Constantin, T.; Bucur, S.; Matei, C.; Raducan, A. Significance and impact of dietary factors on systemic lupus erythematosus pathogenesis. Exp. Ther. Med. 2019, 17, 1085–1090. [Google Scholar] [CrossRef]
- Kumar, A.; Dogra, S.; Prakash, A. Protective effect of curcumin (Curcuma longa), against aluminium toxicity: Possible behavioral and biochemical alterations in rats. Behav. Brain Res. 2009, 205, 384–390. [Google Scholar] [CrossRef]
- Rezaee, R.; Momtazi, A.A.; Monemi, A.; Sahebkar, A. Curcumin: A potentially powerful tool to reverse cisplatin-induced toxicity. Pharmacol. Res. 2017, 117, 218–227. [Google Scholar] [CrossRef]
- Soetikno, V.; Sari, F.R.; Veeraveedu, P.T.; Thandavarayan, R.A.; Harima, M.; Sukumaran, V.; Lakshmanan, A.P.; Suzuki, K.; Kawachi, H.; Watanabe, K. Curcumin ameliorates macrophage infiltration by inhibiting NF-κB activation and proinflammatory cytokines in streptozotocin induced-diabetic nephropathy. Nutr. Metab. 2011, 8, 1–11. [Google Scholar] [CrossRef]
- Shishodia, S.; Sethi, G.; Aggarwal, B.B. Curcumin: Getting back to the roots. Ann. N. Y. Acad. Sci. 2005, 1056, 206–217. [Google Scholar] [CrossRef]
- Shishodia, S.; Singh, T.; Chaturvedi, M.M. Modulation of transcription factors by curcumin. Mol. Targets Ther. Uses Curcumin Health Dis. 2007, 595, 127–148. [Google Scholar]
- Gonzales, A.M.; Orlando, R.A. Curcumin and resveratrol inhibit nuclear factor-kappaB-mediated cytokine expression in adipocytes. Nutr. Metab. 2008, 5, 17. [Google Scholar] [CrossRef] [PubMed]
- JIANG, C.-X. Curcumin analog exhibited anti-inflammatory activity through inhibiting ERK/JNK and NF-κB signaling pathway. Chin. Tradit. Herb. Drugs 2016, 24, 2871–2876. [Google Scholar]
- Han, S.-S.; Keum, Y.-S.; Seo, H.-J.; Surh, Y.-J. Curcumin suppresses activation of NF-κB and AP-1 induced by phorbol ester in cultured human promyelocytic leukemia cells. BMB Rep. 2002, 35, 337–342. [Google Scholar] [CrossRef]
- Kocaadam, B.; Şanlier, N. Curcumin, an active component of turmeric (Curcuma longa), and its effects on health. Crit. Rev. Food Sci. Nutr. 2017, 57, 2889–2895. [Google Scholar] [CrossRef] [PubMed]
- Lao, C.D.; Ruffin, M.T.; Normolle, D.; Heath, D.D.; Murray, S.I.; Bailey, J.M.; Boggs, M.E.; Crowell, J.; Rock, C.L.; Brenner, D.E. Dose escalation of a curcuminoid formulation. BMC Complement. Altern. Med. 2006, 6, 1–4. [Google Scholar] [CrossRef]
- Sharma, R.A.; Euden, S.A.; Platton, S.L.; Cooke, D.N.; Shafayat, A.; Hewitt, H.R.; Marczylo, T.H.; Morgan, B.; Hemingway, D.; Plummer, S.M. Phase I clinical trial of oral curcumin: Biomarkers of systemic activity and compliance. Clin. Cancer Res. 2004, 10, 6847–6854. [Google Scholar] [CrossRef]
- Srinivas, G.; Babykutty, S.; Sathiadevan, P.P.; Srinivas, P. Molecular mechanism of emodin action: Transition from laxative ingredient to an antitumor agent. Med. Res. Rev. 2007, 27, 591–608. [Google Scholar] [CrossRef]
- Zhang, B.; Shi, Y.; Lei, T.C. Detection of active P-glycoprotein in systemic lupus erythematosus patients with poor disease control. Exp. Ther. Med. 2012, 4, 705–710. [Google Scholar] [CrossRef]
- Sharifi-Rad, J.; Herrera-Bravo, J.; Kamiloglu, S.; Petroni, K.; Mishra, A.P.; Monserrat-Mesquida, M.; Sureda, A.; Martorell, M.; Aidarbekovna, D.S.; Yessimsiitova, Z. Recent advances in the therapeutic potential of emodin for human health. Biomed. Pharmacother. 2022, 154, 113555. [Google Scholar] [CrossRef]
- Akkol, E.K.; Tatlı, I.I.; Karatoprak, G.Ş.; Ağar, O.T.; Yücel, Ç.; Sobarzo-Sánchez, E.; Capasso, R. Is emodin with anticancer effects completely innocent? Two sides of the coin. Cancers 2021, 13, 2733. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Sheng, L.; Chen, Y.; Li, Z.; Wu, H.; Ma, J.; Zhang, D.; Chen, X.; Zhang, S. Total coumarin derivates from Hydrangea paniculata attenuate renal injuries in cationized-BSA induced membranous nephropathy by inhibiting complement activation and interleukin 10-mediated interstitial fibrosis. Phytomedicine 2022, 96, 153886. [Google Scholar] [CrossRef]
- Tubaro, A.; Del Negro, P.; Ragazzi, E.; Zampiron, S.; Della Loggia, R. Anti-inflammatory and peripheral analgesic activity of esculetin in vivo. Pharmacol. Res. Commun. 1988, 20, 83–85. [Google Scholar] [CrossRef] [PubMed]
- Lum, P.T.; Sekar, M.; Gan, S.H.; Jeyabalan, S.; Bonam, S.R.; Rani, N.N.I.M.; Ku-Mahdzir, K.-M.; Seow, L.J.; Wu, Y.S.; Subramaniyan, V. Therapeutic potential of mangiferin against kidney disorders and its mechanism of action: A review. Saudi J. Biol. Sci. 2022, 29, 1530–1542. [Google Scholar] [CrossRef] [PubMed]
- Jangra, A.; Arora, M.K.; Kisku, A.; Sharma, S. The multifaceted role of mangiferin in health and diseases: A review. Adv. Tradit. Med. 2021, 21, 619–643. [Google Scholar] [CrossRef]
- Morozkina, S.N.; Nhung Vu, T.H.; Generalova, Y.E.; Snetkov, P.P.; Uspenskaya, M.V. Mangiferin as new potential anti-cancer agent and mangiferin-integrated polymer systems—A novel research direction. Biomolecules 2021, 11, 79. [Google Scholar] [CrossRef]
- Mei, S.; Ma, H.; Chen, X. Anticancer and anti-inflammatory properties of mangiferin: A review of its molecular mechanisms. Food Chem. Toxicol. 2021, 149, 111997. [Google Scholar] [CrossRef]
- Reddeman, R.A.; Glávits, R.; Endres, J.R.; Clewell, A.E.; Hirka, G.; Vértesi, A.; Béres, E.; Szakonyiné, I.P. A toxicological evaluation of mango leaf extract (Mangifera indica) containing 60% mangiferin. J. Toxicol. 2019, 2019, 4763015. [Google Scholar] [CrossRef] [PubMed]
- Hamidpour, M.; Hamidpour, R.; Hamidpour, S.; Shahlari, M. Chemistry, pharmacology, and medicinal property of sage (Salvia) to prevent and cure illnesses such as obesity, diabetes, depression, dementia, lupus, autism, heart disease, and cancer. J. Tradit. Complement. Med. 2014, 4, 82–88. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.-Y.; Song, Z.-Y.; Gan, H.-L.; Zheng, M.-H.; Liu, Q.; Meng, X.-T.; Pan, T.; Li, Z.-Y.; Peng, R.-X.; Liu, K. Non-clinical safety evaluation of salvianolic acid A: Acute, 4-week intravenous toxicities and genotoxicity evaluations. BMC Pharmacol. Toxicol. 2022, 23, 83. [Google Scholar] [CrossRef]
- Du, G.; Song, J.; Du, L.; Zhang, L.; Qiang, G.; Wang, S.; Yang, X.; Fang, L. Chemical and pharmacological research on the polyphenol acids isolated from Danshen: A review of salvianolic acids. Adv. Pharmacol. 2020, 87, 1–41. [Google Scholar] [PubMed]
- Wang, Q.; Meng, J.; Dong, A.; Yu, J.-z.; Zhang, G.-X.; Ma, C.-G. The pharmacological effects and mechanism of Tripterygium wilfordii Hook F in central nervous system autoimmunity. J. Altern. Complement. Med. 2016, 22, 496–502. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Z.-L.; Yang, Y.-X.; Ding, J.; Li, Y.-C.; Miao, Z.-H. Triptolide: Structural modifications, structure–activity relationships, bioactivities, clinical development and mechanisms. Nat. Prod. Rep. 2012, 29, 457–475. [Google Scholar] [CrossRef] [PubMed]
- Crews, G.; Erickson, L.; Pan, F.; Fisniku, O.; Jang, M.-S.; Wynn, C.; Benediktsson, H.; Kobayashi, M.; Jiang, H. Down-regulation of TGF-β and VCAM-1 is associated with successful treatment of chronic rejection in rats. Transplant. Proc. 2005, 1926–1928. [Google Scholar] [CrossRef]
- Hong, Y.; Zhou, W.; Li, K.; Sacks, S.H. Triptolide is a potent suppressant of C3, CD40 and B7h expression in activated human proximal tubular epithelial cells. Kidney Int. 2002, 62, 1291–1300. [Google Scholar] [CrossRef]
- Zhou, Y.; Hong, Y.; Huang, H. Triptolide attenuates inflammatory response in membranous glomerulo-nephritis rat via downregulation of NF-κB signaling pathway. Kidney Blood Press. Res. 2016, 41, 901–910. [Google Scholar] [CrossRef]
- Li, Y.; Yu, C.; Zhu, W.-M.; Xie, Y.; Qi, X.; Li, N.; Li, J.-S. Triptolide ameliorates IL-10-deficient mice colitis by mechanisms involving suppression of IL-6/STAT3 signaling pathway and down-regulation of IL-17. Mol. Immunol. 2010, 47, 2467–2474. [Google Scholar] [CrossRef]
- Qi, Q.; Li, H.; Lin, Z.-M.; Yang, X.-Q.; Zhu, F.-H.; Liu, Y.-T.; Shao, M.-J.; Zhang, L.-Y.; Xu, Y.-S.; Yan, Y.-X. (5 R)-5-hydroxytriptolide ameliorates anti-glomerular basement membrane glomerulonephritis in NZW mice by regulating Fcγ receptor signaling. Acta Pharmacol. Sin. 2018, 39, 107–116. [Google Scholar] [CrossRef]
- Fan, D.; Guo, Q.; Shen, J.; Zheng, K.; Lu, C.; Zhang, G.; Lu, A.; He, X. The effect of triptolide in rheumatoid arthritis: From basic research towards clinical translation. Int. J. Mol. Sci. 2018, 19, 376. [Google Scholar] [CrossRef]
- Xi, C.; Peng, S.; Wu, Z.; Zhou, Q.; Zhou, J. Toxicity of triptolide and the molecular mechanisms involved. Biomed. Pharmacother. 2017, 90, 531–541. [Google Scholar] [CrossRef]
- Zhao, M.; Liang, G.-P.; Tang, M.-N.; Luo, S.-Y.; Zhang, J.; Cheng, W.-J.; Chan, T.-M.; Lu, Q.-J. Total glucosides of paeony induces regulatory CD4+ CD25+ T cells by increasing Foxp3 demethylation in lupus CD4+ T cells. Clin. Immunol. 2012, 143, 180–187. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Wei, W. Anti-inflammatory and immunoregulatory effects of paeoniflorin and total glucosides of paeony. Pharmacol. Ther. 2020, 207, 107452. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Wang, L.; Cao, Y.; Li, N. Total glucosides of Paeonia lactiflora for safely reducing disease activity in systemic lupus erythematosus: A systematic review and meta-analysis. Front. Pharmacol. 2022, 13, 834947. [Google Scholar] [CrossRef] [PubMed]
- Jun, L.; Junshan, L.; Aiwu, Z.; Minzhu, C.; Shuyun, X. Modulatory effects of total glucosides of paeony on B lymphocyte proliferation and interleukin 1 production. Chin. J. Pharmacol. Toxicol. 1994, 8, 53–55. [Google Scholar]
- Wang, X.W.; Chen, M.Z.; Xu, S.Y. The effects of total glucosides of paeony (TGP) on T lymphocyte subsets. Chin. Pharmacol. Bull. 1992, 8, 340–343. [Google Scholar]
- Wang, X.; Cheng, M.; Xu, S. Effects of total glucosides of paeony on immune system. Zhongguo Bing Li Sheng Li Za Zhi 1991, 7, 609–611. [Google Scholar]
- Wang, X.; Chen, M.; Xu, S. The effects of total glucosides’ of paeony (TGP) on T lymphocyte subsets. Zhongguo Yao Li Xue Tong Bao 1992, 8, 340–343. [Google Scholar]
- Li, M.; Li, Y.; Xiang, L.; Li, L. Efficacy and safety of total glucosides of paeony as an add-on treatment in adolescents and adults with chronic urticaria: A systematic review and meta-analysis. Front. Pharmacol. 2022, 13, 961371. [Google Scholar] [CrossRef]
- Goh, E.; Tan, L.; Chow, S.; Teh, L.; Yeap, S. Use of complementary medicine in systemic lupus erythematosus patients in Malaysia. APLAR J. Rheumatol. 2003, 6, 21–25. [Google Scholar] [CrossRef]
- Hamedi, A.; Sohrabpour, M.; Zarshenas, M.M.; Pasdaran, A. Phytochemical investigation and quantitative analysis of the fatty acids and sterol compounds of seven pharmaceutical valuable seeds. Curr. Pharm. Anal. 2018, 14, 475–482. [Google Scholar] [CrossRef]
- Leiba, A.; Amital, H.; Gershwin, M.E.; Shoenfeld, Y. Diet and lupus. Lupus 2001, 10, 246–248. [Google Scholar] [CrossRef] [PubMed]
- Maki, P.A.; Newberne, P.M. Dietary lipids and immune function. J. Nutr. 1992, 122, 610–614. [Google Scholar] [CrossRef] [PubMed]
- Harbige, L.S. Fatty acids, the immune response, and autoimmunity: A question of n − 6 essentiality and the balance between n − 6 and n − 3. Lipids 2003, 38, 323–341. [Google Scholar] [CrossRef] [PubMed]
- Ramessar, N.; Borad, A.; Schlesinger, N. The effect of Omega-3 fatty acid supplementation in systemic lupus erythematosus patients: A systematic review. Lupus 2022, 31, 287–296. [Google Scholar] [CrossRef] [PubMed]
- Hejr, H.; Ghareghani, M.; Zibara, K.; Ghafari, M.; Sadri, F.; Salehpour, Z.; Hamedi, A.; Negintaji, K.; Azari, H.; Ghanbari, A. The ratio of 1/3 linoleic acid to alpha linolenic acid is optimal for oligodendrogenesis of embryonic neural stem cells. Neurosci. Lett. 2017, 651, 216–225. [Google Scholar] [CrossRef]
- Wei, Y.; Meng, Y.; Li, N.; Wang, Q.; Chen, L. The effects of low-ratio n-6/n-3 PUFA on biomarkers of inflammation: A systematic review and meta-analysis. Food Funct. 2021, 12, 30–40. [Google Scholar] [CrossRef]
- Borges, M.C.; Santos, F.d.M.M.; Telles, R.W.; Correia, M.I.T.D.; Lanna, C.C.D. Polyunsaturated omega-3 fatty acids and systemic lupus erythematosus: What do we know? Rev. Bras. Reumatol. 2014, 54, 459–466. [Google Scholar] [CrossRef]
- MacLean, C.H.; Mojica, W.A.; Morton, S.C.; Pencharz, J.; Garland, R.H.; Tu, W.; Newberry, S.J.; Jungvig, L.K.; Grossman, J.; Khanna, P. Effects of omega-3 fatty acids on lipids and glycemic control in type II diabetes and the metabolic syndrome and on inflammatory bowel disease, rheumatoid arthritis, renal disease, systemic lupus erythematosus, and osteoporosis: Summary. In AHRQ Evidence Report Summaries; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2004. [Google Scholar]
- Pestka, J.J. n-3 polyunsaturated fatty acids and autoimmune-mediated glomerulonephritis. Prostaglandins Leukot. Essent. Fat. Acids (PLEFA) 2010, 82, 251–258. [Google Scholar] [CrossRef]
- Fassett, R.G.; Gobe, G.C.; Peake, J.M.; Coombes, J.S. Omega-3 polyunsaturated fatty acids in the treatment of kidney disease. Am. J. Kidney Dis. 2010, 56, 728–742. [Google Scholar] [CrossRef]
- Tam, L.S.; Li, E.K.; Leung, V.Y.; Griffith, J.F.; Benzie, I.F.; Lim, P.L.; Whitney, B.; Lee, V.W.; Lee, K.K.; Thomas, G.N. Effects of vitamins C and E on oxidative stress markers and endothelial function in patients with systemic lupus erythematosus: A double blind, placebo controlled pilot study. J. Rheumatol. 2005, 32, 275–282. [Google Scholar]
- Kamen, D.L.; Cooper, G.S.; Bouali, H.; Shaftman, S.R.; Hollis, B.W.; Gilkeson, G.S. Vitamin D deficiency in systemic lupus erythematosus. Autoimmun. Rev. 2006, 5, 114–117. [Google Scholar] [CrossRef] [PubMed]
- Solovastru, L.G.; Vâta, D.; Statescu, L.; Constantin, M.M.; Andrese, E. Skin cancer between myth and reality, yet ethically constrained. Rev. Romana Bioet. 2014, 12, 47–52. [Google Scholar]
- Klack, K.; Bonfa, E.; Borba Neto, E.F. Diet and nutritional aspects in systemic lupus erythematosus. Rev. Bras. Reumatol. 2012, 52, 395–408. [Google Scholar] [CrossRef]
- Falcão, S.; Barros, R.; Mateus, M.; Nero, P.; De Matos, A.A.; Pimentão, J.B.; Ribeiro, I.; Weigert, A.; Branco, J. Lúpus eritematoso sistiémico e anemia. Acta Reumatol. Port. 2007, 32, 73–79. [Google Scholar]
- Sahebari, M.; Rezaieyazdi, Z.; Khodashahi, M. Selenium and autoimmune diseases: A review article. Curr. Rheumatol. Rev. 2019, 15, 123–134. [Google Scholar] [CrossRef] [PubMed]
- Brown, A.C. Lupus erythematosus and nutrition: A review of the literature. J. Ren. Nutr. 2000, 10, 170–183. [Google Scholar] [CrossRef] [PubMed]
- Selmi, C.; Tsuneyama, K. Nutrition, geoepidemiology, and autoimmunity. Autoimmun. Rev. 2010, 9, A267–A270. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.-X.; Sun, H.-X. Immunosuppressive effect of ethanol extract of Artemisia annua on specific antibody and cellular responses of mice against ovalbumin. Immunopharmacol. Immunotoxicol. 2009, 31, 625–630. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X. Effects of Astragalus membranaceus and Tripterygium hypoglancum on natural killer cell activity of peripheral blood mononuclear in systemic lupus erythematosus. Zhongguo Zhong Xi Yi Jie He Za Zhi Zhongguo Zhongxiyi Jiehe Zazhi = Chin. J. Integr. Tradit. West. Med. 1992, 12, 669–671, 645. [Google Scholar]
- Nurdiana; Dantara, T.W.I.; Syaban, M.F.R.; Mustafa, S.A.; Ikhsani, H.; Syafitri, F.E.; Hapsari, N.K.; Khoirunnisa, A. Efficacy and side effects studies of Bryophyllum pinnatum leaves ethanol extract in pristane-induced SLE BALB/c mice model. AIP Conf. Proc. 2019, 2108, 020016. [Google Scholar] [CrossRef]
- Dantara, T.W.I.; Syaban, M.F.R.; Mustafa, S.A.; Ikhsani, H.; Syafitri, F.E.; Hapsari, N.K.; Khoirunnisa, A. Effect of Bryophyllum pinnatum leaves Ethanol extract in TNF-α and TGF-β as candidate therapy of SLE in pristane-induced SLE BALB/c mice model. Res. J. Pharm. Technol. 2021, 14, 1069–1072. [Google Scholar]
- Handono, K.; Dantara, T.W.; Dewi, E.S.; Pratama, M.Z.; Nurdiana, N. Bryophyllum pinnatum leaves ethanol extract inhibit maturation and promote apoptosis of systemic lupus erythematosus BALB/c mice B cells. Med. J. Indones. 2017, 26, 253–260. [Google Scholar] [CrossRef]
- Indriyanti, N.; Garmana, A.N.; Setiawan, F. Repairing effects of aqueous extract of Kalanchoe pinnata (Lmk) Pers. on lupus nephritis mice. Pharmacogn. J. 2018, 10, 548–552. [Google Scholar] [CrossRef]
- Shamekhi, Z.; Amani, R.; Habibagahi, Z.; Namjoyan, F.; Ghadiri, A.; Saki Malehi, A. A Randomized, Double-blind, Placebo-controlled Clinical Trial Examining the Effects of Green Tea Extract on Systemic Lupus Erythematosus Disease Activity and Quality of Life. Phytother. Res. 2017, 31, 1063–1071. [Google Scholar] [CrossRef] [PubMed]
- Khajehdehi, P.; Zanjaninejad, B.; Aflaki, E.; Nazarinia, M.; Azad, F.; Malekmakan, L.; Dehghanzadeh, G.-R. Oral supplementation of turmeric decreases proteinuria, hematuria, and systolic blood pressure in patients suffering from relapsing or refractory lupus nephritis: A randomized and placebo-controlled study. J. Ren. Nutr. 2012, 22, 50–57. [Google Scholar] [CrossRef]
- Cai, Z.; Wong, C.K.; Dong, J.; Jiao, D.; Chu, M.; Leung, P.C.; San Lau, C.B.; Lau, C.P.; Tam, L.S.; Lam, C.W.K. Anti-inflammatory activities of Ganoderma lucidum (Lingzhi) and San-Miao-San supplements in MRL/lpr mice for the treatment of systemic lupus erythematosus. Chin. Med. 2016, 11, 23. [Google Scholar] [CrossRef] [PubMed]
- Lai, N.; Lin, R.; Lai, R.; Kun, U.; Leu, S. Prevention of autoantibody formation and prolonged survival in New Zealand Black/New Zealand White F1 mice with an ancient Chinese herb, Ganoderma tsugae. Lupus 2001, 10, 461–465. [Google Scholar] [CrossRef]
- Yuan, Z.; Feng, J. Observation on the treatment of systemic lupus erythematous with a Gentiana macrophylla complex tablet and a minimal dose of prednisone. Zhong Xi Yi Jie He Za Zhi = Chin. J. Mod. Dev. Tradit. Med. 1989, 9, 156–157, 133. [Google Scholar]
- Sheu, M.-J.; Chiu, C.-C.; Yang, D.-J.; Hsu, T.-C.; Tzang, B.-S. The root extract of Gentiana macrophylla Pall. alleviates B19-NS1-exacerbated liver injuries in NZB/W F1 mice. J. Med. Food 2017, 20, 56–64. [Google Scholar] [CrossRef]
- Clark, W.F.; Kortas, C.; Heidenheim, A.P.; Garland, J.; Spanner, E.; Parbtani, A. Flaxseed in lupus nephritis: A two-year nonplacebo-controlled crossover study. J. Am. Coll. Nutr. 2001, 20, 143–148. [Google Scholar] [CrossRef] [PubMed]
- Clark, W.F.; Parbtani, A.; Huff, M.W.; Spanner, E.; de Salis, H.; Chin-Yee, I.; Philbrick, D.J.; Holub, B.J. Flaxseed: A potential treatment for lupus nephritis. Kidney Int. 1995, 48, 475–480. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.-L.; Chen, Y.-C.; Yang, S.-H.; Ko, Y.-F.; Chen, S.-Y. Immunological alterations in lupus-prone autoimmune (NZB/NZW) F1 mice by mycelia Chinese medicinal fungus Cordyceps sinensis-induced redistributions of peripheral mononuclear T lymphocytes. Clin. Exp. Med. 2009, 9, 277–284. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.-R.; Yen, J.-H.; Lin, C.-C.; Tsai, W.-J.; Liu, W.-J.; Tsai, J.-J.; Lin, S.-F.; Liu, H.-W. The effects of Chinese herbs on improving survival and inhibiting anti-ds DNA antibody production in lupus mice. Am. J. Chin. Med. 1993, 21, 257–262. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Cao, L.; Wang, X.; Fan, Y. Radix Paeoniae Rubra Ameliorates Lupus Nephritis in Lupus-Like Symptoms of Mrl Mice by Reducing Intercellular Cell Adhesion Molecule-1, Vascular Cell Adhesion Molecule-1, and Platelet Endothelial Cell Adhesion Molecule-1 Expression. Comb. Chem. High Throughput Screen. 2020, 23, 675–683. [Google Scholar] [CrossRef] [PubMed]
- Yine, H.; Dai, S.; Wang, B.; Wei, Q. Effect of moutan cortex extract on Th17 cells of patients with systemic lupus erythematosus. Chin. J. Biochem. Pharm. 2015, 6, 119–121. [Google Scholar]
- Ming, L.; Jingjing, M.; Zhao, X.; Zhu, Y. Clinical study of Radix Astragali, Radix Rehmanniae combined with glucocorticoid in treating systemic lupus erythematosus. Int. J. Tradit. Chin. Med. 2012, 34, 203–206. [Google Scholar]
- Chae, B.-S.; Yang, J.-H. Regulatory effect of fresh rehmanniae radix extract on the in vitro production of proinflammatory cytokines in pristane-induced lupus mice. Nat. Prod. Sci. 2007, 13, 322–327. [Google Scholar]
- Shin, T.-Y.; Oh, C.-H.; Kim, D.-K.; Eun, J.-S.; Jeon, H.; Park, J.-S.; Kim, M.-S.; Yang, J.-H.; Chae, B.-S. Regulatory effect of Scutellariae radix on the proinflammatory cytokine production and abnormal T-cell activation in vitro in pristane-induced lupus mice. Nat. Prod. Sci. 2007, 13, 207–213. [Google Scholar]
- Wang, B.; Yuan, Z. A tablet of Tripterygium wilfordii in treating lupus erythematosus. Zhong Xi Yi Jie He Za Zhi = Chin. J. Mod. Dev. Tradit. Med. 1989, 9, 407–408, 389. [Google Scholar]
- Qin, W.Z.; Zhu, G.D.; Yang, S.M.; Han, K.Y.; Wang, J. Clinical observations on Tripterygium wilfordii in the treatment of 26 cases of discoid lupus erythematosus. J. Trad. Chin. Med. 1983, 3, 131–132. [Google Scholar]
- Treasure, J. Urtica semen reduces serum creatinine levels. J. Am. Herb. Guild 2003, 4, 22–25. [Google Scholar]
- Musette, P.; Galelli, A.; Chabre, H.; Callard, P.; Peumans, W.; Truffa-Bachi, P.; Kourilsky, P.; Gachelin, G. Urtica dioica agglutinin, a Vβ8. 3-specific superantigen, prevents the development of the systemic lupus erythematosus-like pathology of MRL lpr/lpr mice. Eur. J. Immunol. 1996, 26, 1707–1711. [Google Scholar] [CrossRef]
- Tao, X.; Davis, L.S.; Lipsky, P.E. Effect of an extract of the Chinese herbal remedy Tripterygium wilfordii Hook F on human immune responsiveness. Arthritis Rheum. Off. J. Am. Coll. Rheumatol. 1991, 34, 1274–1281. [Google Scholar] [CrossRef] [PubMed]
- Tao, X.; Lipsky, P.E. The Chinese anti-inflammatory and immunosuppressive herbal remedy Tripterygium wilfordii Hook F. Rheum. Dis. Clin. North Am. 2000, 26, 29–50. [Google Scholar] [CrossRef] [PubMed]
- Setty, A.R.; Sigal, L.H. Herbal medications commonly used in the practice of rheumatology: Mechanisms of action, efficacy, and side effects. Semin. Arthritis Rheum. 2005, 773–784. [Google Scholar] [CrossRef] [PubMed]
- Li, X.-Y. Anti-inflammatory and immunosuppressive components of Tripterygium wilfordii Hook F. Int. J. Immunother. 1993, 9, 181–187. [Google Scholar]
- Takaishi, Y.; Shishido, K.; Wariishi, N.; Shibuya, M.; Goto, K.; Kido, M.; Taka, M.; Ono, Y. Triptoquinone A and B novel interleukin-1 inhibitors from Tripterygium wilfordii var Regeli. Tetrahedron Lett. 1992, 33, 7177–7180. [Google Scholar] [CrossRef]
- Juling, G.; Shixiang, Y.; Xichun, W.; Shixi, X.; Deda, L. Tripterygium wilfordii Hook, f. in rheumatoid arthritis and ankylosing spondylitis. Zhonghua Yixue Zazhi 1981, 94, 405–412. [Google Scholar]
- Wong, K.-F.; Yuan, Y.; Luk, J.M. Tripterygium wilfordii bioactive compounds as anticancer and anti-inflammatory agents. Clin. Exp. Pharmacol. Physiol. 2012, 39, 311–320. [Google Scholar] [CrossRef]
- Qin, W.; Wanzhang, Q.; Chenghuang, L.; Shumei, Y.; Guangdou, Z. Tripterygium wilfordii Hook F in systemic lupus erythematosus: Report of 103 cases. Chin. Med. J. 1981, 94, 827–834. [Google Scholar]
- Xu, G.; Tu, W.; Jiang, D.; Xu, C. Tripterygium wilfordii Hook F treatment for idiopathic refractory nephrotic syndrome in adults: A meta-analysis. Nephron Clin. Pract. 2009, 111, c223–c228. [Google Scholar] [CrossRef] [PubMed]
- Ge, Y.; Xie, H.; Li, S.; Jin, B.; Hou, J.; Zhang, H.; Shi, M.; Liu, Z. Treatment of diabetic nephropathy with Tripterygium wilfordii Hook F extract: A prospective, randomized, controlled clinical trial. J. Transl. Med. 2013, 11, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Ji, S.-M.; Wang, Q.-W.; Chen, J.-S.; Sha, G.-Z.; Liu, Z.-H.; Li, L.-S. Clinical trial of Tripterygium wilfordii Hook F. in human kidney transplantation in China. Transplant. Proc. 2006, 1274–1279. [Google Scholar] [CrossRef] [PubMed]
- Baral, B.; Shrestha, B.; da Silva, J.T. A review of Chinese Cordyceps with special reference to Nepal, focusing on conservation. Environ. Exp. Biol. 2015, 13, 61–73. [Google Scholar]
- Xu, J.; Huang, Y.; Chen, X.X.; Zheng, S.C.; Chen, P.; Mo, M.H. The mechanisms of pharmacological activities of Ophiocordyceps sinensis fungi. Phytother. Res. 2016, 30, 1572–1583. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Li, Q.-Z.; Li, L.-D.-J.; Zhou, X.-W. Immunostimulatory effects of the intracellular polysaccharides isolated from liquid culture of Ophiocordyceps sinensis (Ascomycetes) on RAW264.7 cells via the MAPK and PI3K/Akt signaling pathways. J. Ethnopharmacol. 2021, 275, 114130. [Google Scholar] [CrossRef] [PubMed]
- Qian, G.-M.; Pan, G.-F.; Guo, J.-Y. Anti-inflammatory and antinociceptive effects of cordymin, a peptide purified from the medicinal mushroom Cordyceps sinensis. Nat. Prod. Res. 2012, 26, 2358–2362. [Google Scholar] [CrossRef] [PubMed]
- Ng, T.B.; Wong, J.H.; Fang, E.F. Recent Research on Pharmacological Activities of the Medicinal Fungus Cordyceps sinensis. In Antitumor Potential and other Emerging Medicinal Properties of Natural Compounds; Fang, E.F., Ng, T.B., Eds.; Springer: Dordrecht, The Netherlands, 2013; pp. 303–314. [Google Scholar]
- Yang, M.-L.; Kuo, P.-C.; Hwang, T.-L.; Wu, T.-S. Anti-inflammatory principles from Cordyceps sinensis. J. Nat. Prod. 2011, 74, 1996–2000. [Google Scholar] [CrossRef]
- Tong, X.; Guo, J. High Throughput Identification of the Potential Antioxidant Peptides in Ophiocordyceps sinensis. Molecules 2022, 27, 438. [Google Scholar] [CrossRef]
- Xiang, F.; Lin, L.; Hu, M.; Qi, X. Therapeutic efficacy of a polysaccharide isolated from Cordyceps sinensis on hypertensive rats. Int. J. Biol. Macromol. 2016, 82, 308–314. [Google Scholar] [CrossRef]
- Ding, C.; Tian, P.; Xue, W.; Ding, X.; Yan, H.; Pan, X.; Feng, X.; Xiang, H.; Hou, J.; Tian, X. Efficacy of Cordyceps sinensis in long term treatment of renal transplant patients. Front. Biosci.-Elite 2011, 3, 301–307. [Google Scholar]
- Chen, B.; Sun, Y.; Luo, F.; Wang, C. Bioactive metabolites and potential mycotoxins produced by Cordyceps fungi: A review of safety. Toxins 2020, 12, 410. [Google Scholar] [CrossRef] [PubMed]
- Maczynska, I.; Millo, B.; Ratajczak-Stefańska, V.; Maleszka, R.; Szych, Z.; Kurpisz, M.; Giedrys-Kalemba, S. Proinflammatory cytokine (IL-1β, IL-6, IL-12, IL-18 and TNF-α) levels in sera of patients with subacute cutaneous lupus erythematosus (SCLE). Immunol. Lett. 2006, 102, 79–82. [Google Scholar] [CrossRef]
- Umare, V.; Pradhan, V.; Nadkar, M.; Rajadhyaksha, A.; Patwardhan, M.; Ghosh, K.K.; Nadkarni, A.H. Effect of proinflammatory cytokines (IL-6, TNF-α, and IL-1β) on clinical manifestations in Indian SLE patients. Mediat. Inflamm. 2014, 2014, 385297. [Google Scholar] [CrossRef] [PubMed]
- Bao, Y.X.; Wong, K.C.; Li, E.K.M.; Tam, S.L.; Leung, C.P.; Yin, B.Y.; Lam, C.W.K. Immunomodulatory effects of lingzhi and san-miao-san supplementation on patients with rheumatoid arthritis. Immunopharmacol. Immunotoxicol. 2006, 28, 197–200. [Google Scholar] [CrossRef]
- Pazzi, F.; Fraile-Fabero, R. Effects of Ganoderma Lucidum on Pain in Women with Fibromyalgia. Fibrom Open Access 2017, 2, 2. [Google Scholar]
- Tang, W.; Gao, Y.; Chen, G.; Gao, H.; Dai, X.; Ye, J.; Chan, E.; Huang, M.; Zhou, S. A randomized, double-blind and placebo-controlled study of a Ganoderma lucidum polysaccharide extract in neurasthenia. J. Med. Food 2005, 8, 53–58. [Google Scholar] [CrossRef]
- Zhong, L.; Yan, P.; Lam, W.C.; Yao, L.; Bian, Z. Coriolus versicolor and Ganoderma lucidum related natural products as an adjunct therapy for cancers: A systematic review and meta-analysis of randomized controlled trials. Front. Pharmacol. 2019, 10, 703. [Google Scholar] [CrossRef]
- Klupp, N.L.; Kiat, H.; Bensoussan, A.; Steiner, G.Z.; Chang, D.H. A double-blind, randomised, placebo-controlled trial of Ganoderma lucidum for the treatment of cardiovascular risk factors of metabolic syndrome. Sci. Rep. 2016, 6, 1–10. [Google Scholar] [CrossRef]
- Noguchi, M.; Kakuma, T.; Tomiyasu, K.; Yamada, A.; Itoh, K.; Konishi, F.; Kumamoto, S.; Shimizu, K.; Kondo, R.; Matsuoka, K. Randomized clinical trial of an ethanol extract of Ganoderma lucidum in men with lower urinary tract symptoms. Asian J. Androl. 2008, 10, 777–785. [Google Scholar] [CrossRef]
- Henao, S.L.D.; Urrego, S.A.; Cano, A.M.; Higuita, E.A. Randomized Clinical Trial for the Evaluation of Immune Modulation by Yogurt Enriched with β-Glucans from Lingzhi or Reishi Medicinal Mushroom, Ganoderma lucidum (Agaricomycetes), in Children from Medellin, Colombia. Int. J. Med. Mushrooms 2018, 20, 705–716. [Google Scholar] [CrossRef] [PubMed]
- Hamedi, A.; Rezaei, H.; Azarpira, N.; Jafarpour, M.; Ahmadi, F. Effects of Malva sylvestris and its isolated polysaccharide on experimental ulcerative colitis in rats. J. Evid.-Based Complement. Altern. Med. 2016, 21, 14–22. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.; Shen, M.; Song, Q.; Xie, J. Biological activities and pharmaceutical applications of polysaccharide from natural resources: A review. Carbohydr. Polym. 2018, 183, 91–101. [Google Scholar] [CrossRef] [PubMed]
- Lu, J.; He, R.; Sun, P.; Zhang, F.; Linhardt, R.J.; Zhang, A. Molecular mechanisms of bioactive polysaccharides from Ganoderma lucidum (Lingzhi), a review. Int. J. Biol. Macromol. 2020, 150, 765–774. [Google Scholar] [CrossRef]
- Ren, L.; Zhang, J.; Zhang, T. Immunomodulatory activities of polysaccharides from Ganoderma on immune effector cells. Food Chem. 2021, 340, 127933. [Google Scholar] [CrossRef] [PubMed]
- Koo, M.H.; Chae, H.-J.; Lee, J.H.; Suh, S.-S.; Youn, U.J. Antiinflammatory lanostane triterpenoids from Ganoderma lucidum. Nat. Prod. Res. 2021, 35, 4295–4302. [Google Scholar] [CrossRef]
- Liang, C.; Tian, D.; Liu, Y.; Li, H.; Zhu, J.; Li, M.; Xin, M.; Xia, J. Review of the molecular mechanisms of Ganoderma lucidum triterpenoids: Ganoderic acids A, C2, D, F, DM, X and Y. Eur. J. Med. Chem. 2019, 174, 130–141. [Google Scholar] [CrossRef] [PubMed]
- Sharma, C.; Bhardwaj, N.; Sharma, A.; Tuli, H.S.; Batra, P.; Beniwal, V.; Gupta, G.K.; Sharma, A.K. Bioactive metabolites of Ganoderma lucidum: Factors, mechanism and broad spectrum therapeutic potential. J. Herb. Med. 2019, 17, 100268. [Google Scholar] [CrossRef]
- Ahmad, M.F. Ganoderma lucidum: Persuasive biologically active constituents and their health endorsement. Biomed. Pharmacother. 2018, 107, 507–519. [Google Scholar] [CrossRef]
- Dewi, S.C.; Sargowo, D.; Widodo, M.A.; Wihastuti, T.A.; Heriansyah, T.; Hartanto, M.A.T.; Pambayun, I.D.A.; Bakhri, S.; A’ini, N.Q.; Sahudi, D.P. Ganoderma lucidum subchronic toxicity on the liver as anti-oxidant and anti-inflamatory agent for cardivascular disease. J. Hypertens. 2015, 33, e30. [Google Scholar] [CrossRef]
- Fattahi, S.; Golpour, M.; Akhavan Niaki, H. Urtica Dioica, An emerauld in the medical Kingdom. Int. Biol. Biomed. J. 2016, 2, 1–10. [Google Scholar]
- Yarnell, E.; Abascal, K. Lupus erythematosus and herbal medicine. Altern. Complement. Ther. 2008, 14, 9–12. [Google Scholar] [CrossRef]
- Francišković, M.; Gonzalez-Pérez, R.; Orčić, D.; Sanchez de Medina, F.; Martínez-Augustin, O.; Svirčev, E.; Simin, N.; Mimica-Dukić, N. Chemical Composition and Immuno-Modulatory Effects of Urtica dioica L. (Stinging Nettle) Extracts. Phytother. Res. 2017, 31, 1183–1191. [Google Scholar] [CrossRef] [PubMed]
- Akbay, P.; Basaran, A.A.; Undeger, U.; Basaran, N. In vitro immunomodulatory activity of flavonoid glycosides from Urtica dioica L. Phytother. Res. Int. J. Devoted Pharmacol. Toxicol. Eval. Nat. Prod. Deriv. 2003, 17, 34–37. [Google Scholar] [CrossRef] [PubMed]
- Semalty, M.; Adhikari, L.; Semwal, D.; Chauhan, A.; Mishra, A.; Kotiyal, R.; Semalty, A. A comprehensive review on phytochemistry and pharmacological effects of stinging nettle (Urtica dioica). Curr. Tradit. Med. 2017, 3, 156–167. [Google Scholar] [CrossRef]
- Grauso, L.; de Falco, B.; Lanzotti, V.; Motti, R. Stinging nettle, Urtica dioica L.: Botanical, phytochemical and pharmacological overview. Phytochem. Rev. 2020, 19, 1341–1377. [Google Scholar] [CrossRef]
- Taheri, Y.; Quispe, C.; Herrera-Bravo, J.; Sharifi-Rad, J.; Ezzat, S.M.; Merghany, R.M.; Shaheen, S.; Azmi, L.; Prakash Mishra, A.; Sener, B. Urtica dioica-derived phytochemicals for pharmacological and therapeutic applications. Evid.-Based Complement. Altern. Med. 2022, 2022, 4024331. [Google Scholar] [CrossRef]
- Showkat, Q.A.; Rather, J.A.; Jabeen, A.; Dar, B.; Makroo, H.A.; Majid, D. Bioactive components, physicochemical and starch characteristics of different parts of lotus (Nelumbo nucifera Gaertn.) plant: A review. Int. J. Food Sci. Technol. 2021, 56, 2205–2214. [Google Scholar] [CrossRef]
- Limwachiranon, J.; Huang, H.; Shi, Z.; Li, L.; Luo, Z. Lotus flavonoids and phenolic acids: Health promotion and safe consumption dosages. Compr. Rev. Food Sci. Food Saf. 2018, 17, 458–471. [Google Scholar] [CrossRef]
- Bishayee, A.; Patel, P.A.; Sharma, P.; Thoutireddy, S.; Das, N. Lotus (Nelumbo nucifera Gaertn.) and its bioactive phytocompounds: A tribute to cancer prevention and intervention. Cancers 2022, 14, 529. [Google Scholar] [CrossRef]
- Ekiert, H.; Świątkowska, J.; Klin, P.; Rzepiela, A.; Szopa, A. Artemisia annua–Importance in Traditional Medicine and Current State of Knowledge on the Chemistry, Biological Activity and Possible Applications. Planta Med. 2021, 87, 584–599. [Google Scholar] [CrossRef] [PubMed]
- Rolta, R.; Salaria, D.; Sharma, P.; Sharma, B.; Kumar, V.; Rathi, B.; Verma, M.; Sourirajan, A.; Baumler, D.J.; Dev, K. Phytocompounds of Rheum emodi, Thymus serpyllum, and Artemisia annua Inhibit Spike Protein of SARS-CoV-2 Binding to ACE2 Receptor: In Silico Approach. Curr. Pharmacol. Rep. 2021, 7, 135–149. [Google Scholar] [CrossRef]
- Law, S.; Leung, A.W.; Xu, C. Is the traditional Chinese herb “Artemisia annua” possible to fight against COVID-19? Integr. Med. Res. 2020, 9, 100474. [Google Scholar] [CrossRef]
- Fuzimoto, A.D. An overview of the anti-SARS-CoV-2 properties of Artemisia annua, its antiviral action, protein-associated mechanisms, and repurposing for COVID-19 treatment. J. Integr. Med. 2021, 19, 375–388. [Google Scholar] [CrossRef] [PubMed]
- Yang, L. 杨岚; Zhang, D. 张东. 双氢青蒿素及其红斑狼疮新适应症研究概述. 科学通报 2017, 62, 2007–2012. [Google Scholar]
- Willcox, M.; Bodeker, G.; Rasoanaivo, P.; Addae-Kyereme, J. Traditional Medicinal Plants and Malaria; CRC Press: Boca Raton, FL, USA, 2004; Volume 4. [Google Scholar]
- Ashok, P.K.; Upadhyaya, K. Preliminary Phytochemical Screening and Physico-Chemical Parameters of Artemisia absinthium and Artemisia annua. J. Pharmacogn. Phytochem. 2013, 1, 229–235. [Google Scholar]
- Zhuang, G. Clinical study on the treatment of lupus erythematosus with Artemisia apiacea Hce. Zhonghua Yi Xue Za Zhi 1982, 62, 365–367. [Google Scholar]
- Guokang, Z. Discoid Lupus Erythematosus Treated by Artemisia Annua. Altern. Complement. Ther. 2008, 14, 9–12. [Google Scholar]
- Jun, D.Y.; Dong, L.W.; You, T.Y.; Na, Z.H.; Zhong, Z.W.; Lan, Y.; Bin, L.Z. The effects of DQHS on the pathologic changes in BXSB mice lupus nephritis and the effect mechanism. Chin. Pharmacol. Bull. 2003, 19, 1125–1128. [Google Scholar]
- Dong, Y.; Li, W.; Tu, Y. Effect of dihydro-qinghaosu on auto-antibody production, TNF alpha secretion and pathologic change of lupus nephritis in BXSB mice. Zhongguo Zhong Xi Yi Jie He Za Zhi Zhongguo Zhongxiyi Jiehe Zazhi = Chin. J. Integr. Tradit. West. Med. 2003, 23, 676–679. [Google Scholar]
- Yang, J.; Wen, C.; Duan, Y.; Deng, Q.; Peng, D.; Zhang, H.; Ma, H. The composition, extraction, analysis, bioactivities, bioavailability and applications in food system of flaxseed (Linum usitatissimum L.) oil: A review. Trends Food Sci. Technol. 2021, 118, 252–260. [Google Scholar] [CrossRef]
- Akter, Y.; Junaid, M.; Afrose, S.S.; Nahrin, A.; Alam, M.S.; Sharmin, T.; Akter, R.; Hosen, S. A Comprehensive Review on Linum usitatissimum Medicinal Plant: Its Phytochemistry, Pharmacology, and Ethnomedicinal Uses. Mini Rev. Med. Chem. 2021, 21, 2801–2834. [Google Scholar] [CrossRef] [PubMed]
- Liang, S.; Li, X.; Ma, X.; Li, A.; Wang, Y.; Reaney, M.J.; Shim, Y.Y. A flaxseed heteropolysaccharide stimulates immune responses and inhibits hepatitis B virus. Int. J. Biol. Macromol. 2019, 136, 230–240. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, I.; Shalaby, A.; Abdallah, H.; El-Zohairy, N.; Bahr, H. Immunomodulatory and anti-angiogenic properties of Linum usitatissium (flaxseed) seeds ethanolic extract in atherogenic diet treated rats. Adv. Anim. Vet. Sci 2020, 8, 18–25. [Google Scholar] [CrossRef]
- Touré, A.; Xu, X. Flaxseed lignans: Source, biosynthesis, metabolism, antioxidant activity, bio-active components, and health benefits. Compr. Rev. Food Sci. Food Saf. 2010, 9, 261–269. [Google Scholar] [CrossRef]
- Yuan, B.; Han, J.; Cheng, Y.; Cheng, S.; Huang, D.; Mcclements, D.J.; Cao, C. Identification and characterization of antioxidant and immune-stimulatory polysaccharides in flaxseed hull. Food Chem. 2020, 315, 126266. [Google Scholar]
- Bashir, S.; Ali, S.; Khan, F. Partial reversal of obesity-induced insulin resistance owing to anti-inflammatory immunomodulatory potential of flaxseed oil. Immunol. Investig. 2015, 44, 451–469. [Google Scholar] [CrossRef]
- Chytilová, M.; Mudroňová, D.; Nemcová, R.; Gancarčíková, S.; Buleca, V.; Koščová, J.; Tkáčiková, Ľ. Anti-inflammatory and immunoregulatory effects of flax-seed oil and Lactobacillus plantarum—Biocenol™ LP96 in gnotobiotic pigs challenged with enterotoxigenic Escherichia coli. Res. Vet. Sci. 2013, 95, 103–109. [Google Scholar] [CrossRef]
- Herchi, W.; Harrabi, S.; Sebei, K.; Rochut, S.; Boukhchina, S.; Pepe, C.; Kallel, H. Phytosterols accumulation in the seeds of Linum usitatissimum L. Plant Physiol. Biochem. 2009, 47, 880–885. [Google Scholar] [CrossRef]
- Vilahur, G.; Ben-Aicha, S.; Diaz-Riera, E.; Badimon, L.; Padró, T. Phytosterols and inflammation. Curr. Med. Chem. 2019, 26, 6724–6734. [Google Scholar] [CrossRef]
- Hamedi, A.; Ghanbari, A.; Razavipour, R.; Saeidi, V.; Zarshenas, M.M.; Sohrabpour, M.; Azari, H. Alyssum homolocarpum seeds: Phytochemical analysis and effects of the seed oil on neural stem cell proliferation and differentiation. J. Nat. Med. 2015, 69, 387–396. [Google Scholar] [CrossRef] [PubMed]
- Ogborn, M.R.; Nitschmann, E.; Bankovic-Calic, N.; Weiler, H.A.; Aukema, H. Dietary flax oil reduces renal injury, oxidized LDL content, and tissue n− 6/n− 3 FA ratio in experimental polycystic kidney disease. Lipids 2002, 37, 1059–1065. [Google Scholar] [CrossRef] [PubMed]
- Naqshbandi, A.; Rizwan, S.; Khan, F. Dietary supplementation of flaxseed oil ameliorates the effect of cisplatin on rat kidney. J. Funct. Foods 2013, 5, 316–326. [Google Scholar] [CrossRef]
- Al Za’abi, M.; Ali, H.; Ali, B.H. Effect of flaxseed on systemic inflammation and oxidative stress in diabetic rats with or without chronic kidney disease. PLoS ONE 2021, 16, e0258800. [Google Scholar] [CrossRef]
- Ogborn, M.R. Flaxseed and flaxseed products in kidney disease. In Flaxseed in Human Nutrition; AOCS Press: Champaign, IL, USA, 2003; pp. 301–318. [Google Scholar]
- Parikh, M.; Maddaford, T.G.; Austria, J.A.; Aliani, M.; Netticadan, T.; Pierce, G.N. Dietary flaxseed as a strategy for improving human health. Nutrients 2019, 11, 1171. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.-H.; Yook, T.-H.; Kim, J.-U. Rehmanniae radix, an effective treatment for patients with various inflammatory and metabolic diseases: Results from a review of Korean publications. J. Pharmacopunct. 2017, 20, 81. [Google Scholar]
- Li, M.; Ma, J.-J.; Zhao, X.-L.; Zhu, Y. Treating lupus nephritis by a drug pair of radix astragali and rehmanniae radix combined with glucocorticoid: A preliminary clinical study. Zhongguo Zhong Xi Yi Jie He Za Zhi Zhongguo Zhongxiyi Jiehe Zazhi = Chin. J. Integr. Tradit. West. Med. 2014, 34, 956–959. [Google Scholar]
- Li, M.; Jiang, H.; Hao, Y.; Du, K.; Du, H.; Ma, C.; Tu, H.; He, Y. A systematic review on botany, processing, application, phytochemistry and pharmacological action of Radix Rehmnniae. J. Ethnopharmacol. 2022, 285, 114820. [Google Scholar] [CrossRef]
- Lu, M.-K.; Chang, C.-C.; Chao, C.-H.; Hsu, Y.-C. Structural changes, and anti-inflammatory, anti-cancer potential of polysaccharides from multiple processing of Rehmannia glutinosa. Int. J. Biol. Macromol. 2022, 206, 621–632. [Google Scholar] [CrossRef]
- Zhou, Y.; Wang, S.; Feng, W.; Zhang, Z.; Li, H. Structural characterization and immunomodulatory activities of two polysaccharides from Rehmanniae Radix Praeparata. Int. J. Biol. Macromol. 2021, 186, 385–395. [Google Scholar] [CrossRef]
- Choi, Y.H. Catalpol attenuates lipopolysaccharide-induced inflammatory responses in BV2 microglia through inhibiting the TLR4-mediated NF-κB pathway. Gen. Physiol. Biophys. 2019, 38, 111–122. [Google Scholar] [CrossRef] [PubMed]
- Chi, X.; Wang, S.; Baloch, Z.; Zhang, H.; Li, X.; Zhang, Z.; Zhang, H.; Dong, Z.; Lu, Y.; Yu, H. Research progress on classical traditional Chinese medicine formula Lily Bulb and Rehmannia Decoction in the treatment of depression. Biomed. Pharmacother. 2019, 112, 108616. [Google Scholar] [CrossRef] [PubMed]
- Song, W.-H.; Cheng, Z.-H.; Chen, D.-F. Anticomplement monoterpenoid glucosides from the root bark of Paeonia suffruticosa. J. Nat. Prod. 2014, 77, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.-J.; Li, Y.-X.; Li, S.; He, W.; Wang, Z.-R.; Zhan, T.-P.; Lv, C.-Y.; Liu, Y.-P.; Yang, Y.; Zeng, X.-X. Progress in traditional Chinese medicine and natural extracts for the treatment of lupus nephritis. Biomed. Pharmacother. 2022, 149, 112799. [Google Scholar] [CrossRef] [PubMed]
- Ekiert, H.; Klimek-Szczykutowicz, M.; Szopa, A. Paeonia × suffruticosa (Moutan Peony)—A review of the chemical composition, traditional and professional use in medicine, position in cosmetics industries, and biotechnological studies. Plants 2022, 11, 3379. [Google Scholar] [CrossRef] [PubMed]
- Tan, Y.-Q.; Chen, H.-W.; Li, J.; Wu, Q.-J. Efficacy, chemical constituents, and pharmacological actions of Radix Paeoniae rubra and Radix Paeoniae alba. Front. Pharmacol. 2020, 11, 1054. [Google Scholar] [CrossRef]
- Parker, S.; May, B.; Zhang, C.; Zhang, A.L.; Lu, C.; Xue, C.C. A pharmacological review of bioactive constituents of Paeonia lactiflora Pallas and Paeonia veitchii Lynch. Phytother. Res. 2016, 30, 1445–1473. [Google Scholar] [CrossRef]
- Pasdaran, A.; Butovska, D.; Kerr, P.; Naychov, Z.; Aneva, I.; Kozuharova, E. Gentians, natural remedies for future of visceral pain control; an ethnopharmacological review with an in silico approach. Biol. Futur. 2022, 73, 219–227. [Google Scholar] [CrossRef]
- Cui, Y.; Jiang, L.; Shao, Y.; Mei, L.; Tao, Y. Anti-alcohol liver disease effect of Gentianae macrophyllae extract through MAPK/JNK/p38 pathway. J. Pharm. Pharmacol. 2019, 71, 240–250. [Google Scholar] [CrossRef]
- Lohar, A.V.; Wankhade, A.M.; Faisal, M.; Jagtap, A. A review on Glycyrrhiza glabra linn (liquorice)—An excellent medicinal plant. Eur. J. Biomed. 2020, 7, 330–334. [Google Scholar]
- Pandey, S.; Verma, B.; Arya, P. A review on constituents, pharmacological activities and medicinal uses of Glycyrrhiza glabra. Pharm. Res. 2017, 2, 26–31. [Google Scholar] [CrossRef]
- Damle, M. Glycyrrhiza glabra (Liquorice)—A potent medicinal herb. Int. J. Herb. Med. 2014, 2, 132–136. [Google Scholar]
- Kwon, Y.-J.; Son, D.-H.; Chung, T.-H.; Lee, Y.-J. A review of the pharmacological efficacy and safety of licorice root from corroborative clinical trial findings. J. Med. Food 2020, 23, 12–20. [Google Scholar] [CrossRef] [PubMed]
- Yang, R.; Yuan, B.-C.; Ma, Y.-S.; Zhou, S.; Liu, Y. The anti-inflammatory activity of licorice, a widely used Chinese herb. Pharm. Biol. 2017, 55, 5–18. [Google Scholar] [CrossRef] [PubMed]
- Mollica, L.; De Marchis, F.; Spitaleri, A.; Dallacosta, C.; Pennacchini, D.; Zamai, M.; Agresti, A.; Trisciuoglio, L.; Musco, G.; Bianchi, M.E. Glycyrrhizin binds to high-mobility group box 1 protein and inhibits its cytokine activities. Chem. Biol. 2007, 14, 431–441. [Google Scholar] [CrossRef]
- Li, X.; Yue, Y.; Zhu, Y.; Xiong, S. Extracellular, but not intracellular HMGB1, facilitates self-DNA induced macrophage activation via promoting DNA accumulation in endosomes and contributes to the pathogenesis of lupus nephritis. Mol. Immunol. 2015, 65, 177–188. [Google Scholar] [CrossRef]
- Nazari, S.; Rameshrad, M.; Hosseinzadeh, H. Toxicological effects of Glycyrrhiza glabra (licorice): A review. Phytother. Res. 2017, 31, 1635–1650. [Google Scholar] [CrossRef] [PubMed]
- Wahab, S.; Ahmad, I.; Irfan, S.; Siddiqua, A.; Usmani, S.; Ahmad, M.P. Pharmacological Efficacy and Safety of Glycyrrhiza glabra in the treatment of respiratory tract infections. Mini Rev. Med. Chem. 2022, 22, 1476–1494. [Google Scholar] [CrossRef]
- Liu, T.; Qiao, X.; Kong, K.; Wang, X.; Li, R.; Zhang, X. Bioinformatics-based Identification of the Mechanism Whereby Astragalus Membranaceus Inhibits Inflammation and Autophagy in Lupus Nephritis. preprint 2021. [Google Scholar] [CrossRef]
- Sheik, A.; Kim, K.; Varaprasad, G.L.; Lee, H.; Kim, S.; Kim, E.; Shin, J.-Y.; Oh, S.Y.; Huh, Y.S. The anti-cancerous activity of adaptogenic herb Astragalus membranaceus. Phytomedicine 2021, 91, 153698. [Google Scholar] [CrossRef]
- Kamboj, A.; Saluja, A. Bryophyllum pinnatum (Lam.) Kurz.: Phytochemical and pharmacological profile: A review. Pharmacogn. Rev. 2009, 3, 364. [Google Scholar]
- Handono, K.; Dantara, T.; Dewi, E.; Pratama, M.; Nurdiana, N. 94 Development of therapy using bryophyllum pinnatum to decrease maturation and increase apoptotic b cells from balb/c lupus mice: In silico and in vitro study approach. Lupus Sci. Med. 2017, 4. [Google Scholar] [CrossRef]
- Kalsum, U.; Nurdiana, N.; Pratama, M.; Kalim, H.; Handono, K. 91 Potential novel natural b cell depleting and immunosuppression agent in lupus treapment using bryophyllum pinnatum. in silico and in pristane induced lupus mice. Lupus Sci. Med. 2017, 4. [Google Scholar] [CrossRef]
- Indriyanti, N.; Soeroso, J.; Khotib, J. T-cell activation controlling effects of ethyl acetate fraction of Kalanchoe pinnata (lmk) pers on tmpd-treated lupus mice. Int. J. Pharm. Sci. Res. 2018, 9, 475–482. [Google Scholar]
- Indriyanti, N.; Soeroso, J.; Khotib, J. The benefits of active compounds in Kalanchoe pinnata (LMK) pers ethyl acetate fraction on lupus arthritis mice. Asian J. Pharm. Clin. Res. 2017, 10, 1–5. [Google Scholar] [CrossRef]
- Indriyanti, N.; Soeroso, J.; Khotib, J. Positive Impact of Ethyl Acetate Fraction of Kalanchoe pinnata on Anti-Smith Antibody and T Reg in Lupus Mice. J. Ilmu Kefarmasian Indones. 2017, 15, 57–62. [Google Scholar]
- Indriyanti, N.; Garmana, A.N. Ekstrak Daun Cocor Bebek (Kalanchoe pinnata) Untuk Terapi Preventif Lupus pada Mencit yang Diinduksi dengan 2, 6, 10, 14 Tetramethylpentadecane. J. Trop. Pharm. Chem. 2011, 1, 221–226. [Google Scholar] [CrossRef]
- Fernandes, J.M.; Cunha, L.M.; Azevedo, E.P.; Lourenço, E.M.; Fernandes-Pedrosa, M.F.; Zucolotto, S.M. Kalanchoe laciniata and Bryophyllum pinnatum: An updated review about ethnopharmacology, phytochemistry, pharmacology and toxicology. Rev. Bras. Farmacogn. 2019, 29, 529–558. [Google Scholar] [CrossRef]
- Liu, T.; An, X.-N.; Liu, D.-L.; Wei, Y.-J. A comparison of several second-order algorithms for simultaneous determination of neomangiferin and mangiferin with severe spectral overlapping in Anemarrhenae Rhizoma. Spectrochim. Acta Part A Mol. Biomol. Spectrosc. 2019, 208, 172–178. [Google Scholar] [CrossRef]
- Singh, K.G.; Sonia, S.; Konsoor, N. In-vitro and ex-vivo studies on the antioxidant, anti-inflammatory and antiarthritic properties of Camellia sinensis, Hibiscus rosa sinensis, Matricaria chamomilla, Rosa SP., Zingiber officinale tea extracts. Inflammation 2018, 49, 50. [Google Scholar]
- Mawarti, H.; Nugraha, J.; Purwanto, D.A.; Soeroso, J. Identifying and Revealing Active Compound from Green Tea (Camellia sinensis) for Curing Systemic Lupus Erythematosus by Acting as CASPASE 1 Inhibitor. Med. -Leg. Update 2020, 20, 323–329. [Google Scholar]
- Bedrood, Z.; Rameshrad, M.; Hosseinzadeh, H. Toxicological effects of Camellia sinensis (green tea): A review. Phytother. Res. 2018, 32, 1163–1180. [Google Scholar] [CrossRef] [PubMed]
- Labban, L. Medicinal and pharmacological properties of Turmeric (Curcuma longa): A review. Int. J. Pharm. Biomed. Sci. 2014, 5, 17–23. [Google Scholar]
- Gurung, P.; De, P. Spectrum of biological properties of Cinchona alkaloids: A brief review. J. Pharmacogn. Phytochem. 2017, 6, 162–166. [Google Scholar]
- Kinsley-Scott, T.R.; Norton, S.A. Useful plants of dermatology. VII: Cinchona and antimalarials. J. Am. Acad. Dermatol. 2003, 49, 499–502. [Google Scholar] [CrossRef]
- Weng, J.-K. Plant solutions for the COVID-19 pandemic and beyond: Historical reflections and future perspectives. Mol. Plant 2020, 13, 803–807. [Google Scholar] [CrossRef]
- Shah, R.R. Chloroquine and hydroxychloroquine for COVID-19: Perspectives on their failure in repurposing. J. Clin. Pharm. Ther. 2021, 46, 17–27. [Google Scholar] [CrossRef]
- Wu, G.-C.; Wu, H.; Fan, L.-Y.; Pan, H.-F. Saikosaponins: A potential treatment option for systemic lupus erythematosus. Ir. J. Med. Sci. 2011, 180, 259–261. [Google Scholar] [CrossRef]
- Brinkhaus, B.; Lindner, M.; Schuppan, D.; Hahn, E. Chemical, pharmacological and clinical profile of the East Asian medical plant Centella aslatica. Phytomedicine 2000, 7, 427–448. [Google Scholar] [CrossRef]
- Kundu, P.; Sharma, P.; Mahato, R.; Saha, M.; Das, S.; Ghosh, P. A brief review for the development of bio-nanoparticles using some important Indian ethnomedicinal plants. J. Med. Plants 2020, 8, 26–33. [Google Scholar] [CrossRef]
- Islam, M. A Review on Tinospora cordifolia and its Immunomodulatory Activities. Ph.D. Thesis, Brac University, Dhaka, Bangladesh, 2020. [Google Scholar]
- Abrantes, V.E.F.; Matias da Rocha, B.A.; Batista da Nóbrega, R.; Silva-Filho, J.C.; Teixeira, C.S.; Cavada, B.S.; de Almeida Gadelha, C.A.; Ferreira, S.H.; Figueiredo, J.G.; Santi-Gadelha, T. Molecular modeling of Lectin-like protein from Acacia farnesiana reveals a possible anti-inflammatory mechanism in carrageenan-induced inflammation. BioMed Res. Int. 2013, 2013, 253483. [Google Scholar] [CrossRef]
- Delgadillo Puga, C.; Cuchillo Hilario, M.; Navarro Ocaña, A.; Medina Campos, O.N.; Nieto Camacho, A.; Ramírez Apan, T.; López Tecpoyotl, Z.G.; Díaz Martínez, M.; Álvarez Izazaga, M.A.; Cruz Martínez, Y.R. Phenolic Compounds in Organic and Aqueous Extracts from Acacia farnesiana Pods Analyzed by ULPS-ESI-Q-oa/TOF-MS. In Vitro Antioxidant Activity and Anti-Inflammatory Response in CD-1 Mice. Molecules 2018, 23, 2386. [Google Scholar]
- Leal, L.S.S.; Silva, R.O.; Araújo, T.d.S.L.; Silva, V.G.d.; Barbosa, A.L.d.R.; Medeiros, J.V.R.; Oliveira, J.S.; Ventura, C.A. The anti-inflammatory and antinociceptive effects of proteins extracted from Acacia farnesiana seeds. Rev. Bras. Plantas Med. 2016, 18, 38–47. [Google Scholar] [CrossRef]
- Almeida, É.S.; de Oliveira, D.; Hotza, D. Properties and applications of Morinda citrifolia (noni): A review. Compr. Rev. Food Sci. Food Saf. 2019, 18, 883–909. [Google Scholar] [CrossRef] [PubMed]
- Dixon, A.R.; McMillen, H.; Etkin, N.L. Ferment this: The transformation of Noni, a traditional Polynesian medicine (Morinda citrifolia, Rubiaceae). Econ. Bot. 1999, 53, 51–68. [Google Scholar] [CrossRef]
- McClatchey, W. From Polynesian healers to health food stores: Changing perspectives of Morinda citrifolia (Rubiaceae). Integr. Cancer Ther. 2002, 1, 110–120. [Google Scholar] [CrossRef]
- Dong, Y.; Feng, Z.-L.; Chen, H.-B.; Wang, F.-S.; Lu, J.-H. Corni Fructus: A review of chemical constituents and pharmacological activities. Chin. Med. 2018, 13, 1–20. [Google Scholar] [CrossRef]
- Sung, Y.-H.; Chang, H.-K.; Kim, S.-E.; Kim, Y.-M.; Seo, J.-H.; Shin, M.-C.; Shin, M.-S.; Yi, J.-W.; Shin, D.-H.; Kim, H. Anti-inflammatory and analgesic effects of the aqueous extract of corni fructus in murine RAW 264.7 macrophage cells. J. Med. Food 2009, 12, 788–795. [Google Scholar] [CrossRef]
- Park, C.H.; Tanaka, T.; Yokozawa, T. Anti-diabetic action of 7-O-galloyl-D-sedoheptulose, a polyphenol from Corni Fructus, through ameliorating inflammation and inflammation-related oxidative stress in the pancreas of type 2 diabetics. Biol. Pharm. Bull. 2013, 36, 723–732. [Google Scholar] [CrossRef]
- Tao, J.-H.; Zhao, M.; Jiang, S.; Pu, X.-L.; Wei, X.-Y. Comparative metabolism of two major compounds in Fructus Corni extracts by gut microflora from normal and chronic nephropathy rats in vitro by UPLC-Q-TOF/MS. J. Chromatogr. B 2018, 1073, 170–176. [Google Scholar] [CrossRef]
- Londhe, V.; Gavasane, A.; Nipate, S.; Bandawane, D.; Chaudhari, P. Role of garlic (Allium sativum) in various diseases: An overview. Angiogenesis 2011, 12, 13. [Google Scholar]
- Abdou, I.; Abou-Zeid, A.; El-Sherbeeny, M.; Abou-El-Gheat, Z. Antimicrobial activities of Allium sativum, Allium cepa, Raphanus sativus, Capsicum frutescens, Eruca sativa, Allium kurrat on bacteria. Qual. Plant. Mater. Veg. 1972, 22, 29–35. [Google Scholar] [CrossRef]
- Zou, Y.-T.; Zhou, J.; Wu, C.-Y.; Zhang, W.; Shen, H.; Xu, J.-D.; Zhang, Y.-Q.; Long, F.; Li, S.-L. Protective effects of Poria cocos and its components against cisplatin-induced intestinal injury. J. Ethnopharmacol. 2021, 269, 113722. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; He, Y.; Zeng, P.; Liu, Y.; Zhang, M.; Hao, C.; Wang, H.; Lv, Z.; Zhang, L. Molecular basis for Poria cocos mushroom polysaccharide used as an antitumour drug in China. J. Cell. Mol. Med. 2019, 23, 4–20. [Google Scholar] [CrossRef]
- Bae, M.-J.; See, H.-J.; Choi, G.; Kang, C.-Y.; Shon, D.-H.; Shin, H.S. Regulatory T cell induced by Poria cocos bark exert therapeutic effects in murine models of atopic dermatitis and food allergy. Mediat. Inflamm. 2016, 2016, 3472608. [Google Scholar] [CrossRef]
- Knorr, R.; Hamburger, M. Quantitative analysis of anti-inflammatory and radical scavenging triterpenoid esters in evening primrose oil. J. Agric. Food Chem. 2004, 52, 3319–3324. [Google Scholar] [CrossRef]
- Ismail, M.F.; El-Maraghy, S.A.; Sadik, N.A. Study of the immunomodulatory and anti-inflammatory effects of evening primrose oil in adjuvant arthritis. Afr. J. Biochem. Res. 2008, 2, 074–080. [Google Scholar]
- Belch, J.J.; Hill, A. Evening primrose oil and borage oil in rheumatologic conditions. Am. J. Clin. Nutr. 2000, 71, 352s–356s. [Google Scholar] [CrossRef]
- Chao, W.-W.; Lin, B.-F. Isolation and identification of bioactive compounds in Andrographis paniculata (Chuanxinlian). Chin. Med. 2010, 5, 17. [Google Scholar] [CrossRef]
- Bukoye, O.; Musbau, A. Immune modulation potentials of aqueous extract of Andrographis paniculata leaves in male rat. Researcher 2011, 3, 48–57. [Google Scholar]
- Jantan, I.; Haque, M.; Ilangkovan, M.; Arshad, L. An insight into the modulatory effects and mechanisms of action of phyllanthus species and their bioactive metabolites on the immune system. Front. Pharmacol. 2019, 10, 878. [Google Scholar] [CrossRef] [PubMed]
- Ishida, M.; Nishi, K.; Kunihiro, N.; Onda, H.; Nishimoto, S.; Sugahara, T. Immunostimulatory effect of aqueous extract of Coriandrum sativum L. seed on macrophages. J. Sci. Food Agric. 2017, 97, 4727–4736. [Google Scholar] [CrossRef]
- Efferth, T.; Oesch, F. Anti-inflammatory and anti-cancer activities of frankincense: Targets, treatments and toxicities. Semin. Cancer Biol. 2022, 80, 39–57. [Google Scholar] [CrossRef] [PubMed]
- Maksimović, Z. On Frankincense. Arch. Pharm. 2021, 71, 1–21. [Google Scholar]
- WERZ, O. Gender Medicine and Frankincense: Novel Findings in Inflammation Research. Sci. Pharm. 2009, 77, 163. [Google Scholar] [CrossRef]
- Soni, A.; Bohra, N. Boswellia serrata-Propogation and uses—A Review. Int. J. Adv. Res. Biol. Sci. 2021, 8, 35–46. [Google Scholar]
- Stürner, K.H.; Stellmann, J.-P.; Dörr, J.; Paul, F.; Friede, T.; Schammler, S.; Reinhardt, S.; Gellissen, S.; Weissflog, G.; Faizy, T.D. A standardised frankincense extract reduces disease activity in relapsing-remitting multiple sclerosis (the SABA phase IIa trial). J. Neurol. Neurosurg. Psychiatry 2018, 89, 330–338. [Google Scholar] [CrossRef]
- Lim, J.S.; Hahn, D.; Gu, M.J.; Oh, J.; Lee, J.S.; Kim, J.-S. Anti-inflammatory and antioxidant effects of 2, 7-dihydroxy-4, 6-dimethoxy phenanthrene isolated from Dioscorea batatas Decne. Appl. Biol. Chem. 2019, 62, 1–9. [Google Scholar]
- Chen, Y.-F.; Zhu, Q.; Wu, S. Preparation of oligosaccharides from Chinese yam and their antioxidant activity. Food Chem. 2015, 173, 1107–1110. [Google Scholar] [CrossRef]
- Jiao, B.; Gao, J. Intensive research on the prospective use of complementary and alternative medicine to treat systemic lupus erythematosus. Drug Discov. Ther. 2013, 7, 167–171. [Google Scholar] [CrossRef]
- Alabi, Q.K.; Akomolafe, R.O.; Akomolafe, J.G.; Aturamu, A.; Ige, M.S.; Kayode, O.O.; Kajewole, D.I. Polyphenol-rich extract of Ocimum gratissimum leaves Prevented Toxic Effects of Cyclophosphamide on the kidney Function of Wistar rats. BMC Complement. Med. Ther. 2021, 21, 274. [Google Scholar] [CrossRef] [PubMed]
- Mahapatra, S.K.; Chakraborty, S.P.; Roy, S. Immunomodulatory role of Ocimum gratissimum and ascorbic acid against nicotine-induced murine peritoneal macrophages in vitro. Oxidative Med. Cell. Longev. 2011, 2011, 734319. [Google Scholar] [CrossRef] [PubMed]
- Batiha, G.E.-S.; Magdy Beshbishy, A.; Wasef, L.; Elewa, Y.H.; El-Hack, A.; Mohamed, E.; Taha, A.E.; Al-Sagheer, A.A.; Devkota, H.P.; Tufarelli, V. Uncaria tomentosa (Willd. ex Schult.) DC.: A review on chemical constituents and biological activities. Appl. Sci. 2020, 10, 2668. [Google Scholar] [CrossRef]
- Kemper, K.J. Cat’s Claw (Uncaria tomentosa); The Center for Holistic Pediatric Education and Research: Boston, MA, USA, 1999. [Google Scholar]
- Hilepo, J.N.; Bellucci, A.G.; Mossey, R.T. Acute renal failure caused by’cat’s claw’herbal remedy in a patient with systemic lupus erythematosus. Nephron 1997, 77, 361. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.H.; Kim, S.; Jung, M.Y.; Ham, I.H.; Whang, W.K. Anti-inflammatory phenylpropanoid glycosides from Clerodendron trichotomum leaves. Arch. Pharmacal Res. 2009, 32, 7–13. [Google Scholar] [CrossRef]
- Chae, S.; Kim, J.S.; Kang, K.A.; Bu, H.D.; Lee, Y.; Hyun, J.W.; Kang, S.S. Antioxidant activity of jionoside D from Clerodendron trichotomum. Biol. Pharm. Bull. 2004, 27, 1504–1508. [Google Scholar] [CrossRef]
- Ren, D.; Shen, Z.-Y.; Qin, L.-P.; Zhu, B. Pharmacology, phytochemistry, and traditional uses of Scrophularia ningpoensis Hemsl. J. Ethnopharmacol. 2020, 269, 113688. [Google Scholar] [CrossRef]
- Chang, C.-M.; Chu, H.-T.; Wei, Y.-H.; Chen, F.-P.; Wang, S.; Wu, P.-C.; Yen, H.-R.; Chen, T.-J.; Chang, H.-H. The core pattern analysis on chinese herbal medicine for Sjögren’s syndrome: A nationwide population-based study. Sci. Rep. 2015, 5, 1–11. [Google Scholar] [CrossRef]


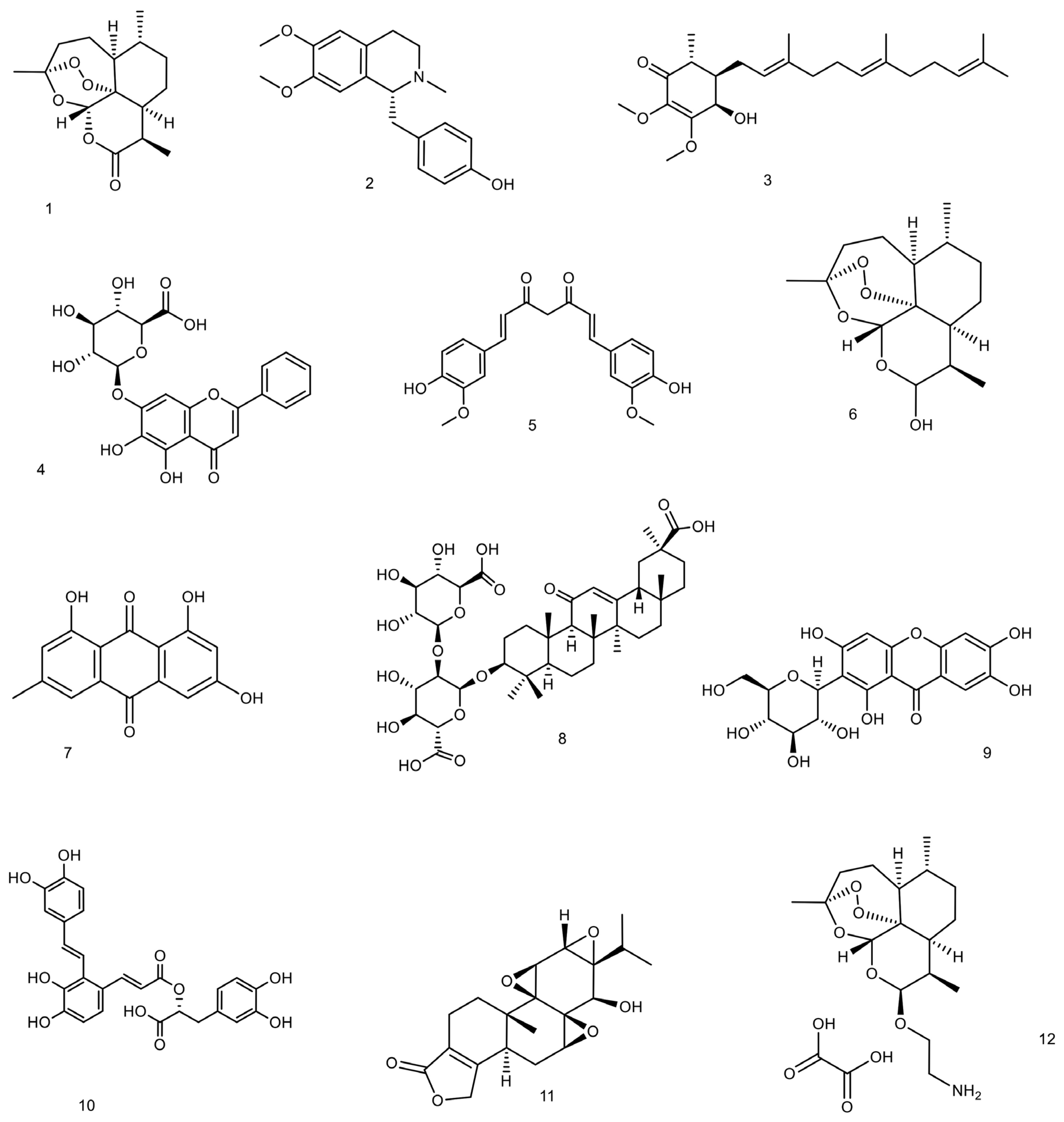{kind=link}
| Plant Name (Scientific Name or Species) | English Name | Endemic Region Endemic Name | Family | Main Parts Used | Main Botanical Characteristics (Description) | Preparations | Main Pharmacological Benefits/Activities/Properties | Reference |
|---|---|---|---|---|---|---|---|---|
| Taiwanofungus camphoratus (M.Zang and C.H.Su) Sheng H.Wu, Z.H.Yu, Y.C.Dai and C.H.Su (Basionym: Ganoderma camphoratum) M.Zang and C.H.Su | Stout camphor fungus | In Taiwan as “Niu-chang-chih” or “Chang-chih” or “Niu-chang-ku” or “Chang-ku” | Polyporaceae | Fruiting bodies | A parasitic fungus on the endemic rotting trees of Cinnamomum kanehirai Hayata causing a brown heart rot | Extract | Antioxidant Anti-inflammatory Immunomodulatory Antimicrobial Anti-diabetic Hepatoprotective Neuroprotective Vasorelaxation Antitumor Anti-hypertensive | [46,47,48] |
| Artemisia annua L. | Annual absinthe, Sweet wormwood, Sweet annie Annual mugwort, Annual wormwood, Sweet wormwood, Chinese wormwood, Sweet sagewort | -Mild climates of Asia -In China as Qinghao | Asteraceae | Leaves | An annual plant with hairless brown erect stems (a height of 50 to 100 cm) and tender leaves about 3 to 5 cm long and many small yellowish-green flowers and brown rounded seeds | Extract | Anti-inflammatory Immunomodulatory Immunosuppressive Antioxidant, Antitumor Anti-malarial, Antibacterial Antifungal, Anti-cancer Anti-obesity, Hepatoprotective, Anti-asthmatic | [49,50] |
| Astragalus propinquus Schischkin (Syn. A. membranaceus fo. propinquus (Schischk.)) Kitag. | Mongolian milkvetch | Huang Qi, in Chinese, Ogi, in Japanese, Milk-Vetch, in English, and Gavan, in Persian | Fabaceae (or Leguminosae) | Roots | A Perennial flowering plant 50–150 cm high, including a straight and long (up to 50 cm) cylindrical root, erect stems branched in the upper parts with small ovate-lanceolate or elliptical leaves | Extract | Anti-inflammatory Immune system boosting Antioxidant, Anti-cancer Neuroprotection, Renoprotection (reduces proteinuria and creatinine), Hepatoprotection, Hypoglycemic Anti-osteoporosis, Anti-fatigue, Cardioprotection | [51] |
| Kalanchoe pinnata (Lam.) Pers. Syn. Bryophyllum pinnatum (Lam.) Oken | Air plant Canterbury bells Cathedral bells Curtain plant Life-plant Fortune plant Good luck leaf Green mother of millions Air plant Mexican love plant | Madagascar In Brazil as “folha-da-fortuna” or “folha-de-pirarucu” or saião “coirama”, In Caribbean as “bruja” | Crassulaceae | Leaves | A perennial succulent herb 0.3–1.2 m tall, including four-angled stems and fleshy simple/compound dark green leaves to 20 cm long and red pendulous flowers | Extract | Anti-inflammatory, Antinociceptive Antianaphylactic Immunomodulator, Immunosuppressive, Antitumor, Antiulcer, Anti-diabetic, Hypotensive, CNS depressant, Antimicrobial Antileishmania, Anthelmintic, Gastroprotective Hepatoprotective Anti-urolithiatic | [52,53,54] |
| Camellia sinensis (L.) Kuntze | Tea plant tea shrub Tea tree | China and Southeast Asia | Theaceae | Leaves | Evergreen shrub or small tree with strong taproot and yellow-white flowers with seven or eight petals | Extract | Antioxidant, Analgesic Anti-inflammatory, Anti-cancer, Anti-fibrotic, Antimutagenic, Cholesterol lowering, Cardiovascular protection, Hepatoprotective, Neuroprotective Anti-diabetic, Anti-obesity Analgesic | [55,56,57] |
| Curcuma longa L. | Turmeric | Indian subcontinent South-east Asian Curcum in the Arab region Indian saffron Haridra (Sanskrit, Ayurvedic) Jianghuang (yellow ginger in Chinese) Kyoo or Ukon (Japanese) | Zingiberaceae | Rhizome | A perennial herbaceous plant with 1 m high with highly branched, yellow to orange, cylindrical, aromatic rhizomes and oblong, pointed leaves and bears funnel-shaped yellow flowers | Powder Extract | Anti-inflammatory Antioxidant Hepatoprotective Anticarcinogenic Anti-diabetic Antimicrobial Antidepressant Lowering cholesterol, triglyceride and low-density lipoprotein (LDL) levels | [58,59,60] |
| Ganoderma lucidum aggregate | Reishi | In China as Lingzhi or herb of spiritual potency | Ganodermataceae Or Polyporaceae | Mycelia Spores Fruit body | Polypore mushroom grows on decaying hardwood trees | Powders Dietary supplements Tea | Immunomodulation Anti-inflammatory, Antioxidant Radical-scavenging Analgesic, Chemo-preventive Antitumor, Chemo and radio protective, Anti-atherosclerotic, Sleep promoting Antimicrobial, Hypolipidemic, Anti-fibrotic Hepatoprotective, Anti-diabetic, Anti-androgenic Anti-angiogenic, Anti-aging, Estrogenic activity, Anti-ulcer | [61,62,63] |
| Ganoderma tsugae Murrill | Hemlock varnish shelf | Ganodermataceae Or Polyporaceae | Fruit body Mycelium | Flat polypore mushroom | Extract | High antioxidant Immunomodulatory, Antitumor, Anti-inflammatory Anti-fibrotic, Antiautoantibody formation | [64] | |
| Gentiana burseri subsp. villarsii (Griseb.) Rouy (Syn. G. macrophylla Pall., G. macrophylla Bertol.) | Large leaf gentian | qin jiao in Chinese | Gentianaceae | Roots Radix Gentianae macrophyllae Flowers | A glabrous pale green perennial with erect, gross, 3–6 mm in diameter and 40–70 cm long stems and very large, acute, elongate-lanceolate and up to 40 cm long leaves with intensely bluish-violet and bell-shaped flowers and brown, bright and wingless seeds. | Extract | Anti-inflammatory, Wound healing, Analgesic, Antioxidant, Immunomodulation Hepatic protection, Joint protection, Cardio-protective Neuro-protective Anti-influenza | [65,66,67,68] |
| Glycyrrhiza glabra L. | Licorice Liquorice | “Sus”, “Mahak”,“Mehak”, “Bikh-e-Mahak”, in Persian ethnomedicine, “Shirin Bayan” (Persian) and “Irk-es-sus” (Arabic). | Fabaceae | Roots | An herbaceous perennial plant, growing to 1 m in height, with pinnate leaves about 7–15 cm long, with 9–17 leaflets. The flowers are 8–12 mm long, purple to pale whitish blue, produced in a loose inflorescence. The roots are stoloniferous. | Extract | Immunomodulatory Anti-inflammatory Antiapoptotic Neuroprotective Nephroprotective | [69,70,71,72] |
| Linum usitatissimum L. | Flax Flaxseed linseed | Cooler parts of Asia, Europe and Mediterranean regions In Persian as Bazr-e katan | Linaceae | Seeds | Annual small flowering plant with an approximate 60–100 cm length and 5 petal pale blue flowers and dark to yellow, oval, flat and pointed seed | Oil Extract Bread | Antioxidant, Immunomodulatory, Anti-inflammatory Antimicrobial, Antiprotozoal, Analgesic, Antihyperlipidemia, Antihyperglycemic, Antitumor | [73,74,75] |
| Nelumbo nucifera Gaertn. (Syn.: Nelumbium nelumbo, N. speciosa, N. speciosum, Nymphaea nelumbo etc.) | Lotus | sacred lotus, Laxmi lotus, Indian lotus, Egyptian bean In Chinese, seeds are called Lian Zi Xin, In India (lotus, kamala, pundarika or padma) | Nelumbonaceae | All parts of the plant (seeds, root, flowers, leaf, stem) | An aquatic species. The flowers (up to 30 cm in diameter) are on thick stems rising several centimeters above the leaves (that spread up to 80 cm in diameter). The leaf stalks grow up to 200 cm long while the peltate leaf blade or lamina can have a horizontal spread of 1 m | Extracts | Anti-inflammatory Immunomodulatory Antipyretic Antioxidant Cardioprotective Hepatoprotective | [76,77] |
| Ophiocordyceps sinensis (Berk.) G.H.Sung, J.M.Sung, Hywel-Jones and Spatafora (syn. Cordyceps sinensis) | Caterpillar fungus | In Tibet as yartsa gunbu In Chinese as “Dong Chong Xia Cao” or “winter worm summer grass” In India as keera jhar, keeda jadi, keeda ghas | Clavicipitaceae Ophiocordycipitaceae | fruiting body | A mushroom with plant-like fruiting body fill with mycelia | Oral liquids Capsules | Immunomodulatory Anti-inflammatory Antioxidative Anti-fibrogenic Antitumor Anti-thrombotic Anti-viral Antifungal | [78,79] |
| Paeonia lactiflora Pall. | Chinese peony Chinese herbaceous peony Common garden peony White Peony | East Asia In Chinese as “Bai Shao Yao”. | Paeoniaceae Or Ranunculaceae | Root (Radix Paeoniae Alba) | Herbaceous perennial flowering plant is about 60–100 cm tall with fleshy roots, annual stems and large compound leaves. The flower buds are large and round, opening into large flowers with 5–10 white, pink, or crimson petals and yellow stamen. | Dried root bark Extract | Anti-inflammatory Immunomodulatory Analgesic Antioxidative Hepatoprotective | [80] |
| Paeonia × suffruticosa Andrews | Cortex Moutan (king of flowers) | In China as mǔdān or Mudanpi | Ranunculaceae or Paeoniaceae | Roots bark | Collective name of cultivated tree peonies, originated from the hybridization of multiple species of wild tree peonies, belong to P. suffruticosa complex. A bush or a tree with attractive flowers and woody stems | Dried root bark Extract | Anti-inflammatory Antioxidative Anti-allergic Antitumor Cardiovascular System Protective Anti-Diabetic Neuroprotective Hepatoprotective Analgesic Sedative | [81] |
| Rehmannia glutinosa (Gaertn.) Liboschitz ex Fischer and C. A. Meyer | Rehmanniae Radix | In China as Di-Huang | Orobanchaceae or Scrophulariaceae | Roots Root tuber | A perennial plant that the roots of it are thick and yellowish in color, while the stems have grayish short hairs. The leaves appear to be gathered at the roots with edges that are blunt and serrated. The flowering form is raceme and blooms purple flowers from June to July. | Extract | Anti-inflammatory Antitumor Immunomodulatory Neuroprotective Hypoglycemic Cardioprotective Antioxidant Hematopoiesis promotion Antianxiety | [82,83] |
| Scutellaria baicalensis Georgi | Baikal skullcap Chinese skullcap Wogonin, baicalin, and baicalein | In China as huángqín | Lamiaceae | Roots and rhizomes | A perennial flowering herb with thick, fleshy, elongated and branched rhizome up to 2 cm in diameter. The leaves are lanceolate to linear lanceolate, 1.5–4.5 cm in length and 0.5–1.2 cm in width. The fruits are hard, ovoid, dark brown with a tumor, 1.5 mm in height, and 1 mm in diameter | Dried Extract | Anti-inflammatory, Antioxidant, Antitumor, Antibacterial, Antiviral, Liver protection, Effects on the nervous system, Effects on the immune system | [84,85,86] |
| Tripterygium wilfordii Hook. f. | -Thunder god vine -Thunder duke vine | In China (Mandarin) as léi gōng téng | Celastraceae | Roots without bark | wood vine plant perennial vien | Extract | Anti-inflammatory Immunomodulatory Immunosuppressive Anti-cancer Anti-fertility | [87,88] |
| Urtica dioica L. | Common nettle Burn nettle Stinging nettle | Europe Asia Africa | Urticaceae | leaves Roots Seeds Aerial parts | A perennial herbaceous plant with underground rhizome and bi-arch root and erect, green and quadrangular stem with dark-green, oblong or ovate leaves and small dioecious, brown to greenish flowers. Tinging trichomes cover both stems and leaves and contain a fluid. | Extract | Anti-inflammatory Antioxidant Analgesic | [89] |
| Phytochemicals | ||||||
|---|---|---|---|---|---|---|
| Compound Name | Class of Compound | Natural Source | Type of Study | Method | Result or Side Effect or Mechanism | Ref. |
| Antroquinonol | Farnesylated quinone | Antrodia camphorata | In vivo | NZB/NZW F1 mice were used Doses: 15 mg/kg antroquinonol orally for 5 weeks. |
| [93] |
| In vivo | SLE-prone NZB/W F1 mice Doses: 100, 200, and 400 mg/kg of the mycelial extract of A. camphorate for 5 consecutive days per week for 12 weeks via gavage. |
| [46] | |||
| (S)-Armepavine | Benzylisoquinoline alkaloid | N. nucifera | In vivo | MRL/MpJ-lpr/lpr mice Doses: 5 and 10 mg/kg/day of oral (S)-armepavine, for 6 weeks. |
| [94] |
| Artemisinin | sesquiterpene lactone | A. annua | Clinical trial | Treatment group: 31 patients were treated with 2–4 g/d of C. sinensis and 0.6 g/d of artemisinin. C. sinensis was taken before three main meals and artemisinin after three main meals for three years. Control group: 30 patients received tripterygiitotorum and/or Baoshenkang. |
| [95] |
| In vivo | MRL lpr/lpr mice aged 12 weeks Doses: 40 µg/kg/d of H1-A daily for 8 weeks. |
| [96] | |||
| Beta-Aminoarteether maleate (SM934) | Synthetic artemisinin derivative (Sesquiterpenes) | an analogue of artemisinin | In vivo, in vitro and ex vivo | In vitro: the effects of SM934 on the activation of polyclonal CD4+ T cells and the differentiation of naive CD4+ T cells were investigated. In vivo: preventive or therapeutic effects of SM934 were investigated in MRL/lpr mice. Ex vivo: the treatment mechanisms were investigated. |
| [97] |
| Baicalin | Flavone glycoside | Scutellaria baicalensis | In vivo | MRL/lpr lupus-prone mice Doses: 200 mg/kg of baicalin daily for 4 weeks, intraperitoneally |
| [98] |
| In vivo | Adult female BALB/c mice Doses: 50 mg/kg of baicalin, orally, once in a day for 10 days. |
| [99] | |||
| Curcumin | Diarylheptanoid | C. longa (turmeric) | Clinical trial | The study was conducted on six SLE patients and six healthy individuals. CD4+ of these people was collected then stimulated by Th17 differentiating factors and exposed to 0.1 and 1 µg/mL curcumin. |
| [100] |
| In vivo and in vitro | Female MRL/lpr mice were treated with 200 mg/kg of curcumin for 8 weeks. |
| [101] | |||
| In vivo | Female NZBWF1 have been treated with 500 mg/kg/day curcumin by oral gavage for 14 days. |
| [102] | |||
| In vivo | Female BALB/c mice with lupus (0.5 cc pristane, i.p.) Doses: 0, 12.5, 50, and 200 mg/kg bw/day curcumin intragastrically daily for 16 weeks. |
| [103] | |||
| Dihydroartemisinin | A derivative of artemisinin (Sesquiterpenes) | A. annua | In vivo | Male BXSB mice Doses: of 5 mg/kg, 25 mg/kg, or 125 mg/kg |
| [104] |
| In vivo | BALB/C female mice were infected with Toxoplasma gondii or Plasmodium berghei. Doses: 2 mg of dihydroartemisinin daily. Spleen and blood samples were collected. |
| [105] | |||
| In vivo and In vitro | Female BALB/c mice have been used. Dose:100 mg/kg of dihydroartemisinin, the fourth group was given 5 mg/kg prednisolone, and the last group was given a combination of prednisolone and dihydroartemisinin with the same previous doses. Dihydroartemisinin and prednisolone were administered daily and orally for two months. |
| [106] | |||
| Emodin | Anthraquinone | Rheum palmatum | In vivo | BXSB lupus mice Mice were treated with different doses of emodin for 30 days. |
| [107] |
| In vivo | Lupus-prone male BXSB mice Doses: 0, 5, 10, and 20 mg/kg/day emodin for 30 days |
| [108] | |||
| Esculetin | Coumarin | C. intybus and H. paniculate | In vivo and In vitro | MRL/lpr mice Doses: esculetin (20 mg/kg and 40 mg/kg) from 10 to 20 weeks |
| [109] |
| Glycyrrhizin (Glycyrrhizic acid) | Triterpenoid saponin | G. glabra | In vivo and In vitro | Female BALB/c mice received 0.5 mg/day of glycyrrhizin for two months. |
| [110] |
| In vivo and In vitro | Glycyrrhizin (10 mg/kg) was injected every other three days into female BALB/c mice for 12 weeks. |
| [111] | |||
| In vitro |
| [112] | ||||
| Mangiferin | Xanthone | A. aspheloidis | In vivo and In vitro | lupus-prone B6/gld mice Doses: 20 or 40 mg/kg/day of mangiferin for 12 weeks, orally |
| [113] |
| Salvianolic acid A | A type of phenolic acid | Salvia miltiorrhiza | In vivo | BALB/c mice Doses: 5 mg/kg/day of salvianolic acid A for 5 months |
| [114] |
| Total glucosides of paeony (TGP) | Glucosides of paeony | P. lactiflora | Clinical trial | One group of 29 cases received TGP for 5 years or more, the other group of 47 cases received TGP for 1 year or more (but less than 5 years), and the third group was the control. |
| [115] |
| Clinical trial | 70 SLE patients were divided into control and treatment groups. Both groups used conventional medicine, but the treatment group also received TGP for three months. |
| [116] | |||
| Meta-analysis on clinical trials |
|
| [117] | |||
| In vivo | MRL/lpr mice were treated with 50 mg/kg/d of TGP by gavage for 4 weeks. |
| [118] | |||
| In vivo | The effect of TGP on lupus nephritis has been investigated on MRL/lpr mice |
| [119] | |||
| In vitro | CD4+ T cells were treated with doses of 0, 62.5, 312.5, and 1562.5 mg/L of TGP for 48 h to elevate the effect of TGP on expression and DNA methylation status of ITGAL gene (CD11a) in CD4+ T cells. |
| [120] | |||
| Triptolide | Diterpenoid epoxide | T. wilfordii | In vitro | To evaluate the effect of triptolide doses: 0, 5, 10, 30 μg/L of triptolide |
| [121] |
| In vivo | BALB/c-in nude mice Dose: 5 mg/kg/d of triptolide, orally blood samples were collected before treatment and 1, 3, and 6 months after treatment. |
| [122] | |||
| In vivo | (NZB×NZW) F1 mice Dose: 6 µg of triptolide or tripdiolide, orally for 15 weeks. |
| [123] | |||
| In vivo | Female MRL/lpr mice Control group received 20 mg/kg/w of cyclophosphamide. treatment groups received 0.2 or 0.3 mg/kg/d of triptolide for 13 weeks. |
| [124] | |||
| (5R)-5-Hydroxytriptolide (LLDT-8) | Diterpenoid epoxide | In vivo | The effect of LLDT-8 on lupus nephritis was investigated so, female MRL/lpr mice were treated with 0.125 mg/kg/2 days of LLDT-8 for 9 weeks. |
| [125] | |
| Fatty acids, vitamins, and minerals | ||||||
| Fatty acids | Fatty acids | meta-analysis | A systematic review and meta-analysis study has been conducted to evaluate the effect of omega-3 fatty acids on SLE disease activity in adults. |
| [22] | |
| In vivo | Weanling (NZB 3 NZW) F1 female mice mice were switched to semi purified diets containing 10% corn oil as control oil and FOs enriched in either EPA or DHA |
| [126] | |||
| Vit A | Vitamin | Clinical trial | 45 female patients with SLE and 45 healthy age-matched and sex-matched patients as control group |
| [127] | |
| Clinical trial | Sixty-two female SLE patients and sixty-two female controls |
| [128] | |||
| Vitamin B | Vitamin | Clinical trial | The association of each nutrient intake with the risk of developing active disease was investigated in 216 patients who initially had inactive disease. The association with atherosclerotic vascular events was assessed in 196 women with inactive disease and no history of atherosclerotic disease at baseline. |
| [129] | |
| Clinical trial | Seventeen patients with SLE were used for 12 weeks |
| [130] | |||
| Vitamin C | Vitamin | Clinical trial | 279 female patients with SLE were followed over 4 years |
| [131] | |
| Vitamin D | Vitamin | Clinical trial | 25-OH vitamin D levels were measured in 198 consecutively recruited SLE patients. |
| [132] | |
| Systematic review | 1268 articles have been reviewed to determine whether supplementation with vitamin D can reduce the risk or modify the course of autoimmune diseases. |
| [133] | |||
| Vitamin E | Vitamin | Clinical trial | 12 women among 36 outpatients received vitamin E (150 to 300 mg/day) together with prednisolone (PSL). |
| [134] | |
| Iron | Mineral | In vivo | Weanling female MRL/MPJ-lpr/lpr mice were used. Mice were fed diets with 3, 10, 35, and 250 mg Fe/kg diet |
| [135] | |
| Selenium | Mineral | In vivo | NZB/NZW female mice Selenium supplementation was provided by adding sodium selenite to the drinking water at 0, 2, or 4 parts per million (mg/L). |
| [136] | |
| In vivo and in vitro | They have investigated the impact of Se on B cells and macrophages using in vitro Se supplementation assays and the B6.Sle1b mouse model of lupus with an oral Se or placebo supplementation regimen. |
| [137] | |||
| Plant Name | Other Names | Type of Study | Method | Result or Side Effect or Mechanism | Ref. |
|---|---|---|---|---|---|
| Antrodia camphorata | Stout camphor fungus | In vivo | SLE-prone NZB/W F1 mice took 100, 200, and 400 mg/kg of A. camphorata extract, orally on 5 consecutive days per week for 12 weeks. |
| [46] |
| Artemisia annua Pall. | Annual wormwood, sweet wormwood, Chinese wormwood, sweet sagewort sweet Annie | In vivo and in vitro | Six groups of female ICR mice were used and there were 5 mice in each group. Splenocytes of immunized mice were isolated and exposed to different concentrations, and finally the number of specific antibodies was counted by indirect ELISA. |
| [228] |
| Astragalus propinquus Schischkin (syn. Astragalus membranaceus (Fisch.) Bunge) | Mongolian milkvetch | In vitro | NK activity of peripheral blood mononuclear cells (PBMC) from 28 patients with SLE was measured using enzyme-release assay. |
| [229] |
| Bryophyllum pinnatum (Lam.) Oken | Kalanchoe pinnata, Zakham-e-hyat, life plant, cathedral bells | In vivo and in vitro | BALB/c mice were treated with different doses of ethanolic extract of B. pinnatum leaves Doses: 10.5, 21, and 42 mg/kg/day for 12 weeks. |
| [230,231] |
| In vitro | The effect of ethanolic extract of B. pinnatum leaves on spleen cells of BALB/c mice Doses: 0, 0.02, 0.1, or 0.5 µg/mL |
| [232] | ||
| In vivo and in silico | The effect of aqueous extract of B. pinnatum leaf on lupus nephritis in female Balb/c mice Doses: 200, 400, or 600 mg/kg/day, orally for 21 days |
| [233] | ||
| Camellia sinensis (L.) Kuntze | Tea | Clinical trial | 68 SLE patients were divided into control and study groups. The study group was treated with 1000 mg of C. sinensis extract daily for 12 weeks. |
| [234] |
| Curcuma longa L. | Turmeric | Clinical trial | 24 patients with lupus nephritis divided into study and control groups. The study group was treated with 1500 mg of turmeric daily for 3 months. |
| [235] |
| Ganoderma lucidum and Ganoderma tsugae | Lingzhi Reishi | In vivo | Female MRL/lpr mice with mild, moderate, and severe lupus Doses: Initially, 500 mg/kg/day was administered orally for 7 days, and then 50 mg/kg/day was injected intraperitoneally for 7 days. |
| [236] |
| In vivo | All groups of NZB/NZW F1 mice (two months of age) were given standard laboratory chow feeding. The first study group was given 0.1 cm3 of oral ganoderma extract, and the second study group was given 0.2 cm3 of oral ganoderma extract, daily. The third study group was given 0.5 mg/kg/day of prednisolone. |
| [237] | ||
| Gentiana macrophylla Pall. | Qinjiao | Clinical trial | Treatment group: 62 patients with SLE were treated with G. macrophylla complex tablets (10 tablets BID or 5 tablets TID) with 10 to 30 mg of prednisolone daily. Control group: 19 SLE patients were treated with prednisolone alone. |
| [238] |
| In vivo and In vitro | Female NZB/W F1 mice divided into the control group, the cholesterol consuming group and the cholesterol and G. macrophylla consuming group. (a 12-week study, heart tissues were examined) |
| [67] | ||
| In vivo and In vitro | Female NZB/W F1 mice—an 8-week study |
| [239] | ||
| Linum usitatissimum L. | Flaxseed, linseed | Clinical trial | 23 patients with lupus nephritis (15 volunteers remained) Doses: 30 g/day A two-year nonplacebo-controlled crossover study |
| [240] |
| Clinical trial | 8 patients with lupus nephritis Doses: 15, 30, and 45 mg of flaxseed daily for four weeks, with a washout of 5 weeks between doses. |
| [241] | ||
| Ophiocordyceps sinensis (syn. Cordyceps sinensis) | Yartsa gumba caterpillar fungus | meta-analysis study | This meta-analysis study was conducted on a total of 14 studies comprising 1301 participants. |
| [142] |
| In vivo | Lupus-prone (NZB/NZW) F1 hybrid mice with different ages (three, six, and eight months) Doses: 2.4 mg/g/day of cultured mycelia of C. sinensis orally |
| [242] | ||
| In vivo | MRL lpr/lpr mice aged 12 weeks Doses: 40 µg/kg/d of H1-A daily for 8 weeks. |
| [96] | ||
| In vivo | The plants studied in this article include: Cordyceps sinensis, Anqelica sinensis, Atractylodes ovata, Codonopsis pilosula, Ligustrum lucidum, and Homo sapiens. 144 NZB/NZW F1 mice at one month of age were divided into 19 groups |
| [243] | ||
| Paeonia lactiflora Pall. | Chinese peony common garden peony shaoyao | In vivo and In vitro | MRL/lpr lupus mice Received Radix Paeoniae Rubra for 12 weeks |
| [244] |
| Paeonia × suffruticosa Andrews | mǔdān Moutan Cortex | Clinical trial | Moutan Cortex extract group: 84 patients control group: 84 patients |
| [245] |
| Rehmannia glutinosa (Gaertn.) DC. | Rehmanniae Radix (Di Huang) | Clinical trial | 72 patients were divided into control and treated groups. The control group was given prednisolone and cyclophosphamide. In the treatment group Radix Rehmanniae and Radix Astragali was added to the treatment regime for 6 months. |
| [246] |
| In vitro | The effect of fresh Rehmanniae radix methanol extract has been investigated in adult female BALB/c mice. Mouse splenocytes were investigated. |
| [247] | ||
| Scutellaria baicalensis Georgi | Baikal skullcap Chinese skullcap | In vitro | In vitro study on splenocytes of pristane-induced lupus BALB/c mice. |
| [248] |
| Tripterygium wilfordii Hook. F. | Thunder duke vine Thunder god vine Léi gōng téng | Clinical trial | There were 23 cases of lupus erythematosus, of which 15 had SLE and 8 had DLE. They were given 45 mg/day of crude extract of T. wilfordii. The control group consisted of 19 cases of SLE treated with prednisolone. |
| [249] |
| Clinical trial | 26 DLE cases treated with T. wilfordii |
| [250] | ||
| Urtica dioica L. | stinging nettle grande ortie anonhasquara | Case report | One female lupus with status renal allograft and elevated serum creatinine was consuming immunosuppressants. She consumed an herbal remedy, consisting of a combination of Agropyron repens rhizome and U. dioica seed extracts (1:3, 5 mL, three times a day for 46 days), and then she received U. dioica seed extract as a monotherapy for three months. |
| [251] |
| In vivo | MRL lpr/lpr mice Dose: 100 µg, inj., every 2 weeks for 4.5 months, blood samples were every 3 |
| [252] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pasdaran, A.; Hassani, B.; Tavakoli, A.; Kozuharova, E.; Hamedi, A. A Review of the Potential Benefits of Herbal Medicines, Small Molecules of Natural Sources, and Supplements for Health Promotion in Lupus Conditions. Life 2023, 13, 1589. https://doi.org/10.3390/life13071589
Pasdaran A, Hassani B, Tavakoli A, Kozuharova E, Hamedi A. A Review of the Potential Benefits of Herbal Medicines, Small Molecules of Natural Sources, and Supplements for Health Promotion in Lupus Conditions. Life. 2023; 13(7):1589. https://doi.org/10.3390/life13071589
Chicago/Turabian StylePasdaran, Ardalan, Bahareh Hassani, Ali Tavakoli, Ekaterina Kozuharova, and Azadeh Hamedi. 2023. "A Review of the Potential Benefits of Herbal Medicines, Small Molecules of Natural Sources, and Supplements for Health Promotion in Lupus Conditions" Life 13, no. 7: 1589. https://doi.org/10.3390/life13071589
APA StylePasdaran, A., Hassani, B., Tavakoli, A., Kozuharova, E., & Hamedi, A. (2023). A Review of the Potential Benefits of Herbal Medicines, Small Molecules of Natural Sources, and Supplements for Health Promotion in Lupus Conditions. Life, 13(7), 1589. https://doi.org/10.3390/life13071589