
eHealthResp, a Digital Intervention to Improve Antibiotic Prescribing in Respiratory Infections: A Pilot Study

 ,
,  ,
,  ,
,  , , and
, , and 
Abstract
1. Introduction
2. Methods
2.1. Setting
2.2. Pilot Study
2.2.1. eHealthResp Online Course
2.2.2. eHealthResp Mobile Application
2.3. Global Content Validation Questionnaire
2.4. Statistical Analysis
2.5. Ethics Statement
3. Results
3.1. Sociodemographic Characteristics of the Physicians
3.2. Evaluation of the eHealthResp Online Course
3.3. Evaluation of the eHealthResp Mobile Application
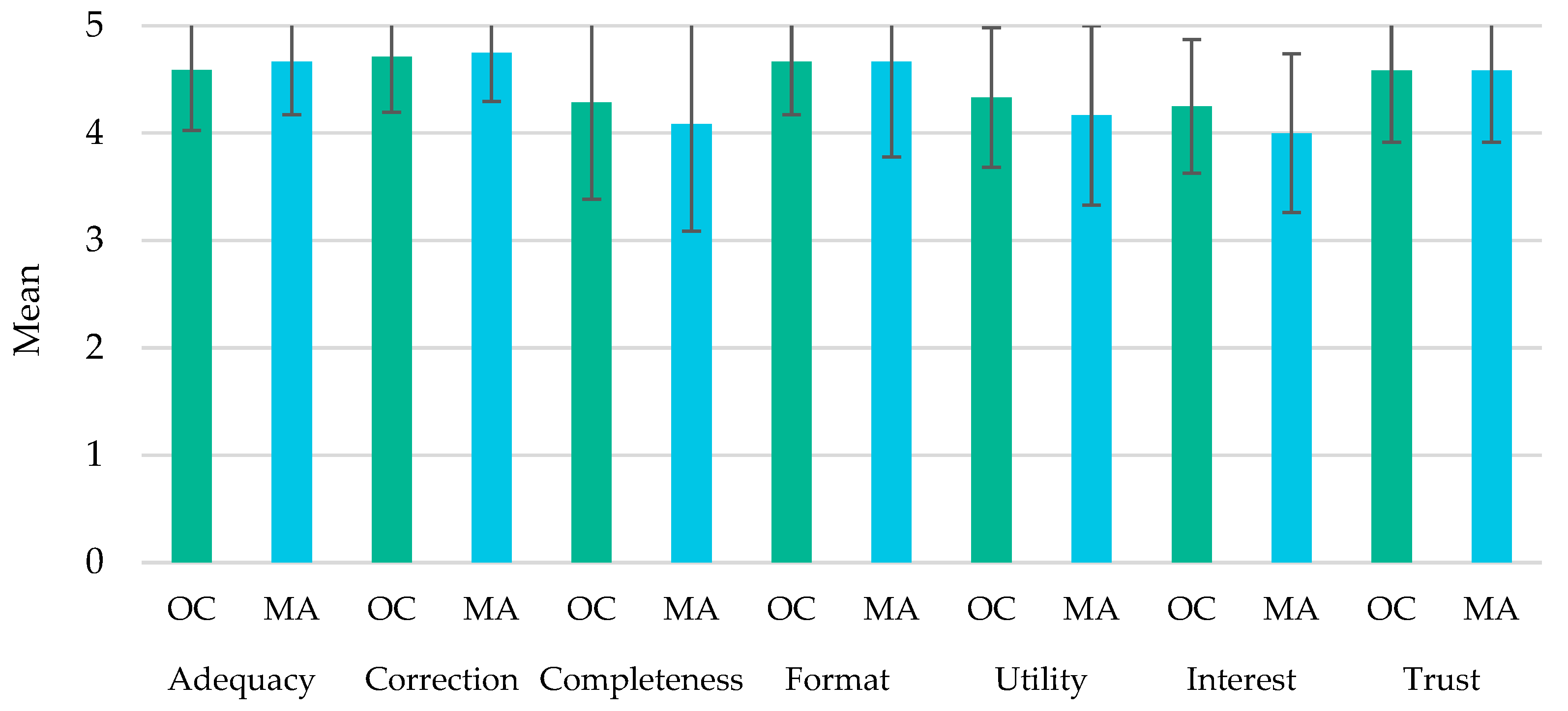
3.4. Comparison between the eHealthResp Online Course and Mobile Application
3.5. Qualitative Evaluation of Physicians’ Feedback
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Laws, M.; Shaaban, A.; Rahman, K.M. Antibiotic Resistance Breakers: Current Approaches and Future Directions. FEMS Microbiol. Rev. 2019, 43, 490–516. [Google Scholar] [CrossRef]
- Klein, E.Y.; Boeckel, T.P.V.; Martinez, E.M.; Pant, S.; Gandra, S.; Levin, S.A.; Goossens, H.; Laxminarayan, R. Global Increase and Geographic Convergence in Antibiotic Consumption between 2000 and 2015. Proc. Natl. Acad. Sci. USA 2018, 115, E3463–E3470. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Ten Threats to Global Health in 2019. 2022. Available online: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019 (accessed on 1 June 2022).
- Murray, C.J.; Ikuta, K.S.; Sharara, F.; Swetschinski, L.; Aguilar, G.R.; Gray, A.; Han, C.; Bisignano, C.; Rao, P.; Wool, E.; et al. Global Burden of Bacterial Antimicrobial Resistance in 2019: A Systematic Analysis. Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef]
- Aslam, B.; Khurshid, M.; Arshad, M.I.; Muzammil, S.; Rasool, M.; Yasmeen, N.; Shah, T.; Chaudhry, T.H.; Rasool, M.H.; Shahid, A.; et al. Antibiotic Resistance: One Health One World Outlook. Front. Cell. Infect. Microbiol. 2021, 11, 771510. [Google Scholar] [CrossRef] [PubMed]
- Sécher, T.; Mayor, A.; Heuzé-Vourc’h, N. Inhalation of Immuno-Therapeutics/-Prophylactics to Fight Respiratory Tract Infections: An Appropriate Drug at the Right Place! Front. Immunol. 2019, 10, 2760. [Google Scholar] [CrossRef] [PubMed]
- Tomczyk, S.; McCracken, J.P.; Contreras, C.L.; Lopez, M.R.; Bernart, C.; Moir, J.C.; Escobar, K.; Reyes, L.; Arvelo, W.; Lindblade, K.; et al. Factors Associated with Fatal Cases of Acute Respiratory Infection (ARI) among Hospitalized Patients in Guatemala. BMC Public Health 2019, 19, 499. [Google Scholar] [CrossRef]
- Schroeck, J.L.; Ruh, C.A.; Sellick, J.A.; Ott, M.C.; Mattappallil, A.; Mergenhagen, K.A. Factors Associated with Antibiotic Misuse in Outpatient Treatment for Upper Respiratory Tract Infections. Antimicrob. Agents Chemother. 2015, 59, 3848–3852. [Google Scholar] [CrossRef][Green Version]
- Iftikhar, S.; Sarwar, M.R.; Saqib, A.; Sarfraz, M.; Shoaib, Q. Antibiotic Prescribing Practices and Errors among Hospitalized Pediatric Patients Suffering from Acute Respiratory Tract Infections: A Multicenter, Cross-Sectional Study in Pakistan. Medicina 2019, 55, 44. [Google Scholar] [CrossRef]
- Machowska, A.; Stålsby Lundborg, C. Drivers of Irrational Use of Antibiotics in Europe. Int. J. Environ. Res. Public Health 2019, 16, 27. [Google Scholar] [CrossRef] [PubMed]
- Chokshi, A.; Sifri, Z.; Cennimo, D.; Horng, H. Global Contributors to Antibiotic Resistance. J. Glob. Infect. Dis. 2019, 11, 36. [Google Scholar] [CrossRef]
- Wall, S. Prevention of Antibiotic Resistance—An Epidemiological Scoping Review to Identify Research Categories and Knowledge Gaps. Glob. Health Action 2019, 12, 1756191. [Google Scholar] [CrossRef] [PubMed]
- Frieri, M.; Kumar, K.; Boutin, A. Antibiotic Resistance. J. Infect. Public Health 2017, 10, 369–378. [Google Scholar] [CrossRef]
- Sánchez, X.; Orrico, M.; Morillo, T.; Manzano, A.; Jimbo, R.; Armijos, L. Reducing Unnecessary Antibiotic Prescription through Implementation of a Clinical Guideline on Self-Limiting Respiratory Tract Infections. PLoS ONE 2021, 16, e0249475. [Google Scholar] [CrossRef]
- McDonagh, M.S.; Peterson, K.; Winthrop, K.; Cantor, A.; Lazur, B.H.; Buckley, D.I. Interventions to Reduce Inappropriate Prescribing of Antibiotics for Acute Respiratory Tract Infections: Summary and Update of a Systematic Review. J. Int. Med. Res. 2018, 46, 3337–3357. [Google Scholar] [CrossRef]
- Mortazhejri, S.; Hong, P.J.; Yu, A.M.; Hong, B.Y.; Stacey, D.; Bhatia, R.S.; Grimshaw, J.M. Systematic Review of Patient-Oriented Interventions to Reduce Unnecessary Use of Antibiotics for Upper Respiratory Tract Infections. Syst. Rev. 2020, 9, 106. [Google Scholar] [CrossRef] [PubMed]
- Roque, F.; Herdeiro, M.T.; Soares, S.; Teixeira Rodrigues, A.; Breitenfeld, L.; Figueiras, A. Educational Interventions to Improve Prescription and Dispensing of Antibiotics: A Systematic Review. BMC Public Health 2014, 14, 1276. [Google Scholar] [CrossRef]
- Roque, F.; Teixeira-Rodrigues, A.; Breitenfeld, L.; Piñeiro-Lamas, M.; Figueiras, A.; Herdeiro, M.T. Decreasing Antibiotic Use through a Joint Intervention Targeting Physicians and Pharmacists. Future Microbiol. 2016, 11, 877–886. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, A.T.; Roque, F.; Piñeiro-Lamas, M.; Falcão, A.; Figueiras, A.; Herdeiro, M.T. Effectiveness of an Intervention to Improve Antibiotic-Prescribing Behaviour in Primary Care: A Controlled, Interrupted Time-Series Study. J. Antimicrob. Chemother. 2019, 74, 2788–2796. [Google Scholar] [CrossRef] [PubMed]
- Nalule, Y. Is Physician Education Effective in Promoting Antibiotic Stewardship? Cent. Dis. Dyn. Econ. Policy. 2011. Available online: https://cddep.org/publications/physician_education_effective_promoting_antibiotic_stewardship/ (accessed on 21 June 2022).
- Bremmer, D.N.; Trienski, T.L.; Walsh, T.L.; Moffa, M.A. Role of Technology in Antimicrobial Stewardship. Med. Clin. N. Am. 2018, 102, 955–963. [Google Scholar] [CrossRef] [PubMed]
- Estrela, M.; Roque, F.; Silva, T.M.; Zapata-Cachafeiro, M.; Figueiras, A.; Herdeiro, M.T. Validation of the EHealthResp Online Course for Pharmacists and Physicians: A Delphi Method Approach. Biomed. Pharmacother. Biomed. Pharmacother. 2021, 140, 111739. [Google Scholar] [CrossRef] [PubMed]
- Moura, J.; Almeida, A.M.P.; Roque, F.; Figueiras, A.; Herdeiro, M.T. A Mobile App to Support Clinical Diagnosis of Upper Respiratory Problems (EHealthResp): Co-Design Approach. J. Med. Internet Res. 2021, 23, e19194. [Google Scholar] [CrossRef] [PubMed]
- Estrela, M.; Magalhães Silva, T.; Pisco Almeida, A.M.; Regueira, C.; Zapata-Cachafeiro, M.; Figueiras, A.; Roque, F.; Herdeiro, M.T. A Roadmap for the Development and Evaluation of the EHealthResp Online Course. Digit. Health 2022, 8, 20552076221089090. [Google Scholar] [CrossRef]
- Moura, J.; Estrela, M.; Almeida, A.M.; Ferraz, I.; Figueiras, A.; Roque, F.; Herdeiro, M.T. A Usability Study of Pharmacists’ Perceptions Toward an Online Course for Respiratory Infections and Antibiotic Use. Procedia Comput. Sci. 2021, 181, 269–276. [Google Scholar] [CrossRef]
- Gordon, W.J.; Landman, A.; Zhang, H.; Bates, D.W. Beyond Validation: Getting Health Apps into Clinical Practice. npj Digit. Med. 2020, 3, 14. [Google Scholar] [CrossRef] [PubMed]
- Powell, A.C.; Landman, A.B.; Bates, D.W. In Search of a Few Good Apps. JAMA 2014, 311, 1851. [Google Scholar] [CrossRef] [PubMed]
- Rawson, T.M.; Moore, L.S.P.; Hernandez, B.; Charani, E.; Castro-Sanchez, E.; Herrero, P.; Hayhoe, B.; Hope, W.; Georgiou, P.; Holmes, A.H. A Systematic Review of Clinical Decision Support Systems for Antimicrobial Management: Are We Failing to Investigate These Interventions Appropriately? Clin. Microbiol. Infect. 2017, 23, 524–532. [Google Scholar] [CrossRef] [PubMed]
- Holstiege, J.; Mathes, T.; Pieper, D. Effects of Computer-Aided Clinical Decision Support Systems in Improving Antibiotic Prescribing by Primary Care Providers: A Systematic Review. J. Am. Med. Inform. Assoc. 2015, 22, 236–242. [Google Scholar] [CrossRef] [PubMed]
- Poss-Doering, R.; Kuehn, L.; Kamradt, M.; Glassen, K.; Wensing, M. Applying Digital Information Delivery to Convert Habits of Antibiotic Use in Primary Care in Germany: Mixed-Methods Study. J. Med. Internet Res. 2020, 22, e18200. [Google Scholar] [CrossRef]
- Linder, J.; Schnipper, J.L.; Volk, L.A.; Tsurikova, R.; Palchuk, M.; Olsha-Yehiav, M.; Melnikas, A.J.; Middleton, B. Clinical Decision Support to Improve Antibiotic Prescribing for Acute Respiratory Infections: Results of a Pilot Study. In Proceedings of the AMIA Annual Symposium Proceedings, Chicago, IL, USA, 10–14 November 2007; Volume 2007, pp. 468–472. [Google Scholar]
- Alshengeti, A.; Slayter, K.; Black, E.; Top, K. On-Line Virtual Patient Learning: A Pilot Study of a New Modality in Antimicrobial Stewardship Education for Pediatric Residents. BMC Res. Notes 2020, 13, 339. [Google Scholar] [CrossRef]
- Bochicchio, G.V.; Smit, P.A.; Moore, R.; Bochicchio, K.; Auwaerter, P.; Johnson, S.B.; Scalea, T.; Bartlett, J.G. Pilot Study of a Web-Based Antibiotic Decision Management Guide. J. Am. Coll. Surg. 2006, 202, 459–467. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, É.; Estrela, M.; Zapata-Cachafeiro, M.; Figueiras, A.; Roque, F.; Herdeiro, M.T. E-Health Tools to Improve Antibiotic Use and Resistances: A Systematic Review. Antibiotics 2020, 9, 505. [Google Scholar] [CrossRef] [PubMed]
- Moore, C.G.; Carter, R.E.; Nietert, P.J.; Stewart, P.W. Recommendations for Planning Pilot Studies in Clinical and Translational Research. Clin. Transl. Sci. 2011, 4, 332–337. [Google Scholar] [CrossRef] [PubMed]
- Cocks, K.; Torgerson, D.J. Sample Size Calculations for Pilot Randomized Trials: A Confidence Interval Approach. J. Clin. Epidemiol. 2013, 66, 197–201. [Google Scholar] [CrossRef] [PubMed]
- Hertzog, M.A. Considerations in Determining Sample Size for Pilot Studies. Res. Nurs. Health 2008, 31, 180–191. [Google Scholar] [CrossRef] [PubMed]
- Johanson, G.A.; Brooks, G.P. Initial Scale Development: Sample Size for Pilot Studies. Educ. Psychol. Meas. 2010, 70, 394–400. [Google Scholar] [CrossRef]
- Julious, S.A. Sample Size of 12 per Group Rule of Thumb for a Pilot Study. Pharm. Stat. 2005, 4, 287–291. [Google Scholar] [CrossRef]


{kind=link}
| Online Course | Parameters | Median (PCT25, PCT75) |
| Format | 5.00 (4.00, 5.00) | |
| Utility | 4.00 (4.00, 5.00) | |
| Interest | 4.00 (4.00, 5.00) | |
| Trust | 5.00 (4.00, 5.00) | |
| Modules | Parameters | Median (PCT25, PCT75) |
| Adequacy | 4.50 (4.00, 5.00) | |
| Module 0 | Correction | 5.00 (4.00, 5.00) |
| Completeness | 4.00 (3.75, 5.00) | |
| Adequacy | 5.00 (4.00, 5.00) | |
| Module 1 | Correction | 5.00 (5.00, 5.00) |
| Completeness | 4.00 (4.00, 5.00) | |
| Adequacy | 5.00 (4.00, 5.00) | |
| Module 2 | Correction | 5.00 (4.75, 5.00) |
| Completeness | 5.00 (4.00, 5.00) | |
| Adequacy | 5.00 (4.75, 5.00) | |
| Module 3 | Correction | 5.00 (4.75, 5.00) |
| Completeness | 5.00 (4.00, 5.00) | |
| Adequacy | 5.00 (4.00, 5.00) | |
| Module 4 | Correction | 5.00 (5.00, 5.00) |
| Completeness | 5.00 (4.00, 5.00) | |
| Adequacy | 5.00 (4.75, 5.00) | |
| Module 5 | Correction | 5.00 (4.75, 5.00) |
| Completeness | 4.50 (4.00, 5.00) | |
| Adequacy | 5.00 (4.00, 5.00) | |
| Module 6 | Correction | 4.50 (4.00, 5.00) |
| Completeness | 4.00 (3.00, 5.00) | |
| Clinical Cases | Parameters | Median (PCT25, PCT75) |
| Adequacy | 4.50 (4.00, 5.00) | |
| Clinical Case 1 | Correction | 5.00 (4.75, 5.00) |
| Completeness | 4.00 (4.00, 5.00) | |
| Adequacy | 4.50 (4.00, 5.00) | |
| Clinical Case 2 | Correction | 5.00 (4.00, 5.00) |
| Completeness | 4.00 (4.00, 5.00) | |
| Adequacy | 5.00 (5.00, 5.00) | |
| Clinical Case 3 | Correction | 5.00 (5.00, 5.00) |
| Completeness | 5.00 (4.00, 5.00) | |
| Adequacy | 5.00 (4.00, 5.00) | |
| Clinical Case 4 | Correction | 5.00 (4.75, 5.00) |
| Completeness | 5.00 (4.00, 5.00) |
| Mobile App | Parameters | Median (PCT25, PCT75) |
|---|---|---|
| Adequacy | 5.00 (4.00, 5.00) | |
| Correction | 5.00 (4.75, 5.00) | |
| Completeness | 4.00 (3.75, 5.00) | |
| Format | 5.00 (5.00, 5.00) | |
| Utility | 4.00 (4.00, 5.00) | |
| Interest | 4.00 (3.75, 4.25) | |
| Trust | 5.00 (4.00, 5.00) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Silva, T.M.; Estrela, M.; Magalhães, S.; Simões, C.; Cachim, A.; Costa, T.; Crexinski, G.; Almeida, M.P.; Figueiras, A.; Roque, F.; et al. eHealthResp, a Digital Intervention to Improve Antibiotic Prescribing in Respiratory Infections: A Pilot Study. Life 2022, 12, 1160. https://doi.org/10.3390/life12081160
Silva TM, Estrela M, Magalhães S, Simões C, Cachim A, Costa T, Crexinski G, Almeida MP, Figueiras A, Roque F, et al. eHealthResp, a Digital Intervention to Improve Antibiotic Prescribing in Respiratory Infections: A Pilot Study. Life. 2022; 12(8):1160. https://doi.org/10.3390/life12081160
Chicago/Turabian StyleSilva, Tânia Magalhães, Marta Estrela, Sandra Magalhães, Catarina Simões, Afonso Cachim, Tainá Costa, Gabriella Crexinski, Margarida Pisco Almeida, Adolfo Figueiras, Fátima Roque, and et al. 2022. "eHealthResp, a Digital Intervention to Improve Antibiotic Prescribing in Respiratory Infections: A Pilot Study" Life 12, no. 8: 1160. https://doi.org/10.3390/life12081160
APA StyleSilva, T. M., Estrela, M., Magalhães, S., Simões, C., Cachim, A., Costa, T., Crexinski, G., Almeida, M. P., Figueiras, A., Roque, F., & Herdeiro, M. T. (2022). eHealthResp, a Digital Intervention to Improve Antibiotic Prescribing in Respiratory Infections: A Pilot Study. Life, 12(8), 1160. https://doi.org/10.3390/life12081160