
Glaucoma and Systemic Disease

Abstract
1. Glaucoma Introduction and Definition
1.1. Introduction and Epidemiology of Glaucoma
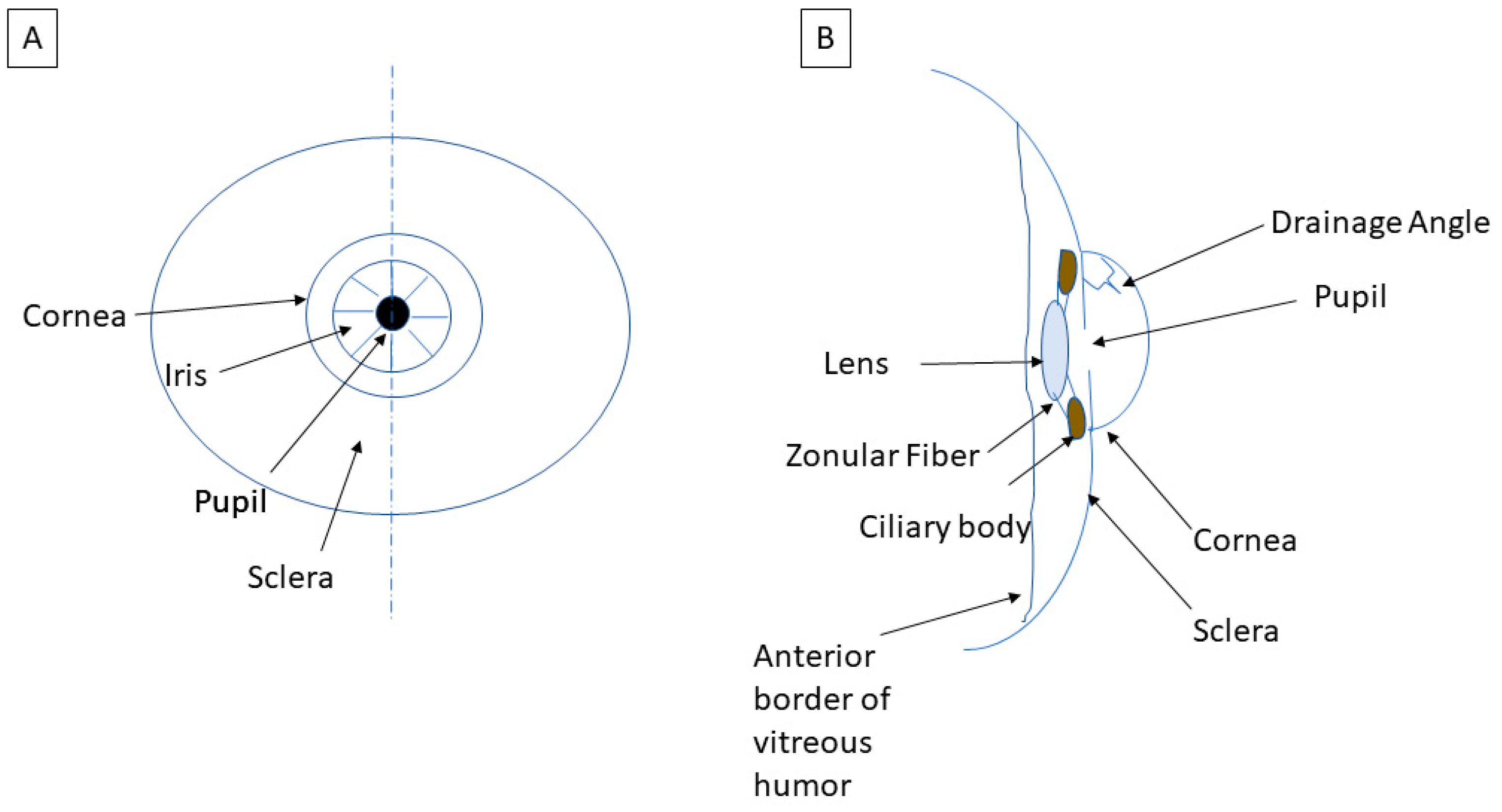
1.2. What Defines Intraocular Pressure?
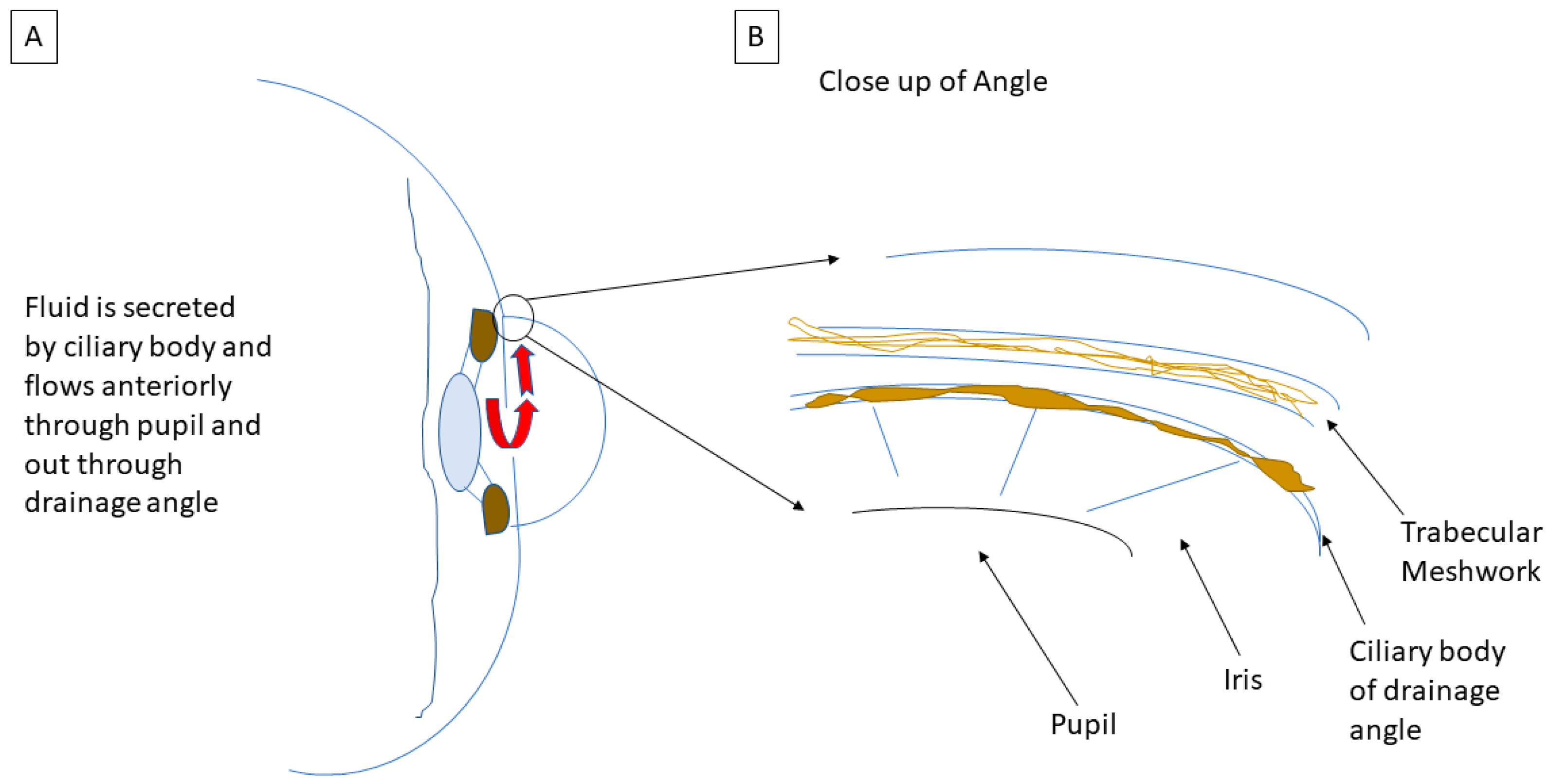
1.3. Mechanism of Open-Angle Glaucoma
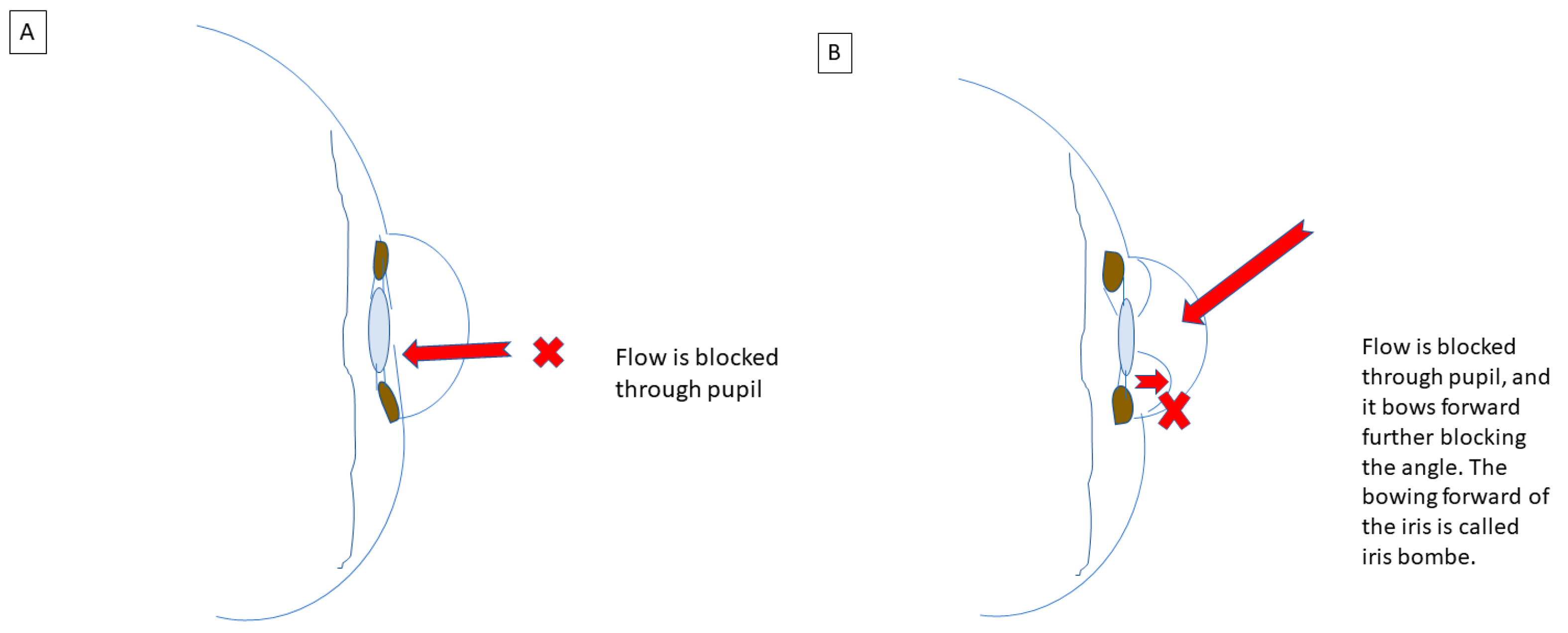
1.4. Mechanisms of Closed-Angle Glaucoma
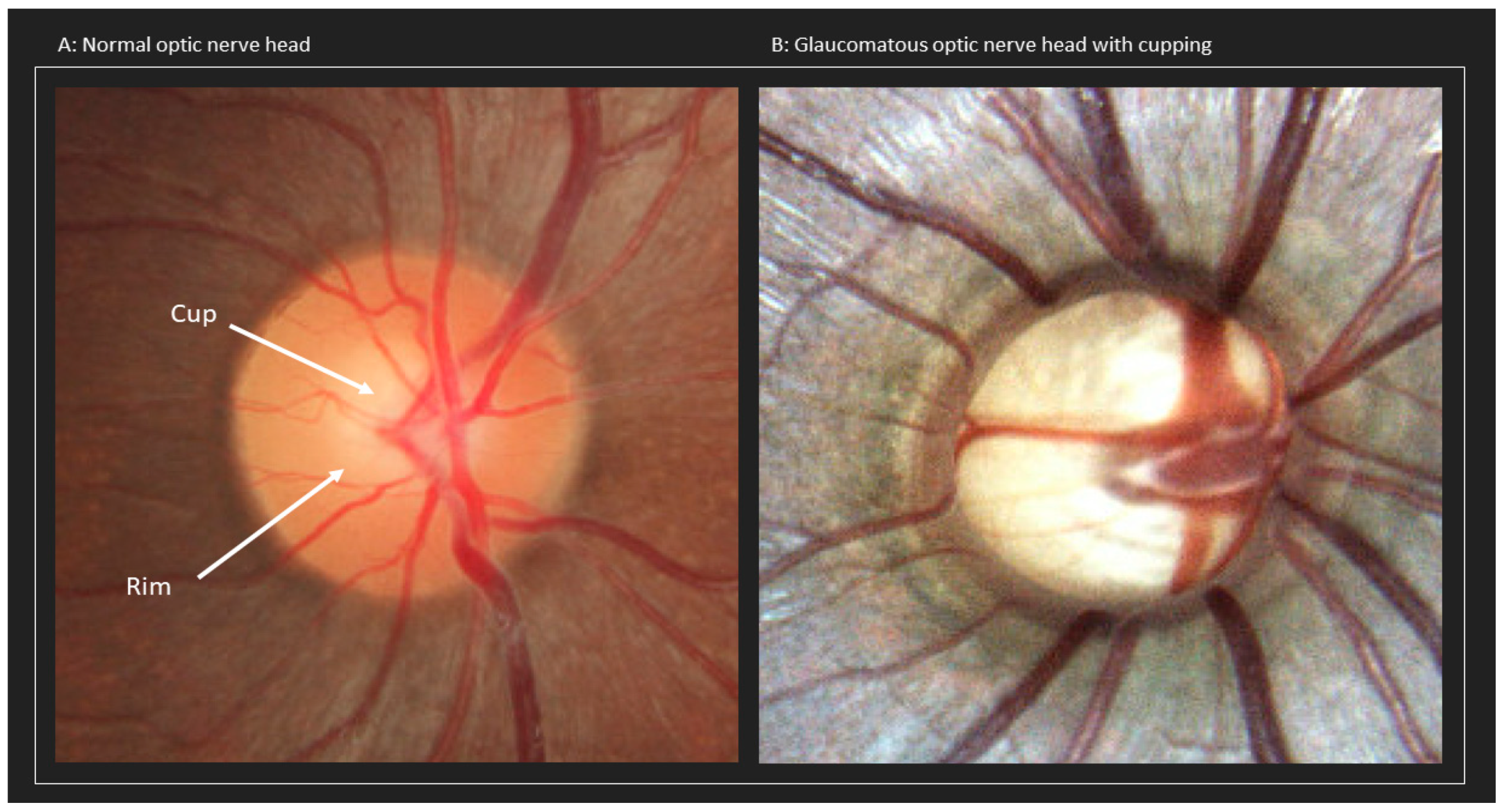
1.5. Mechanisms Leading to Optic Nerve Damage
1.5.1. Mechanical Dysfunction
1.5.2. Vascular Dysfunction
1.5.3. Autonomic Dysfunction
1.6. Outline of the Review
2. Pharmacologically Induced Glaucoma
2.1. Medications Associated with Glaucoma
2.1.1. Topiramate
2.1.2. Anticholinergic and Cholinergic Agonists
2.2. Association of Corticosteroid Use with Glaucoma
2.2.1. Mechanisms of Corticosteroid-Induced IOP Elevation
2.2.2. Management of Corticosteroid-Induced IOP Elevation
2.3. Management of Drug-Induced Glaucoma
3. Inflammatory/Autoimmune and Infectious Diseases
Management of Intraocular Inflammation
4. Dermatologic Conditions Associated with Glaucoma
4.1. Vitiligo
4.2. Cutaneous Sarcoidosis
4.3. Cutaneous Manifestations from Systemic Inflammatory Diseases
5. Cardiovascular Conditions Associated with Glaucoma
5.1. Diabetes Mellitus and Diabetic Retinopathy
5.2. Systemic Hypertension
Hypertension and Central Retinal Vein Occlusion
5.3. Hypotension
5.4. Carotid-Cavernous (CC) Fistula
5.5. Pseudoexfoliation Syndrome
6. Pulmonary Conditions Associated with Glaucoma
6.1. COPD and Obstructive Lung Patterns
6.2. Asthma
6.3. Obstructive Sleep Apnea
7. Renal Conditions Associated with Glaucoma
Chronic Kidney Disease
8. Urologic Conditions Associated with Glaucoma
Overactive Bladder
9. Neurologic Conditions Associated with Glaucoma
9.1. Alzheimer’s and Other Neurodegenerative Diseases
9.1.1. Mechanistic Associations between Glaucoma and Alzheimer’s Disease
9.1.2. Alzheimer’s Disease, Pseudoexfoliation Syndrome, and Glaucoma
9.2. Migraines
10. Psychiatric Conditions Associated with Glaucoma
11. Systemic Malignancies and Intraocular Tumors
11.1. Association of Intraocular Tumors and Elevated IOP
11.2. Metastasis to the Eye from Systemic Malignancies
11.3. Primary Intraocular Tumors
12. Pediatric and Genetic Diseases
12.1. Introduction to Glaucoma in the Pediatric Population
12.2. Management of Pediatric Glaucoma
13. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Flaxman, S.R.; Bourne, R.R.A.; Resnikoff, S.; Ackland, P.; Braithwaite, T.; Cicinelli, M.V.; Das, A.; Jonas, J.B.; Keeffe, J.; Kempen, J.H.; et al. Global causes of blindness and distance vision impairment 1990–2020: A systematic review and meta-analysis. Lancet Glob. Health 2017, 5, e1221–e1234. [Google Scholar] [CrossRef] [PubMed]
- Zhang, N.; Wang, J.; Li, Y.; Jiang, B. Prevalence of primary open angle glaucoma in the last 20 years: A meta-analysis and systematic review. Sci. Rep. 2021, 11, 13762. [Google Scholar] [CrossRef]
- Varma, R.; Ying-Lai, M.; A Francis, B.; Nguyen, B.B.-T.; Deneen, J.; Wilson, M.; Azen, S.P.; Los Angeles Latino Eye Study Group. Prevalence of open-angle glaucoma and ocular hypertension in Latinos: The Los Angeles Latino Eye Study. Ophthalmology 2004, 111, 1439–1448. [Google Scholar] [CrossRef]
- Restrepo, N.A.; Bailey, J.N.C. Primary Open-Angle Glaucoma Genetics in African Americans. Curr. Genet. Med. Rep. 2017, 5, 167–174. [Google Scholar] [CrossRef] [PubMed]
- Mahabadi, N.; Foris, L.A.; Tripathy, K. Open Angle Glaucoma. In StatPearls; StatPearls Publishing: Tampa, FL, USA, 2022. Available online: http://www.ncbi.nlm.nih.gov/books/NBK441887/ (accessed on 6 February 2023).
- Pasquale, L.R. Vascular and Autonomic Dysregulation in Primary Open-Angle Glaucoma. Curr. Opin. Ophthalmol. 2016, 27, 94–101. [Google Scholar] [CrossRef] [PubMed]
- Tutaj, M.; Brown, C.M.; Brys, M.; Marthol, H.; Hecht, M.J.; Dutsch, M.; Michelson, G.; Hilz, M.J. Dynamic cerebral autoregulation is impaired in glaucoma. J. Neurol. Sci. 2004, 220, 49–54. [Google Scholar] [CrossRef]
- Samuels, B.C.; Hammes, N.M.; Johnson, P.L.; Shekhar, A.; McKinnon, S.J.; Allingham, R.R. Dorsomedial/Perifornical Hypothalamic Stimulation Increases Intraocular Pressure, Intracranial Pressure, and the Translaminar Pressure Gradient. Investig. Opthalmol. Vis. Sci. 2012, 53, 7328–7335. [Google Scholar] [CrossRef]
- Agnifili, L.; Mastropasqua, R.; Frezzotti, P.; Fasanella, V.; Motolese, I.; Pedrotti, E.; Di Iorio, A.; Mattei, P.A.; Motolese, E.; Mastropasqua, L. Circadian intraocular pressure patterns in healthy subjects, primary open angle and normal tension glaucoma patients with a contact lens sensor. Acta Ophthalmol. 2015, 93, e14–e21. [Google Scholar] [CrossRef]
- Ah-kee, E.Y.; Egong, E.; Shafi, A.; Lim, L.T.; Yim, J.L. A review of drug-induced acute angle closure glaucoma for non-ophthalmologists. Qatar Med. J. 2015, 2015, 6. [Google Scholar] [CrossRef]
- Razeghinejad, M.R.; Pro, M.J.; Katz, L.J. Non-steroidal drug-induced glaucoma. Eye 2011, 25, 971–980. [Google Scholar] [CrossRef]
- Lachkar, Y.; Bouassida, W. Drug-induced acute angle closure glaucoma. Curr. Opin. Ophthalmol. 2007, 18, 129–133. [Google Scholar] [CrossRef] [PubMed]
- Ciobanu, A.M.; Dionisie, V.; Neagu, C.; Bolog, O.M.; Riga, S.; Popa-Velea, O. Psychopharmacological Treatment, Intraocular Pressure and the Risk of Glaucoma: A Review of Literature. J. Clin. Med. 2021, 10, 2947. [Google Scholar] [CrossRef] [PubMed]
- Lan, Y.W.; Hsieh, J.W. Bilateral acute angle closure glaucoma and myopic shift by topiramate-induced ciliochoroidal effusion: Case report and literature review. Int. Ophthalmol. 2018, 38, 2639–2648. [Google Scholar] [CrossRef]
- Yamashita, T.; Kodama, Y.; Tanaka, M.; Yamakiri, K.; Kawano, Y.; Sakamoto, T. Steroid-induced glaucoma in children with acute lymphoblastic leukemia: A possible complication. J. Glaucoma 2010, 19, 188–190. [Google Scholar] [CrossRef] [PubMed]
- Phulke, S.; Kaushik, S.; Kaur, S.; Pandav, S. Steroid-induced Glaucoma: An Avoidable Irreversible Blindness. J. Curr. Glaucoma Pract. 2017, 11, 67–72. [Google Scholar] [CrossRef]
- Feroze, K.B.; Khazaeni, L. Steroid Induced Glaucoma. In StatPearls; StatPearls Publishing: Tampa, FL, USA, 2022. Available online: http://www.ncbi.nlm.nih.gov/books/NBK430903/ (accessed on 26 January 2023).
- Kersey, J.P.; Broadway, D.C. Corticosteroid-induced glaucoma: A review of the literature. Eye 2006, 20, 407–416. [Google Scholar] [CrossRef]
- Korenfeld, M.S.; Silverstein, S.M.; Cooke, D.L.; Vogel, R.; Crockett, R.S. Difluprednate ophthalmic emulsion 0.05% for postoperative inflammation and pain. J. Cataract. Refract. Surg. 2009, 35, 26–34. [Google Scholar] [CrossRef]
- Hayashi, K.; Hayashi, H. Intravitreal versus retrobulbar injections of triamcinolone for macular edema associated with branch retinal vein occlusion. Am. J. Ophthalmol. 2005, 139, 972–982. [Google Scholar] [CrossRef]
- Boyer, D.S.; Yoon, Y.H.; Belfort, R.; Bandello, F.; Maturi, R.K.; Augustin, A.J.; Li, X.-Y.; Cui, H.; Hashad, Y.; Whitcup, S.M. Three-year, randomized, sham-controlled trial of dexamethasone intravitreal implant in patients with diabetic macular edema. Ophthalmology 2014, 121, 1904–1914. [Google Scholar] [CrossRef]
- Jaffe, G.J.; Martin, D.; Callanan, D.; Pearson, P.A.; Levy, B.; Comstock, T. Fluocinolone Acetonide Implant (Retisert) for Noninfectious Posterior Uveitis: Thirty-Four–Week Results of a Multicenter Randomized Clinical Study. Ophthalmology 2006, 113, 1020–1027. [Google Scholar] [CrossRef]
- Garbe, E.; LeLorier, J.; Boivin, J.F.; Suissa, S. Risk of ocular hypertension or open-angle glaucoma in elderly patients on oral glucocorticoids. Lancet 1997, 350, 979–982. [Google Scholar] [CrossRef]
- Ishii, M.; Horita, N.; Takeuchi, M.; Matsumoto, H.; Ebina-Shibuya, R.; Hara, Y.; Kobayashi, N.; Mizuki, N.; Kaneko, T. Inhaled Corticosteroid and Secondary Glaucoma: A Meta-analysis of 18 Studies. Allergy Asthma Immunol. Res. 2021, 13, 435–449. [Google Scholar] [CrossRef]
- Mitchell, P.; Cumming, R.G.; Mackey, D.A. Inhaled corticosteroids, family history, and risk of glaucoma. Ophthalmology 1999, 106, 2301–2306. [Google Scholar] [CrossRef] [PubMed]
- Ren, R.; Humphrey, A.A.; Kopczynski, C.; Gong, H. Rho Kinase Inhibitor AR-12286 Reverses Steroid-Induced Changes in Intraocular Pressure, Effective Filtration Areas, and Morphology in Mouse Eyes. Investig. Opthalmol. Vis. Sci. 2023, 64, 7. [Google Scholar] [CrossRef] [PubMed]
- Siddique, S.S.; Suelves, A.M.; Baheti, U.; Foster, C.S. Glaucoma and uveitis. Surv. Ophthalmol. 2013, 58, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.H.; McCluskey, P.J.; Wakefield, D. Acute anterior uveitis and HLA-B27. Surv. Ophthalmol. 2005, 50, 364–388. [Google Scholar] [CrossRef] [PubMed]
- Bodh, S.A.; Kumar, V.; Raina, U.K.; Ghosh, B.; Thakar, M. Inflammatory glaucoma. Oman J. Ophthalmol. 2011, 4, 3–9. [Google Scholar] [CrossRef]
- Moorthy, R.S.; Mermoud, A.; Baerveldt, G.; Minckler, D.S.; Lee, P.P.; Rao, N.A. Glaucoma associated with uveitis. Surv. Ophthalmol. 1997, 41, 361–394. [Google Scholar] [CrossRef]
- Salim, S.; Boyle, J.W.; Netland, P.A. Pathophysiology and management uveitic glaucoma. Ophthalmic Pearls Glaucoma 2012. published online. [Google Scholar]
- Prevalence of Glaucoma in Patients with Vitiligo. Available online: https://www.mdedge.com/dermatology/article/108289/pigmentation-disorders/prevalence-glaucoma-patients-vitiligo (accessed on 13 February 2023).
- Qiancheng, D.; Shu, D.; Shengbo, Y.; JinHua, H. Cutaneous sarcoidosis and secondary open-angle glaucoma in a patient: Case report and literature review. An. Bras. Dermatol. 2017, 92, 407–409. [Google Scholar] [CrossRef]
- Shazly, T.A.; Latina, M.A. Neovascular glaucoma: Etiology, diagnosis and prognosis. Semin. Ophthalmol. 2009, 24, 113–121. [Google Scholar] [CrossRef] [PubMed]
- Neovascular Glaucoma: A Review—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/27895936/ (accessed on 12 January 2023).
- Silverstone, B.Z.; Marcus, T. Hypoglycemia due to ophthalmic timolol in a diabetic. Harefuah 1990, 118, 693–694. [Google Scholar]
- Zhao, D.; Cho, J.; Kim, M.H.; Guallar, E. The Association of Blood Pressure and Primary Open-Angle Glaucoma: A Meta-Analysis. Am. J. Ophthalmol. 2014, 158, 615–627. Available online: https://www.ajo.com/article/S0002-9394(14)00301-8/fulltext (accessed on 13 February 2023). [CrossRef] [PubMed]
- Havens, S.J.; Gulati, V. Neovascular Glaucoma. Dev. Ophthalmol. 2016, 55, 196–204. [Google Scholar] [CrossRef]
- Lee, J.Y.; Yoon, Y.H.; Kim, H.K.; Yoon, H.S.; Kang, S.W.; Kim, J.-G.; Park, K.H.; Jo, Y.J. Baseline Characteristics and Risk Factors of Retinal Vein Occlusion: A Study by the Korean RVO Study Group. J. Korean Med. Sci. 2013, 28, 136–144. [Google Scholar] [CrossRef]
- Leske, M.C. Ocular perfusion pressure and glaucoma: Clinical trial and epidemiologic findings. Curr. Opin. Ophthalmol. 2009, 20, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Heijl, A.; Leske, M.C.; Bengtsson, B.; Hyman, L.; Hussein, M. Reduction of intraocular pressure and glaucoma progression: Results from the Early Manifest Glaucoma Trial. Arch. Ophthalmol. 2002, 120, 1268–1279. [Google Scholar] [CrossRef]
- Topouzis, F.; Coleman, A.L.; Harris, A.; Jonescu-Cuypers, C.; Yu, F.; Mavroudis, L.; Anastasopoulos, E.; Pappas, T.; Koskosas, A.; Wilson, M.R. Association of blood pressure status with the optic disk structure in non-glaucoma subjects: The Thessaloniki eye study. Am. J. Ophthalmol. 2006, 142, 60–67. [Google Scholar] [CrossRef]
- Ohkubo, T.; Hozawa, A.; Yamaguchi, J.; Kikuya, M.; Ohmori, K.; Michimata, M.; Matsubara, M.; Hashimoto, J.; Hoshi, H.; Araki, T.; et al. Prognostic significance of the nocturnal decline in blood pressure in individuals with and without high 24-h blood pressure: The Ohasama study. J. Hypertens. 2002, 20, 2183–2189. [Google Scholar] [CrossRef]
- Graham, S.L.; Drance, S.M. Nocturnal hypotension: Role in glaucoma progression. Surv. Ophthalmol. 1999, 43 (Suppl. 1), S10–S16. [Google Scholar] [CrossRef]
- Mitchell, P.; Wang, J.J.; Hourihan, F. The Relationship Between Glaucoma and Pseudoexfoliation: The Blue Mountains Eye Study. Arch. Ophthalmol. 1999, 117, 1319–1324. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.S.; Kim, Y.J.; Kim, S.S.; Park, S.; Choi, W.; Bae, H.W.; Kim, C.Y. Increased risk of open-angle glaucoma in non-smoking women with obstructive pattern of spirometric tests. Sci. Rep. 2022, 12, 16915. [Google Scholar] [CrossRef]
- Brooks, A.M.; Gillies, W.E. Ocular beta-blockers in glaucoma management. Clinical pharmacological aspects. Drugs Aging 1992, 2, 208–221. [Google Scholar] [CrossRef]
- Chaitanya, A.; Pai, V.H.; Mohapatra, A.K.; Ve, R.S. Glaucoma and its association with obstructive sleep apnea: A narrative review. Oman J. Ophthalmol. 2016, 9, 125–134. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Rico, C.; Gutiérrez-Díaz, E.; Mencía-Gutiérrez, E.; Díaz-de-Atauri, M.J.; Blanco, R. Obstructive sleep apnea–hypopnea syndrome (OSAHS) and glaucomatous optic neuropathy. Graefes Arch. Clin. Exp. Ophthalmol. 2014, 252, 1345–1357. [Google Scholar] [CrossRef] [PubMed]
- Ng, F.Y.C.; Song, H.J.J.M.D.; Tan, B.K.J.; Teo, C.B.; Wong, E.T.Y.; Boey, P.Y.; Cheng, C.-Y. Bidirectional association between glaucoma and chronic kidney disease: A systematic review and meta-analysis. eClinicalMedicine 2022, 49, 101498. [Google Scholar] [CrossRef]
- Wong, C.W.; Wong, T.Y.; Cheng, C.Y.; Sabanayagam, C. Kidney and eye diseases: Common risk factors, etiological mechanisms, and pathways. Kidney Int. 2014, 85, 1290–1302. [Google Scholar] [CrossRef] [PubMed]
- Djordjevic-Jocic, J.; Čukuranović, R.; Mitić, B.; Jovanović, P.; Djordjevic, V.; Mihajlović, M.; Veselinovic, A.; Zivkovic, M.; Veljković, S.; Bogdanovic, D.; et al. Ocular and systemic factors associated with glaucoma in chronic kidney disease patients. Int. Urol. Nephrol. 2014, 46, 2191–2198. [Google Scholar] [CrossRef]
- Hoffmanová, I.; Sánchez, D. Metabolic acidosis and anaemia associated with dorzolamide in a patient with impaired renal function. Br. J. Clin. Pharmacol. 2018, 84, 796–799. [Google Scholar] [CrossRef]
- Gani, J.; Perlis, N.; Radomski, S.B. Urologic medications and ophthalmologic side effects: A review. Can. Urol. Assoc. J. 2012, 6, 53–58. [Google Scholar] [CrossRef]
- Bayer, A.U.; Keller, O.N.; Ferrari, F.; Maag, K.P. Association of glaucoma with neurodegenerative diseases with apoptotic cell death: Alzheimer’s disease and Parkinson’s disease. Am. J. Ophthalmol. 2002, 133, 135–137. [Google Scholar] [CrossRef] [PubMed]
- Bayer, A.U.; Ferrari, F.; Erb, C. High Occurrence Rate of Glaucoma among Patients with Alzheimer’s Disease. Eur. Neurol. 2002, 47, 165–168. Available online: https://pubmed.ncbi.nlm.nih.gov/11914555/ (accessed on 13 January 2023).
- Gupta, N.; Greenberg, G.; de Tilly, L.N.; Gray, B.; Polemidiotis, M.; Yücel, Y.H. Atrophy of the lateral geniculate nucleus in human glaucoma detected by magnetic resonance imaging. Br. J. Ophthalmol. 2009, 93, 56–60. [Google Scholar] [CrossRef] [PubMed]
- Gupta, N.; Fong, J.; Ang, L.C.; Yücel, Y.H. Retinal tau pathology in human glaucomas. Can. J. Ophthalmol. J. Can. Ophtalmol. 2008, 43, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Yoneda, S.; Hara, H.; Hirata, A.; Fukushima, M.; Inomata, Y.; Tanihara, H. Vitreous fluid levels of beta-amyloid((1-42)) and tau in patients with retinal diseases. Jpn. J. Ophthalmol. 2005, 49, 106–108. [Google Scholar] [CrossRef]
- Roedl, J.B.; Bleich, S.; Reulbach, U.; Rejdak, R.; Naumann, G.O.H.; Kruse, F.E.; Schlötzer-Schrehardt, U.; Kornhuber, J.; Jünemann, A.G.M. Vitamin deficiency and hyperhomocysteinemia in pseudoexfoliation glaucoma. J. Neural Transm. 2007, 114, 571–575. [Google Scholar] [CrossRef]
- Huang, J.Y.; Su, C.C.; Wang, T.H.; Tsai, I.J. Migraine and increased risk of developing open angle glaucoma: A population-based cohort study. BMC Ophthalmol. 2019, 19, 50. [Google Scholar] [CrossRef]
- Jung, Y.; Han, K.; Wang, S.-M.; Yoon, H.Y.; Moon, J.I. Effect of depressive symptom and depressive disorder on glaucoma incidence in elderly. Sci. Rep. 2021, 11, 5888. [Google Scholar] [CrossRef]
- Shields, C.L.; Materin, M.A.; Shields, J.A.; Gershenbaum, E.; Singh, A.D.; Smith, A. Factors associated with elevated intraocular pressure in eyes with iris melanoma. Br. J. Ophthalmol. 2001, 85, 666–669. [Google Scholar] [CrossRef]
- Wanner, J.B.; Pasquale, L.R. Glaucomas Secondary to Intraocular Melanomas. Semin. Ophthalmol. 2006, 21, 181–189. Available online: https://www.tandfonline.com/doi/abs/10.1080/08820530500351744?journalCode=isio20 (accessed on 13 January 2023). [CrossRef]
- Aponte, E.P.; Diehl, N.; Mohney, B.G. Incidence and clinical characteristics of childhood glaucoma: A population-based study. Arch. Ophthalmol. 2010, 128, 478–482. [Google Scholar] [CrossRef]
- Bermejo, E.; Martínez-Frías, M.L. Congenital eye malformations: Clinical-epidemiological analysis of 1,124,654 consecutive births in Spain. Am. J. Med. Genet. 1998, 75, 497–504. [Google Scholar] [CrossRef]
- Wang, R.; Wiggs, J.L. Common and Rare Genetic Risk Factors for Glaucoma. Cold Spring Harb. Perspect. Med. 2014, 4, a017244. [Google Scholar] [CrossRef]
- Denniston, A.K.O.; Butler, L. Ophthalmic features of Turner’s syndrome. Eye 2004, 18, 680–684. [Google Scholar] [CrossRef]
- Wang, S.; Liu, Y.; Zheng, G. Hypothyroidism as a risk factor for open angle glaucoma: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0186634. [Google Scholar] [CrossRef] [PubMed]
- Tsilou, E.T.; Giri, N.; Weinstein, S.; Mueller, C.; Savage, S.A.; Alter, B.P. Ocular and Orbital Manifestations of the Inherited Bone Marrow Failure Syndromes: Fanconi Anemia and Dyskeratosis Congenita. Ophthalmology 2010, 117, 615–622. [Google Scholar] [CrossRef] [PubMed]
- Matlach, J.; Grehn, F.; Klink, T. Klinefelter syndrome associated with goniodysgenesis. J. Glaucoma 2013, 22, e7–e8. [Google Scholar] [CrossRef]
- Thavikulwat, A.T.; Edward, D.P.; AlDarrab, A.; Vajaranant, T.S. Pathophysiology and management of glaucoma associated with phakomatoses. J. Neurosci. Res. 2019, 97, 57–69. [Google Scholar] [CrossRef] [PubMed]
- Abdolrahimzadeh, S.; Fameli, V.; Mollo, R.; Contestabile, M.T.; Perdicchi, A.; Recupero, S.M. Rare Diseases Leading to Childhood Glaucoma: Epidemiology, Pathophysiogenesis, and Management. Biomed Res. Int. 2015, 2015, 781294. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Medications Associated with Risk of Glaucoma |
|---|
| Systemic sympathomimetics |
|
| Anticholinergic |
|
| Cholinergic |
|
| Antihistamines |
|
| Depression/Anxiety Medications |
|
| Sulfa-Based Drugs |
|
| Others |
|
| Type of Responders | Prevalence | Definition |
|---|---|---|
| High | 4–6% of the Population | IOP > 31 mm Hg or Increase in IOP > 15 mm from baseline |
| Moderate | ⅓ of the population | IOP between 25–31 mm Hg or Increase 6–15 mm Hg from baseline |
| Non-Responders | ⅔ of the population | IOP < 20 mm Hg or Increase < 6 mm from baseline |
| Method of Steroid Administration | Risk of Developing Increased IOP > 20 mm Hg |
|---|---|
| Topical Ocular | Up to 3% in patients taking Difluprednate [19] |
| Periocular (subconjunctival, retrobulbar, sub-tenon) | Up to 7.4% [20] |
| Intravitreal | Up to 33–66% [21,22] |
| Systemic—Oral | Odds ratio of up to 1.41 [23]. Risk is correlated with dosage of corticosteroid |
| Systemic—Inhaled | No increased risk reported in patients without a family or prior history of glaucoma [24]. Odds ratio up to 2.6 in patients with a family history of glaucoma [25]. |
| Inflammatory and Infectious Conditions |
|---|
| Acute retinal necrosis |
| Behcet disease |
| HLA B27—related acute anterior uveitis |
| Juvenile idiopathic arthritis-associated uveitis |
| Sarcoidosis |
| CMV retinitis |
| Congenital rubella |
| Disseminated meningococcemia |
| Hansen disease (leprosy) |
| Herpes virus-associated uveitis |
| Lyme disease |
| Syphilis |
| Toxocariasis |
| Ocular Metastasis from Systemic Malignancies |
|---|
| Cutaneous melanomas |
| Leukemia: |
|
| Lymphoma |
|
| Multiple Myeloma |
| Primary Intraocular Tumors |
|---|
| Uveal melanoma |
| Retinoblastoma |
| Medulloepithelioma |
| Iris melanocytoma |
| Juvenile xanthogranuloma |
| Condition | Mechanism(s) for Development of Glaucoma |
|---|---|
| Trisomy 21 | Congenital glaucoma |
| Trisomy 16–18: Edward Syndrome | Congenital glaucoma |
| Trisomy 13–15: Patau Syndrome | Congenital glaucoma |
| Turner Syndrome | Anterior segment abnormalities [68] |
| Cretinism (Juvenile hypothyroidism) | Deposition of mucopolysaccharides and hyaluronic acids in the trabecular meshwork [69] |
| Diamond–Blackfan Syndrome | Congenital glaucoma [70] |
| Fanconi Anemia | Risk for angle closure due to microphthalmia [70] |
| Ehlers–Danlos Syndrome | Defect in type III collagen |
| Fetal Alcohol Syndrome | Congenital glaucoma |
| Homocystinuria | Anterior displacement of the intraocular lens |
| Kartagener Syndrome | Ciliary dyskinesia |
| Kimmelstiel–Wilson Syndrome | Neovascularization |
| Klinefelter Syndrome | Rare cases of goniodysgenesis/abnormal development of the drainage angle [71] |
| Marfan Syndrome | Lens subluxation, anterior displacement of a maldeveloped intraocular lens |
| Wilms Aniridia | Abnormal development of the drainage angle |
| Neurofibromatosis (von Recklinghausen) | Infiltration of the angle with neurofibromatosis tissue, abnormal development of the drainage angle [72] |
| Pierre Robin Syndrome | Severe congenital myopia |
| Sturge–Weber Syndrome | Abnormal development of the drainage angle [72] |
| Von Hippel–Lindau Disease | Neovascularization, abnormal development of the drainage angle [72] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsu, E.; Desai, M. Glaucoma and Systemic Disease. Life 2023, 13, 1018. https://doi.org/10.3390/life13041018
Hsu E, Desai M. Glaucoma and Systemic Disease. Life. 2023; 13(4):1018. https://doi.org/10.3390/life13041018
Chicago/Turabian StyleHsu, Eugene, and Manishi Desai. 2023. "Glaucoma and Systemic Disease" Life 13, no. 4: 1018. https://doi.org/10.3390/life13041018
APA StyleHsu, E., & Desai, M. (2023). Glaucoma and Systemic Disease. Life, 13(4), 1018. https://doi.org/10.3390/life13041018