
Software-Based Assessment of Well-Aerated Lung at CT for Quantification of Predicted Pulmonary Function in Resected NSCLC

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
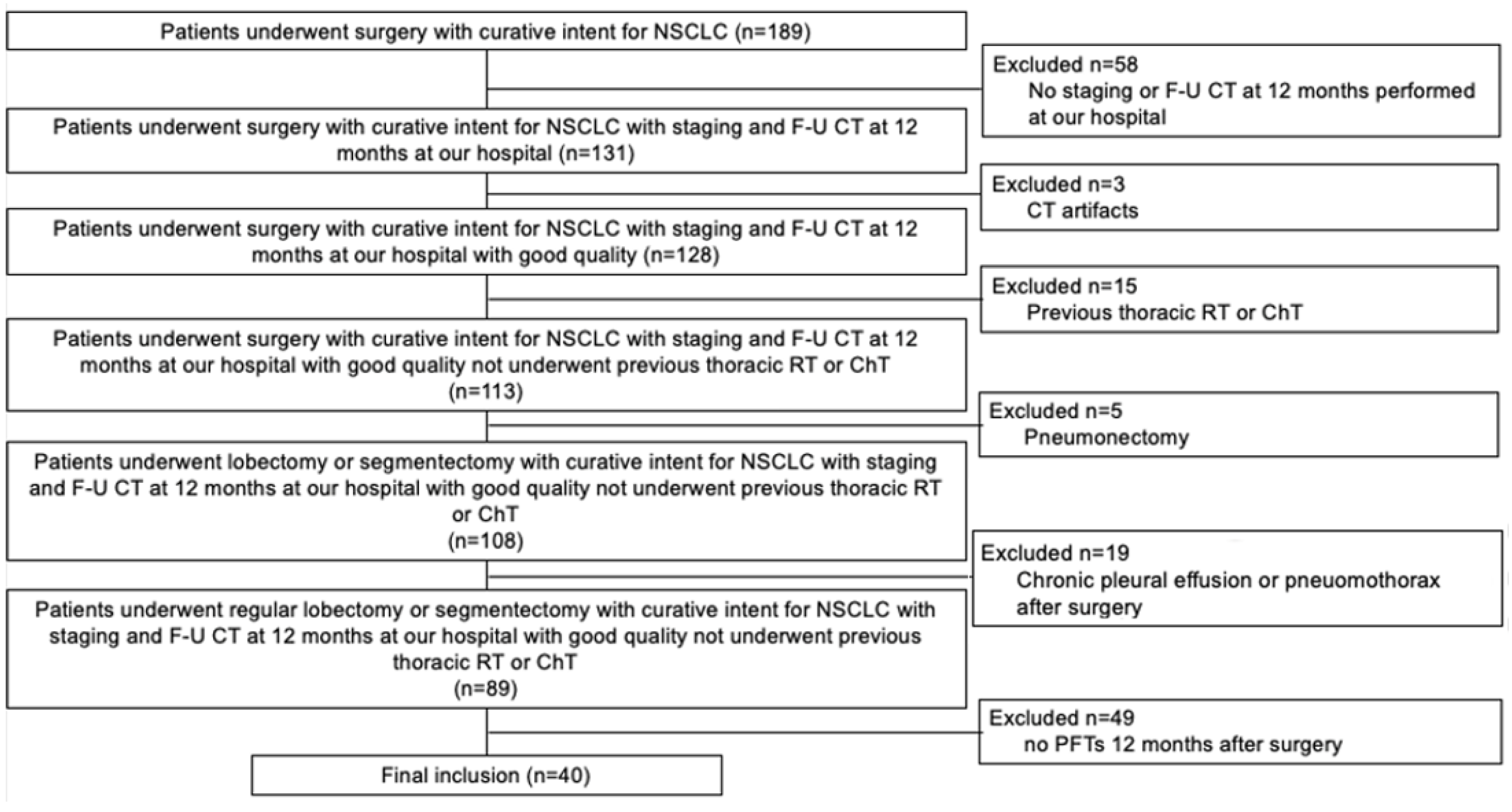
2.1. Study Population
2.2. Pulmonary Function Tests
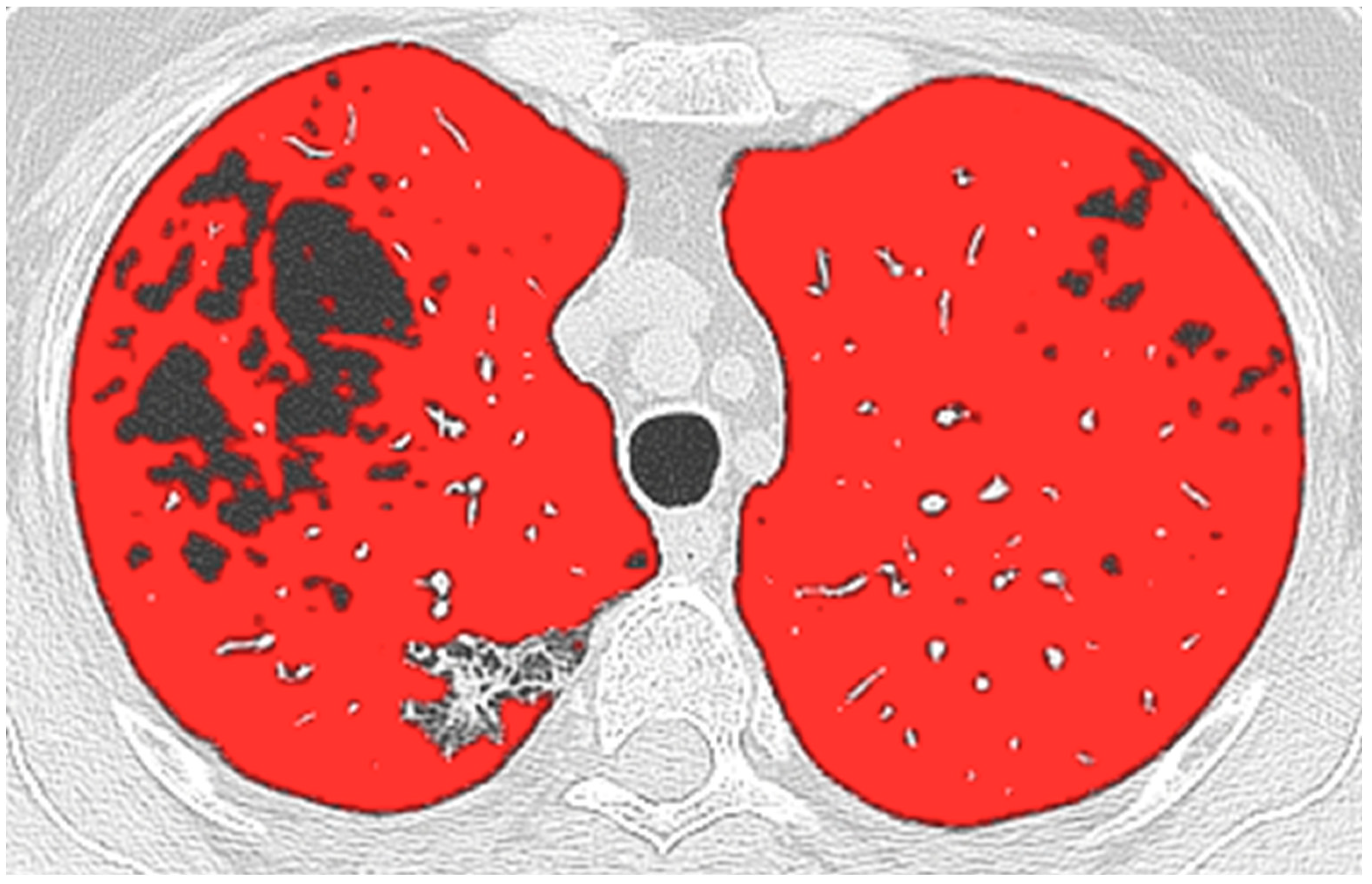
2.3. CT and Computer Analysis
2.4. Surgical Procedures
2.5. Statistical Analysis
3. Results
3.1. Study Population
3.2. Pulmonary Function Tests and Quantitative CT
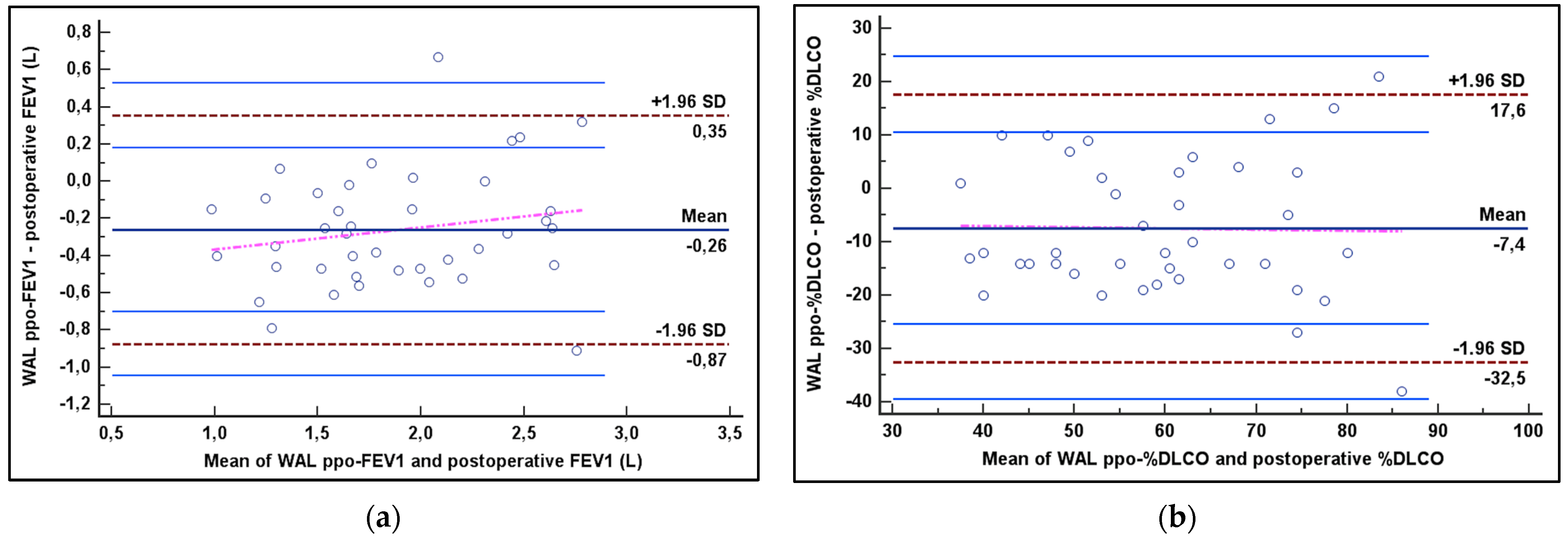
3.3. Correlation and Agreement Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Postmus, P.E.; Kerr, K.M.; Oudkerk, M.; Senan, S.; Waller, D.A.; Vansteenkiste, J.; Escriu, C.; Peters, S. Early and Locally Advanced Non-Small-Cell Lung Cancer (NSCLC): ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up. Ann. Oncol. 2017, 28, iv1–iv21. [Google Scholar] [CrossRef] [PubMed]
- Bade, B.C.; Dela Cruz, C.S. Lung Cancer 2020: Epidemiology, Etiology, and Prevention. Clin. Chest Med. 2020, 41, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Baratella, E.; Cernic, S.; Minelli, P.; Furlan, G.; Crim, F.; Rocco, S.; Ruaro, B.; Cova, M.A. Accuracy of CT-Guided Core-Needle Biopsy in Diagnosis of Thoracic Lesions Suspicious for Primitive Malignancy of the Lung: A Five-Year Retrospective Analysis. Tomography 2022, 8, 2828–2838. [Google Scholar] [CrossRef]
- Baratella, E.; Fiorese, I.; Minelli, P.; Veiluva, A.; Marrocchio, C.; Ruaro, B.; Cova, M.A. Aging-Related Findings of the Respiratory System in Chest Imaging: Pearls and Pitfalls. Curr. Radiol. Rep. 2022, 11, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Tian, S.; Wang, S.; Liu, S.; Liao, M. CT-Guided Percutaneous Core Needle Biopsy in Typing and Subtyping Lung Cancer: A Comparison to Surgery. Technol. Cancer Res. Treat. 2022, 21, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Brunelli, A.; Charloux, A.; Bolliger, C.T.; Rocco, G.; Sculier, J.P.; Varela, G.; Licker, M.; Ferguson, M.K.; Faivre-Finn, C.; Huber, R.M.; et al. ERS/ESTS Clinical Guidelines on Fitness for Radical Therapy in Lung Cancer Patients (Surgery and Chemo-Radiotherapy). Eur. Respir. J. 2009, 34, 17–41. [Google Scholar] [CrossRef] [PubMed]
- Eslick, E.M.; Bailey, D.L.; Harris, B.; Kipritidis, J.; Stevens, M.; Li, B.T.; Bailey, E.; Gradinscak, D.; Pollock, S.; Htun, C.; et al. Measurement of Preoperative Lobar Lung Function with Computed Tomography Ventilation Imaging: Progress towards Rapid Stratification of Lung Cancer Lobectomy Patients with Abnormal Lung Function. Eur. J. Cardio-Thorac. Surg. 2016, 49, 1075–1082. [Google Scholar] [CrossRef]
- Yokoba, M.; Ichikawa, T.; Harada, S.; Shiomi, K.; Mikubo, M.; Ono, M.; Sonoda, D.; Satoh, Y.; Hanawa, H.; Naoki, K.; et al. Comparison between Quantitative Computed Tomography, Scintigraphy, and Anatomical Methods for Prediction of Postoperative FEV1 and DLCO: Effects of Chronic Obstructive Pulmonary Disease Status and Resected Lobes. J. Thorac. Dis. 2020, 12, 5269–5280. [Google Scholar] [CrossRef]
- Sverzellati, N.; Chetta, A.; Calabrò, E.; Carbognani, P.; Internullo, E.; Olivieri, D.; Zompatori, M. Reliability of Quantitative Computed Tomography to Predict Postoperative Lung Function in Patients with Chronic Obstructive Pulmonary Disease Having a Lobectomy. J. Comput. Assist. Tomogr. 2005, 29, 819–824. [Google Scholar] [CrossRef]
- Risoli, C.; Nicol, M.; Colombi, D.; Moia, M.; Rapacioli, F.; Anselmi, P.; Michieletti, E.; Ambrosini, R.; Di Terlizzi, M.; Grazioli, L.; et al. Different Lung Parenchyma Quantification Using Dissimilar Segmentation Software: A Multi-Center Study for COVID-19 Patients. Diagnostics 2022, 92, 1501. [Google Scholar] [CrossRef]
- Colombi, D.; Bodini, F.C.; Petrini, M.; Maffi, G.; Morelli, N.; Milanese, G.; Silva, M.; Sverzellati, N.; Michieletti, E. Well-Aerated Lung on Admitting Chest CT to Predict Adverse Outcome in COVID-19 Pneumonia. Radiology 2020, 296, 201433. [Google Scholar] [CrossRef] [PubMed]
- Goldstraw, P.; Chansky, K.; Crowley, J.; Rami-Porta, R.; Asamura, H.; Eberhardt, W.E.E.; Nicholson, A.G.; Groome, P.; Mitchell, A.; Bolejack, V.; et al. The IASLC Lung Cancer Staging Project: Proposals for Revision of the TNM Stage Groupings in the Forthcoming (Eighth) Edition of the TNM Classification for Lung Cancer. J. Thorac. Oncol. 2016, 11, 39–51. [Google Scholar] [CrossRef] [PubMed]
- Park, K.J.; Bergin, C.J.; Clausen, J.L. Quantitation of Emphysema with Three-Dimensional CT Densitometry: Comparison with Two-Dimensional Analysis, Visual Emphysema Scores, and Pulmonary Function Test Results. Radiology 1999, 211, 541–547. [Google Scholar] [CrossRef] [PubMed]
- Howington, J.A.; Blum, M.G.; Chang, A.C.; Balekian, A.A.; Murthy, S.C. Treatment of Stage I and II Non-Small Cell Lung Cancer: Diagnosis and Management of Lung Cancer, 3rd Ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 2013, 143, e278S–e313S. [Google Scholar] [CrossRef] [PubMed]
- Zeiher, B.G.; Gross, T.J.; Kern, J.A.; Lanza, L.A.; Peterson, M.W. Predicting Postoperative Pulmonary Function in Patients Undergoing Lung Resection. Chest 1995, 108, 68–72. [Google Scholar] [CrossRef]
- Schober, P.; Mascha, E.J.; Vetter, T.R. Statistics From A (Agreement) To. Anesth. Analg. 2021, 133, 1633–1641. [Google Scholar] [CrossRef]
- Colombi, D.; Di Lauro, E.; Silva, M.; Manna, C.; Rossi, C.; De Filippo, M.; Zompatori, M.; Ruffini, L.; Sverzellati, N. Non-Small Cell Lung Cancer after Surgery and Chemoradiotherapy: Follow-up and Response Assessment. Diagn. Interv. Radiol. 2013, 19, 447–456. [Google Scholar] [CrossRef]
- Nishiyama, A.; Kawata, N.; Yokota, H.; Sugiura, T.; Matsumura, Y.; Higashide, T.; Horikoshi, T.; Oda, S.; Tatsumi, K.; Uno, T. A Predictive Factor for Patients with Acute Respiratory Distress Syndrome: CT Lung Volumetry of the Well-Aerated Region as an Automated Method. Eur. J. Radiol. 2020, 122, 108748. [Google Scholar] [CrossRef]
- Leoni, M.L.G.; Lombardelli, L.; Colombi, D.; Bignami, E.G.; Pergolotti, B.; Repetti, F.; Villani, M.; Bellini, V.; Rossi, T.; Halasz, G.; et al. Prediction of 28-Day Mortality in Critically Ill Patients with COVID-19: Development and Internal Validation of a Clinical Prediction Model. PLoS ONE 2021, 16, e0254550. [Google Scholar] [CrossRef]
- Rienmüller, R.K.; Behr, J.; Kalender, W.A.; Schätzl, M.; Altmann, I.; Merin, M.; Beinert, T. Standardized Quantitative High Resolution CT in Lung Diseases. J. Comput. Assist. Tomogr. 1991, 15, 742–749. [Google Scholar] [CrossRef]
- Ohno, Y.; Hatabu, H.; Higashino, T.; Takenaka, D.; Watanabe, H.; Nishimura, Y.; Yoshimura, M.; Sugimura, K. Dynamic Perfusion MRI versus Perfusion Scintigraphy: Prediction of Postoperative Lung Function in Patients with Lung Cancer. AJR. Am. J. Roentgenol. 2004, 182, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Best, A.C.; Meng, J.; Lynch, A.M.; Bozic, C.M.; Miller, D.; Grunwald, G.K.; Lynch, D.A. Idiopathic Pulmonary Fibrosis: Physiologic Tests, Quantitative CT Indexes, and CT Visual Scores as Predictors of Mortality. Radiology 2008, 246, 935–940. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | All Patients (n = 40) |
|---|---|
| Age (y) | 68 (62; 74) |
| Gender | |
| males | 26/40 (65%) |
| females | 14/40 (35%) |
| Smoking history | |
| never | 5/40 (12%) |
| former | 26/40 (65%) |
| current | 9/40 (23%) |
| COPD | 25/40 (62%) |
| Tumor stage (TNM 8th edition) | |
| IA1 | 16/40 (40%) |
| IA2 | 8/40 (20%) |
| IA3 | 3/40 (8%) |
| IB | 9/40 (22%) |
| IIB | 3/40 (8%) |
| IIIA | 1/40 (2%) |
| Histologic type | |
| adenocarcinoma | 38/40 (95%) |
| squamous cell carcinoma | 2/40 (5%) |
| Surgical resection | |
| right upper lobe | 18/40 (45%) |
| left upper lobe | 11/40 (27%) |
| right lower lobe | 5/40 (12%) |
| left lower lobe | 6/40 (16%) |
| Surgery type | |
| lobectomy | 31/40 (78%) |
| typical segmentectomy | 5/40 (12%) |
| atypical segmentectomy | 4/40 (10%) |
| Comparison | Spearman rho Coefficient (p Value) | Limit of Agreement +1.96SD, −1.96 SD | ICC (95% CI) |
|---|---|---|---|
| WAL ppo-FEV1 (L) vs. ASC ppo-FEV1 (L) WAL ppo-FEV1 (L) vs. postoperative-FEV1 (L) ASC ppo-FEV1 (L) vs. postoperative-FEV1 (L) | 0.957 (p < 0.001) 0.842 (p < 0.001) 0.856 (p < 0.001) | +0.20, −0.46 +0.35, −0.87 +0.47, −0.72 | 0.978 (0.958–0.988) 0.904 (0.819–0.949) 0.916 (0.841–0.955) |
| WAL ppo-%DLCO vs. ASC ppo-%DLCO WAL ppo-%DLCO vs. postoperative-%DLCO ASC ppo-%DLCO vs. postoperative-%DLCO | 0.948 (p < 0.001) 0.717 (p < 0.001) 0.751 (p < 0.001) | +4, −12 +17, −32 +19, −26 | 0.977 (0.957–0.988) 0.770 (0.566–0.878) 0.796 (0.615–0.892) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Colombi, D.; Risoli, C.; Delfanti, R.; Chiesa, S.; Morelli, N.; Petrini, M.; Capelli, P.; Franco, C.; Michieletti, E. Software-Based Assessment of Well-Aerated Lung at CT for Quantification of Predicted Pulmonary Function in Resected NSCLC. Life 2023, 13, 198. https://doi.org/10.3390/life13010198
Colombi D, Risoli C, Delfanti R, Chiesa S, Morelli N, Petrini M, Capelli P, Franco C, Michieletti E. Software-Based Assessment of Well-Aerated Lung at CT for Quantification of Predicted Pulmonary Function in Resected NSCLC. Life. 2023; 13(1):198. https://doi.org/10.3390/life13010198
Chicago/Turabian StyleColombi, Davide, Camilla Risoli, Rocco Delfanti, Sara Chiesa, Nicola Morelli, Marcello Petrini, Patrizio Capelli, Cosimo Franco, and Emanuele Michieletti. 2023. "Software-Based Assessment of Well-Aerated Lung at CT for Quantification of Predicted Pulmonary Function in Resected NSCLC" Life 13, no. 1: 198. https://doi.org/10.3390/life13010198
APA StyleColombi, D., Risoli, C., Delfanti, R., Chiesa, S., Morelli, N., Petrini, M., Capelli, P., Franco, C., & Michieletti, E. (2023). Software-Based Assessment of Well-Aerated Lung at CT for Quantification of Predicted Pulmonary Function in Resected NSCLC. Life, 13(1), 198. https://doi.org/10.3390/life13010198