
Comparison of the Use of Desflurane vs. Propofol in Aortic Valve Replacement Surgery: Differences in Nephroprotection: An Explorative and Hypothesis-Generating Study

 ,
,
Abstract
:1. Introduction
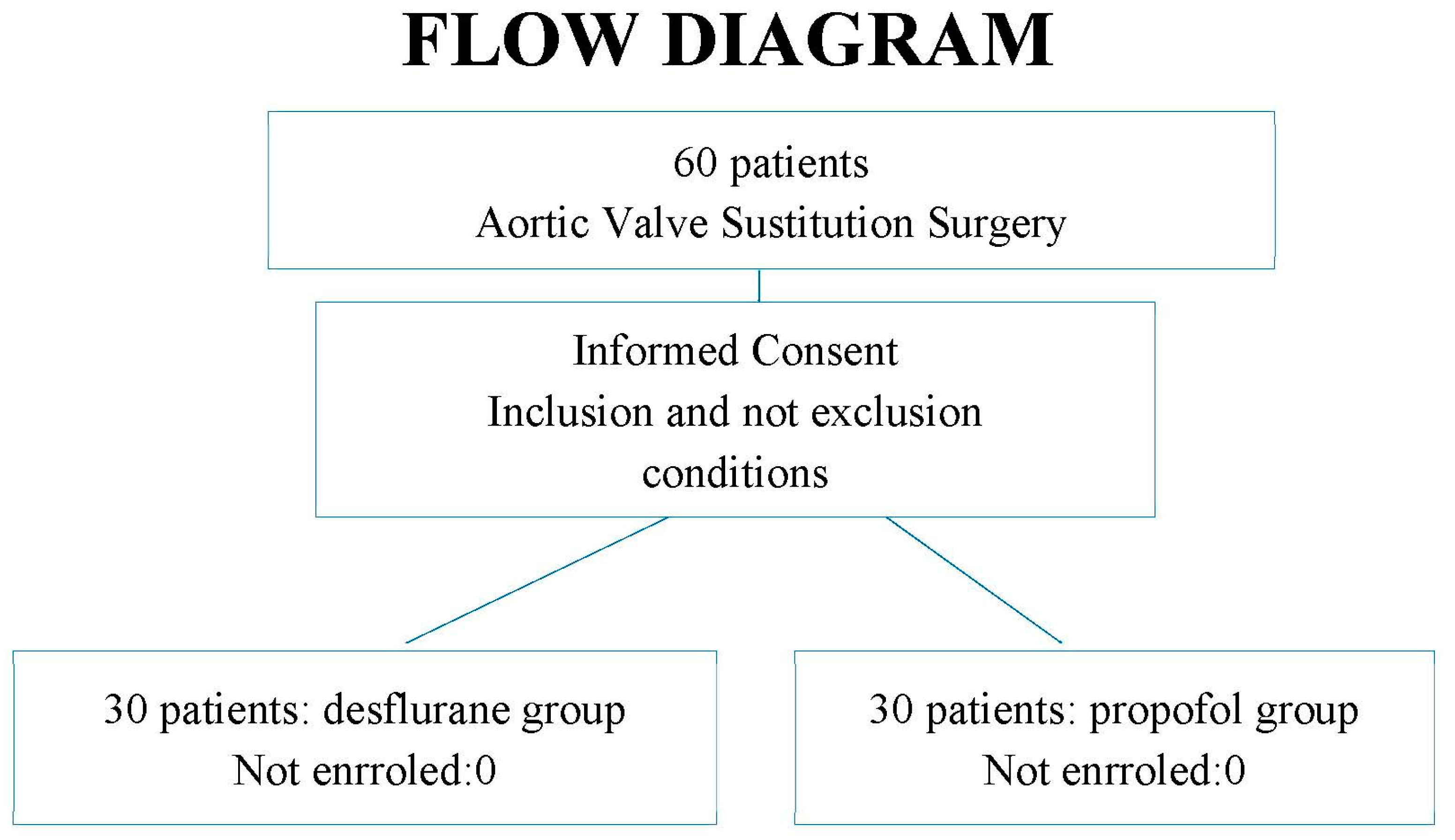
2. Materials and Methods
2.1. Sample Size Justification
2.2. Statistical Analysis
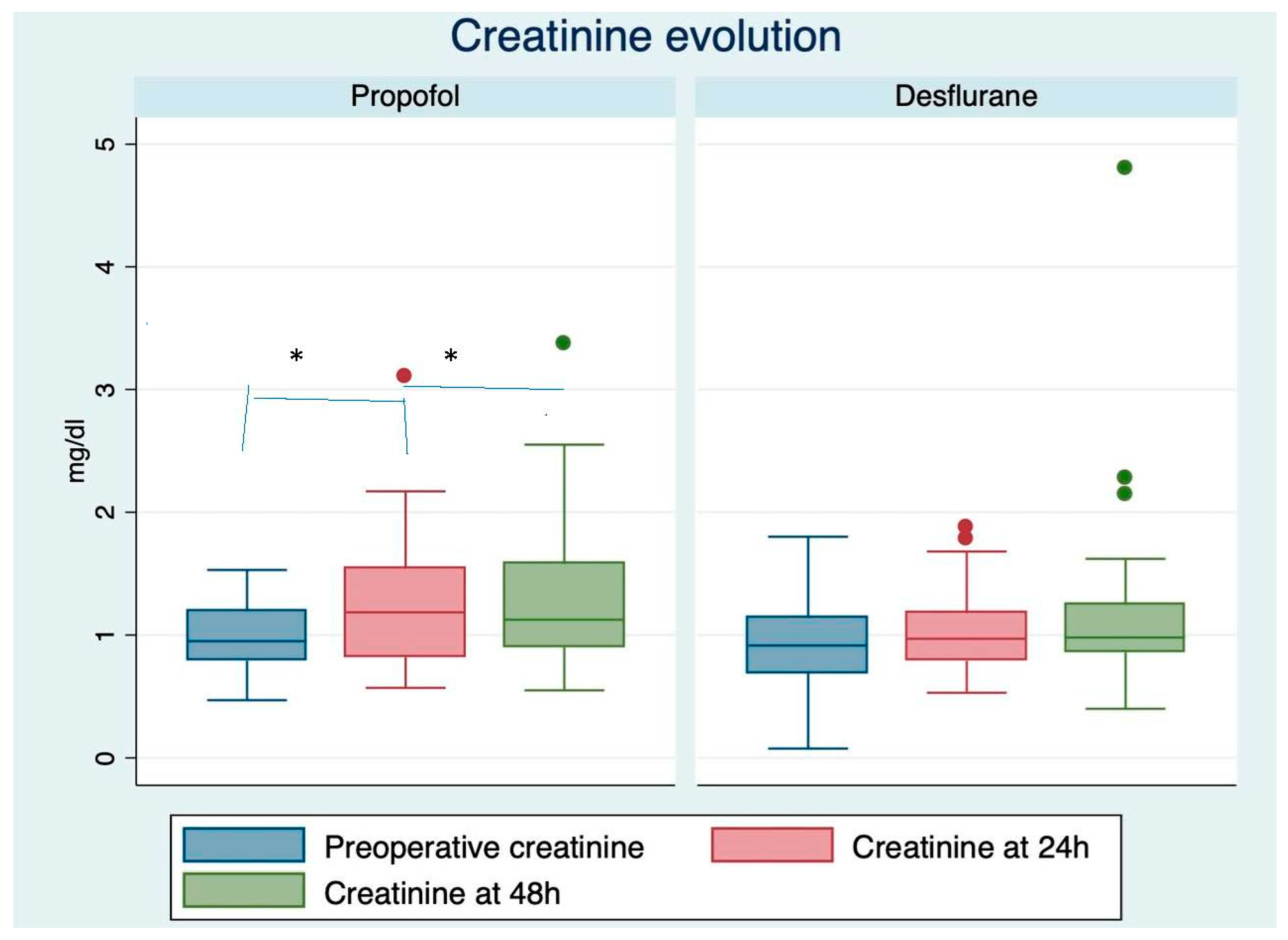
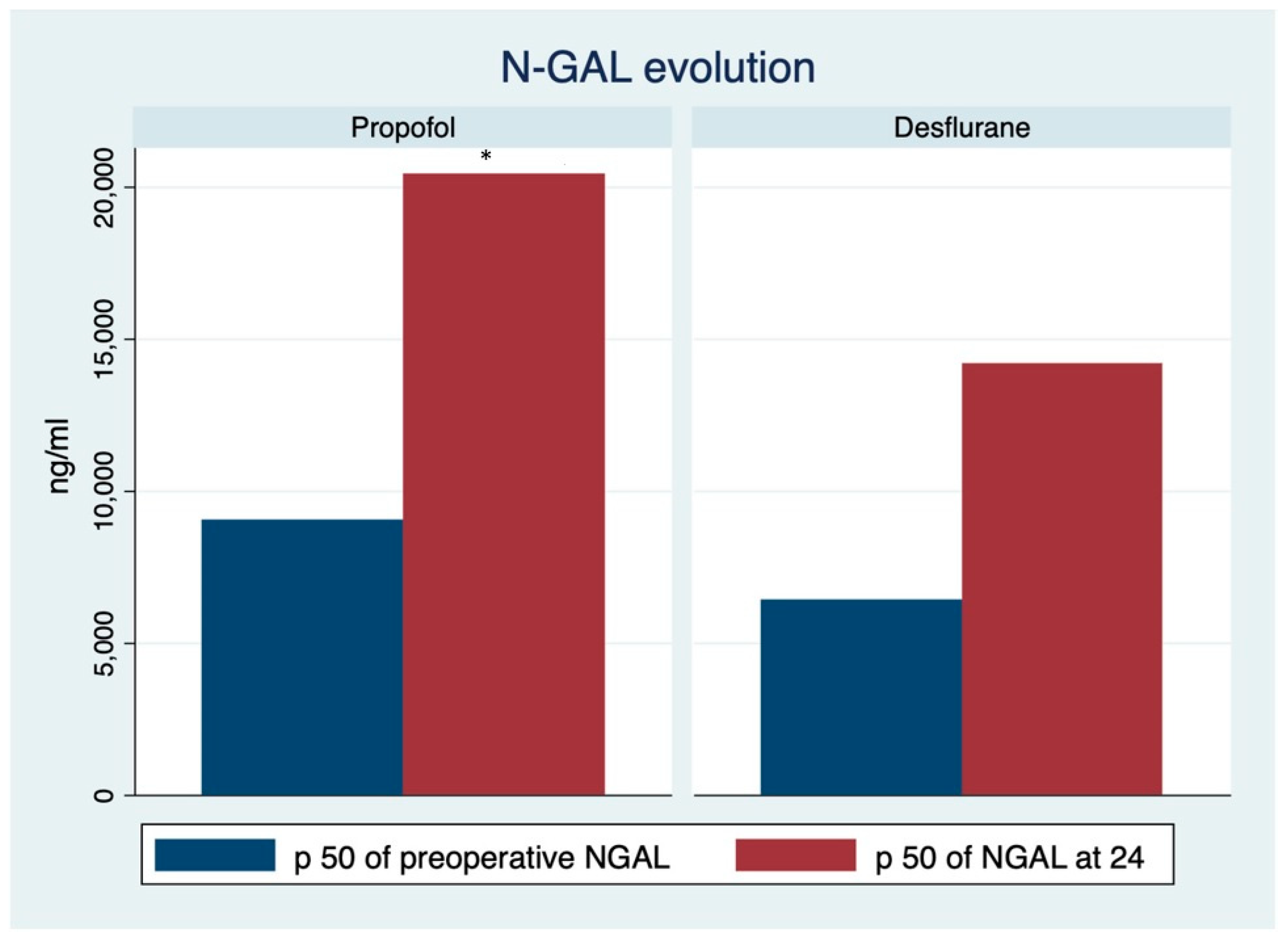
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- De Hert, S.G.; Broecke, P.W.T.; Mertens, E.; Van Sommeren, E.W.; De Blier, I.G.; Stockman, B.A.; Rodrigus, I.E. Sevoflurane but Not Propofol Preserves Myocardial Function in Coronary Surgery Patients. Anesthesiology 2002, 97, 42–49. [Google Scholar] [CrossRef] [PubMed]
- De Hert, S.G.; Van Der Linden, P.J.; Cromheecke, S.S.; Meeus, R.; Broecke, P.P.T.; De Blier, I.I.; Stockman, B.B.; Rodrigus, I.I. Choice of Primary Anesthetic Regimen Can Influence Intensive Care Unit Length of Stay after Coronary Surgery with Cardiopulmonary Bypass. Anesthesiology 2004, 101, 9–20. [Google Scholar] [CrossRef] [PubMed]
- De Hert, S.G.; Van Der Linden, P.J.; Cromheecke, S.S.; Meeus, R.; Nelis, A.A.; Van Reeth, V.V.; Broecke, P.P.T.; De Blier, I.I.; Stockman, B.B.; Rodrigus, I.I. Cardioprotective Properties of Sevoflurane in Patients Undergoing Coronary Surgery with Cardiopulmonary Bypass Are Related to the Modalities of Its Administration. Anesthesiology 2004, 101, 299–310. [Google Scholar] [CrossRef] [PubMed]
- De Hert, S.G.; Cromheecke, S.; Broecke, P.W.T.; Mertens, E.; De Blier, I.G.; Stockman, B.A.; Rodrigus, I.E.; Van Der Linden, P.J. Effects of Propofol, Desflurane, and Sevoflurane on Recovery of Myocardial Function after Coronary Surgery in Elderly High-risk Patients. Anesthesiology 2003, 99, 314–323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warltier, D.C.; Al-Wathiqui, M.H.; Kampine, J.P.; Schmeling, W.T. Recovery of contractile function of stunned myocardium in chronically instrumented dogs is enhanced by halothane or isoflurane. Anesthesiology 1988, 69, 552–565. [Google Scholar] [CrossRef]
- Guerrero Orriach, J.L.; Galán Ortega, M.; Ramirez Fernandez, A.; Ramirez Aliaga, M.; Moreno Cortes, M.I.; Ariza Villanueva, D.; Florez Vela, A.; Alcaide Torres, J.; Santiago Fernandez, C.; Matute Gonzalez, E.; et al. Cardioprotective efficacy of sevoflurane vs. propofol during induction and/or maintenance in patients undergoing coronary artery revascularization surgery with-out pump: A randomized trial. Int. J. Cardiol. 2017, 243, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Gross, E.R.; Gross, G.J. Ligand triggers of classical anesthetic preconditioning and anesthetic postconditioning. Cardiovasc. Res. 2006, 70, 212–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orriach, J.L.G.; Ortega, M.G.; Aliaga, M.R.; Iglesias, P.; Navarro, M.R.; Mañas, J.C. Prolonged sevoflurane administration in the off-pump coronary artery bypass graft surgery: Beneficial effects. J. Crit. Care 2013, 28, 879.e13–879.e18. [Google Scholar] [CrossRef]
- Guerrero Orriach, J.L.; Aliaga, M.R.; Galan Ortega, M.; Rubio Navarro, M.; Navarro Arce, I.; Cruz Mañas, J. Sevoflurane in intraoperative and postoperative cardiac surgery patients. Our experience in intensive care unit with sevoflurane sedation. Curr. Pharm. Des. 2013, 19, 3996–4002. [Google Scholar] [CrossRef]
- Julier, K.; da Silva, R.; Garcia, C.; Bestmann, L.; Frascarolo, P.; Zollinger, A.; Chassot, P.-G.; Schmid, E.R.; Turina, M.I.; von Sagesser, L.K.; et al. Anesthetic preconditioning by sevoflurane decreases biochemical markers for myocardialand renal dysfunction in coronary artery bypass graft surgery: A double-blinded, placebo-controlled, multicenter study. Anesthesiology 2003, 98, 1315–1327. [Google Scholar] [CrossRef] [PubMed]
- Guerrero Orriach, J.L.; Escalona Belmonte, J.J.; Ramirez Aliaga, M.; Ramirez Fernandez, A.; Raigón Ponferrada, A.; Rubio Navarro, M.; Cruz Mañas, J. Anesthetic-induced Myocardial Conditioning: Molecular Fundamentals and Scope. Curr. Med. Chem. 2020, 27, 2147–2160. [Google Scholar] [CrossRef] [PubMed]
- Landoni, G.; Lomivorotov, V.V.; Neto, C.N.; Monaco, F.; Pasyuga, V.V.; Bradic, N.; Lembo, R.; Gazivoda, G.; Likhvantsev, V.V.; Lei, C.; et al. Volatile Anesthetics versus Total Intravenous Anesthesia for Cardiac Surgery. N. Engl. J. Med. 2019, 380, 1214–1225. [Google Scholar] [CrossRef] [PubMed]
- Vela, J.P.; Benítez, J.M.; González, M.C.; De La Cal López, M.A.; Pérez, R.H.; Meneses, V.S.; del Nogal Saez, F.; Grupo de Trabajo de Cuidados Intensivos Cardiológicos y RCP de SEMICYUC, con el aval científico de la SEMICYUC. Guías de práctica clínica para el manejo del síndrome de bajo gasto cardíaco en el postoperatorio de ci-rugía cardíaca [Clinical practice guide for the management of low cardiac output syndrome in the postoperative period of heart surgery]. Med. Intensiva 2012, 36, e1–e44. [Google Scholar] [CrossRef]
- Mehta, R.L.; Kellum, J.A.; Shah, S.V.; Molitoris, B.A.; Ronco, C.; Warnock, D.G.; Levin, A.; Acute Kidney Injury Network. Acute Kidney Injury Network: Report of an initiative to improve outcomes in acute kidney injury. Crit Care 2007, 11, R31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prabhu, A.; Sujatha, D.I.; Ninan, B.; Vijayalakshmi, M.A. Neutrophil Gelatinase Associated Lipocalin as a Biomarker for Acute Kidney Injury in Patients Undergoing Coronary Artery Bypass Grafting with Cardiopulmonary Bypass. Ann. Vasc. Surg. 2010, 24, 525–531. [Google Scholar] [CrossRef] [PubMed]
- Kunst, G.; Klein, A. Peri-operative anaesthetic myocardial preconditioning and protection—Cellular mechanisms and clinical relevance in cardiac anaesthesia. Anaesthesia 2015, 70, 467–482. [Google Scholar] [CrossRef] [PubMed]
- De Hert, S.G.; Turani, F.; Mathur, S.; Stowe, D. Cardioprotection with Volatile Anesthetics: Mechanisms and Clinical Implications. Anesth. Analg. 2005, 100, 1584–1593. [Google Scholar] [CrossRef] [PubMed]
- Guerrero Orriach, J.L.; Navarro Arce, I.; Hernandez Rodriguez, P.; Raigón Ponferrada, A.; Malo Manso, A.; Ramirez Aliaga, M.; Ramirez Fernandez, A.; Escalona Belmonte, J.J.; Bellido Estevez, I.; Gomez Luque, A.; et al. Preservation of renal function in cardiac surgery patients with LCOS: Levosimendan vs. beta agonists. BMC Anesthesiol. 2019, 19, 212. [Google Scholar] [CrossRef] [PubMed]
- Guerrero-Orriach, J.L.; Ariza-Villanueva, D.; Florez-Vela, A.; Garrido-Sánchez, L.; Moreno-Cortés, M.I.; Galán-Ortega, M.; Ramírez-Fernández, A.; Torres, J.A.; Fernandez, C.S.; Arce, I.N.; et al. Cardiac, renal, and neurological benefits of preoperative levosimendan administration in patients with right ventricular dysfunction and pulmonary hypertension undergoing cardiac surgery: Evaluation with two biomarkers neutrophil gelatinase-associated lipocalin and neuronal enolase. Ther. Clin. Risk Manag. 2016, 21, 623–630. [Google Scholar]
- Guerrero-Orriach, J.L.; Belmonte, J.J.E.; Fernandez, A.R.; Aliaga, M.R.; Navarro, M.R.; Mañas, J.C. Cardioprotection with halogenated gases: How does it occur? Drug Des. Dev. Ther. 2017, 16, 837–849. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- EP07-A2; Interference Testing in Clinical Chemistry; Approved Guideline—Second Edition. Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2010.




{kind=link}
{kind=link}
{kind=link}
| Desflurane | Propofol | p | |
|---|---|---|---|
| Clamping time (min) | 43 +/− 8 | 45 +/− 12 | 0.84 |
| ECC time (min) | 83 +/− 5 | 82 +/− 7 | 0.95 |
| Age (years) | 65 +/− 4 | 68 +/− 6 | 0.33 |
| Gender (M/F) | 0.47 | 0.57 | 0.44 |
| Variable | Propofol | Desflurane | p |
|---|---|---|---|
| CVP Pre | 75 +/− 4 | 72 +/− 6 | 0.11 |
| NT-ProBNP pre | 846.3 +/− 345 | 1283.5 +/− 256 | 0.35/0.92 |
| CPR pre | 4.71 +/− 0.65 | 3.03 +/− 1.2 | 0.29/0.94 |
| CKMb pre | 13.11 +/− 2.1 | 1.95 +/− 1.3 | 0.12/0.08 |
| CVS 24 h | 69.1 +/− 2 | 71.5 +/− 1.5 | 0.29 |
| NT-ProBNP 24 h | 2338.9 +/−/− 154 | 2744.5 +/− 358 | 0.58/0.9 |
| CRP 24 h | 146.3 +/− 12.3 | 149.1 +/− 12.7 | 0.83 |
| CKMMB 24 h | 17.4 +/− 3.54 | 16.3 +/− 2.58 | 0.7/0.28 |
| Tropo 24 h | 2.8 +/− 0.32 | 7.8 +/− 0.33 | 0.25/0.52 |
| Lactate 24 h | 1.76 +/− 0.1 | 1.65 +/− 0.2 | 0.59/0.68 |
| Norepinephrine 24 h | 37% | 38% | 0.92 |
| LCOS 24 h | 30% | 20% | 0.37 |
| MAP 24 h | 74 +/− 12 | 77 +/− 9 | 0.35 |
| HCT 24 h | 33.7 + −/− 5 | 32.5 +/− 2.8 | 0.23 |
| CVS 48 h | 71 +/− 5 | 71 +/− 6 | 0.87/0.25 |
| CKMMB 48 | 10.3 +/− 2.36 | 7.7 +/− 5.8 | 0.47/0.68 |
| Tropo 48 h | 1.73 +/− 0.45 | 2 +/− 0.38 | 0.42/0.87 |
| Lactate 48 h | 1.39 +/− 0.35 | 1.31 +/− 0.45 | 0.57/0.48 |
| Norepinephrine 48 h | 40% | 20% | 0.09 |
| LCOS 48 h | 23% | 13% | 0.32 |
| MAP 48 h | 77.7 +/− 6 | 79.6 +/− 8 | 0.47 |
| HCT 48 h | 31.3 +/− 1.2 | 31.3 +/−1.4 | 0.95 |
| AKI 24 | Propofol | Desflurane |
|---|---|---|
| 0 | 17 | 23 |
| Percentage in this stage | 28.33 | 40 |
| 1 | 11 | 5 |
| Percentage in this stage | 18.33 | 8.33 |
| 2 | 2 | 2 |
| Percentage in this stage | 3.33 | 3.33 |
| 3 | 0 | 0 |
| Percentage in this stage | 0 | 0 |
| AKI 48 | Propofol | Desflurane |
| 0 | 17 | 20 |
| Percentage in this stage | 28.33 | 33.33 |
| 1 | 12 | 9 |
| Percentage in this stage | 20.00 | 15.00 |
| 2 | 1 | 0 |
| Percentage in this stage | 1.67 | 0.00 |
| 3 | 0 | 1 |
| Percentage in this stage | 0.00 | 1.67 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guerrero Orriach, J.L.; Malo-Manso, A.; Nuñez Galo, M.; Bellido Estevez, I.; Ruiz Salas, A.; Cruz Mañas, J.; Garrido-Sanchez, L.; Gonzalez-Alvarez, L. Comparison of the Use of Desflurane vs. Propofol in Aortic Valve Replacement Surgery: Differences in Nephroprotection: An Explorative and Hypothesis-Generating Study. Life 2022, 12, 1172. https://doi.org/10.3390/life12081172
Guerrero Orriach JL, Malo-Manso A, Nuñez Galo M, Bellido Estevez I, Ruiz Salas A, Cruz Mañas J, Garrido-Sanchez L, Gonzalez-Alvarez L. Comparison of the Use of Desflurane vs. Propofol in Aortic Valve Replacement Surgery: Differences in Nephroprotection: An Explorative and Hypothesis-Generating Study. Life. 2022; 12(8):1172. https://doi.org/10.3390/life12081172
Chicago/Turabian StyleGuerrero Orriach, Jose Luis, Alfredo Malo-Manso, Mercedes Nuñez Galo, Inmaculada Bellido Estevez, Amalio Ruiz Salas, Jose Cruz Mañas, Lourdes Garrido-Sanchez, and Laura Gonzalez-Alvarez. 2022. "Comparison of the Use of Desflurane vs. Propofol in Aortic Valve Replacement Surgery: Differences in Nephroprotection: An Explorative and Hypothesis-Generating Study" Life 12, no. 8: 1172. https://doi.org/10.3390/life12081172
APA StyleGuerrero Orriach, J. L., Malo-Manso, A., Nuñez Galo, M., Bellido Estevez, I., Ruiz Salas, A., Cruz Mañas, J., Garrido-Sanchez, L., & Gonzalez-Alvarez, L. (2022). Comparison of the Use of Desflurane vs. Propofol in Aortic Valve Replacement Surgery: Differences in Nephroprotection: An Explorative and Hypothesis-Generating Study. Life, 12(8), 1172. https://doi.org/10.3390/life12081172