1. Introduction
Intellectual disability (ID) is characterized by a slow and incomplete development of human cognitive abilities that contribute to the level of general intelligence, as well as to motor, social, and language abilities. In addition, individuals with ID have a reduced ability to understand, learn, remember new things, and even communicate [
1,
2]. The causal or associated factors of ID can be organic, genetic, or sociocultural, although there is no one specific factor, as most cases involve a combination of factors. Trisomy of chromosome 21 (Down syndrome) and fragile X syndrome are the most common genetic causes of ID [
2]. Disability presents before the age of 18, and its prevalence is estimated to range from 1% to 3% worldwide, with a higher occurrence in males [
2]. Individuals with ID typically have an intelligence quotient (IQ) below 70–75. However, the diagnosis of ID is not solely based on IQ, as other factors, such as social adaptation and daily functioning, are also taken into account [
3].
ID can vary in degree and severity, and individuals with ID may have different abilities and needs. Royal Decree (RD) 888/2022 of Spain, which aligns with the social model of the United Nations Convention on the Rights of Persons with Disabilities, came into effect on 20 April 2023 [
4]. With this new legislation, the following levels of ID were established [
5]: Grade 0: 0–4%, the person does not face difficulties in carrying out daily activities; Grade 1: mild (5–24%), with which the person is independent in almost all daily activities; Grade 2: moderate (25–49%), with which the person has independence in self-care but faces some difficulties in daily activities; Grade 3: severe (50–95%), with which the person experiences high difficulty in performing daily activities, including self-care; and Grade 4: profound or complete (96–100%), with which the person has absolute difficulty in daily activities and self-care.
Motor limitations result in imprecise eye movements that affect the vision and learning of subjects with ID, manifesting most commonly in reading. In addition, individuals with ID tend to have more visual problems than people without ID, including refractive errors, strabismus, cataracts, keratoconus, nystagmus, and binocular dysfunctions. Therefore, better optical and visual quality would be useful in the development of skills such as learning and integration, resulting in a better quality of life [
1].
During the reading process, the eyes perform fixation eye movements to extract and process visual information, accompanied by saccadic movements that have different amplitudes depending on the spacing between words, following the direction marked by the lines of the text [
6,
7,
8]. Uncontrolled movements occur with ocular motility problems, making the reading process difficult and diminishing the comprehension of the text [
9].
The Developmental Eye Movement (DEM) test is a psychometric assessment used to evaluate oculomotor performance [
10]; it simulates a reading environment to assess and quantify oculomotor abilities during reading, particularly saccadic eye movements, facilitated by visuo-verbal skills [
11]. The DEM test consists of a preliminary or pretest and three additional subtests: two vertical reading subtests (subtest A and subtest B) and one horizontal reading subtest (subtest C) [
10]. The test utilizes a correction template and standardized parameter tables based on age, as our group described in a previous research paper [
12]. The vertical time (VT), adjusted horizontal time (AdjHT), ratio, and error count are measured and referenced against age-normalized tables to determine percentiles, which indicate whether the subject’s performance is within a normal, high, or low percentile range. A percentile equal to or greater than the 31st percentile is considered normal [
10]. To our knowledge, this test has not been used in a study of subjects with ID. Given the strong association between the DEM test and reading ability, it can be useful in identifying individuals with reading delays [
11]. It is also valuable for assessing children with learning difficulties [
10] and, in the case of this study, individuals with ID. Based on the analysis of previous results, four different categories can be determined: Type I, in which the AdjHT, VT, ratio, and errors are normal for the subject’s age; Type II, in which the VT is normal and the AdjHT is higher, resulting in a higher ratio, indicating potential issues with horizontal saccadic movements; Type III, in which both the VT and AdjHT are higher than normal for the subject’s age, but the ratio is normal, indicating difficulties with automaticity in counting numbers; and Type IV, a combination of Type II and Type III, in which the AdjHT, VT, and ratio are all elevated, indicating problems with both automaticity and oculomotor skills [
13].
The eye tracker is an ocular tracking system that uses near-invisible infrared readers and high-definition cameras; it is capable of identifying and analyzing fixation stability and saccadic movement precision, determining where a subject is looking while performing the investigated tasks [
7,
12]. The data provided with the eye tracker can be considered unbiased, objective, and quantifiable, since the subject’s ocular movements can be observed in real time on the computer screen [
12]. Once analyzed, fixations and saccades can provide clues about the subject’s motivations or cognitive processing. Additionally, the cognitive processes involved in reading can be studied based on the duration of fixations and saccades, which are longer in more challenging parts of the text or due to greater word ambiguity [
7].
The main objective of this study was to quantitatively assess the eye movements made by people with ID during the DEM test using an eye tracker and to calculate the percentiles of the DEM test for a sample of subjects with ID. The eye tracker was used to try to obtain objective data about the execution time of each subtest and the errors made when performing it, and to quantify the fixations and saccades, as well as the speed and amplitude of the latter, in a group of subjects with different degrees of ID. In addition, this study aimed to compare the results of subtest C in subjects with ID against subjects without ID.
2. Materials and Methods
2.1. Sample Description and Selection
The Clinical Research Ethics Committee of Aragón (CEICA) (reference number PI21-074) approved this research, which was conducted from January to April 2023, with the collaboration of the subjects with ID, who attend the Tasubinsa Center in Navarra (Spain) on a daily basis. All individuals within the age range of 18–40 years who agreed to participate were eligible. The objectives of the study were explained, and detailed information was provided about the tests that would be performed. The participants and, in some cases, their legal guardians, signed the informed consent forms.
A screening was performed to identify subjects who met the following inclusion criteria: spherical refractive error between −6.00 D and +3.00 D and astigmatic error of less than 3.00 D; no systemic or ocular pathologies; visual acuity (VA) equal to or greater than 0.80 decimal (20/25 Snellen); and no suppression of one of the eyes, strabismus, or amblyopia.
2.2. Exploratory Protocol
Each subject’s habitual optical correction was measured using a lensometer, VA with correction was assessed, and phoria was quantitatively evaluated using the Maddox Rod test, a light stimulus, and a prism bar. These analyses were performed for distance and near vision, and vertical and horizontal phorias were measured. Participants who met the inclusion criteria had their ocular motility assessed using the DEM test monitored with an eye tracker (Tobii Pro Fusión, Tobii AB, Danderyd, Sweden).
The DEM test was digitized and calibrated for a 21-inch screen, connected to the laptop from which the eye tracker was controlled, and voice was recorded.
The participants were positioned with their chin and forehead resting on the chin rest, 60 cm from the screen, with the DEM test calibrated for a VA of 0.8. The eye tracker was situated just below the screen, also at a distance of 60 cm from the participants.
Once the DEM test was explained, the subjects performed the 4 DEM subtests (pretest, subtest A, subtest B, and subtest C) individually, reading the numbers aloud for the recording of errors (substitutions, additions, omissions, and transpositions). The time it took to perform each subtest was obtained from the eye tracker recordings.
2.3. Data Collection
After the DEM test was performed on all of the subjects, the Tobii Pro Lab program (Tobii AB, Danderyd, Sweden) was used to confirm that the eye tracker had captured both eyes, and the recordings were segmented into four “events”, one for each subtest performed. The duration of these cuts was determined by the first and last fixation that the subject made during each of the subtests.
The recordings of each subject were transferred to the EyeTracker Parse program (University of Zaragoza, Zaragoza, Spain). This program selected the variables from each event, such as the duration of each subtest (s), the number of fixations and saccades in each subtest (n), the pupillary diameter of both the right eye (RE) and the left eye (LE) (mm), and the saccadic speed (m/s) and length (mm) for each eye. Then, each subtest from each participant was analyzed separately and exported to Excel (Microsoft® Office Excel 2011, Microsoft Corporation, Redmond, WA, USA) to create one Excel database for each subtest (subtest A, subtest B, and subtest C).
2.4. Statistical Analysis
The variables were analyzed with the Statistical Package for the Social Sciences (SPSS 24.0 Inc., Chicago, IL, USA). The mean, standard deviation, and maximum and minimum values were calculated for each parameter. The sample did not follow normality according to the Kolmogorov–Smirnov test, so the nonparametric Wilcoxon signed rank test was performed for related samples, and the correlation was determined with Spearman’s test. Variables of subtest C were also compared between subjects with ID and subjects without ID, for which the nonparametric Mann–Whitney U test for independent samples was used. A p value < 0.05 was considered statistically significant. Percentiles, scatter plots, and bar plots were generated using Excel.
4. Discussion
This study aimed to objectively evaluate the ocular motility parameters of the DEM test using an eye tracker in subjects with ID. The DEM test is a visual–verbal test, in which movements such as saccades or fixations, involved in seeing, recognizing, and naming numbers, are measured. Observing the results of this study in participants with ID, there was a significant positive correlation between the length and speed of the saccades of the RE and those of the LE, as well as the pupillary diameter; these results are consistent with those found in a similar study in subjects without ID [
12], which indicates that both eyes of the same subject work together even with ID.
When analyzing the mean traditional parameters of the DEM test in subjects with ID, the VT was in the 35th percentile, the AdjHT was in the 40th percentile, and the ratio was in the 35th percentile. These parameters would be considered normal for the ID group, since they are above the 31st [
10] percentile according to the percentiles of their own ID group (
Table 2). However, according to the normalized percentile table for a sample of subjects without ID, the VT, AdjHT, and ratio values would be in the 1st percentile [
12]. With these results, it could be concluded that people with ID take longer to perform the different subtests and exhibit worse comprehension, since the number of mean errors was 5.50.
Because subjects with ID tend to have more oculomotor dysfunctions, such as nystagmus, abnormal values are expected and can serve as a reference for other investigations. We tried to obtain percentiles for the subjects with ID and determine if there was any difference in the results depending on the degree of ID. When the ID group was divided into two subgroups based on the percentage of ID, the VT of Group 1 was 47.04 s, while that of Group 2 was significantly higher (
p = 0.008), at 73.37 s. The AdjHT was 71.78 s for Group 1 and 98.18 s for Group 2. The ratio was higher for Group 1 than for Group 2 (1.55 and 1.40, respectively). The subjects in Group 2 (6.47) made a greater number of errors than those in Group 1 (4.92). The subjects in Group 2 exhibited a greater number of interruptions and had more difficulty understanding the dynamics of the test than those in Group 1. In addition, Group 1 exhibited a higher percentile (60) in VT than Group 2 (15). For the AdjHT, Group 1 exhibited the 45th percentile, while Group 2 exhibited the 20th percentile. However, for the ratio, Group 1 exhibited the 30th percentile, and Group 2 exhibited the 50th percentile, in some cases similar to a Type IV DEM test result [
13]. When performing the test, the explanation had to be repeated several times for some subjects to complete the test in its entirety. Subjects with ID also took longer to understand the format of subtest C than the formats of subtests A and B.
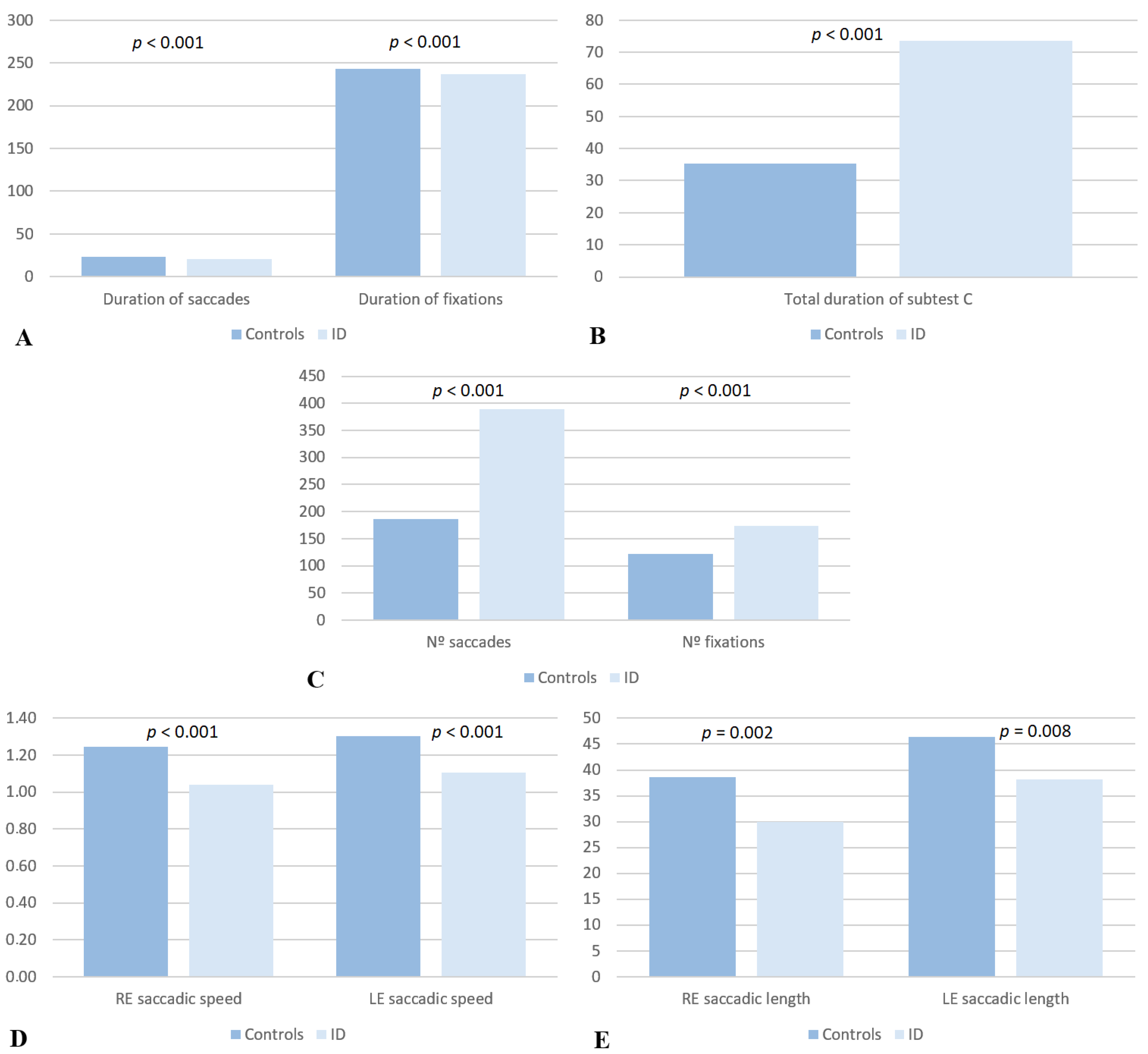
All subjects with ID were compared with a sample of 52 subjects without ID. This comparison verified that the subjects with ID had a greater VT (57.81 ± 21.93 s) than the subjects without ID (33.58 ± 5.56 s), and the same pattern was observed for the AdjHT (subjects with ID: 81.68 ± 35.96 s, subjects without ID: 35.24 ± 6.68 s). In addition, the number of errors made by the subjects with ID was 5.50 ± 8.69, while the subjects without ID did not make any errors. The ratio in the subjects with ID was 1.50 ± 0.59, while in the subjects without ID, it was 1.05 ± 0.09.
This study standardized the DEM test in subjects with ID. To achieve this, we evaluated 45 subjects between the ages of 22 and 40 with a mean age of 31.15 ± 4.26 years. It also demonstrates that it is necessary to create normalized tables with different percentiles for subjects with ID than those used for people without ID, since their fixations and saccades are slower and more numerous, which does not necessarily mean that they have motility problems, but that they are typical for their percentage of ID. In other words, both eyes of the same subject with ID work together, without differences between them, and with a significant positive correlation in terms of saccadic speed and length.
Scheiman [
14] postulated that the fewer saccades performed and the more parafoveal vision is used, the faster the reading, and the better the comprehension will be [
15]. On the other hand, when analyzing a study in which different images were presented to children with mild ID and children without ID, monitored with a GP3 Gazepoint eye-tracking system (Vancouver, BC, Canada), children with mild ID performed fewer fixations than children without ID. The opposite occurred in our study, in which subjects with ID performed a greater number of fixations than subjects without ID. The previous study [
14] suggested that children with mild ID make fewer fixations because they need more time to carry them out. Furthermore, the children with mild ID ignored textual elements in mixed images, instead focusing their attention on the pictorial elements, while the children without ID fixed their gaze more on the textual elements. Therefore, the DEM test may seem unattractive to subjects with ID and take longer to complete. However, subjects with a high percentage of ID were made to look at the numbers and name them, which is generally more difficult than for letters, so fixations are maintained longer.
Other studies have been performed in diverse populations, using devices to monitor ocular motility as objectively as possible. Vakil et al. [
16] compared subjects with ID to subjects with typical development (TD), matched by cognitive level. Participants solved perceptual and conceptual analogies (from the Conceptual and Perceptual Analog Modifiability Test, CPAM), while their eye movements were monitored with an eye tracker, with the TD group having a significantly higher overall percentage of correct answers. The eye movement pattern revealed that there were both quantitative and qualitative differences between the groups in the process of solving the analogies. The authors interpreted this as a reflection of two different types of strategies: constructive matching and response elimination.
In another investigation [
17], the reaction times of saccades were studied in subjects with ID between 13 and 57 years old, using electrooculography, taking into account the IQs of the subjects. It was found that subjects with a higher IQ exhibited a shorter mean saccade reaction time. Although the methodology was different, these conclusions could be reflected in our study, in that subjects with a higher percentage of ID had a longer test duration, since their saccades need a longer reaction time.
In our study, subjects with ID made a greater number of errors on subtest C than on subtests A or B, possibly caused by reading the same line twice or skipping to the next line, since test C is a multiline task [
18]. Therefore, as Hindmarsh et al. [
7] commented, both horizontal and vertical eye movements must be considered to understand the behavior of eye movements during reading.
Conducting a study, with an eye tracker, on the duration of fixations and saccades, as well as the saccadic length and speed of each eye of the same subject with ID, could be useful to detect subjects with eye movement conjugation problems that can affect their reading. This procedure cannot be used as a diagnostic tool for ID, but it can be very useful to understand potential deficiencies in reading. For this reason, it is important to evaluate the DEM test results with normative tables for subjects with ID with their own percentiles, since using normative tables for subjects without ID will result in very low percentiles in the absence of ocular motility dysfunction, due to the intrinsic effects of having an ID.
Individuals with varying ID severities may exhibit distinctive ocular motility features. Those with higher ID percentages, indicative of more severe ID, may struggle to coordinate eye movements during the DEM test, thus impacting both saccadic speed and accuracy. Factors like increased fixation counts and prolonged trial times, particularly in individuals with higher ID percentages, add complexity to interpreting ocular motility data. This necessitates normative tables tailored for those with ID, acknowledging potential deviations from patterns observed in individuals without ID. In clinical evaluations of people with ID, it is crucial to consider the multifaceted nature of ID when interpreting ocular motility results. This study’s establishment of a 76% disability limit underscores the challenges faced by those with higher ID percentages, highlighting slower and less precise eye movements in Group 2 individuals.
A future line of research in subjects with ID could be to perform the test for adults with two-digit numbers, using the Adult Developmental Eye Movement (ADEM) test [
19], or its modified version, the ADEMd test [
20], which involves a task that requires more attention. It could offer valuable insights into the nuanced aspects of ocular motility in people with ID.







{kind=link}
{kind=link}