
Hippocampal Metabolic Alterations in Amyotrophic Lateral Sclerosis: A Magnetic Resonance Spectroscopy Study

 , ,
, ,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethics Approval
2.2. Participants
2.3. Cognitive Assessment
2.4. MRI Data Acquisition
2.5. MRI Data Analysis
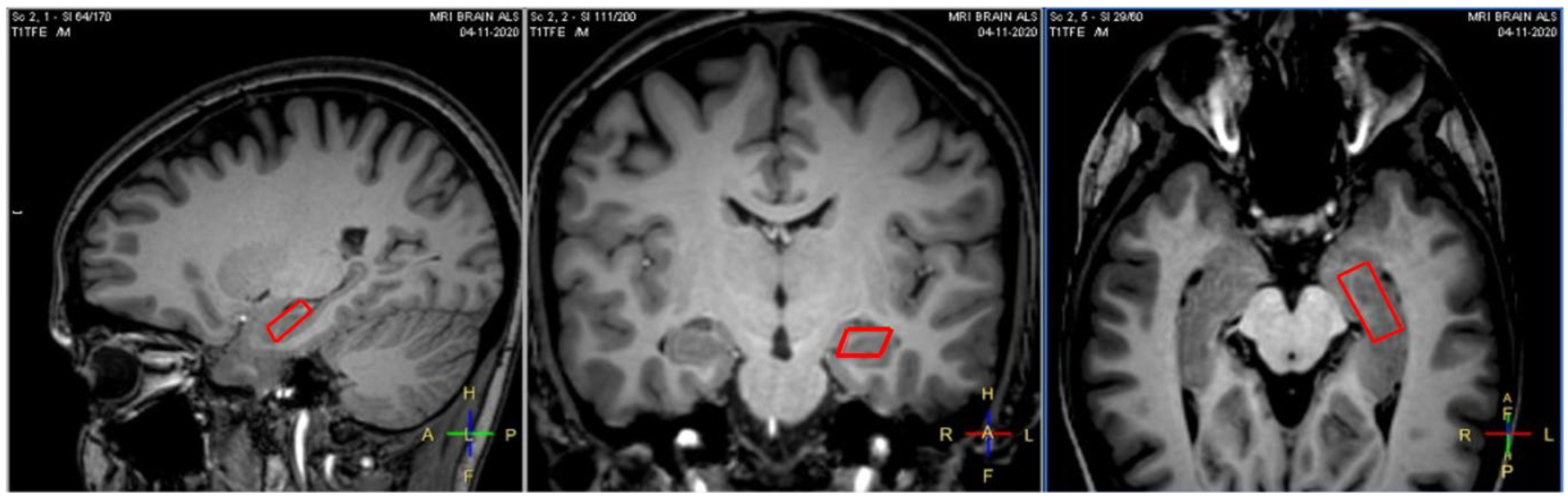
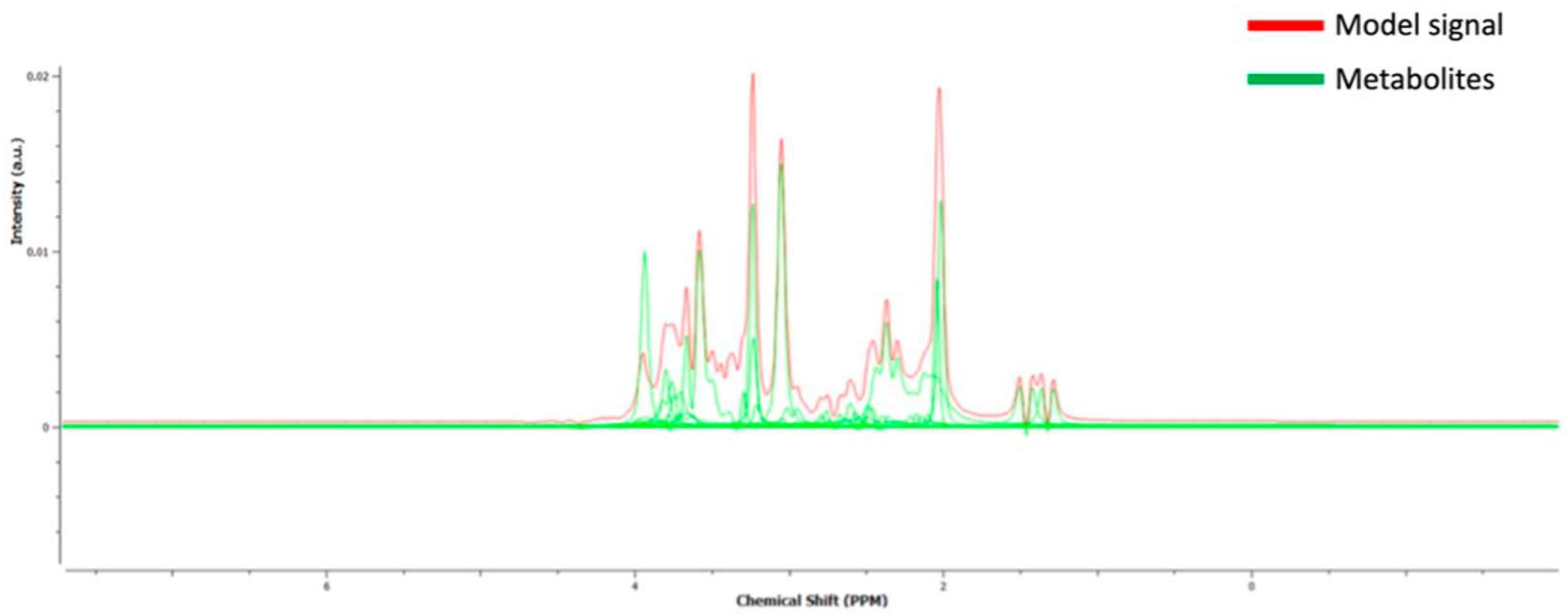
2.5.1. MRS Spectroscopy
2.5.2. Hippocampal GM Analysis
2.5.3. Hippocampal WM Tractography
2.6. Statistical Analyses
3. Results
3.1. Sample Characteristics
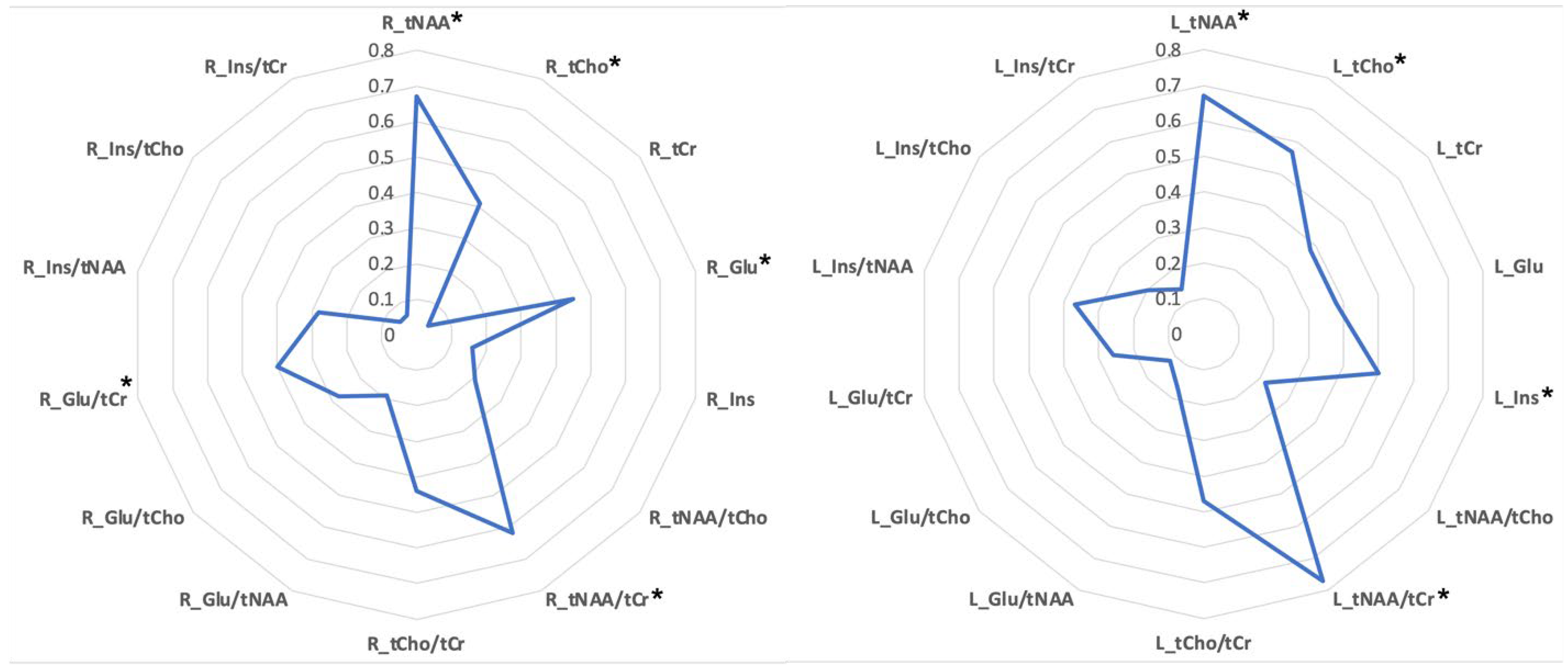
3.2. The MRS Spectroscopy Profile of Hippocampus in ALS
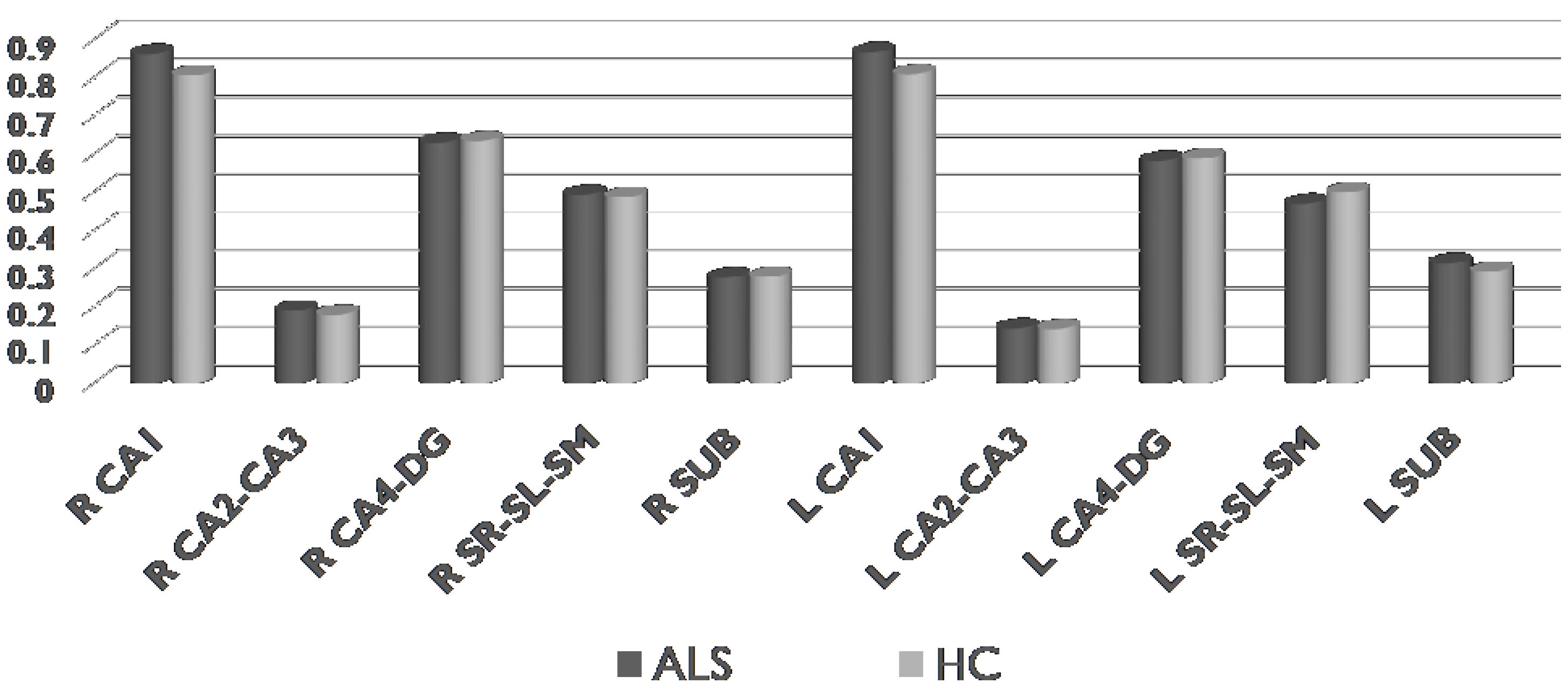
3.3. The GM Profile of Hippocampus in ALS
3.4. The WM Profile of Hippocampus in ALS
3.5. Correlations between MRS Spectroscopy Data and Clinical and Memory-Related Data within ALS
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding

Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Goutman, S.A.; Hardiman, O.; Al-Chalabi, A.; Chio, A.; Savelieff, M.G.; Kiernan, M.C.; Feldman, E.L. Recent advances in the diagnosis and prognosis of amyotrophic lateral sclerosis. Lancet Neurol. 2022, 21, 480–493. [Google Scholar] [CrossRef] [PubMed]
- Simon, N.G.; Turner, M.R.; Vucic, S.; Al-Chalabi, A.; Shefner, J.; Lomen-Hoerth, C.; Kiernan, M.C. Quantifying disease progression in amyotrophic lateral sclerosis. Ann. Neurol. 2014, 76, 643–657. [Google Scholar] [CrossRef]
- Strong, M.J. Revisiting the concept of amyotrophic lateral sclerosis as a multisystems disorder of limited phenotypic expression. Curr. Opin. Neurol. 2017, 30, 599–607. [Google Scholar] [CrossRef] [PubMed]
- Meo, G.; Ferraro, P.M.; Cillerai, M.; Gemelli, C.; Cabona, C.; Zaottini, F.; Roccatagliata, L.; Villani, F.; Schenone, A.; Caponnetto, C. MND Phenotypes Differentiation: The Role of Multimodal Characterization at the Time of Diagnosis. Life 2022, 12, 1506. [Google Scholar] [CrossRef] [PubMed]
- Christidi, F.; Karavasilis, E.; Rentzos, M.; Kelekis, N.; Evdokimidis, I.; Bede, P. Clinical and Radiological Markers of Extra-Motor Deficits in Amyotrophic Lateral Sclerosis. Front. Neurol. 2018, 9, 1005. [Google Scholar] [CrossRef]
- Beeldman, E.; Raaphorst, J.; Twennaar, M.K.; de Visser, M.; Schmand, B.A.; de Haan, R.J. The cognitive profile of ALS: A systematic review and meta-analysis update. J. Neurol. Neurosurg. Psychiatry 2016, 87, 611–619. [Google Scholar] [CrossRef]
- Ferraro, P.M.; Gervino, E.; De Maria, E.; Meo, G.; Ponzano, M.; Pardini, M.; Signori, A.; Schenone, A.; Roccatagliata, L.; Caponnetto, C. Mild behavioral impairment as a potential marker of predementia risk states in motor neuron diseases. Eur. J. Neurol. 2022, 30, 47–56. [Google Scholar] [CrossRef]
- Shing, S.L.H.; Bede, P. The neuroradiology of upper motor neuron degeneration: PLS, HSP, ALS. Amyotroph. Lateral Scler. Front. Degener. 2021, 23, 1–3. [Google Scholar] [CrossRef]
- McKenna, M.C.; Corcia, P.; Couratier, P.; Siah, W.F.; Pradat, P.F.; Bede, P. Frontotemporal Pathology in Motor Neuron Disease Phenotypes: Insights from Neuroimaging. Front. Neurol. 2021, 12, 723450. [Google Scholar] [CrossRef]
- Trojsi, F.; Monsurro, M.R.; Esposito, F.; Tedeschi, G. Widespread structural and functional connectivity changes in amyotrophic lateral sclerosis: Insights from advanced neuroimaging research. Neural Plast. 2012, 2012, 473538. [Google Scholar] [CrossRef]
- Menke, R.A.; Agosta, F.; Grosskreutz, J.; Filippi, M.; Turner, M.R. Neuroimaging Endpoints in Amyotrophic Lateral Sclerosis. Neurother. J. Am. Soc. Exp. Neurother. 2017, 14, 11–23. [Google Scholar] [CrossRef]
- de Carvalho, M. Ensuring continued progress in biomarkers for amyotrophic lateral sclerosis: Another view. Muscle Nerve 2015, 51, 460–461. [Google Scholar] [CrossRef]
- van der Graaf, M. In vivo magnetic resonance spectroscopy: Basic methodology and clinical applications. Eur. Biophys. J. 2010, 39, 527–540. [Google Scholar] [CrossRef]
- Di Costanzo, A.; Trojsi, F.; Tosetti, M.; Schirmer, T.; Lechner, S.M.; Popolizio, T.; Scarabino, T. Proton MR spectroscopy of the brain at 3 T: An update. Eur. Radiol. 2007, 17, 1651–1662. [Google Scholar] [CrossRef]
- Block, W.; Traber, F.; Flacke, S.; Jessen, F.; Pohl, C.; Schild, H. In-vivo proton MR-spectroscopy of the human brain: Assessment of N-acetylaspartate (NAA) reduction as a marker for neurodegeneration. Amino Acids 2002, 23, 317–323. [Google Scholar] [CrossRef]
- Zhu, H.; Barker, P.B. MR spectroscopy and spectroscopic imaging of the brain. Methods Mol. Biol. 2011, 711, 203–226. [Google Scholar] [CrossRef]
- Puts, N.A.; Edden, R.A. In vivo magnetic resonance spectroscopy of GABA: A methodological review. Prog. Nucl. Magn. Reason. Spectrosc. 2012, 60, 29–41. [Google Scholar] [CrossRef]
- Pioro, E.P.; Antel, J.P.; Cashman, N.R.; Arnold, D.L. Detection of cortical neuron loss in motor neuron disease by proton magnetic resonance spectroscopic imaging in vivo. Neurology 1994, 44, 1933–1938. [Google Scholar] [CrossRef]
- Christidi, F.; Karavasilis, E.; Argyropoulos, G.D.; Velonakis, G.; Zouvelou, V.; Murad, A.; Evdokimidis, I.; Rentzos, M.; Seimenis, I.; Bede, P. Neurometabolic Alterations in Motor Neuron Disease: Insights from Magnetic Resonance Spectroscopy. J. Integr. Neurosci. 2022, 21, 87. [Google Scholar] [CrossRef]
- Carew, J.D.; Nair, G.; Pineda-Alonso, N.; Usher, S.; Hu, X.; Benatar, M. Magnetic resonance spectroscopy of the cervical cord in amyotrophic lateral sclerosis. Amyotroph. Lateral Scler. 2011, 12, 185–191. [Google Scholar] [CrossRef]
- Caldwell, S.; Rothman, D.L. (1)H Magnetic Resonance Spectroscopy to Understand the Biological Basis of ALS, Diagnose Patients Earlier, and Monitor Disease Progression. Front. Neurol. 2021, 12, 701170. [Google Scholar] [CrossRef] [PubMed]
- Kalra, S.; Cashman, N.R.; Genge, A.; Arnold, D.L. Recovery of N-acetylaspartate in corticomotor neurons of patients with ALS after riluzole therapy. Neuroreport 1998, 9, 1757–1761. [Google Scholar] [CrossRef] [PubMed]
- Cervo, A.; Cocozza, S.; Sacca, F.; Giorgio, S.; Morra, V.B.; Tedeschi, E.; Marsili, A.; Vacca, G.; Palma, V.; Brunetti, A.; et al. The combined use of conventional MRI and MR spectroscopic imaging increases the diagnostic accuracy in amyotrophic lateral sclerosis. Eur. J. Radiol. 2015, 84, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Charil, A.; Corbo, M.; Filippi, M.; Kesavadas, C.; Agosta, F.; Munerati, E.; Gambini, A.; Comi, G.; Scotti, G.; Falini, A. Structural and metabolic changes in the brain of patients with upper motor neuron disorders: A multiparametric MRI study. Amyotroph. Lateral Scler. 2009, 10, 269–279. [Google Scholar] [CrossRef] [PubMed]
- Foerster, B.R.; Carlos, R.C.; Dwamena, B.A.; Callaghan, B.C.; Petrou, M.; Edden, R.A.; Mohamed, M.A.; Welsh, R.C.; Barker, P.B.; Feldman, E.L.; et al. Multimodal MRI as a diagnostic biomarker for amyotrophic lateral sclerosis. Ann. Clin. Transl. Neurol. 2014, 1, 107–114. [Google Scholar] [CrossRef]
- Bede, P.; Chipika, R.H.; Finegan, E.; Shing, S.L.H.; Doherty, M.A.; Hengeveld, J.C.; Vajda, A.; Hutchinson, S.; Donaghy, C.; McLaughlin, R.L.; et al. Brainstem pathology in amyotrophic lateral sclerosis and primary lateral sclerosis: A longitudinal neuroimaging study. NeuroImage Clin. 2019, 24, 102054. [Google Scholar] [CrossRef]
- Bede, P.; Chipika, R.H.; Christidi, F.; Hengeveld, J.C.; Karavasilis, E.; Argyropoulos, G.D.; Lope, J.; Shing, S.L.H.; Velonakis, G.; Dupuis, L.; et al. Genotype-associated cerebellar profiles in ALS: Focal cerebellar pathology and cerebro-cerebellar connectivity alterations. J. Neurol. Neurosurg. Psychiatry 2021, 92, 1197–1205. [Google Scholar] [CrossRef]
- Chipika, R.H.; Finegan, E.; Shing, S.L.H.; McKenna, M.C.; Christidi, F.; Chang, K.M.; Doherty, M.A.; Hengeveld, J.C.; Vajda, A.; Pender, N.; et al. “Switchboard” malfunction in motor neuron diseases: Selective pathology of thalamic nuclei in amyotrophic lateral sclerosis and primary lateral sclerosis. NeuroImage Clin. 2020, 27, 102300. [Google Scholar] [CrossRef]
- Christidi, F.; Karavasilis, E.; Riederer, F.; Zalonis, I.; Ferentinos, P.; Velonakis, G.; Xirou, S.; Rentzos, M.; Argiropoulos, G.; Zouvelou, V.; et al. Gray matter and white matter changes in non-demented amyotrophic lateral sclerosis patients with or without cognitive impairment: A combined voxel-based morphometry and tract-based spatial statistics whole-brain analysis. Brain Imaging Behav. 2018, 12, 547–563. [Google Scholar] [CrossRef]
- Christidi, F.; Karavasilis, E.; Rentzos, M.; Velonakis, G.; Zouvelou, V.; Xirou, S.; Argyropoulos, G.; Papatriantafyllou, I.; Pantolewn, V.; Ferentinos, P.; et al. Hippocampal pathology in amyotrophic lateral sclerosis: Selective vulnerability of subfields and their associated projections. Neurobiol. Aging 2019, 84, 178–188. [Google Scholar] [CrossRef]
- Abidi, M.; de Marco, G.; Couillandre, A.; Feron, M.; Mseddi, E.; Termoz, N.; Querin, G.; Pradat, P.F.; Bede, P. Adaptive functional reorganization in amyotrophic lateral sclerosis: Coexisting degenerative and compensatory changes. Eur. J. Neurol. 2020, 27, 121–128. [Google Scholar] [CrossRef]
- Proudfoot, M.; Bede, P.; Turner, M.R. Imaging Cerebral Activity in Amyotrophic Lateral Sclerosis. Front. Neurol. 2018, 9, 1148. [Google Scholar] [CrossRef]
- Muller, H.P.; Kassubek, J. MRI-Based Mapping of Cerebral Propagation in Amyotrophic Lateral Sclerosis. Front. Neurosci. 2018, 12, 655. [Google Scholar] [CrossRef]
- Turner, M.R.; Verstraete, E. What does imaging reveal about the pathology of amyotrophic lateral sclerosis? Curr. Neurol. Neurosci. Rep. 2015, 15, 45. [Google Scholar] [CrossRef]
- Quinn, C.; Elman, L.; McCluskey, L.; Hoskins, K.; Karam, C.; Woo, J.H.; Poptani, H.; Wang, S.; Chawla, S.; Kasner, S.E.; et al. Frontal lobe abnormalities on MRS correlate with poor letter fluency in ALS. Neurology 2012, 79, 583–588. [Google Scholar] [CrossRef]
- Abe, K.; Takanashi, M.; Watanabe, Y.; Tanaka, H.; Fujita, N.; Hirabuki, N.; Yanagihara, T. Decrease in N-acetylaspartate/creatine ratio in the motor area and the frontal lobe in amyotrophic lateral sclerosis. Neuroradiology 2001, 43, 537–541. [Google Scholar] [CrossRef]
- Strong, M.J.; Grace, G.M.; Orange, J.B.; Leeper, H.A.; Menon, R.S.; Aere, C. A prospective study of cognitive impairment in ALS. Neurology 1999, 53, 1665–1670. [Google Scholar] [CrossRef]
- Usman, U.; Choi, C.; Camicioli, R.; Seres, P.; Lynch, M.; Sekhon, R.; Johnston, W.; Kalra, S. Mesial prefrontal cortex degeneration in amyotrophic lateral sclerosis: A high-field proton MR spectroscopy study. AJNR Am. J. Neuroradiol. 2011, 32, 1677–1680. [Google Scholar] [CrossRef]
- Sudharshan, N.; Hanstock, C.; Hui, B.; Pyra, T.; Johnston, W.; Kalra, S. Degeneration of the mid-cingulate cortex in amyotrophic lateral sclerosis detected in vivo with MR spectroscopy. AJNR Am. J. Neuroradiol. 2011, 32, 403–407. [Google Scholar] [CrossRef]
- Sharma, K.R.; Saigal, G.; Maudsley, A.A.; Govind, V. 1H MRS of basal ganglia and thalamus in amyotrophic lateral sclerosis. NMR Biomed. 2011, 24, 1270–1276. [Google Scholar] [CrossRef]
- Omer, T.; Finegan, E.; Hutchinson, S.; Doherty, M.; Vajda, A.; McLaughlin, R.L.; Pender, N.; Hardiman, O.; Bede, P. Neuroimaging patterns along the ALS-FTD spectrum: A multiparametric imaging study. Amyotroph. Lateral Scler. Front. Degener. 2017, 18, 611–623. [Google Scholar] [CrossRef] [PubMed]
- Floeter, M.K.; Bageac, D.; Danielian, L.E.; Braun, L.E.; Traynor, B.J.; Kwan, J.Y. Longitudinal imaging in C9orf72 mutation carriers: Relationship to phenotype. NeuroImage Clin. 2016, 12, 1035–1043. [Google Scholar] [CrossRef] [PubMed]
- Bede, P.; Omer, T.; Finegan, E.; Chipika, R.H.; Iyer, P.M.; Doherty, M.A.; Vajda, A.; Pender, N.; McLaughlin, R.L.; Hutchinson, S.; et al. Connectivity-based characterisation of subcortical grey matter pathology in frontotemporal dementia and ALS: A multimodal neuroimaging study. Brain Imaging Behav. 2018, 12, 1696–1707. [Google Scholar] [CrossRef] [PubMed]
- Abidi, M.; de Marco, G.; Grami, F.; Termoz, N.; Couillandre, A.; Querin, G.; Bede, P.; Pradat, P.F. Neural Correlates of Motor Imagery of Gait in Amyotrophic Lateral Sclerosis. J. Magn. Reason. Imaging 2021, 53, 223–233. [Google Scholar] [CrossRef]
- Bede, P.; Hardiman, O. Longitudinal structural changes in ALS: A three time-point imaging study of white and gray matter degeneration. Amyotroph. Lateral Scler. Front. Degener. 2018, 19, 232–241. [Google Scholar] [CrossRef]
- Christidi, F.; Karavasilis, E.; Velonakis, G.; Rentzos, M.; Zambelis, T.; Zouvelou, V.; Xirou, S.; Ferentinos, P.; Efstathopoulos, E.; Kelekis, N.; et al. Motor and extra-motor gray matter integrity may underlie neurophysiologic parameters of motor function in amyotrophic lateral sclerosis: A combined voxel-based morphometry and transcranial stimulation study. Brain Imaging Behav. 2018, 12, 1730–1741. [Google Scholar] [CrossRef]
- Burke, T.; Pinto-Grau, M.; Lonergan, K.; Bede, P.; O’Sullivan, M.; Heverin, M.; Vajda, A.; McLaughlin, R.L.; Pender, N.; Hardiman, O. A Cross-sectional population-based investigation into behavioral change in amyotrophic lateral sclerosis: Subphenotypes, staging, cognitive predictors, and survival. Ann. Clin. Transl. Neurol. 2017, 4, 305–317. [Google Scholar] [CrossRef]
- Brettschneider, J.; Del Tredici, K.; Toledo, J.B.; Robinson, J.L.; Irwin, D.J.; Grossman, M.; Suh, E.; Van Deerlin, V.M.; Wood, E.M.; Baek, Y.; et al. Stages of pTDP-43 pathology in amyotrophic lateral sclerosis. Ann. Neurol. 2013, 74, 20–38. [Google Scholar] [CrossRef]
- Brettschneider, J.; Libon, D.J.; Toledo, J.B.; Xie, S.X.; McCluskey, L.; Elman, L.; Geser, F.; Lee, V.M.; Grossman, M.; Trojanowski, J.Q. Microglial activation and TDP-43 pathology correlate with executive dysfunction in amyotrophic lateral sclerosis. Acta Neuropathol. 2012, 123, 395–407. [Google Scholar] [CrossRef]
- Geser, F.; Prvulovic, D.; O’Dwyer, L.; Hardiman, O.; Bede, P.; Bokde, A.L.; Trojanowski, J.Q.; Hampel, H. On the development of markers for pathological TDP-43 in amyotrophic lateral sclerosis with and without dementia. Prog. Neurobiol. 2011, 95, 649–662. [Google Scholar] [CrossRef]
- Kassubek, J.; Muller, H.P.; Del Tredici, K.; Brettschneider, J.; Pinkhardt, E.H.; Lule, D.; Bohm, S.; Braak, H.; Ludolph, A.C. Diffusion tensor imaging analysis of sequential spreading of disease in amyotrophic lateral sclerosis confirms patterns of TDP-43 pathology. Brain J. Neurol. 2014, 137, 1733–1740. [Google Scholar] [CrossRef]
- Christidi, F.; Karavasilis, E.; Velonakis, G.; Ferentinos, P.; Rentzos, M.; Kelekis, N.; Evdokimidis, I.; Bede, P. The Clinical and Radiological Spectrum of Hippocampal Pathology in Amyotrophic Lateral Sclerosis. Front. Neurol. 2018, 9, 523. [Google Scholar] [CrossRef]
- Liu, S.; Ren, Q.; Gong, G.; Sun, Y.; Zhao, B.; Ma, X.; Zhang, N.; Zhong, S.; Lin, Y.; Wang, W.; et al. Hippocampal subfield and anterior-posterior segment volumes in patients with sporadic amyotrophic lateral sclerosis. NeuroImage Clin. 2021, 32, 102816. [Google Scholar] [CrossRef]
- Westeneng, H.J.; Verstraete, E.; Walhout, R.; Schmidt, R.; Hendrikse, J.; Veldink, J.H.; van den Heuvel, M.P.; van den Berg, L.H. Subcortical structures in amyotrophic lateral sclerosis. Neurobiol. Aging 2015, 36, 1075–1082. [Google Scholar] [CrossRef]
- Trojsi, F.; Di Nardo, F.; Caiazzo, G.; Siciliano, M.; D’Alvano, G.; Ferrantino, T.; Passaniti, C.; Ricciardi, D.; Esposito, S.; Lavorgna, L.; et al. Hippocampal connectivity in Amyotrophic Lateral Sclerosis (ALS): More than Papez circuit impairment. Brain Imaging Behav. 2021, 15, 2126–2138. [Google Scholar] [CrossRef]
- Christidi, F.; Karavasilis, E.; Rentzos, M.; Argyropoulos, G.; Velonakis, G.; Zouvelou, V.; Xirou, S.; Zambelis, T.; Bede, P.; Kelekis, N.; et al. Association between the anatomico-behavioral features of hippocampus and rate of disease progression in amyotrophic lateral sclerosis: A multiparametric study [article in Greek]. Nevrologia 2019, 28, 44. [Google Scholar]
- Braak, H.; Brettschneider, J.; Ludolph, A.C.; Lee, V.M.; Trojanowski, J.Q.; Del Tredici, K. Amyotrophic lateral sclerosis—A model of corticofugal axonal spread. Nat. Rev. Neurol. 2013, 9, 708–714. [Google Scholar] [CrossRef]
- Takeda, T.; Uchihara, T.; Arai, N.; Mizutani, T.; Iwata, M. Progression of hippocampal degeneration in amyotrophic lateral sclerosis with or without memory impairment: Distinction from Alzheimer disease. Acta Neuropathol. 2009, 117, 35–44. [Google Scholar] [CrossRef]
- Takeda, T.; Uchihara, T.; Mochizuki, Y.; Mizutani, T.; Iwata, M. Memory deficits in amyotrophic lateral sclerosis patients with dementia and degeneration of the perforant pathway A clinicopathological study. J. Neurol. Sci. 2007, 260, 225–230. [Google Scholar] [CrossRef]
- Bede, P.; Elamin, M.; Byrne, S.; McLaughlin, R.L.; Kenna, K.; Vajda, A.; Pender, N.; Bradley, D.G.; Hardiman, O. Basal ganglia involvement in amyotrophic lateral sclerosis. Neurology 2013, 81, 2107–2115. [Google Scholar] [CrossRef]
- Machts, J.; Loewe, K.; Kaufmann, J.; Jakubiczka, S.; Abdulla, S.; Petri, S.; Dengler, R.; Heinze, H.J.; Vielhaber, S.; Schoenfeld, M.A.; et al. Basal ganglia pathology in ALS is associated with neuropsychological deficits. Neurology 2015, 85, 1301–1309. [Google Scholar] [CrossRef] [PubMed]
- Bede, P.; Iyer, P.M.; Finegan, E.; Omer, T.; Hardiman, O. Virtual brain biopsies in amyotrophic lateral sclerosis: Diagnostic classification based on in vivo pathological patterns. NeuroImage Clin. 2017, 15, 653–658. [Google Scholar] [CrossRef] [PubMed]
- McCombe, P.A.; Wray, N.R.; Henderson, R.D. Extra-motor abnormalities in amyotrophic lateral sclerosis: Another layer of heterogeneity. Expert Rev. Neurother. 2017, 17, 561–577. [Google Scholar] [CrossRef] [PubMed]
- Verber, N.S.; Shepheard, S.R.; Sassani, M.; McDonough, H.E.; Moore, S.A.; Alix, J.J.P.; Wilkinson, I.D.; Jenkins, T.M.; Shaw, P.J. Biomarkers in Motor Neuron Disease: A State of the Art Review. Front. Neurol. 2019, 10, 291. [Google Scholar] [CrossRef]
- Bede, P.; Hardiman, O. Lessons of ALS imaging: Pitfalls and future directions—A critical review. NeuroImage Clin. 2014, 4, 436–443. [Google Scholar] [CrossRef]
- Mitsumoto, H.; Brooks, B.R.; Silani, V. Clinical trials in amyotrophic lateral sclerosis: Why so many negative trials and how can trials be improved? Lancet Neurol. 2014, 13, 1127–1138. [Google Scholar] [CrossRef]
- Ludolph, A.; Drory, V.; Hardiman, O.; Nakano, I.; Ravits, J.; Robberecht, W.; Shefner, J.; WFN Research Group On ALS/MND. A revision of the El Escorial criteria—2015. Amyotroph. Lateral Scler. Front. Degener. 2015, 16, 291–292. [Google Scholar] [CrossRef]
- Kourtesis, P.; Christidi, F.; Margioti, E.; Demenega, C.; Rentzos, M.; Evdokimidis, I.; Abrahams, S. The Edinburgh cognitive and behavioral amyotrophic lateral sclerosis screen (ECAS): Sensitivity in differentiating between ALS and Alzheimer’s disease in a Greek population. Amyotroph. Lateral Scler. Front. Degener. 2020, 21, 78–85. [Google Scholar] [CrossRef]
- Abrahams, S.; Newton, J.; Niven, E.; Foley, J.; Bak, T.H. Screening for cognition and behaviour changes in ALS. Amyotroph. Lateral Scler. Front. Degener. 2014, 15, 9–14. [Google Scholar] [CrossRef]
- Wilson, M.; Reynolds, G.; Kauppinen, R.A.; Arvanitis, T.N.; Peet, A.C. A constrained least-squares approach to the automated quantitation of in vivo (1)H magnetic resonance spectroscopy data. Magn. Reason. Med. 2011, 65, 1–12. [Google Scholar] [CrossRef]
- Gill, S.K.; Wilson, M.; Davies, N.P.; MacPherson, L.; English, M.; Arvanitis, T.N.; Peet, A.C. Diagnosing relapse in children’s brain tumors using metabolite profiles. Neuro-Oncology 2014, 16, 156–164. [Google Scholar] [CrossRef]
- Barker, P.B.; Soher, B.J.; Blackband, S.J.; Chatham, J.C.; Mathews, V.P.; Bryan, R.N. Quantitation of proton NMR spectra of the human brain using tissue water as an internal concentration reference. NMR Biomed. 1993, 6, 89–94. [Google Scholar] [CrossRef]
- Christiansen, P.; Henriksen, O.; Stubgaard, M.; Gideon, P.; Larsson, H.B. In vivo quantification of brain metabolites by 1H-MRS using water as an internal standard. Magn. Reason. Imaging 1993, 11, 107–118. [Google Scholar] [CrossRef]
- Mikkelsen, M.; Rimbault, D.L.; Barker, P.B.; Bhattacharyya, P.K.; Brix, M.K.; Buur, P.F.; Cecil, K.M.; Chan, K.L.; Chen, D.Y.; Craven, A.R.; et al. Big GABA II: Water-referenced edited MR spectroscopy at 25 research sites. Neuroimage 2019, 191, 537–548. [Google Scholar] [CrossRef]
- Wilson, M. Adaptive baseline fitting for 1H MR spectroscopy analysis. Magn. Reason. Med. 2021, 85, 13–29. [Google Scholar] [CrossRef]
- Dhamala, E.; Abdelkefi, I.; Nguyen, M.; Hennessy, T.J.; Nadeau, H.; Near, J. Validation of in vivo MRS measures of metabolite concentrations in the human brain. NMR Biomed. 2019, 32, e4058. [Google Scholar] [CrossRef]
- Romero, J.E.; Coupe, P.; Manjon, J.V. HIPS: A new hippocampus subfield segmentation method. NeuroImage 2017, 163, 286–295. [Google Scholar] [CrossRef]
- Romero, J.E.; Coupe, P.; Manjón, J.V. High Resolution Hippocampus Subfield Segmentation Using Multispectral Multiatlas Patch-Based Label Fusion. In Patch-Based Techniques in Medical Imaging, Proceedings of the International Workshop on Patch-based Techniques in Medical Imaging, Athens, Greece, 17 October 2016; Springer: Berlin/Heidelberg, Germany, 2016; Volume 9993, pp. 117–124. [Google Scholar] [CrossRef]
- Winterburn, J.L.; Pruessner, J.C.; Chavez, S.; Schira, M.M.; Lobaugh, N.J.; Voineskos, A.N.; Chakravarty, M.M. A novel in vivo atlas of human hippocampal subfields using high-resolution 3 T magnetic resonance imaging. NeuroImage 2013, 74, 254–265. [Google Scholar] [CrossRef]
- Christidi, F.; Karavasilis, E.; Zalonis, I.; Ferentinos, P.; Giavri, Z.; Wilde, E.A.; Xirou, S.; Rentzos, M.; Zouvelou, V.; Velonakis, G.; et al. Memory-related white matter tract integrity in amyotrophic lateral sclerosis: An advanced neuroimaging and neuropsychological study. Neurobiol. Aging 2017, 49, 69–78. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Lawrence Erlbaum Associates: New York, NY, USA, 1988. [Google Scholar]
- Kalra, S. Magnetic Resonance Spectroscopy in ALS. Front. Neurol. 2019, 10, 482. [Google Scholar] [CrossRef]
- Mader, I.; Rauer, S.; Gall, P.; Klose, U. (1)H MR spectroscopy of inflammation, infection and ischemia of the brain. Eur. J. Radiol. 2008, 67, 250–257. [Google Scholar] [CrossRef] [PubMed]
- Groenendaal, F.; Veenhoven, R.H.; van der Grond, J.; Jansen, G.H.; Witkamp, T.D.; de Vries, L.S. Cerebral lactate and N-acetyl-aspartate/choline ratios in asphyxiated full-term neonates demonstrated in vivo using proton magnetic resonance spectroscopy. Pediatr. Res. 1994, 35, 148–151. [Google Scholar] [CrossRef] [PubMed]
- Costello, E.; Rooney, J.; Pinto-Grau, M.; Burke, T.; Elamin, M.; Bede, P.; McMackin, R.; Dukic, S.; Vajda, A.; Heverin, M.; et al. Cognitive reserve in amyotrophic lateral sclerosis (ALS): A population-based longitudinal study. J. Neurol. Neurosurg. Psychiatry 2021, 92, 460–465. [Google Scholar] [CrossRef] [PubMed]
- Consonni, M.; Bella, E.D.; Bersano, E.; Telesca, A.; Lauria, G. Cognitive reserve is associated with altered clinical expression in amyotrophic lateral sclerosis. Amyotroph. Lateral Scler. Front. Degener. 2021, 22, 237–247. [Google Scholar] [CrossRef]
- Temp, A.G.M.; Prudlo, J.; Vielhaber, S.; Machts, J.; Hermann, A.; Teipel, S.J.; Kasper, E. Cognitive reserve and regional brain volume in amyotrophic lateral sclerosis. Cortex 2021, 139, 240–248. [Google Scholar] [CrossRef]
- Bede, P.; Bogdahn, U.; Lope, J.; Chang, K.M.; Xirou, S.; Christidi, F. Degenerative and regenerative processes in amyotrophic lateral sclerosis: Motor reserve, adaptation and putative compensatory changes. Neural. Regen. Res. 2021, 16, 1208–1209. [Google Scholar] [CrossRef]
- Schuster, C.; Elamin, M.; Hardiman, O.; Bede, P. The segmental diffusivity profile of amyotrophic lateral sclerosis associated white matter degeneration. Eur. J. Neurol. 2016, 23, 1361–1371. [Google Scholar] [CrossRef]
- Verstraete, E.; Turner, M.R.; Grosskreutz, J.; Filippi, M.; Benatar, M. Mind the gap: The mismatch between clinical and imaging metrics in ALS. Amyotroph. Lateral Scler. Front. Degener. 2015, 16, 524–529. [Google Scholar] [CrossRef]
- Sass, K.J.; Sass, A.; Westerveld, M.; Lencz, T.; Novelly, R.A.; Kim, J.H.; Spencer, D.D. Specificity in the correlation of verbal memory and hippocampal neuron loss: Dissociation of memory, language, and verbal intellectual ability. J. Clin. Exp. Neuropsychol. 1992, 14, 662–672. [Google Scholar] [CrossRef]
- Ezzati, A.; Katz, M.J.; Zammit, A.R.; Lipton, M.L.; Zimmerman, M.E.; Sliwinski, M.J.; Lipton, R.B. Differential association of left and right hippocampal volumes with verbal episodic and spatial memory in older adults. Neuropsychologia 2016, 93, 380–385. [Google Scholar] [CrossRef]
- Raaphorst, J.; van Tol, M.J.; de Visser, M.; van der Kooi, A.J.; Majoie, C.B.; van den Berg, L.H.; Schmand, B.; Veltman, D.J. Prose memory impairment in amyotrophic lateral sclerosis patients is related to hippocampus volume. Eur. J. Neurol. 2015, 22, 547–554. [Google Scholar] [CrossRef]
- Nyberg, L.; McIntosh, A.R.; Cabeza, R.; Habib, R.; Houle, S.; Tulving, E. General and specific brain regions involved in encoding and retrieval of events: What, where, and when. Proc. Natl. Acad. Sci. USA 1996, 93, 11280–11285. [Google Scholar] [CrossRef]
- Chipika, R.H.; Finegan, E.; Shing, S.L.H.; Hardiman, O.; Bede, P. Tracking a Fast-Moving Disease: Longitudinal Markers, Monitoring, and Clinical Trial Endpoints in ALS. Front. Neurol. 2019, 10, 229. [Google Scholar] [CrossRef]
- Shing, S.L.H.; McKenna, M.C.; Siah, W.F.; Chipika, R.H.; Hardiman, O.; Bede, P. The imaging signature of C9orf72 hexanucleotide repeat expansions: Implications for clinical trials and therapy development. Brain Imaging Behav. 2021, 15, 2693–2719. [Google Scholar] [CrossRef]
- Bede, P.; Murad, A.; Lope, J.; Shing, S.L.H.; Finegan, E.; Chipika, R.H.; Hardiman, O.; Chang, K.M. Phenotypic categorisation of individual subjects with motor neuron disease based on radiological disease burden patterns: A machine-learning approach. J. Neurol. Sci. 2021, 432, 120079. [Google Scholar] [CrossRef]
- Bede, P.; Chang, K.M.; Tan, E.L. Machine-learning in motor neuron diseases: Prospects and pitfalls. Eur. J. Neurol. 2022, 29, 2555–2556. [Google Scholar] [CrossRef]
- Grollemund, V.; Pradat, P.F.; Querin, G.; Delbot, F.; Le Chat, G.; Pradat-Peyre, J.F.; Bede, P. Machine Learning in Amyotrophic Lateral Sclerosis: Achievements, Pitfalls, and Future Directions. Front. Neurosci. 2019, 13, 135. [Google Scholar] [CrossRef]
- Bede, P.; Querin, G.; Pradat, P.F. The changing landscape of motor neuron disease imaging: The transition from descriptive studies to precision clinical tools. Curr. Opin. Neurol. 2018, 31, 431–438. [Google Scholar] [CrossRef]
- Grollemund, V.; Chat, G.L.; Secchi-Buhour, M.S.; Delbot, F.; Pradat-Peyre, J.F.; Bede, P.; Pradat, P.F. Development and validation of a 1-year survival prognosis estimation model for Amyotrophic Lateral Sclerosis using manifold learning algorithm UMAP. Sci. Rep. 2020, 10, 13378. [Google Scholar] [CrossRef]
- Grollemund, V.; Le Chat, G.; Secchi-Buhour, M.S.; Delbot, F.; Pradat-Peyre, J.F.; Bede, P.; Pradat, P.F. Manifold learning for amyotrophic lateral sclerosis functional loss assessment: Development and validation of a prognosis model. J. Neurol. 2021, 268, 825–850. [Google Scholar] [CrossRef]
- Westeneng, H.J.; Debray, T.P.A.; Visser, A.E.; van Eijk, R.P.A.; Rooney, J.P.K.; Calvo, A.; Martin, S.; McDermott, C.J.; Thompson, A.G.; Pinto, S.; et al. Prognosis for patients with amyotrophic lateral sclerosis: Development and validation of a personalised prediction model. Lancet Neurol. 2018, 17, 423–433. [Google Scholar] [CrossRef] [PubMed]
- Bede, P.; Murad, A.; Hardiman, O. Pathological neural networks and artificial neural networks in ALS: Diagnostic classification based on pathognomonic neuroimaging features. J. Neurol. 2021, 269, 2440–2452. [Google Scholar] [CrossRef] [PubMed]
- Schuster, C.; Hardiman, O.; Bede, P. Survival prediction in Amyotrophic lateral sclerosis based on MRI measures and clinical characteristics. BMC Neurol. 2017, 17, 73. [Google Scholar] [CrossRef] [PubMed]
- McKenna, M.C.; Murad, A.; Huynh, W.; Lope, J.; Bede, P. The changing landscape of neuroimaging in frontotemporal lobar degeneration: From group-level observations to single-subject data interpretation. Expert Rev. Neurother. 2022, 22, 179–207. [Google Scholar] [CrossRef] [PubMed]
- Schuster, C.; Hardiman, O.; Bede, P. Development of an Automated MRI-Based Diagnostic Protocol for Amyotrophic Lateral Sclerosis Using Disease-Specific Pathognomonic Features: A Quantitative Disease-State Classification Study. PLoS ONE 2016, 11, e0167331. [Google Scholar] [CrossRef]
- Tan, H.H.G.; Westeneng, H.J.; Nitert, A.D.; van Veenhuijzen, K.; Meier, J.M.; van der Burgh, H.K.; van Zandvoort, M.J.E.; van Es, M.A.; Veldink, J.H.; van den Berg, L.H. MRI clustering reveals three ALS subtypes with unique neurodegeneration patterns. Ann. Neurol. 2022, 92, 1030–1045. [Google Scholar] [CrossRef]
- Dukic, S.; McMackin, R.; Costello, E.; Metzger, M.; Buxo, T.; Fasano, A.; Chipika, R.; Pinto-Grau, M.; Schuster, C.; Hammond, M.; et al. Resting-state EEG reveals four subphenotypes of amyotrophic lateral sclerosis. Brain J. Neurol. 2022, 145, 621–631. [Google Scholar] [CrossRef]
- Bede, P.; Murad, A.; Lope, J.; Hardiman, O.; Chang, K.M. Clusters of anatomical disease-burden patterns in ALS: A data-driven approach confirms radiological subtypes. J. Neurol. 2022, 269, 4404–4413. [Google Scholar] [CrossRef]
- Bede, P.; Lope, J. Biomarker development in amyotrophic lateral sclerosis: Challenges and viable strategies. Eur. J. Neurol. 2022, 29, 1867–1868. [Google Scholar] [CrossRef]
- Muller, H.P.; Turner, M.R.; Grosskreutz, J.; Abrahams, S.; Bede, P.; Govind, V.; Prudlo, J.; Ludolph, A.C.; Filippi, M.; Kassubek, J. A large-scale multicentre cerebral diffusion tensor imaging study in amyotrophic lateral sclerosis. J. Neurol. Neurosurg. Psychiatry 2016, 87, 570–579. [Google Scholar] [CrossRef]
- Bharti, K.; Khan, M.; Beaulieu, C.; Graham, S.J.; Briemberg, H.; Frayne, R.; Genge, A.; Korngut, L.; Zinman, L.; Kalra, S. Involvement of the dentate nucleus in the pathophysiology of amyotrophic lateral sclerosis: A multi-center and multi-modal neuroimaging study. NeuroImage. Clin. 2020, 28, 102385. [Google Scholar] [CrossRef]
- Bharti, K.; Graham, S.J.; Benatar, M.; Briemberg, H.; Chenji, S.; Dupré, N.; Dionne, A.; Frayne, R.; Genge, A.; Korngut, L.; et al. Functional alterations in large-scale resting-state networks of amyotrophic lateral sclerosis: A multi-site study across Canada and the United States. PLoS ONE 2022, 17, e0269154. [Google Scholar] [CrossRef]
- Vora, M.; Kumar, S.; Sharma, S.; Sharma, S.; Makhaik, S.; Sood, R.G. Advanced magnetic resonance neuroimaging in bulbar and limb onset early amyotrophic lateral sclerosis. J. Neurosci. Rural. Pract. 2016, 7, 102–108. [Google Scholar] [CrossRef]
- Govind, V.; Sharma, K.R.; Maudsley, A.A.; Arheart, K.L.; Saigal, G.; Sheriff, S. Comprehensive evaluation of corticospinal tract metabolites in amyotrophic lateral sclerosis using whole-brain 1H MR spectroscopy. PLoS ONE 2012, 7, e35607. [Google Scholar] [CrossRef]
- Stagg, C.J.; Knight, S.; Talbot, K.; Jenkinson, M.; Maudsley, A.A.; Turner, M.R. Whole-brain magnetic resonance spectroscopic imaging measures are related to disability in ALS. Neurology 2013, 80, 610–615. [Google Scholar] [CrossRef]
- Younis, S.; Hougaard, A.; Christensen, C.E.; Vestergaard, M.B.; Petersen, E.T.; Boer, V.O.; Paulson, O.B.; Ashina, M.; Marsman, A.; Larsson, H.B.W. Feasibility of Glutamate and GABA Detection in Pons and Thalamus at 3T and 7T by Proton Magnetic Resonance Spectroscopy. Front. Neurosci. 2020, 14, 559314. [Google Scholar] [CrossRef]
- Gonen, O.M.; Moffat, B.A.; Kwan, P.; O’Brien, T.J.; Desmond, P.M.; Lui, E. Reproducibility of Glutamate, Glutathione, and GABA Measurements in vivo by Single-Voxel STEAM Magnetic Resonance Spectroscopy at 7-Tesla in Healthy Individuals. Front. Neurosci. 2020, 14, 566643. [Google Scholar] [CrossRef]
- Tkac, I.; Andersen, P.; Adriany, G.; Merkle, H.; Ugurbil, K.; Gruetter, R. In vivo 1H NMR spectroscopy of the human brain at 7 T. Magn. Reason. Med. 2001, 46, 451–456. [Google Scholar] [CrossRef]
- Chipika, R.H.; Mulkerrin, G.; Murad, A.; Lope, J.; Hardiman, O.; Bede, P. Alterations in somatosensory, visual and auditory pathways in amyotrophic lateral sclerosis: An under-recognised facet of ALS. J. Integr. Neurosci. 2022, 21, 88. [Google Scholar] [CrossRef]
- Rubio, M.A.; Herrando-Grabulosa, M.; Navarro, X. Sensory Involvement in Amyotrophic Lateral Sclerosis. Int. J. Mol. Sci. 2022, 23, 15521. [Google Scholar] [CrossRef]
- Bede, P.; Iyer, P.M.; Schuster, C.; Elamin, M.; McLaughlin, R.L.; Kenna, K.; Hardiman, O. The selective anatomical vulnerability of ALS: ‘disease-defining’ and ‘disease-defying’ brain regions. Amyotroph. Lateral Scler. Front. Degener. 2016, 17, 561–570. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ALS (n = 12) | HC (n = 12) | Statistical Difference | |
|---|---|---|---|
| Age (years) | 59.83 ± 10.53 | 52.92 ± 9.37 | 0.103 |
| Sex (M/F) | 7/5 | 5/7 | 0.414 |
| Education (years) | 14.08 ± 2.81 | 14.17 ± 2.59 | 0.940 |
| Handedness (Rt/Lt) | 12/0 | 12/0 | - |
| MMSE | 28.25 ± 1.22 | 28.50 ± 1.17 | 0.613 |
| Disease duration from symptom onset (m) | 25.33 ± 22.74 | - | - |
| ALSFRS-R | 38.25 ± 7.89 | - | - |
| ALS (n = 12) | HC (n = 12) | p-Value | |
|---|---|---|---|
| Right hippocampus | |||
| tNAA | 8.71 ± 1.29 | 6.25 ± 1.34 | <0.001 |
| tCho | 2.33 ± 0.66 | 1.95 ± 0.44 | 0.044 |
| tCr | 8.58 ± 1.34 | 8.85 ± 2.58 | 0.886 |
| Glu | 9.14 ± 3.20 | 5.86 ± 3.50 | 0.028 |
| Ins | 11.32 ± 2.37 | 10.01 ± 3.89 | 0.433 |
| tNAA/tCho | 4.04 ± 1.32 | 3.36 ± 0.97 | 0.311 |
| tNAA/tCr | 1.02 ± 0.12 | 0.76 ± 0.25 | 0.001 |
| tCho/tCr | 0.27 ± 0.06 | 0.23 ± 0.05 | 0.033 |
| Glu/tNAA | 1.07 ± 0.40 | 0.88 ± 0.47 | 0.371 |
| Glu/tCho | 4.49 ± 2.52 | 3.11 ± 1.90 | 0.175 |
| Glu/tCr | 1.09 ± 0.42 | 0.69 ± 0.40 | 0.051 |
| Ins/tNAA | 1.35 ± 0.49 | 1.65 ± 0.65 | 0.178 |
| Ins/tCho | 5.91 ± 4.71 | 5.57 ± 3.01 | 0.799 |
| Ins/tCr | 1.37 ± 0.45 | 1.24 ± 0.58 | 0.799 |
| Left hippocampus | |||
| tNAA | 11.45 ± 4.31 | 5.57 ± 2.22 | <0.001 |
| tCho | 3.00 ±1.50 | 1.82 ± 0.78 | 0.004 |
| tCr | 9.34 ± 4.03 | 7.35 ± 1.82 | 0.066 |
| Glu | 11.26 ± 9.24 | 5.82 ± 2.59 | 0.065 |
| Ins | 12.34 ± 4.04 | 8.52 ± 1.96 | 0.013 |
| tNAA/tCho | 5.03 ± 4.12 | 3.29 ± 1.31 | 0.284 |
| tNAA/tCr | 1.27 ± 0.17 | 0.78 ± 0.31 | <0.001 |
| tCho/tCr | 0.31 ± 0.08 | 0.24 ± 0.07 | 0.020 |
| Glu/tNAA | 0.90 ± 0.54 | 1.27 ± 0.88 | 0.431 |
| Glu/tCho | 3.35 ± 2.15 | 3.74 ± 1.94 | 0.578 |
| Glu/tCr | 1.09 ± 0.66 | 0.83 ± 0.37 | 0.214 |
| Ins/tNAA | 1.37 ± 1.21 | 2.10 ± 2.00 | 0.075 |
| Ins/tCho | 11.26 ± 24.98 | 5.66 ± 2.84 | 0.342 |
| Ins/tCr | 1.87 ± 2.06 | 1.23 ± 0.39 | 0.514 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Christidi, F.; Argyropoulos, G.D.; Karavasilis, E.; Velonakis, G.; Zouvelou, V.; Kourtesis, P.; Pantoleon, V.; Tan, E.L.; Daponte, A.; Aristeidou, S.; et al. Hippocampal Metabolic Alterations in Amyotrophic Lateral Sclerosis: A Magnetic Resonance Spectroscopy Study. Life 2023, 13, 571. https://doi.org/10.3390/life13020571
Christidi F, Argyropoulos GD, Karavasilis E, Velonakis G, Zouvelou V, Kourtesis P, Pantoleon V, Tan EL, Daponte A, Aristeidou S, et al. Hippocampal Metabolic Alterations in Amyotrophic Lateral Sclerosis: A Magnetic Resonance Spectroscopy Study. Life. 2023; 13(2):571. https://doi.org/10.3390/life13020571
Chicago/Turabian StyleChristidi, Foteini, Georgios D. Argyropoulos, Efstratios Karavasilis, Georgios Velonakis, Vasiliki Zouvelou, Panagiotis Kourtesis, Varvara Pantoleon, Ee Ling Tan, Ariadne Daponte, Stavroula Aristeidou, and et al. 2023. "Hippocampal Metabolic Alterations in Amyotrophic Lateral Sclerosis: A Magnetic Resonance Spectroscopy Study" Life 13, no. 2: 571. https://doi.org/10.3390/life13020571
APA StyleChristidi, F., Argyropoulos, G. D., Karavasilis, E., Velonakis, G., Zouvelou, V., Kourtesis, P., Pantoleon, V., Tan, E. L., Daponte, A., Aristeidou, S., Xirou, S., Ferentinos, P., Evdokimidis, I., Rentzos, M., Seimenis, I., & Bede, P. (2023). Hippocampal Metabolic Alterations in Amyotrophic Lateral Sclerosis: A Magnetic Resonance Spectroscopy Study. Life, 13(2), 571. https://doi.org/10.3390/life13020571