

Direct Mechanical Thrombectomy Versus Prior Bridging Intravenous Thrombolysis in Acute Ischemic Stroke: A Systematic Review and Meta-Analysis

 , ,
, ,
Abstract
1. Introduction
2. Methods
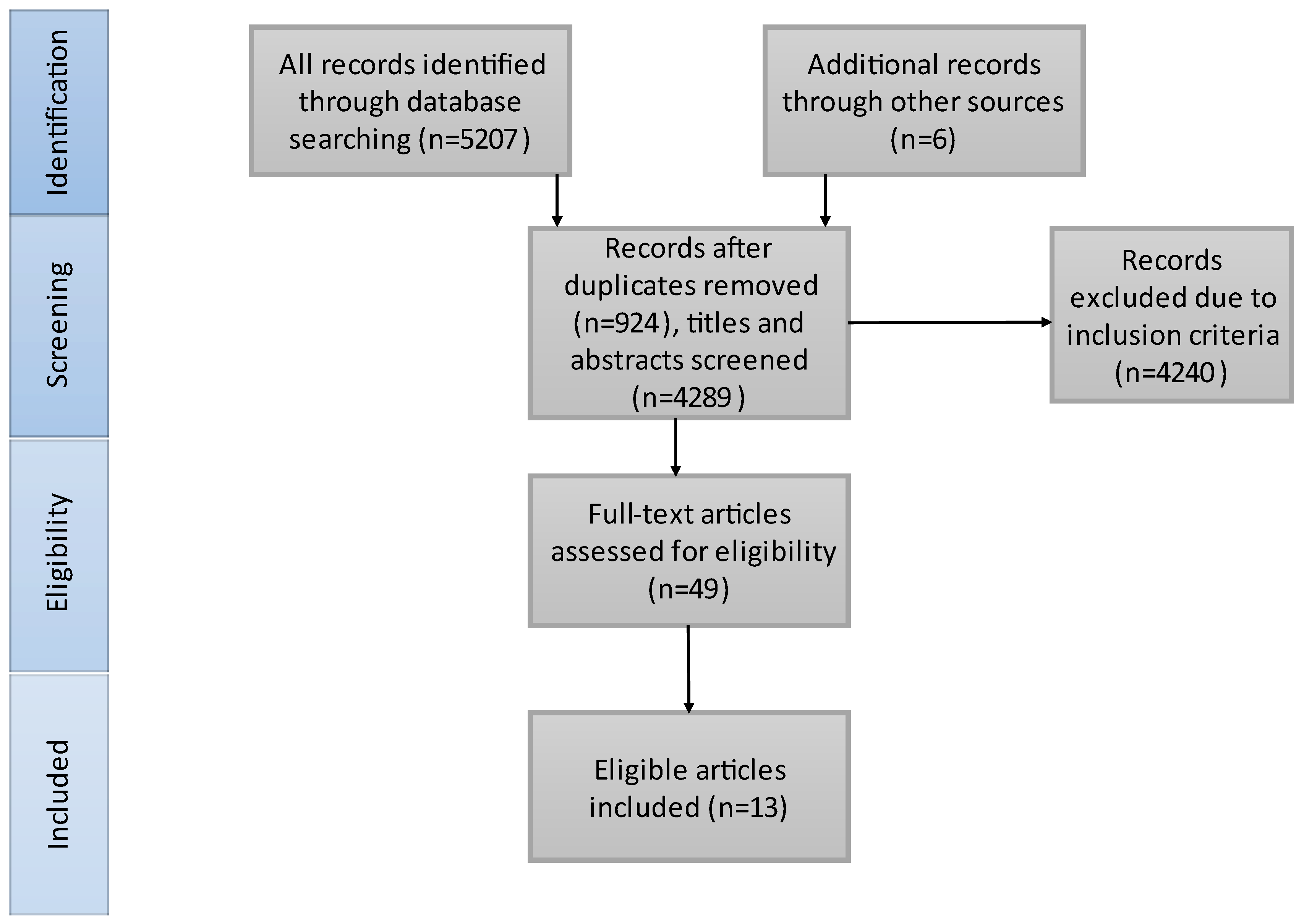
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Outcome Definition
2.4. Data Extraction and Assessment
2.5. Quality Evaluation of the Included Studies
2.6. Statistical Analysis
3. Results
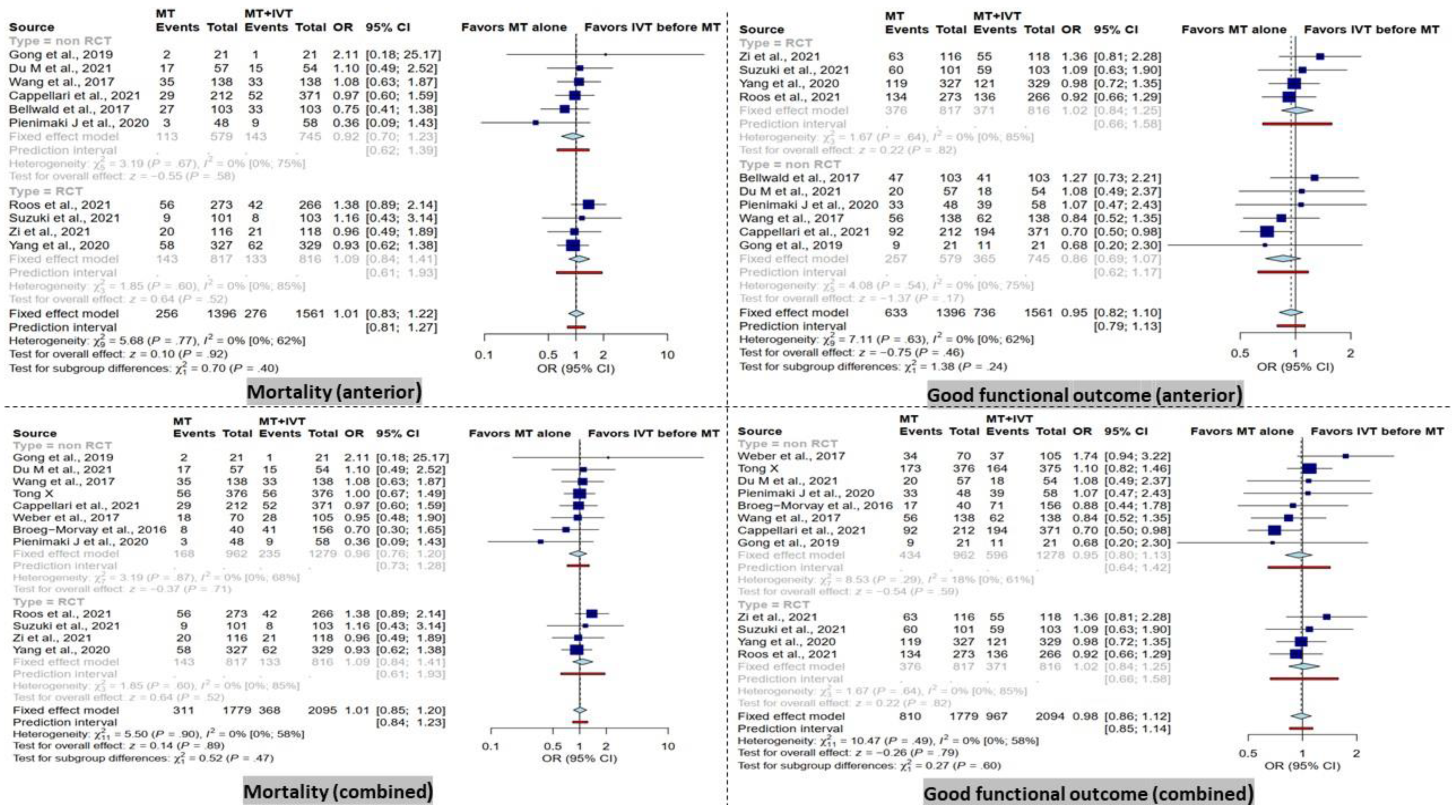
3.1. Mortality at 90 Days
3.2. Functional Outcome at 90 Days
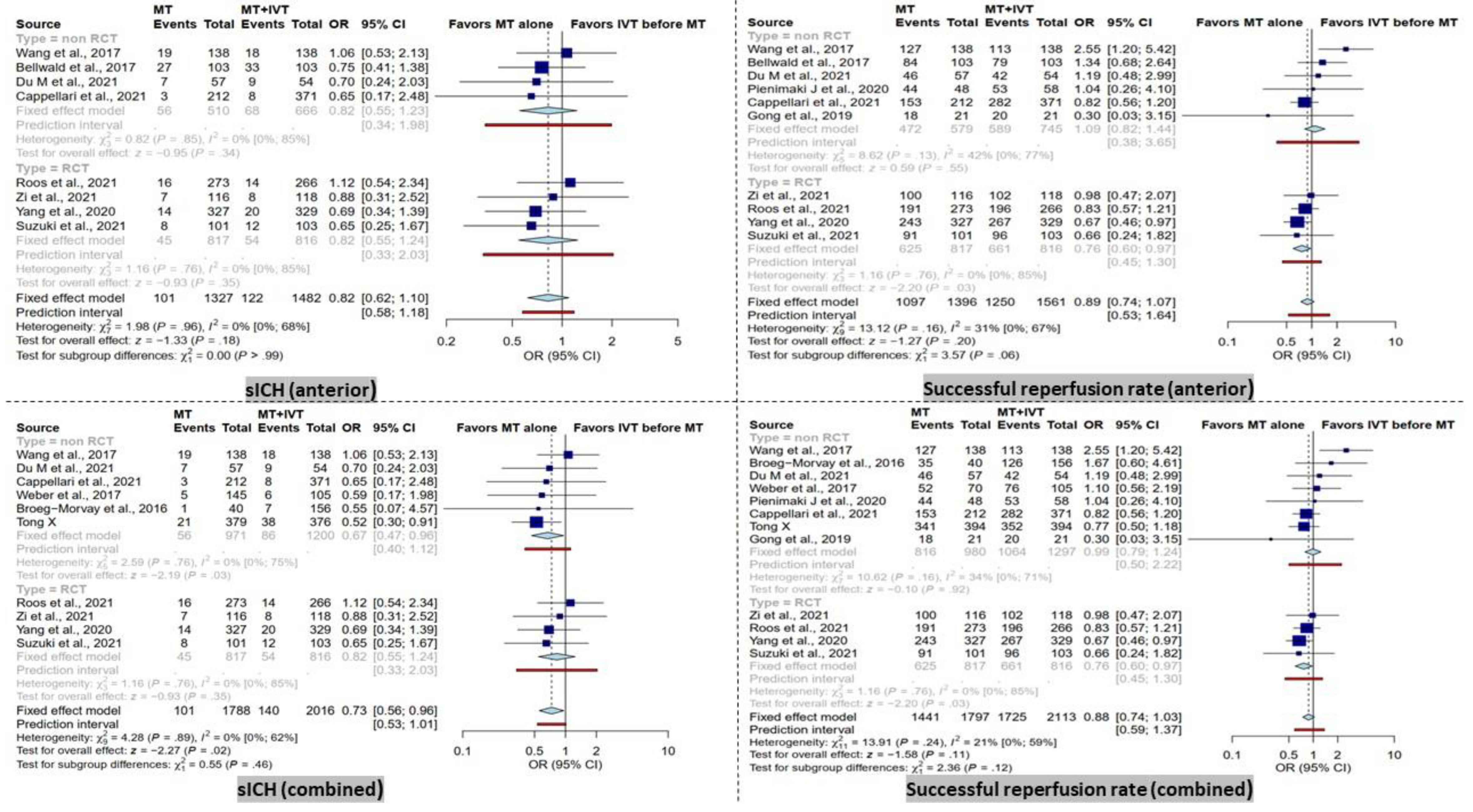
3.3. sICH
3.4. Successful Recanalization
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Strong, K.; Mathers, C.; Bonita, R. Preventing stroke: Saving lives around the world. Lancet Neurol. 2007, 6, 182–187. [Google Scholar] [CrossRef] [PubMed]
- Feigin, V.L.; Lawes, C.M.; Bennett, D.A.; Barker-Collo, S.L.; Parag, V. Worldwide stroke incidence and early case fatality reported in 56 population-based studies: A systematic review. Lancet Neurol. 2009, 8, 355–369. [Google Scholar] [CrossRef]
- Li, L.; Scott, C.A.; Rothwell, P.M. Trends in Stroke Incidence in High-Income Countries in the 21st Century: Population-Based Study and Systematic Review. Stroke 2020, 51, 1372–1380. [Google Scholar] [CrossRef]
- Kuriakose, D.; Xiao, Z. Pathophysiology and Treatment of Stroke: Present Status and Future Perspectives. Int. J. Mol. Sci. 2020, 21, 7609. [Google Scholar] [CrossRef]
- Soto-Cámara, R.; González-Bernal, J.J.; González-Santos, J.; Aguilar-Parra, J.M.; Trigueros, R.; López-Liria, R. Knowledge on Signs and Risk Factors in Stroke Patients. J. Clin. Med. 2020, 9, 2557. [Google Scholar] [CrossRef] [PubMed]
- Rennert, R.C.; Wali, A.R.; Steinberg, J.A.; Santiago-Dieppa, D.R.; Olson, S.E.; Pannell, J.S.; Khalessi, A.A. Epidemiology, Natural History, and Clinical Presentation of Large Vessel Ischemic Stroke. Neurosurgery 2019, 85, S4–S8. [Google Scholar] [CrossRef] [PubMed]
- Fink, J.N.; Selim, M.H.; Kumar, S.; Voetsch, B.; Fong, W.C.; Caplan, L.R. Insular cortex infarction in acute middle cerebral artery territory stroke: Predictor of stroke severity and vascular lesion. Arch. Neurol. 2005, 62, 1081–1085. [Google Scholar] [CrossRef] [PubMed]
- Kodumuri, N.; Sebastian, R.; Davis, C.; Posner, J.; Kim, E.H.; Tippett, D.C.; Wright, A.; Hillis, A.E. The association of insular stroke with lesion volume. Neuroimage Clin. 2016, 11, 41–45. [Google Scholar] [CrossRef]
- Cooray, C.; Fekete, K.; Mikulik, R.; Lees, K.R.; Wahlgren, N.; Ahmed, N. Threshold for NIH stroke scale in predicting vessel occlusion and functional outcome after stroke thrombolysis. Int. J. Stroke 2015, 10, 822–829. [Google Scholar] [CrossRef]
- Heldner, M.R.; Zubler, C.; Mattle, H.P.; Schroth, G.; Weck, A.; Mono, M.L.; Gralla, J.; Jung, S.; El-Koussy, M.; Lüdi, R.; et al. National Institutes of Health stroke scale score and vessel occlusion in 2152 patients with acute ischemic stroke. Stroke 2013, 44, 1153–1157. [Google Scholar] [CrossRef]
- Smith, W.S.; Tsao, J.W.; Billings, M.E.; Johnston, S.C.; Hemphill, J.C., 3rd; Bonovich, D.C.; Dillon, W.P. Prognostic significance of angiographically confirmed large vessel intracranial occlusion in patients presenting with acute brain ischemia. Neurocrit. Care 2006, 4, 14–17. [Google Scholar] [CrossRef] [PubMed]
- Smith, W.S.; Lev, M.H.; English, J.D.; Camargo, E.C.; Chou, M.; Johnston, S.C.; Gonzalez, G.; Schaefer, P.W.; Dillon, W.P.; Koroshetz, W.J.; et al. Significance of large vessel intracranial occlusion causing acute ischemic stroke and TIA. Stroke 2009, 40, 3834–3840. [Google Scholar] [CrossRef] [PubMed]
- Minhas, J.S.; Wang, X.; Lindley, R.I.; Delcourt, C.; Song, L.; Woodward, M.; Lee, T.H.; Broderick, J.P.; Pontes-Neto, O.M.; Kim, J.S.; et al. Comparative effects of intensive-blood pressure versus standard-blood pressure-lowering treatment in patients with severe ischemic stroke in the ENCHANTED trial. J. Hypertens. 2021, 39, 280–285. [Google Scholar] [CrossRef] [PubMed]
- Malhotra, K.; Gornbein, J.; Saver, J.L. Ischemic Strokes Due to Large-Vessel Occlusions Contribute Disproportionately to Stroke-Related Dependence and Death: A Review. Front. Neurol. 2017, 8, 651. [Google Scholar] [CrossRef]
- Hopkins, L.N. Blazing the frontiers of stroke therapy. Neurosurgery 2019, 85, S1–S2. [Google Scholar] [CrossRef]
- Adeoye, O.; Hornung, R.; Khatri, P.; Kleindorfer, D. Recombinant tissue-type plasminogen activator use for ischemic stroke in the United States: A doubling of treatment rates over the course of 5 years. Stroke 2011, 42, 1952–1955. [Google Scholar] [CrossRef]
- Saqqur, M.; Uchino, K.; Demchuk, A.M.; Molina, C.A.; Garami, Z.; Calleja, S.; Akhtar, N.; Orouk, F.O.; Salam, A.; Shuaib, A.; et al. Site of arterial occlusion identified by transcranial Doppler predicts the response to intravenous thrombolysis for stroke. Stroke 2007, 38, 948–954. [Google Scholar] [CrossRef]
- Paciaroni, M.; Balucani, C.; Agnelli, G.; Caso, V.; Silvestrelli, G.; Grotta, J.C.; Demchuk, A.M.; Sohn, S.I.; Orlandi, G.; Leys, D.; et al. Systemic thrombolysis in patients with acute ischemic stroke and Internal Carotid ARtery Occlusion: The ICARO study. Stroke 2012, 43, 125–130. [Google Scholar] [CrossRef]
- De Silva, D.A.; Brekenfeld, C.; Ebinger, M.; Christensen, S.; Barber, P.A.; Butcher, K.S.; Levi, C.R.; Parsons, M.W.; Bladin, C.F.; Donnan, G.A.; et al. The benefits of intravenous thrombolysis relate to the site of baseline arterial occlusion in the Echoplanar Imaging Thrombolytic Evaluation Trial (EPITHET). Stroke 2010, 41, 295–299. [Google Scholar] [CrossRef]
- Jansen, O.; von Kummer, R.; Forsting, M.; Hacke, W.; Sartor, K. Thrombolytic therapy in acute occlusion of the intracranial internal carotid artery bifurcation. AJNR Am. J. Neuroradiol. 1995, 16, 1977–1986. [Google Scholar]
- Tissue Plasminogen Activator for Acute Ischemic Stroke. N. Engl. J. Med. 1995, 333, 1581–1588. [CrossRef] [PubMed]
- Goyal, M.; Menon, B.K.; van Zwam, W.H.; Dippel, D.W.; Mitchell, P.J.; Demchuk, A.M.; Dávalos, A.; Majoie, C.B.; van der Lugt, A.; de Miquel, M.A.; et al. Endovascular thrombectomy after large-vessel ischaemic stroke: A meta-analysis of individual patient data from five randomised trials. Lancet 2016, 387, 1723–1731. [Google Scholar] [CrossRef] [PubMed]
- Broderick, J.P.; Palesch, Y.Y.; Demchuk, A.M.; Yeatts, S.D.; Khatri, P.; Hill, M.D.; Jauch, E.C.; Jovin, T.G.; Yan, B.; Silver, F.L.; et al. Endovascular therapy after intravenous t-PA versus t-PA alone for stroke. N. Engl. J. Med. 2013, 368, 893–903. [Google Scholar] [CrossRef] [PubMed]
- Ciccone, A.; Valvassori, L.; Nichelatti, M.; Sgoifo, A.; Ponzio, M.; Sterzi, R.; Boccardi, E. Endovascular treatment for acute ischemic stroke. N. Engl. J. Med. 2013, 368, 904–913. [Google Scholar] [CrossRef] [PubMed]
- Kidwell, C.S.; Jahan, R.; Gornbein, J.; Alger, J.R.; Nenov, V.; Ajani, Z.; Feng, L.; Meyer, B.C.; Olson, S.; Schwamm, L.H.; et al. A trial of imaging selection and endovascular treatment for ischemic stroke. N. Engl. J. Med. 2013, 368, 914–923. [Google Scholar] [CrossRef] [PubMed]
- Berkhemer, O.A.; Fransen, P.S.; Beumer, D.; van den Berg, L.A.; Lingsma, H.F.; Yoo, A.J.; Schonewille, W.J.; Vos, J.A.; Nederkoorn, P.J.; Wermer, M.J.; et al. A randomized trial of intraarterial treatment for acute ischemic stroke. N. Engl. J. Med. 2015, 372, 11–20. [Google Scholar] [CrossRef]
- Campbell, B.C.; Mitchell, P.J.; Kleinig, T.J.; Dewey, H.M.; Churilov, L.; Yassi, N.; Yan, B.; Dowling, R.J.; Parsons, M.W.; Oxley, T.J.; et al. Endovascular therapy for ischemic stroke with perfusion-imaging selection. N. Engl. J. Med. 2015, 372, 1009–1018. [Google Scholar] [CrossRef]
- Goyal, M.; Demchuk, A.M.; Menon, B.K.; Eesa, M.; Rempel, J.L.; Thornton, J.; Roy, D.; Jovin, T.G.; Willinsky, R.A.; Sapkota, B.L.; et al. Randomized assessment of rapid endovascular treatment of ischemic stroke. N. Engl. J. Med. 2015, 372, 1019–1030. [Google Scholar] [CrossRef] [PubMed]
- Jovin, T.G.; Chamorro, A.; Cobo, E.; de Miquel, M.A.; Molina, C.A.; Rovira, A.; San Román, L.; Serena, J.; Abilleira, S.; Ribó, M.; et al. Thrombectomy within 8 hours after symptom onset in ischemic stroke. N. Engl. J. Med. 2015, 372, 2296–2306. [Google Scholar] [CrossRef]
- Saver, J.L.; Goyal, M.; Bonafe, A.; Diener, H.C.; Levy, E.I.; Pereira, V.M.; Albers, G.W.; Cognard, C.; Cohen, D.J.; Hacke, W.; et al. Stent-retriever thrombectomy after intravenous t-PA vs. t-PA alone in stroke. N. Engl. J. Med. 2015, 372, 2285–2295. [Google Scholar] [CrossRef]
- Powers, W.J.; Rabinstein, A.A.; Ackerson, T.; Adeoye, O.M.; Bambakidis, N.C.; Becker, K.; Biller, J.; Brown, M.; Demaerschalk, B.M.; Hoh, B.; et al. Guidelines for the Early Management of Patients With Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke 2019, 50, e344–e418. [Google Scholar] [CrossRef] [PubMed]
- Desilles, J.P.; Loyau, S.; Syvannarath, V.; Gonzalez-Valcarcel, J.; Cantier, M.; Louedec, L.; Lapergue, B.; Amarenco, P.; Ajzenberg, N.; Jandrot-Perrus, M.; et al. Alteplase Reduces Downstream Microvascular Thrombosis and Improves the Benefit of Large Artery Recanalization in Stroke. Stroke 2015, 46, 3241–3248. [Google Scholar] [CrossRef] [PubMed]
- Seners, P.; Turc, G.; Maïer, B.; Mas, J.L.; Oppenheim, C.; Baron, J.C. Incidence and Predictors of Early Recanalization After Intravenous Thrombolysis: A Systematic Review and Meta-Analysis. Stroke 2016, 47, 2409–2412. [Google Scholar] [CrossRef] [PubMed]
- Bhatia, R.; Hill, M.D.; Shobha, N.; Menon, B.; Bal, S.; Kochar, P.; Watson, T.; Goyal, M.; Demchuk, A.M. Low Rates of Acute Recanalization With Intravenous Recombinant Tissue Plasminogen Activator in Ischemic Stroke. Stroke 2010, 41, 2254–2258. [Google Scholar] [CrossRef]
- Bellwald, S.; Weber, R.; Dobrocky, T.; Nordmeyer, H.; Jung, S.; Hadisurya, J.; Mordasini, P.; Mono, M.L.; Stracke, C.P.; Sarikaya, H.; et al. Direct Mechanical Intervention Versus Bridging Therapy in Stroke Patients Eligible for Intravenous Thrombolysis: A Pooled Analysis of 2 Registries. Stroke 2017, 48, 3282–3288. [Google Scholar] [CrossRef]
- Wardlaw, J.M.; Murray, V.; Berge, E.; del Zoppo, G.J. Thrombolysis for acute ischaemic stroke. Cochrane Database Syst. Rev. 2014, 2014, Cd000213. [Google Scholar] [CrossRef]
- Kamal, H.; Mehta, B.K.; Ahmed, M.K.; Kavak, K.S.; Zha, A.; Lail, N.S.; Shirani, P.; Al-Mufti, F.; Sawyer, R.N.; Mowla, A. Laboratory factors associated with symptomatic hemorrhagic conversion of acute stroke after systemic thrombolysis. J. Neurol. Sci. 2021, 420, 117265. [Google Scholar] [CrossRef]
- Mowla, A.; Sharifian-Dorche, M.; Mehla, S.; Lail, N.S.; Sharifian-Dorche, A.; Vaughn, C.B.; Sawyer, R.N.; Shirani, P. Safety and efficacy of antiplatelet use before intravenous thrombolysis for acute Ischemic stroke. J. Neurol. Sci. 2021, 425, 117451. [Google Scholar] [CrossRef] [PubMed]
- Alves, H.C.; Treurniet, K.M.; Jansen, I.G.H.; Yoo, A.J.; Dutra, B.G.; Zhang, G.; Yo, L.; van Es, A.; Emmer, B.J.; van den Berg, R.; et al. Thrombus Migration Paradox in Patients with Acute Ischemic Stroke. Stroke 2019, 50, 3156–3163. [Google Scholar] [CrossRef]
- Kaesmacher, J.; Maegerlein, C.; Kaesmacher, M.; Zimmer, C.; Poppert, H.; Friedrich, B.; Boeckh-Behrens, T.; Kleine, J.F. Thrombus Migration in the Middle Cerebral Artery: Incidence, Imaging Signs, and Impact on Success of Endovascular Thrombectomy. J. Am. Heart Assoc. 2017, 6, e005149. [Google Scholar] [CrossRef]
- Weber, R.; Nordmeyer, H.; Hadisurya, J.; Heddier, M.; Stauder, M.; Stracke, P.; Berger, K.; Chapot, R. Comparison of outcome and interventional complication rate in patients with acute stroke treated with mechanical thrombectomy with and without bridging thrombolysis. J. Neurointerv. Surg. 2017, 9, 229–233. [Google Scholar] [CrossRef] [PubMed]
- Broeg-Morvay, A.; Mordasini, P.; Bernasconi, C.; Bühlmann, M.; Pult, F.; Arnold, M.; Schroth, G.; Jung, S.; Mattle, H.P.; Gralla, J.; et al. Direct Mechanical Intervention Versus Combined Intravenous and Mechanical Intervention in Large Artery Anterior Circulation Stroke: A Matched-Pairs Analysis. Stroke 2016, 47, 1037–1044. [Google Scholar] [CrossRef] [PubMed]
- Tsivgoulis, G.; Zand, R.; Katsanos, A.H.; Goyal, N.; Uchino, K.; Chang, J.; Dardiotis, E.; Putaala, J.; Alexandrov, A.W.; Malkoff, M.D.; et al. Safety of intravenous thrombolysis in stroke mimics: Prospective 5-year study and comprehensive meta-analysis. Stroke 2015, 46, 1281–1287. [Google Scholar] [CrossRef] [PubMed]
- Zi, W.; Qiu, Z.; Li, F.; Sang, H.; Wu, D.; Luo, W.; Liu, S.; Yuan, J.; Song, J.; Shi, Z.; et al. Effect of Endovascular Treatment Alone vs Intravenous Alteplase Plus Endovascular Treatment on Functional Independence in Patients With Acute Ischemic Stroke: The DEVT Randomized Clinical Trial. Jama 2021, 325, 234–243. [Google Scholar] [CrossRef] [PubMed]
- Yang, P.; Zhang, Y.; Zhang, L.; Zhang, Y.; Treurniet, K.M.; Chen, W.; Peng, Y.; Han, H.; Wang, J.; Wang, S.; et al. Endovascular Thrombectomy with or without Intravenous Alteplase in Acute Stroke. N. Engl. J. Med. 2020, 382, 1981–1993. [Google Scholar] [CrossRef]
- Suzuki, K.; Matsumaru, Y.; Takeuchi, M.; Morimoto, M.; Kanazawa, R.; Takayama, Y.; Kamiya, Y.; Shigeta, K.; Okubo, S.; Hayakawa, M.; et al. Effect of Mechanical Thrombectomy Without vs With Intravenous Thrombolysis on Functional Outcome Among Patients With Acute Ischemic Stroke: The SKIP Randomized Clinical Trial. Jama 2021, 325, 244–253. [Google Scholar] [CrossRef]
- LeCouffe, N.E.; Kappelhof, M.; Treurniet, K.M.; Rinkel, L.A.; Bruggeman, A.E.; Berkhemer, O.A.; Wolff, L.; van Voorst, H.; Tolhuisen, M.L.; Dippel, D.W.J.; et al. A Randomized Trial of Intravenous Alteplase before Endovascular Treatment for Stroke. N. Engl. J. Med. 2021, 385, 1833–1844. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef]
- Huedo-Medina, T.B.; Sánchez-Meca, J.; Marín-Martínez, F.; Botella, J. Assessing heterogeneity in meta-analysis: Q statistic or I2 index? Psychol. Methods 2006, 11, 193–206. [Google Scholar] [CrossRef]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.; Rothstein, H.R. A basic introduction to fixed-effect and random-effects models for meta-analysis. Res. Synth. Methods 2010, 1, 97–111. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629. [Google Scholar] [CrossRef]
- Du, M.; Li, S.; Huang, X.; Zhang, S.; Bai, Y.; Yan, B.; Guo, H.; Xu, G.; Liu, X. Intravenous Thrombolysis before Thrombectomy may Increase the Incidence of Intracranial Hemorrhage inTreating Carotid T Occlusion. J. Stroke Cerebrovasc. Dis. 2021, 30, 105473. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Wu, X.; Zhu, C.; Mossa-Basha, M.; Malhotra, A. Bridging Thrombolysis Achieved Better Outcomes Than Direct Thrombectomy After Large Vessel Occlusion: An Updated Meta-Analysis. Stroke 2021, 52, 356–365. [Google Scholar] [CrossRef] [PubMed]
- Tong, X.; Wang, Y.; Fiehler, J.; Bauer, C.T.; Jia, B.; Zhang, X.; Huo, X.; Luo, G.; Wang, A.; Pan, Y.; et al. Thrombectomy Versus Combined Thrombolysis and Thrombectomy in Patients With Acute Stroke: A Matched-Control Study. Stroke 2021, 52, 1589–1600. [Google Scholar] [CrossRef]
- Gong, L.; Zheng, X.; Feng, L.; Zhang, X.; Dong, Q.; Zhou, X.; Wang, H.; Zhang, X.; Shu, Z.; Zhao, Y.; et al. Bridging Therapy Versus Direct Mechanical Thrombectomy in Patients with Acute Ischemic Stroke due to Middle Cerebral Artery Occlusion: A Clinical- Histological Analysis of Retrieved Thrombi. Cell Transplant. 2019, 28, 684–690. [Google Scholar] [CrossRef]
- Cappellari, M.; Saia, V.; Pracucci, G.; Sallustio, F.; Gandini, R.; Nappini, S.; Nencini, P.; Vallone, S.; Zini, A.; Bigliardi, G.; et al. Functional and radiological outcomes after bridging therapy versus direct thrombectomy in stroke patients with unknown onset: Bridging therapy versus direct thrombectomy in unknown onset stroke patients with 10-point ASPECTS. Eur. J. Neurol. 2021, 28, 209–219. [Google Scholar] [CrossRef]
- Pienimäki, J.P.; Ollikainen, J.; Sillanpää, N.; Protto, S. In-Hospital Intravenous Thrombolysis Offers No Benefit in Mechanical Thrombectomy in Optimized Tertiary Stroke Center Setting. Cardiovasc. Interv. Radiol. 2021, 44, 580–586. [Google Scholar] [CrossRef]
- Wang, H.; Zi, W.; Hao, Y.; Yang, D.; Shi, Z.; Lin, M.; Wang, S.; Liu, W.; Wang, Z.; Liu, X.; et al. Direct endovascular treatment: An alternative for bridging therapy in anterior circulation large-vessel occlusion stroke. Eur. J. Neurol. 2017, 24, 935–943. [Google Scholar] [CrossRef]
- Mowla, A.; Shakibajahromi, B.; Arora, A.; Seifi, A.; Sawyer, R.N.; Shirani, P. Thrombolysis for stroke in elderly in the late window period. Acta Neurol. Scand. 2021, 144, 663–668. [Google Scholar] [CrossRef]
- Mowla, A.; Memon, A.; Razavi, S.M.; Lail, N.S.; Vaughn, C.B.; Mohammadi, P.; Sawyer, R.N.; Shirani, P. Safety of Intravenous Thrombolysis for Acute Ischemic Stroke in Patients Taking Warfarin with Subtherapeutic INR. J. Stroke Cerebrovasc. Dis. 2021, 30, 105678. [Google Scholar] [CrossRef] [PubMed]
- Shahjouei, S.; Tsivgoulis, G.; Goyal, N.; Sadighi, A.; Mowla, A.; Wang, M.; Seiffge, D.J.; Zand, R. Safety of Intravenous Thrombolysis Among Patients Taking Direct Oral Anticoagulants: A Systematic Review and Meta-Analysis. Stroke 2020, 51, 533–541. [Google Scholar] [CrossRef] [PubMed]
- Mowla, A.; Kamal, H.; Lail, N.S.; Vaughn, C.; Shirani, P.; Mehla, S.; Rajabzadeh-Oghaz, H.; Deline, C.; Ching, M.; Crumlish, A.; et al. Intravenous Thrombolysis for Acute Ischemic Stroke in Patients with Thrombocytopenia. J. Stroke Cerebrovasc. Dis. 2017, 26, 1414–1418. [Google Scholar] [CrossRef] [PubMed]
- AbdelRazek, M.A.; Mowla, A.; Hojnacki, D.; Zimmer, W.; Elsadek, R.; Abdelhamid, N.; Elsadek, L.; Farooq, S.; Kamal, H.; Crumlish, A.; et al. Prior Asymptomatic Parenchymal Hemorrhage Does Not Increase the Risk for Intracranial Hemorrhage after Intravenous Thrombolysis. Cerebrovasc. Dis. 2015, 40, 201–204. [Google Scholar] [CrossRef]
- Mowla, A.; Singh, K.; Mehla, S.; Ahmed, M.K.; Shirani, P.; Kamal, H.; Krishna, C.; Sawyer, R.N., Jr.; Ching, M.; Siddiqui, A.H.; et al. Is acute reperfusion therapy safe in acute ischemic stroke patients who harbor unruptured intracranial aneurysm? Int. J. Stroke 2015, 10 (Suppl. S100), 113–118. [Google Scholar] [CrossRef]
- Singh, K.; Mowla, A.; Mehla, S.; Ahmed, M.K.; Shirani, P.; Zimmer, W.E.; Sawyer, R.N.; Kamal, H.; Crumlish, A.; Ching, M. Safety of intravenous thrombolysis for acute ischemic stroke in patients with preexisting intracranial neoplasms: A case series. Int. J. Stroke 2015, 10, E29–E30. [Google Scholar] [CrossRef]
- Al Kasab, S.; Holmstedt, C.A.; Jauch, E.C.; Schrock, J. Acute ischemic stroke due to large vessel occlusion. Emerg. Med. Rep. 2018, 39. Available online: https://www.reliasmedia.com/articles/142040-acute-ischemic-stroke-due-to-large-vessel-occlusion (accessed on 18 December 2022).
- Brouns, R.; De Deyn, P.P. The complexity of neurobiological processes in acute ischemic stroke. Clin. Neurol. Neurosurg. 2009, 111, 483–495. [Google Scholar] [CrossRef]
- Rossi, R.; Fitzgerald, S.; Molina, S.; Mereuta, O.M.; Douglas, A.; Pandit, A.; Santos, A.M.S.; Murphy, B.; Alderson, J.; Brennan, P.; et al. The administration of rtPA before mechanical thrombectomy in acute ischemic stroke patients is associated with a significant reduction of the retrieved clot area but it does not influence revascularization outcome. J. Thromb. Thrombolysis 2021, 51, 545–551. [Google Scholar] [CrossRef]
- Gralla, J.; Schroth, G.; Remonda, L.; Nedeltchev, K.; Slotboom, J.; Brekenfeld, C. Mechanical thrombectomy for acute ischemic stroke: Thrombus-device interaction, efficiency, and complications in vivo. Stroke 2006, 37, 3019–3024. [Google Scholar] [CrossRef]
- Gralla, J.; Schroth, G.; Remonda, L.; Fleischmann, A.; Fandino, J.; Slotboom, J.; Brekenfeld, C. A dedicated animal model for mechanical thrombectomy in acute stroke. AJNR Am. J. Neuroradiol. 2006, 27, 1357–1361. [Google Scholar] [PubMed]
- Saver, J.L.; Goyal, M.; van der Lugt, A.; Menon, B.K.; Majoie, C.B.; Dippel, D.W.; Campbell, B.C.; Nogueira, R.G.; Demchuk, A.M.; Tomasello, A.; et al. Time to Treatment With Endovascular Thrombectomy and Outcomes From Ischemic Stroke: A Meta-analysis. Jama 2016, 316, 1279–1288. [Google Scholar] [CrossRef] [PubMed]
- Tsivgoulis, G.; Katsanos, A.H.; Schellinger, P.D.; Köhrmann, M.; Varelas, P.; Magoufis, G.; Paciaroni, M.; Caso, V.; Alexandrov, A.W.; Gurol, E.; et al. Successful Reperfusion with Intravenous Thrombolysis Preceding Mechanical Thrombectomy in Large-Vessel Occlusions. Stroke 2018, 49, 232–235. [Google Scholar] [CrossRef] [PubMed]
- Mishra, S.M.; Dykeman, J.; Sajobi, T.T.; Trivedi, A.; Almekhlafi, M.; Sohn, S.I.; Bal, S.; Qazi, E.; Calleja, A.; Eesa, M.; et al. Early reperfusion rates with IV tPA are determined by CTA clot characteristics. AJNR Am. J. Neuroradiol. 2014, 35, 2265–2272. [Google Scholar] [CrossRef] [PubMed]
- Behrens, L.; Möhlenbruch, M.; Stampfl, S.; Ringleb, P.A.; Hametner, C.; Kellert, L.; Pham, M.; Herweh, C.; Bendszus, M.; Rohde, S. Effect of thrombus size on recanalization by bridging intravenous thrombolysis. Eur. J. Neurol. 2014, 21, 1406–1410. [Google Scholar] [CrossRef]
- Rha, J.H.; Saver, J.L. The impact of recanalization on ischemic stroke outcome: A meta-analysis. Stroke 2007, 38, 967–973. [Google Scholar] [CrossRef]
- Zhang, J.; Chen, S.; Shi, S.; Zhang, Y.; Kong, D.; Xie, Y.; Deng, X.; Tang, J.; Luo, J.; Liang, Z. Direct endovascular treatment versus bridging therapy in patients with acute ischemic stroke eligible for intravenous thrombolysis: Systematic review and meta-analysis. J. NeuroInterventional Surg. 2022, 14, 321. [Google Scholar] [CrossRef]
- Whiteley, W.N.; Emberson, J.; Lees, K.R.; Blackwell, L.; Albers, G.; Bluhmki, E.; Brott, T.; Cohen, G.; Davis, S.; Donnan, G.; et al. Risk of intracerebral haemorrhage with alteplase after acute ischaemic stroke: A secondary analysis of an individual patient data meta-analysis. Lancet Neurol. 2016, 15, 925–933. [Google Scholar] [CrossRef]
- Emberson, J.; Lees, K.R.; Lyden, P.; Blackwell, L.; Albers, G.; Bluhmki, E.; Brott, T.; Cohen, G.; Davis, S.; Donnan, G.; et al. Effect of treatment delay, age, and stroke severity on the effects of intravenous thrombolysis with alteplase for acute ischaemic stroke: A meta-analysis of individual patient data from randomised trials. Lancet 2014, 384, 1929–1935. [Google Scholar] [CrossRef]
- Zambrano Espinoza, M.D.; Lail, N.S.; Vaughn, C.B.; Shirani, P.; Sawyer, R.N.; Mowla, A. Does Body Mass Index Impact the Outcome of Stroke Patients Who Received Intravenous Thrombolysis? Cerebrovasc. Dis. 2021, 50, 141–146. [Google Scholar] [CrossRef]
- Mowla, A.; Shah, H.; Lail, N.S.; Vaughn, C.B.; Shirani, P.; Sawyer, R.N. Statins Use and Outcome of Acute Ischemic Stroke Patients after Systemic Thrombolysis. Cerebrovasc. Dis. 2020, 49, 503–508. [Google Scholar] [CrossRef] [PubMed]
- Keep, R.F.; Zhou, N.; Xiang, J.; Andjelkovic, A.V.; Hua, Y.; Xi, G. Vascular disruption and blood-brain barrier dysfunction in intracerebral hemorrhage. Fluids Barriers CNS 2014, 11, 18. [Google Scholar] [CrossRef] [PubMed]
- Docagne, F.; Parcq, J.; Lijnen, R.; Ali, C.; Vivien, D. Understanding the functions of endogenous and exogenous tissue-type plasminogen activator during stroke. Stroke 2015, 46, 314–320. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, Y.; Nagai, N.; Yamakawa, K.; Kawakami, J.; Lijnen, H.R.; Umemura, K. Tissue-type plasminogen activator (t-PA) induces stromelysin-1 (MMP-3) in endothelial cells through activation of lipoprotein receptor-related protein. Blood 2009, 114, 3352–3358. [Google Scholar] [CrossRef]
- Ning, M.; Furie, K.L.; Koroshetz, W.J.; Lee, H.; Barron, M.; Lederer, M.; Wang, X.; Zhu, M.; Sorensen, A.G.; Lo, E.H.; et al. Association between tPA therapy and raised early matrix metalloproteinase-9 in acute stroke. Neurology 2006, 66, 1550–1555. [Google Scholar] [CrossRef] [PubMed]
- Hao, Y.; Yang, D.; Wang, H.; Zi, W.; Zhang, M.; Geng, Y.; Zhou, Z.; Wang, W.; Xu, H.; Tian, X.; et al. Predictors for Symptomatic Intracranial Hemorrhage After Endovascular Treatment of Acute Ischemic Stroke. Stroke 2017, 48, 1203–1209. [Google Scholar] [CrossRef] [PubMed]
- Jiang, F.; Zhao, W.; Wu, C.; Zhang, Z.; Li, C.; Che, R.; Chen, J.; Hu, W.; Song, H.; Duan, J.; et al. Asymptomatic Intracerebral Hemorrhage May Worsen Clinical Outcomes in Acute Ischemic Stroke Patients Undergoing Thrombectomy. J. Stroke Cerebrovasc. Dis. 2019, 28, 1752–1758. [Google Scholar] [CrossRef] [PubMed]
- Constant Dit Beaufils, P.; Preterre, C.; De Gaalon, S.; Labreuche, J.; Mazighi, M.; Di Maria, F.; Sibon, I.; Marnat, G.; Gariel, F.; Blanc, R.; et al. Prognosis and risk factors associated with asymptomatic intracranial hemorrhage after endovascular treatment of large vessel occlusion stroke: A prospective multicenter cohort study. Eur. J. Neurol. 2021, 28, 229–237. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study | Study Design | Country | Year(s) of Study | Occlusion Site(s) | Alteplase Dosage (mg per kg) |
|---|---|---|---|---|---|
| Yang P. et al. [45] | RCT | China | 2019 | ICA, M1 and M2 | 0.9 |
| Zi W. et al. [44] | RCT | China | 2018–2020 | ICA and M1 | 0.9 |
| Suzuki K. et al. [46] | RCT | Japan | 2017–2019 | ICA and M1 | 0.6 |
| LeCouffe N. E. et al. [47] | RCT | Netherlands, France and Belgium | 2020 | ICA, M1 and M2 | 0.9 |
| Broeg–Morvay A. et al. [42] | Retrospective observational | Switzerland | 2009–2014 | ICA, M1 and M2 | 0.9 or 0.6 |
| Bellwald S. et al. [35] | Retrospective observational | Switzerland, Germany | 2009–2014 | ICA, M1 and M2 | 0.9 or 0.6 |
| Gong L. et al. [56] | Retrospective observational | China | 2015–2018 | MCA | No data |
| Weber R. et al. [41] | Retrospective observational | Germany | 2012–2013 | ICA, M1, M2, carotid T, basilar, A1, P1 and vertebral artery | 0.9 or 0.6 |
| Cappellari M. et al. [57] | Prospective cohort | Italy | 2011–2017 | ICA, M1 and M2 | No data |
| Du M. et al [53] | Retrospective observational | China | 2015–2018 | Carotid T | 0.9 |
| Pienimäki J. P. et al. [58] | Retrospective observational | Finland | 2016–2019 | ICA and M1 | 0.9 |
| Tong X. et al. [55] | Prospective observational | China | 2017–2019 | ICA, M1, M2, A1, A2, vertebrobasilar and P1 | 0.9 |
| Wang H. et al. [59] | Retrospective observational | China | 2014–2016 | ICA, M1, M2 and A1 | 0.9 |
| Study | Number of Patients | Male % | Median Age (Years) | Onset NIHSS (Median) | DM | HTN | AF | Smoking | Cardiac Disease | HLP | Anticoagulant Use | ASA/Antiplatelet Use | Prior Stroke | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Yang P. et al. [45] | dMT | 327 | 57.8 | 69 | 17 | 59 | 193 | 152 | 73 | 24 | 13 | 28 | 48 | 43 |
| BT | 329 | 55 | 69 | 17 | 65 | 201 | 149 | 68 | 17 | 14 | 36 | 56 | 47 | |
| Zi W. et al. [44] | dMT | 116 | 56.9 | 70 | 16 | 25 | 69 | 62 | 28 | 30 | 18 | NDA | NDA | 14 |
| BT | 118 | 55.9 | 70 | 16 | 20 | 74 | 62 | 29 | 19 | 22 | NDA | NDA | 19 | |
| Suzuki K. et al. [46] | dMT | 101 | 55 | 74 | 19 | 16 | 61 | 57 | 42 | 7 | 30 | 19 | 16 | 12 |
| BT | 103 | 70 | 76 | 17 | 17 | 61 | 64 | 54 | 7 | 37 | 17 | 18 | 14 | |
| LeCouffe N. E. et al. [47] | dMT | 273 | 59 | 72 | 16 | 40 | 121/273 | 86 | 73/263 | 15 | 79 | 15 | 94 | 47 |
| BT | 266 | 54 | 69 | 16 | 50 | 139/265 | 63 | 66/260 | 15 | 73 | 20 | 96 | 43 | |
| Broeg-Morvay A. et al. [42] | dMT | 40 | 62.5 | 77 * | 17 | 5 | 30 | 19 | 33 | 12 | 30 | NDA | NDA | NDA |
| BT | 156 | 52.6 | 73 * | 15 | 28 | 100 | 61 | 8 | 24 | 83 | NDA | NDA | NDA | |
| Bellwald S. et al. [35] | dMT | 103 | 55.9 | 75 * | 16 | † 17/108 | † 85/111 | † 47/101 | † 21/104 | † 29/107 | † 46/108 | NDA | NDA | NDA |
| BT | 103 | 52.4 | 75 * | 16 | † 42/246 | † 171/246 | † 85/227 | † 47/214 | † 40/241 | † 98/242 | NDA | NDA | NDA | |
| Gong L. et al. [56] | dMT | 21 | 52 | 71 * | 15 | 5 | 13 | 19 | NDA | NDA | NDA | NDA | NDA | NDA |
| BT | 21 | 57 | 70 * | 14 | 4 | 15 | 19 | NDA | NDA | NDA | NDA | NDA | NDA | |
| Weber R. et al. [41] | dMT | 70 | 38 | 70.7 | 15 | 11 | 49 | 25 | 12 | NDA | 31 | NDA | NDA | 34 |
| BT | 105 | 52 | 70.2 | 15.5 | 16 | 82 | 26 | 15 | NDA | 17 | NDA | NDA | 13 | |
| Cappellari M. et al. [57] | dMT | 212 | 47 | 70.4 * | 16 & 19 ‡ | 31 | 116 | 52 | NDA | NDA | NDA | 11 | 82 | 12 |
| BT | 371 | 45 | 70.3 * | 17 & 18 ‡ | 38 | 218 | 76 | NDA | NDA | NDA | 12 | 123 | 13 | |
| Du M. et al. [53] | dMT | 57 | 32 | 66.9 * | 18 | 12 | 33 | 33 | 15 | 17 | NDA | 10 | 39 | 7 |
| BT | 54 | 28 | 65.2 * | 18 | 7 | 28 | 31 | 10 | 10 | NDA | 9 | 39 | 5 | |
| Pienimaki J et al. [58] | dMT | 48 | 62 | 72 * | 14 | 11 | 31 | 19 | NDA | 7 | NDA | NDA | NDA | NDA |
| BT | 58 | 64 | 69 * | 16.5 | 13 | 29 | 37 | NDA | 12 | NDA | NDA | NDA | NDA | |
| Tong X. et al. [55] | dMT | 394 | 64.7 | 65 | 17 | 67 | 214 | 124 | 165 | 76 | 26 | 7 | 56 | 76 |
| BT | 394 | 62.7 | 65 | 16 | 63 | 214 | 124 | 166 | 63 | 31 | 4 | 60 | 63 | |
| Wang H. et al. [59] | dMT | 138 | 76 | 67 | 16 | † 38/203 | † 130/203 | † 92/203 | † 49/203 | † 557/203 | NDA | 9 | NDA | 15 |
| BT | 138 | 78 | 67 | 17 | † 27/160 | † 99/160 | † 75/160 | † 43/160 | † 32/160 | NDA | 0 | NDA | 16 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kolahchi, Z.; Rahimian, N.; Momtazmanesh, S.; Hamidianjahromi, A.; Shahjouei, S.; Mowla, A. Direct Mechanical Thrombectomy Versus Prior Bridging Intravenous Thrombolysis in Acute Ischemic Stroke: A Systematic Review and Meta-Analysis. Life 2023, 13, 185. https://doi.org/10.3390/life13010185
Kolahchi Z, Rahimian N, Momtazmanesh S, Hamidianjahromi A, Shahjouei S, Mowla A. Direct Mechanical Thrombectomy Versus Prior Bridging Intravenous Thrombolysis in Acute Ischemic Stroke: A Systematic Review and Meta-Analysis. Life. 2023; 13(1):185. https://doi.org/10.3390/life13010185
Chicago/Turabian StyleKolahchi, Zahra, Nasrin Rahimian, Sara Momtazmanesh, Anahid Hamidianjahromi, Shima Shahjouei, and Ashkan Mowla. 2023. "Direct Mechanical Thrombectomy Versus Prior Bridging Intravenous Thrombolysis in Acute Ischemic Stroke: A Systematic Review and Meta-Analysis" Life 13, no. 1: 185. https://doi.org/10.3390/life13010185
APA StyleKolahchi, Z., Rahimian, N., Momtazmanesh, S., Hamidianjahromi, A., Shahjouei, S., & Mowla, A. (2023). Direct Mechanical Thrombectomy Versus Prior Bridging Intravenous Thrombolysis in Acute Ischemic Stroke: A Systematic Review and Meta-Analysis. Life, 13(1), 185. https://doi.org/10.3390/life13010185