



Association of Electrical Cardioversion with Brain Perfusion and Cognitive Function in Patients with Atrial Fibrillation

 , ,
, ,  , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethical Considerations and Informed Consent
2.2. Study Design and Patients
2.3. Outcomes
2.4. Medical History and Clinical Parameters
2.5. Cardiologic Assessment and Surveillance
2.6. Cognitive Assessment
2.7. MRI Examinations
2.8. Image Analysis
2.9. Statistical Analysis
3. Results
3.1. Outcomes of ECV
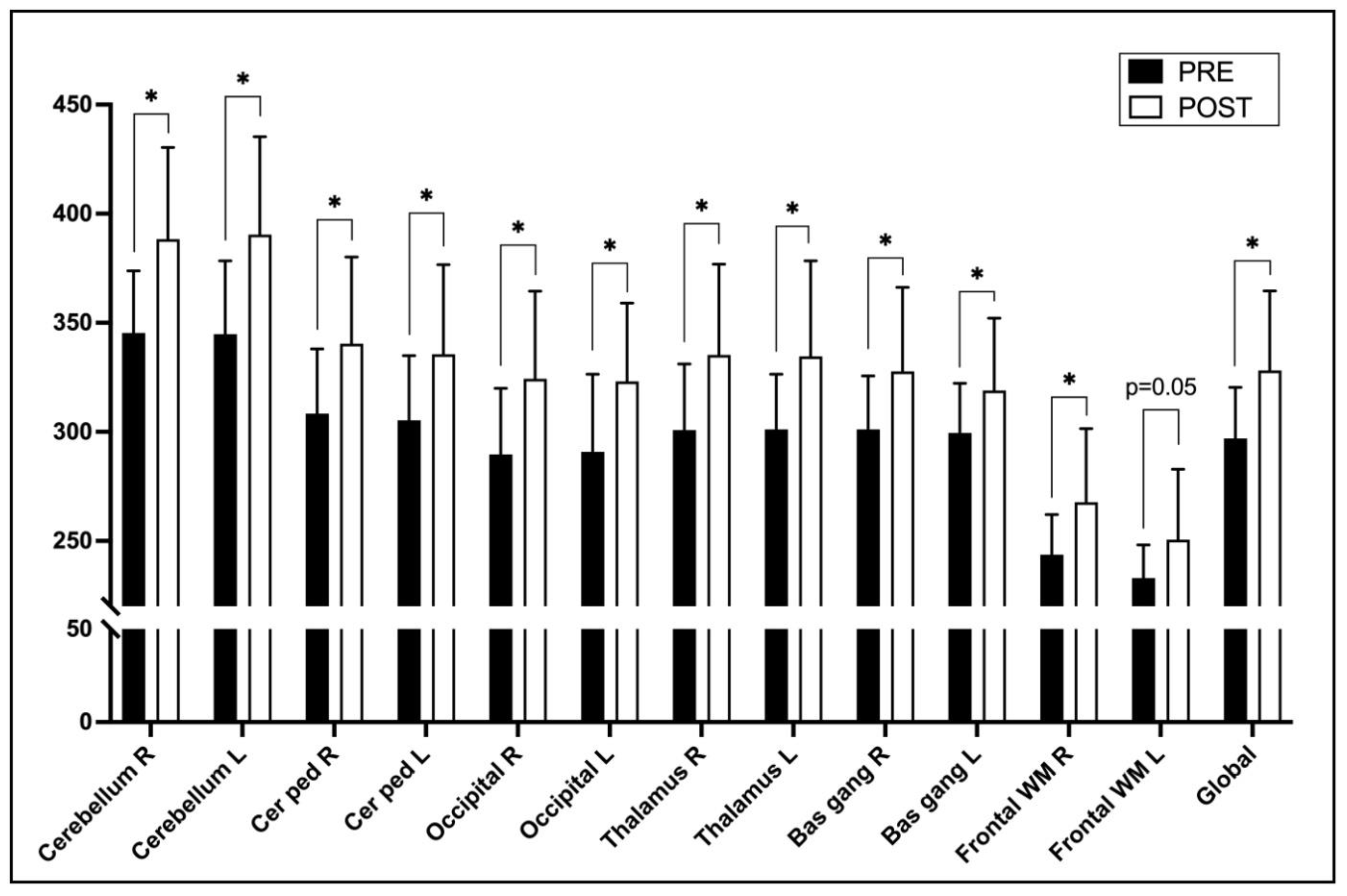
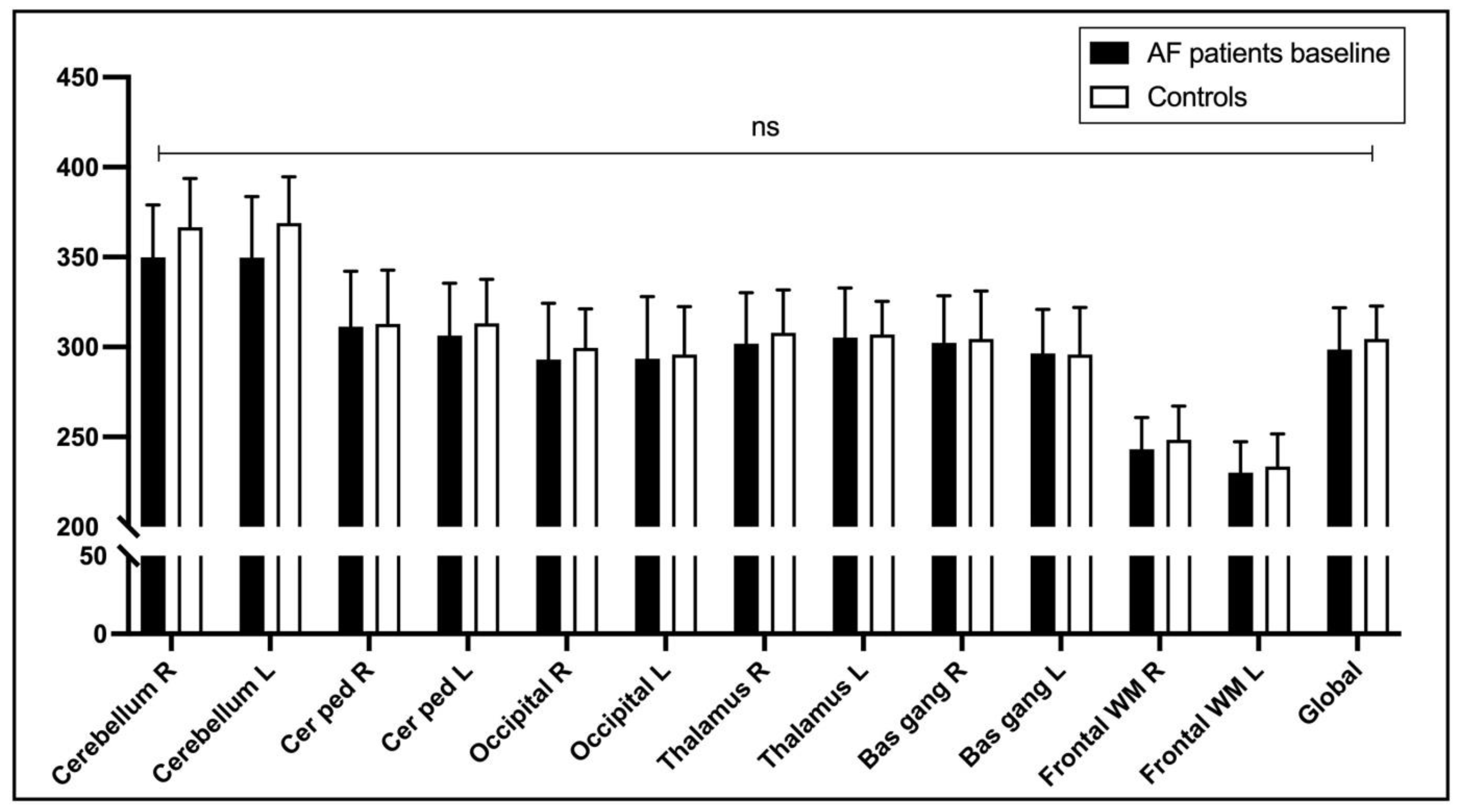
3.2. Brain MRI and ASL
3.3. Cognitive Function Assessment
4. Discussion
5. Conclusions
6. Patents
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Odutayo, A.; Wong, C.X.; Hsiao, A.J.; Hopewell, S.; Altman, D.G.; Emdin, C.A. Atrial fibrillation and risks of cardiovascular disease, renal disease, and death: Systematic review and meta-analysis. BMJ 2016, 354, i4482. [Google Scholar] [CrossRef]
- Lane, D.A.; Skjøth, F.; Lip, G.Y.H.; Larsen, T.B.; Kotecha, D. Temporal Trends in Incidence, Prevalence, and Mortality of Atrial Fibrillation in Primary Care. J. Am. Heart Assoc. 2017, 6, e005155. [Google Scholar] [CrossRef] [PubMed]
- Yiin, G.S.C.; Li, L.; Bejot, Y.; Rothwell, P.M. Time Trends in Atrial Fibrillation-Associated Stroke and Premorbid Anticoagulation: Population-Based Study and Systematic Review. Stroke 2019, 50, 21–27. [Google Scholar] [CrossRef]
- Leys, D.; Hénon, H.; Mackowiak-Cordoliani, M.-A.; Pasquier, F. Poststroke dementia. Lancet Neurol. 2005, 4, 752–759. [Google Scholar] [CrossRef]
- Kim, D.; Yang, P.-S.; Yu, H.T.; Kim, T.-H.; Jang, E.; Sung, J.-H.; Pak, H.-N.; Lee, M.-Y.; Lee, M.-H.; Lip, G.Y.H.; et al. Risk of dementia in stroke-free patients diagnosed with atrial fibrillation: Data from a population-based cohort. Eur. Heart J. 2019, 40, 2313–2323. [Google Scholar] [CrossRef] [PubMed]
- Koh, Y.H.; Lew, L.Z.W.; Franke, K.B.; Elliott, A.D.; Lau, D.H.; Thiyagarajah, A.; Linz, D.; Arstall, M.; Tully, P.J.; Baune, B.T.; et al. Predictive role of atrial fibrillation in cognitive decline: A systematic review and meta-analysis of 2.8 million individuals. EP Eur. 2022, 24, 1229–1239. [Google Scholar] [CrossRef]
- Dietzel, J.; Haeusler, K.G.; Endres, M. Does atrial fibrillation cause cognitive decline and dementia? EP Eur. 2018, 20, 408–419. [Google Scholar] [CrossRef] [PubMed]
- Stefansdottir, H.; Arnar, D.O.; Aspelund, T.; Sigurdsson, S.; Jonsdottir, M.K.; Hjaltason, H.; Launer, L.J.; Gudnason, V. Atrial Fibrillation is Associated With Reduced Brain Volume and Cognitive Function Independent of Cerebral Infarcts. Stroke 2013, 44, 1020–1025. [Google Scholar] [CrossRef] [PubMed]
- Gardarsdottir, M.; Sigurdsson, S.; Aspelund, T.; Rokita, H.; Launer, L.J.; Gudnason, V.; Arnar, D.O. Atrial fibrillation is associated with decreased total cerebral blood flow and brain perfusion. EP Eur. 2018, 20, 1252–1258. [Google Scholar] [CrossRef] [PubMed]
- Gardarsdottir, M.; Sigurdsson, S.; Aspelund, T.; Gardarsdottir, V.A.; Forsberg, L.; Gudnason, V.; Arnar, D.O. Improved brain perfusion after electrical cardioversion of atrial fibrillation. EP Eur. 2020, 22, 530–537. [Google Scholar] [CrossRef]
- Wolters, F.J.; Zonneveld, H.I.; Hofman, A.; van der Lugt, A.; Koudstaal, P.J.; Vernooij, M.W.; Ikram, M.A. Cerebral Perfusion and the Risk of Dementia: A Population-Based Study. Circulation 2017, 136, 719–728. [Google Scholar] [CrossRef] [PubMed]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.-A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef]
- Thomas, L.; Mckay, T.; Byth, K.; Marwick, T.H. Abnormalities of left atrial function after cardioversion: An atrial strain rate study. Heart 2007, 93, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Iverson, G.L.; Marsh, J.M.; Connors, E.J.; Terry, D.P. Normative Reference Values, Reliability, and Item-Level Symptom Endorsement for the PROMIS® v2.0 Cognitive Function-Short Forms 4a, 6a and 8a. Arch. Clin. Neuropsychol. 2021, 36, 1341–1349. [Google Scholar] [CrossRef]
- Wang, J.-N.; Li, J.; Liu, H.-J.; Yin, X.-P.; Zhou, H.; Zheng, Y.-T.; An, N.; Liang, S.; Geng, Z.-J. Application value of three-dimensional arterial spin labeling perfusion imaging in investigating cerebral blood flow dynamics in normal full-term neonates. BMC Pediatr. 2019, 19, 495. [Google Scholar] [CrossRef] [PubMed]
- Yoshihisa, A.; Kono, S.; Kaneshiro, T.; Ichijo, Y.; Misaka, T.; Yamada, S.; Oikawa, M.; Miura, I.; Yabe, H.; Takeishi, Y. Impaired brain activity in patients with persistent atrial fibrillation assessed by near-infrared spectroscopy and its changes after catheter ablation. Sci. Rep. 2022, 12, 7866. [Google Scholar] [CrossRef]
- Knecht, S.; Oelschlager, C.; Duning, T.; Lohmann, H.; Albers, J.; Stehling, C.; Heindel, W.; Breithardt, G.; Berger, K.; Ringelstein, E.B.; et al. Atrial fibrillation in stroke-free patients is associated with memory impairment and hippocampal atrophy. Eur. Heart J. 2008, 29, 2125–2132. [Google Scholar] [CrossRef] [PubMed]
- van Dalen, J.W.; Mutsaerts, H.J.; Petr, J.; Caan, M.W.; van Charante, E.P.M.; MacIntosh, B.J.; van Gool, W.A.; Nederveen, A.J.; Richard, E. Longitudinal relation between blood pressure, antihypertensive use and cerebral blood flow, using arterial spin labelling MRI. J. Cereb. Blood Flow Metab. 2021, 41, 1756–1766. [Google Scholar] [CrossRef]
- Elbejjani, M.; Auer, R.; Dolui, S.; Jacobs, D.R.; Haight, T.; Goff, D.C.; Detre, J.A.; Davatzikos, C.; Bryan, R.N.; Launer, L.J. Cigarette smoking and cerebral blood flow in a cohort of middle-aged adults. J. Cereb. Blood Flow Metab. 2019, 39, 1247–1257. [Google Scholar] [CrossRef] [PubMed]
- Dagres, N.; Chao, T.-F.; Fenelon, G.; Aguinaga, L.; Benhayon, D.; Benjamin, E.J.; Bunch, T.J.; Chen, L.Y.; Chen, S.-A.; Darrieux, F.; et al. European Heart Rhythm Association (EHRA)/Heart Rhythm Society (HRS)/Asia Pacific Heart Rhythm Society (APHRS)/Latin American Heart Rhythm Society (LAHRS) expert consensus on arrhythmias and cognitive function: What is the best practice? EP Eur. 2018, 20, 1399–1421. [Google Scholar]
- Jennings, J.R.; Heim, A.F.; Kuan, D.C.-H.; Gianaros, P.J.; Muldoon, M.F.; Manuck, S.B. Use of Total Cerebral Blood Flow as an Imaging Biomarker of Known Cardiovascular Risks. Stroke 2013, 44, 2480–2485. [Google Scholar] [CrossRef]
- Kim, D.; Yang, P.-S.; Jang, E.; Tae Yu, H.; Kim, T.-H.; Uhm, J.-S.; Kim, J.-Y.; Sung, J.-H.; Pak, H.-N.; Lee, M.-H.; et al. Blood Pressure Control and Dementia Risk in Midlife Patients With Atrial Fibrillation. Hypertension 2020, 75, 1296–1304. [Google Scholar] [CrossRef]
- Takahashi, Y.; Yamamoto, T.; Oyama, J.; Sugihara, G.; Shirai, Y.; Tao, S.; Takigawa, M.; Sato, H.; Sasaki, M.; Hirakawa, A.; et al. Increase in Cerebral Blood Flow After Catheter Ablation of Atrial Fibrillation. JACC Clin. Electrophysiol. 2022, 8, 1369–1377. [Google Scholar] [CrossRef]
- Saglietto, A.; Scarsoglio, S.; Canova, D.; Roatta, S.; Gianotto, N.; Piccotti, A.; Franzin, S.; Gaita, F.; De Ferrari, G.M.; Ridolfi, L.; et al. Increased beat-to-beat variability of cerebral microcirculatory perfusion during atrial fibrillation: A near-infrared spectroscopy study. EP Eur. 2021, 23, 1219–1226. [Google Scholar] [CrossRef] [PubMed]
- Wutzler, A.; Nee, J.; Boldt, L.-H.; Kuhnle, Y.; Graser, S.; Schroder, T.; Haverkamp, W.; Storm, C. Improvement of cerebral oxygen saturation after successful electrical cardioversion of atrial fibrillation. Europace 2014, 16, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Elbers, P.W.G.; Prins, W.B.; Plokker, H.W.M.; van Dongen, E.P.A.; van Iterson, M.; Ince, C. Electrical Cardioversion for Atrial Fibrillation Improves Microvascular Flow Independent of Blood Pressure Changes. J. Cardiothorac. Vasc. Anesth. 2012, 26, 799–803. [Google Scholar] [CrossRef] [PubMed]
- Efimova, I.; Efimova, N.; Chernov, V.; Popov, S.; Lishmanov, Y. Ablation and Pacing: Improving Brain Perfusion and Cognitive Function in Patients with Atrial Fibrillation and Uncontrolled Ventricular Rates: Ablation and pacing: Improving bp anf cf. Pacing Clin. Electrophysiol. 2012, 35, 320–326. [Google Scholar] [CrossRef] [PubMed]
- Cacciatore, F.; Testa, G.; Langellotto, A.; Galizia, G.; Della-Morte, D.; Gargiulo, G.; Bevilacqua, A.; Del Genio, M.T.; Canonico, V.; Rengo, F.; et al. Role of ventricular rate response on dementia in cognitively impaired elderly subjects with atrial fibrillation: A 10-year study. Dement. Geriatr. Cogn. Disord. 2012, 34, 143–148. [Google Scholar] [CrossRef]
- Saglietto, A.; Scarsoglio, S.; Ridolfi, L.; Gaita, F.; Anselmino, M. Higher ventricular rate during atrial fibrillation relates to increased cerebral hypoperfusions and hypertensive events. Sci. Rep. 2019, 9, 3779. [Google Scholar] [CrossRef]
- de Bruijn, R.F.A.G.; Heeringa, J.; Wolters, F.J.; Franco, O.H.; Stricker, B.H.C.; Hofman, A.; Koudstaal, P.J.; Ikram, M.A. Association Between Atrial Fibrillation and Dementia in the General Population. JAMA Neurol. 2015, 72, 1288. [Google Scholar] [CrossRef]
- Willems, S.; Borof, K.; Brandes, A.; Breithardt, G.; Camm, A.J.; Crijns, H.J.G.M.; Eckardt, L.; Gessler, N.; Goette, A.; Haegeli, L.M.; et al. Systematic, early rhythm control strategy for atrial fibrillation in patients with or without symptoms: The EAST-AFNET 4 trial. Eur. Heart J. 2022, 43, 1219–1230. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| AF Patients (N = 25) | Controls (N = 16) | p Value | |
|---|---|---|---|
| Sex (male) | 16 (64%) | 10 (63%) | 0.99 |
| Age (years) | 67 ± 8 | 66 ± 4 | 0.77 |
| Height (cm) | 178 ± 10 | 178 ± 11 | 0.98 |
| Weight (kg) | 93 ± 13 | 90 ± 12 | 0.59 |
| BMI (kg/m2) | 29 ± 3 | 28 ± 3 | 0.49 |
| SBP (mm Hg) | 134 ± 16 | 136 ± 18 | 0.77 |
| DBP (mm Hg) | 80 ± 8 | 80 ± 11 | 0.93 |
| Heart rate (bpm) | 90 ± 16 | 70 ± 11 | <0.0001 * |
| Diagnostic tests | |||
| Hgb (g/L) | 142 ± 15 | 146 ± 9 | 0.34 |
| Htc | 0.423 ± 0.043 | 0.427 ± 0.023 | 0.79 |
| Creatinine (mol/L) | 85 ± 19 | 79 ± 9 | 0.27 |
| eGFR (ml/min) | 74 ± 20 | 70 ± 10 | 0.37 |
| Blood glucose (mmol/L) | 6.3 ± 2.5 | 6.7 ± 2.5 | 0.67 |
| Albumin (g/L) | 43.8 ± 3.3 | 43.8 ± 2.8 | 0.96 |
| Total cholesterol (mmol/L) | 5.0 ± 1.0 | 5.4 ± 1.0 | 0.23 |
| LDL (mmol/L) | 3.0 ± 0.9 | 3.1 ± 0.7 | 0.59 |
| NT-proBNP (pg/mL) | 1069 ± 605 | 108 ± 72 | <0.0001 * |
| hs-TnT (ng/L) | 9.8 ± 4.1 | 12.4 ± 4.8 | 0.07 |
| vWF | 1.8 ± 0.7 | 1.4 ± 0.4 | 0.04 * |
| PROMIS | 52.2 ± 9.6 | 51.2 ± 6.2 | 0.71 |
| Comorbidities | |||
| Smoking | 7 (28%) | 4 (25%) | 0.99 |
| Hypertension | 18 (72%) | 12 (75%) | 0.99 |
| Diabetes | 4 (16%) | 3 (19%) | 0.99 |
| CKD | 0 (0%) | 0 (0%) | NS |
| Medications | |||
| Anticoagulation | 25 (100%) | 1 (6%) | <0.0001 * |
| Antiplatelets | 0 (0%) | 4 (25%) | 0.02 * |
| β blocker | 23 (92%) | 3 (19%) | <0.0001 * |
| ACE inhibitor | 15 (60%) | 11 (69%) | 0.74 |
| Statin | 7 (28%) | 4 (25%) | 0.99 |
| Parameter | PRE | POST | p Value |
|---|---|---|---|
| SBP (mm Hg) | 136 ± 19 | 143 ± 18 | 0.02 * |
| DPB (mm Hg) | 79 ± 9 | 80 ± 7 | 0.67 |
| HR (bpm) | 91 ± 15 | 65 ± 8 | 0.0002 * |
| NT-proBNP (pg/mL) | 979 ± 379 | 284 ± 145 | <0.0001 * |
| hs-TnT (ng/L) | 9.7 ± 4.1 | 9.2 ± 4.0 | 0.31 |
| vWF | 1.8 ± 0.8 | 1.7 ± 0.4 | 0.45 |
| PROMIS. | 53 ± 10 | 54 ± 9 | 0.46 |
| Brain Perfusion | ||||||
|---|---|---|---|---|---|---|
| without Arrhythmia Recurrence (N = 15) | with Arrhythmia Recurrence (N = 8) | |||||
| PRE | POST | p Value | PRE | POST | p Value | |
| Cerebellum R | 345 ± 26 | 388 ± 42 | 0.003 * | 352 ±27 | 369 ± 27 | 0.23 |
| Cerebellum L | 345 ± 35 | 390 ± 45 | 0.002 * | 351 ± 30 | 364 ± 26 | 0.29 |
| Cer ped R | 309 ± 31 | 340 ± 40 | 0.01 * | 307 ± 19 | 321 ± 30 | 0.32 |
| Cer ped L | 305 ± 31 | 336 ± 41 | 0.01 * | 301 ± 21 | 317 ± 33 | 0.29 |
| Occipital R | 289 ± 31 | 324 ± 40 | 0.004 * | 292 ± 29 | 302 ± 37 | 0.48 |
| Occipital L | 292 ± 37 | 323 ±36 | 0.01 * | 290 ± 22 | 297 ± 36 | 0.61 |
| Talamus R | 303 ± 30 | 335 ± 42 | 0.01 * | 298 ± 23 | 304 ± 25 | 0.70 |
| Talamus L | 303 ± 25 | 335 ± 44 | 0.01 * | 309 ± 32 | 311 ± 25 | 0.89 |
| Bas gang R | 302 ± 25 | 328 ± 39 | 0.03 * | 302 ± 32 | 315 ± 22 | 0.39 |
| Bas gang L | 297 ± 21 | 319 ± 33 | 0.04 * | 295 ± 27 | 301 ± 23 | 0.65 |
| Front WM R | 244 ± 19 | 268 ± 34 | 0.01 * | 240 ± 17 | 251 ± 19 | 0.32 |
| Front WM L | 234 ± 16 | 251 ± 32 | 0.05 | 230 ± 14 | 235 ± 24 | 0.67 |
| Global | 297 ± 24 | 328 ± 37 | 0.008 * | 297 ± 22 | 307 ± 24 | 0.45 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kedžo, J.; Lovrić Kojundžić, S.; Marinović Guić, M.; Tandara, L.; Brešković, T.; Jurišić, Z. Association of Electrical Cardioversion with Brain Perfusion and Cognitive Function in Patients with Atrial Fibrillation. Life 2023, 13, 935. https://doi.org/10.3390/life13040935
Kedžo J, Lovrić Kojundžić S, Marinović Guić M, Tandara L, Brešković T, Jurišić Z. Association of Electrical Cardioversion with Brain Perfusion and Cognitive Function in Patients with Atrial Fibrillation. Life. 2023; 13(4):935. https://doi.org/10.3390/life13040935
Chicago/Turabian StyleKedžo, Josip, Sanja Lovrić Kojundžić, Maja Marinović Guić, Leida Tandara, Toni Brešković, and Zrinka Jurišić. 2023. "Association of Electrical Cardioversion with Brain Perfusion and Cognitive Function in Patients with Atrial Fibrillation" Life 13, no. 4: 935. https://doi.org/10.3390/life13040935
APA StyleKedžo, J., Lovrić Kojundžić, S., Marinović Guić, M., Tandara, L., Brešković, T., & Jurišić, Z. (2023). Association of Electrical Cardioversion with Brain Perfusion and Cognitive Function in Patients with Atrial Fibrillation. Life, 13(4), 935. https://doi.org/10.3390/life13040935