
A Reproducible Deep-Learning-Based Computer-Aided Diagnosis Tool for Frontotemporal Dementia Using MONAI and Clinica Frameworks

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Neuroimaging in Frontotemporal Dementia Database
2.2. Clinica: An Open-Source Software Platform for Reproducible Clinical Neuroscience Studies
2.3. MONAI: Medical Open Network for Artificial Intelligence
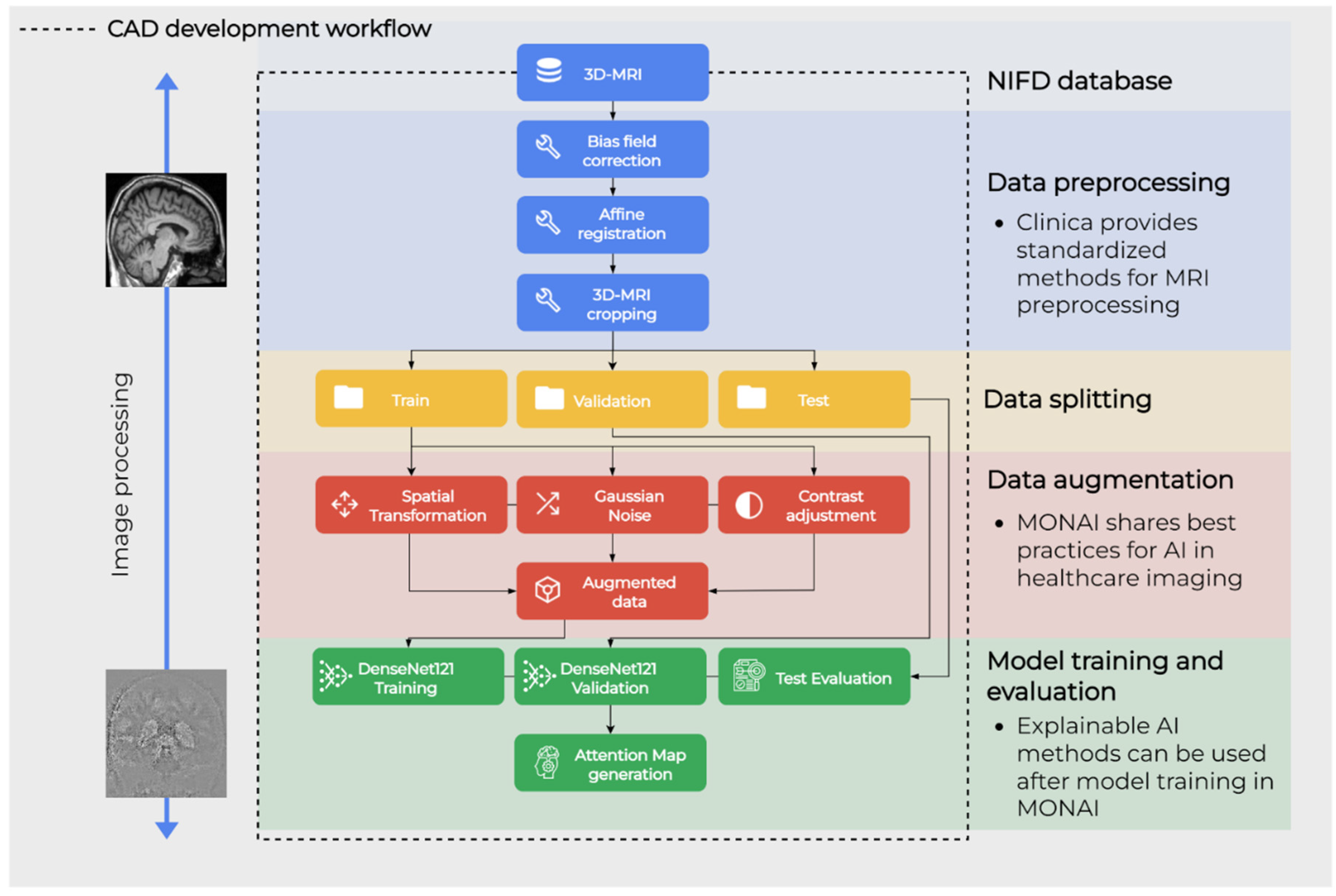
2.4. Workflow Overview
2.5. Data Collection
2.6. Preprocessing Pipeline
2.7. Data Augmentation Pipeline
2.8. Deep Learning Pipeline
2.9. Explainable AI Using the Attention Map Method
3. Results
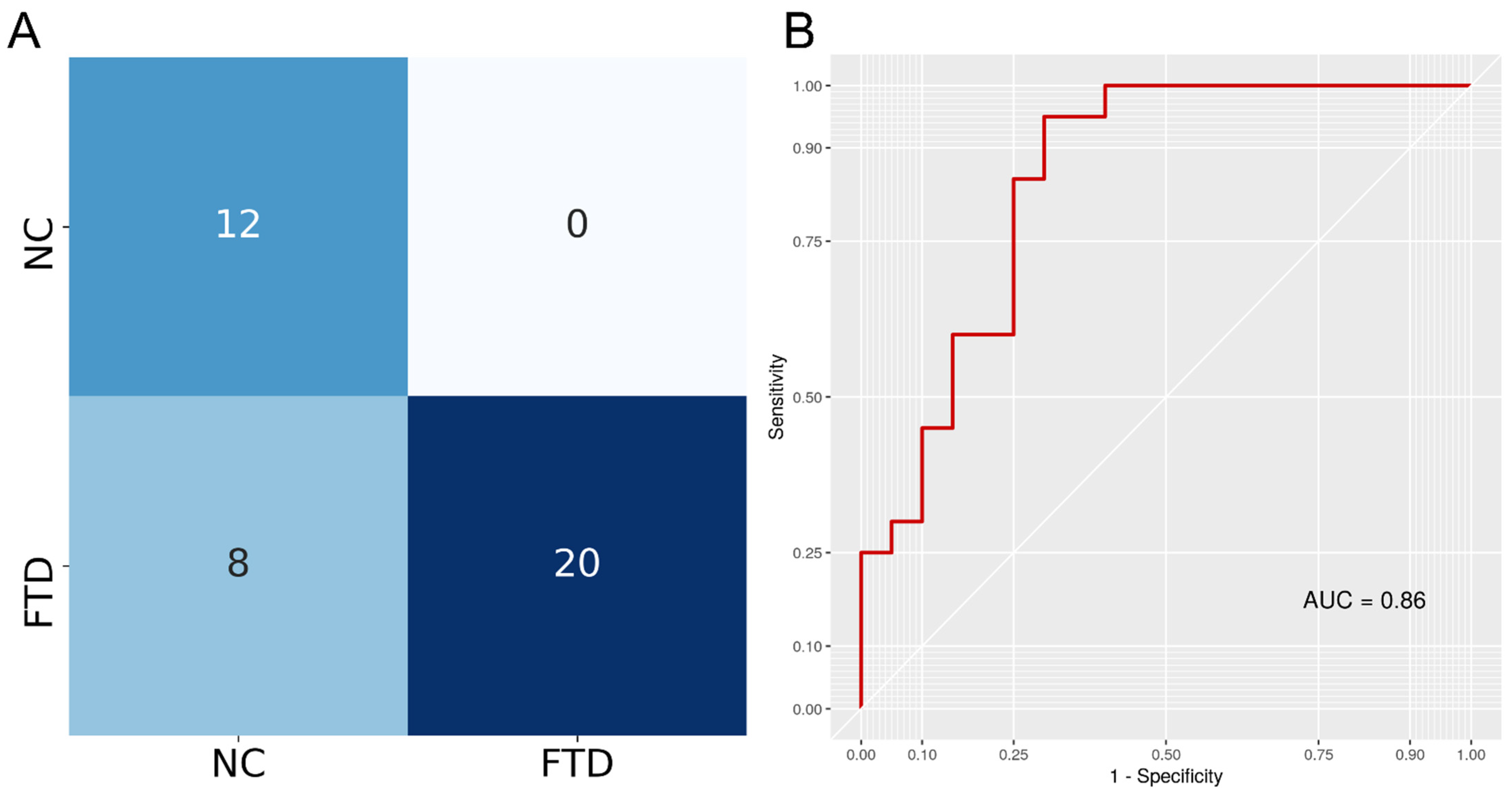
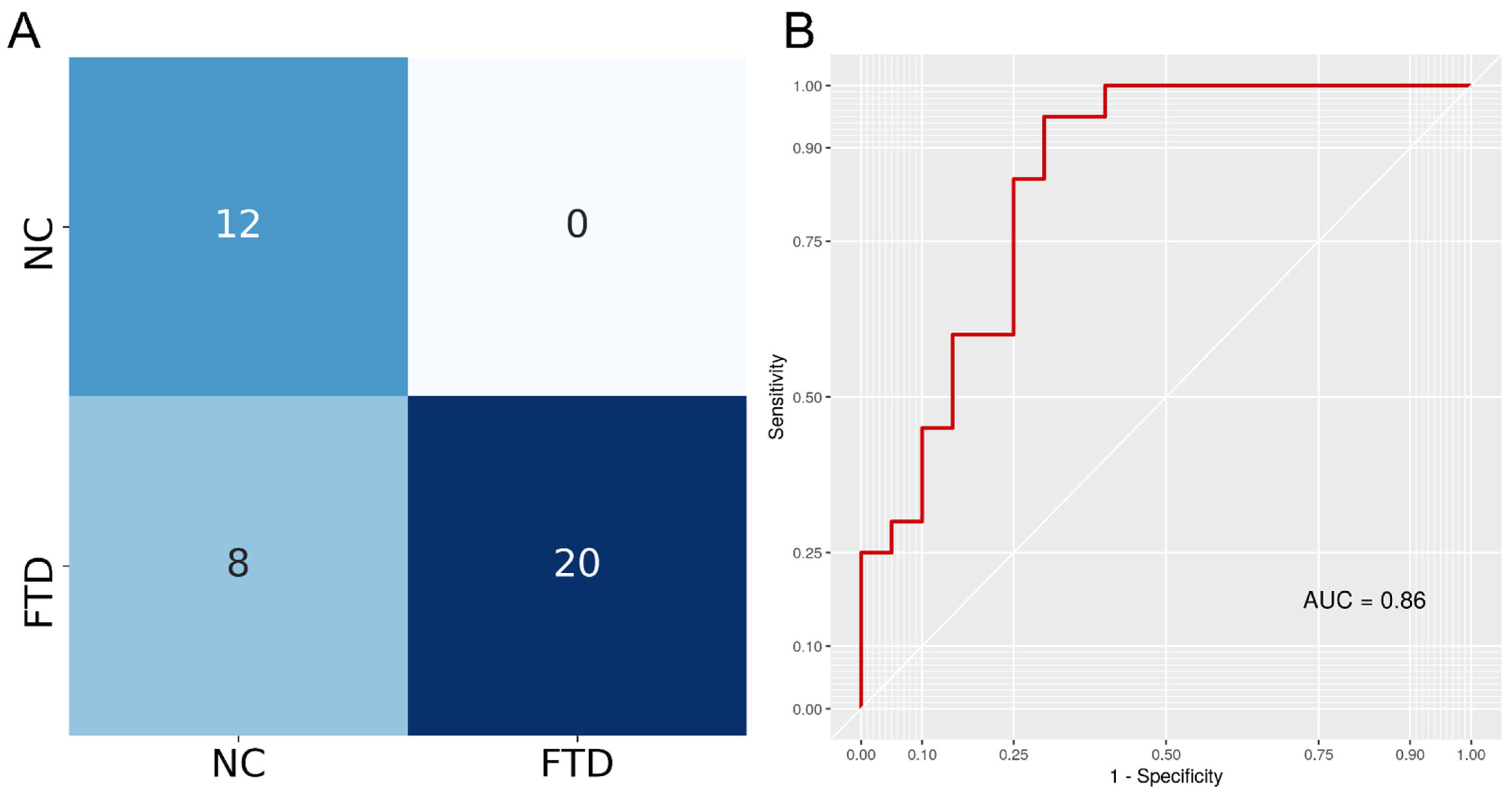
3.1. CAD Train and Test
3.2. Comparison with Previous FTD Classification Approaches
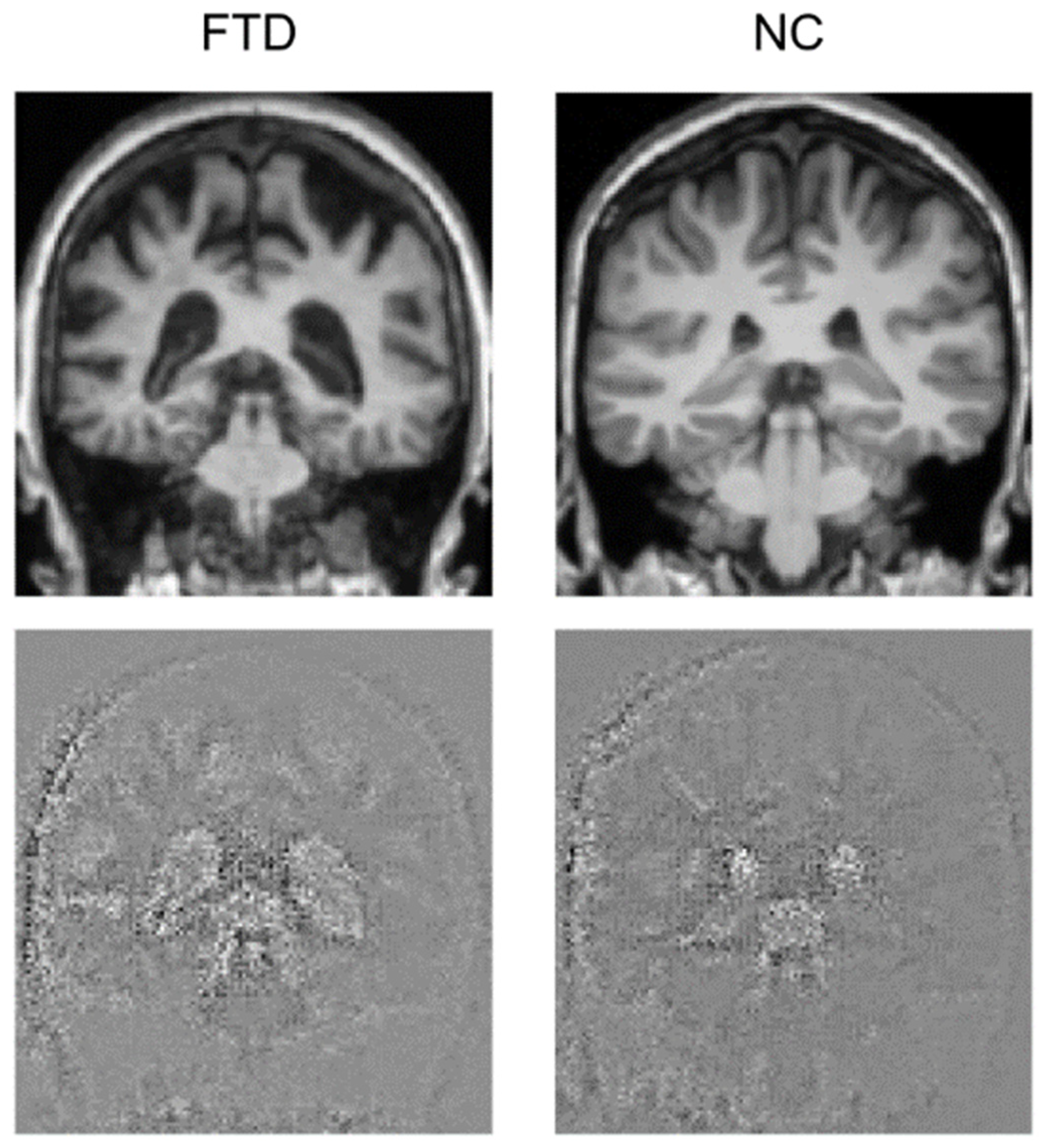
3.3. Attention Maps
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Halalli, B.; Makandar, A. Computer Aided Diagnosis-Medical Image Analysis Techniques. In Breast Imaging; 2018; Volume 85, Available online: https://www.intechopen.com/chapters/56615 (accessed on 20 May 2022).
- Choi, J.-H.; Kang, B.J.; Baek, J.E.; Lee, H.S.; Kim, S.H. Application of Computer-Aided Diagnosis in Breast Ultrasound Interpretation: Improvements in Diagnostic Performance According to Reader Experience. Ultrasonography 2018, 37, 217–225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, H.-P.; Hadjiiski, L.M.; Samala, R.K. Computer-aided Diagnosis in the Era of Deep Learning. Med. Phys. 2020, 47, e218–e227. [Google Scholar] [CrossRef] [PubMed]
- Tacchella, A.; Romano, S.; Ferraldeschi, M.; Salvetti, M.; Zaccaria, A.; Crisanti, A.; Grassi, F. Collaboration between a Human Group and Artificial Intelligence Can Improve Prediction of Multiple Sclerosis Course: A Proof-of-Principle Study. F1000Research 2017, 6, 2172. [Google Scholar] [CrossRef] [PubMed]
- Jumper, J.; Evans, R.; Pritzel, A.; Green, T.; Figurnov, M.; Ronneberger, O.; Tunyasuvunakool, K.; Bates, R.; Žídek, A.; Potapenko, A.; et al. Highly Accurate Protein Structure Prediction with AlphaFold. Nature 2021, 596, 583–589. [Google Scholar] [CrossRef]
- Ramesh, A.; Dhariwal, P.; Nichol, A.; Chu, C.; Chen, M. Hierarchical Text-Conditional Image Generation with CLIP Latents. arXiv 2022, arXiv:2204.06125. [Google Scholar]
- Vinyals, O.; Babuschkin, I.; Czarnecki, W.M.; Mathieu, M.; Dudzik, A.; Chung, J.; Choi, D.H.; Powell, R.; Ewalds, T.; Georgiev, P.; et al. Grandmaster Level in StarCraft II Using Multi-Agent Reinforcement Learning. Nature 2019, 575, 350–354. [Google Scholar] [CrossRef]
- Fabrizio, C.; Termine, A.; Caltagirone, C.; Sancesario, G. Artificial Intelligence for Alzheimer’s Disease: Promise or Challenge? Diagnostics 2021, 11, 1473. [Google Scholar] [CrossRef]
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep Learning. Nature 2015, 521, 436–444. [Google Scholar] [CrossRef]
- Healthcare Industry Trends 2022: Accessible Data, Pharma AI. Available online: https://cloud.google.com/blog/topics/healthcare-life-sciences/healthcare-industry-trends-2022-life-sciences-technology-predictions-data-ai-interoperability/ (accessed on 13 June 2022).
- Davenport, T.; Kalakota, R. The Potential for Artificial Intelligence in Healthcare. Future Healthc. J. 2019, 6, 94–98. [Google Scholar] [CrossRef] [Green Version]
- Gunning, D.; Stefik, M.; Choi, J.; Miller, T.; Stumpf, S.; Yang, G.-Z. XAI—Explainable Artificial Intelligence. Sci. Robot. 2019, 4, eaay7120. [Google Scholar] [CrossRef] [Green Version]
- Bang, J.; Spina, S.; Miller, B.L. Frontotemporal Dementia. Lancet 2015, 386, 1672–1682. [Google Scholar] [CrossRef] [Green Version]
- Vieira, R.T.; Caixeta, L.; Machado, S.; Silva, A.C.; Nardi, A.E.; Arias-Carrión, O.; Carta, M.G. Epidemiology of Early-Onset Dementia: A Review of the Literature. Clin. Pract. Epidemiol. Ment. Health 2013, 9, 88–95. [Google Scholar] [CrossRef]
- Brun, A.; Liu, X.; Erikson, C. Synapse Loss and Gliosis in the Molecular Layer of the Cerebral Cortex in Alzheimer’s Disease and in Frontal Lobe Degeneration. Neurodegeneration 1995, 4, 171–177. [Google Scholar] [CrossRef] [PubMed]
- Dugger, B.N.; Dickson, D.W. Pathology of Neurodegenerative Diseases. Cold Spring Harb. Perspect. Biol. 2017, 9, a028035. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mackenzie, I.R.; Neumann, M. Molecular Neuropathology of Frontotemporal Dementia: Insights into Disease Mechanisms from Postmortem Studies. J. Neurochem. 2016, 138, 54–70. [Google Scholar] [CrossRef]
- Pijnenburg, Y.A.L.; Gillissen, F.; Jonker, C.; Scheltens, P. Initial Complaints in Frontotemporal Lobar Degeneration. Dement. Geriatr. Cogn. Disord. 2004, 17, 302–306. [Google Scholar] [CrossRef]
- Rosness, T.A.; Haugen, P.K.; Passant, U.; Engedal, K. Frontotemporal Dementia: A Clinically Complex Diagnosis. Int. J. Geriatr. Psychiatry 2008, 23, 837–842. [Google Scholar] [CrossRef]
- Gorno-Tempini, M.L.; Hillis, A.E.; Weintraub, S.; Kertesz, A.; Mendez, M.; Cappa, S.F.; Ogar, J.M.; Rohrer, J.D.; Black, S.; Boeve, B.F.; et al. Classification of Primary Progressive Aphasia and Its Variants. Neurology 2011, 76, 1006–1014. [Google Scholar] [CrossRef] [Green Version]
- Höglinger, G.U.; Respondek, G.; Stamelou, M.; Kurz, C.; Josephs, K.A.; Lang, A.E.; Mollenhauer, B.; Müller, U.; Nilsson, C.; Whitwell, J.L.; et al. Clinical Diagnosis of Progressive Supranuclear Palsy: The Movement Disorder Society Criteria. Mov. Disord. 2017, 32, 853–864. [Google Scholar] [CrossRef]
- Rascovsky, K.; Hodges, J.R.; Knopman, D.; Mendez, M.F.; Kramer, J.H.; Neuhaus, J.; van Swieten, J.C.; Seelaar, H.; Dopper, E.G.P.; Onyike, C.U.; et al. Sensitivity of Revised Diagnostic Criteria for the Behavioural Variant of Frontotemporal Dementia. Brain J. Neurol. 2011, 134, 2456–2477. [Google Scholar] [CrossRef]
- Benussi, A.; Di Lorenzo, F.; Dell’Era, V.; Cosseddu, M.; Alberici, A.; Caratozzolo, S.; Cotelli, M.S.; Micheli, A.; Rozzini, L.; Depari, A. Transcranial Magnetic Stimulation Distinguishes Alzheimer Disease from Frontotemporal Dementia. Neurology 2017, 89, 665–672. [Google Scholar] [CrossRef] [PubMed]
- Perri, R.; Koch, G.; Carlesimo, G.A.; Serra, L.; Fadda, L.; Pasqualetti, P.; Pettenati, C.; Caltagirone, C. Alzheimer’s Disease and Frontal Variant of Frontotemporal Dementia. J. Neurol. 2005, 252, 1238–1244. [Google Scholar] [CrossRef] [PubMed]
- Di Lorenzo, F.; Motta, C.; Caltagirone, C.; Koch, G.; Mercuri, N.B.; Martorana, A. Lacosamide in the Management of Behavioral Symptoms in Frontotemporal Dementia: A 2-Case Report. Alzheimer Dis. Assoc. Disord. 2018, 32, 364–365. [Google Scholar] [CrossRef] [PubMed]
- Mourik, J.C.; Rosso, S.M.; Niermeijer, M.F.; Duivenvoorden, H.J.; Van Swieten, J.C.; Tibben, A. Frontotemporal Dementia: Behavioral Symptoms and Caregiver Distress. Dement. Geriatr. Cogn. Disord. 2004, 18, 299–306. [Google Scholar] [CrossRef]
- Benussi, A.; Dell’Era, V.; Cosseddu, M.; Cantoni, V.; Cotelli, M.S.; Cotelli, M.; Manenti, R.; Benussi, L.; Brattini, C.; Alberici, A.; et al. Transcranial Stimulation in Frontotemporal Dementia: A Randomized, Double-Blind, Sham-Controlled Trial. Alzheimer’s Dement. 2020, 6. [Google Scholar] [CrossRef]
- Bonnì, S.; Koch, G.; Miniussi, C.; Bassi, M.S.; Caltagirone, C.; Gainotti, G. Role of the Anterior Temporal Lobes in Semantic Representations: Paradoxical Results of a CTBS Study. Neuropsychologia 2015, 76, 163–169. [Google Scholar] [CrossRef] [Green Version]
- Gerfo, E.L.; Oliveri, M.; Torriero, S.; Salerno, S.; Koch, G.; Caltagirone, C. The Influence of RTMS over Prefrontal and Motor Areas in a Morphological Task: Grammatical vs. Semantic Effects. Neuropsychologia 2008, 46, 764–770. [Google Scholar] [CrossRef]
- Jiskoot, L.C.; Panman, J.L.; Meeter, L.H.; Dopper, E.G.; Donker Kaat, L.; Franzen, S.; van der Ende, E.L.; van Minkelen, R.; Rombouts, S.A.; Papma, J.M. Longitudinal Multimodal MRI as Prognostic and Diagnostic Biomarker in Presymptomatic Familial Frontotemporal Dementia. Brain 2019, 142, 193–208. [Google Scholar] [CrossRef] [Green Version]
- Seeley, W.W.; Crawford, R.; Rascovsky, K.; Kramer, J.H.; Weiner, M.; Miller, B.L.; Gorno-Tempini, M.L. Frontal Paralimbic Network Atrophy in Very Mild Behavioral Variant Frontotemporal Dementia. Arch. Neurol. 2008, 65, 249–255. [Google Scholar] [CrossRef] [Green Version]
- Frings, L.; Yew, B.; Flanagan, E.; Lam, B.Y.; Hüll, M.; Huppertz, H.-J.; Hodges, J.R.; Hornberger, M. Longitudinal Grey and White Matter Changes in Frontotemporal Dementia and Alzheimer’s Disease. PLoS ONE 2014, 9, e90814. [Google Scholar]
- Whitwell, J.L.; Boeve, B.F.; Weigand, S.D.; Senjem, M.L.; Gunter, J.L.; Baker, M.C.; DeJesus-Hernandez, M.; Knopman, D.S.; Wszolek, Z.K.; Petersen, R.C. Brain Atrophy over Time in Genetic and Sporadic Frontotemporal Dementia: A Study of 198 Serial Magnetic Resonance Images. Eur. J. Neurol. 2015, 22, 745–752. [Google Scholar] [CrossRef] [PubMed]
- Knopman, D.S.; Jack, C.R.; Kramer, J.H.; Boeve, B.F.; Caselli, R.J.; Graff-Radford, N.R.; Mendez, M.F.; Miller, B.L.; Mercaldo, N.D. Brain and Ventricular Volumetric Changes in Frontotemporal Lobar Degeneration over 1 Year. Neurology 2009, 72, 1843–1849. [Google Scholar] [CrossRef] [PubMed]
- Manera, A.L.; Dadar, M.; Collins, D.L.; Ducharme, S.; Frontotemporal Lobar Degeneration Neuroimaging Initiative; Alzheimer’s Disease Neuroimaging Initiative. Ventricular Features as Reliable Differentiators between BvFTD and Other Dementias. NeuroImage Clin. 2022, 33, 102947. [Google Scholar] [CrossRef] [PubMed]
- Davatzikos, C.; Resnick, S.M.; Wu, X.; Parmpi, P.; Clark, C.M. Individual Patient Diagnosis of AD and FTD via High-Dimensional Pattern Classification of MRI. NeuroImage 2008, 41, 1220–1227. [Google Scholar] [CrossRef] [Green Version]
- Du, A.-T.; Schuff, N.; Kramer, J.H.; Rosen, H.J.; Gorno-Tempini, M.L.; Rankin, K.; Miller, B.L.; Weiner, M.W. Different Regional Patterns of Cortical Thinning in Alzheimer’s Disease and Frontotemporal Dementia. Brain 2007, 130, 1159–1166. [Google Scholar] [CrossRef]
- Spasov, S.; Passamonti, L.; Duggento, A.; Lio, P.; Toschi, N.; Alzheimer’s Disease Neuroimaging Initiative. A Parameter-Efficient Deep Learning Approach to Predict Conversion from Mild Cognitive Impairment to Alzheimer’s Disease. NeuroImage 2019, 189, 276–287. [Google Scholar] [CrossRef] [Green Version]
- Termine, A.; Fabrizio, C.; Strafella, C.; Caputo, V.; Petrosini, L.; Caltagirone, C.; Giardina, E.; Cascella, R. Multi-Layer Picture of Neurodegenerative Diseases: Lessons from the Use of Big Data through Artificial Intelligence. J. Pers. Med. 2021, 11, 280. [Google Scholar] [CrossRef]
- Crüwell, S.; van Doorn, J.; Etz, A.; Makel, M.C.; Moshontz, H.; Niebaum, J.C.; Orben, A.; Parsons, S.; Schulte-Mecklenbeck, M. Seven Easy Steps to Open Science. Zeitschrift Psychologie 2019, 227, 237–248. [Google Scholar] [CrossRef]
- Wilkinson, M.D.; Dumontier, M.; Aalbersberg, J.I.; Appleton, G.; Axton, M.; Baak, A.; Blomberg, N.; Boiten, J.-W.; da Silva Santos, L.B.; Bourne, P.E. The FAIR Guiding Principles for Scientific Data Management and Stewardship. Sci. Data 2016, 3, 160018. [Google Scholar] [CrossRef] [Green Version]
- Hu, J.; Qing, Z.; Liu, R.; Zhang, X.; Lv, P.; Wang, M.; Wang, Y.; He, K.; Gao, Y.; Zhang, B. Deep Learning-Based Classification and Voxel-Based Visualization of Frontotemporal Dementia and Alzheimer’s Disease. Front. Neurosci. 2020, 14, 626154. [Google Scholar] [CrossRef]
- Bron, E.E.; Smits, M.; Papma, J.M.; Steketee, R.M.E.; Meijboom, R.; de Groot, M.; van Swieten, J.C.; Niessen, W.J.; Klein, S. Multiparametric Computer-Aided Differential Diagnosis of Alzheimer’s Disease and Frontotemporal Dementia Using Structural and Advanced MRI. Eur. Radiol. 2017, 27, 3372–3382. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Tartaglia, M.C.; Schuff, N.; Chiang, G.C.; Ching, C.; Rosen, H.J.; Gorno-Tempini, M.L.; Miller, B.L.; Weiner, M.W. MRI Signatures of Brain Macrostructural Atrophy and Microstructural Degradation in Frontotemporal Lobar Degeneration Subtypes. J. Alzheimer’s Dis. 2013, 33, 431–444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muñoz-Ruiz, M.Á.; Hartikainen, P.; Koikkalainen, J.; Wolz, R.; Julkunen, V.; Niskanen, E.; Herukka, S.-K.; Kivipelto, M.; Vanninen, R.; Rueckert, D.; et al. Structural MRI in Frontotemporal Dementia: Comparisons between Hippocampal Volumetry, Tensor-Based Morphometry and Voxel-Based Morphometry. PLoS ONE 2012, 7, e52531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dukart, J.; Mueller, K.; Horstmann, A.; Barthel, H.; Möller, H.E.; Villringer, A.; Sabri, O.; Schroeter, M.L. Combined Evaluation of FDG-PET and MRI Improves Detection and Differentiation of Dementia. PLoS ONE 2011, 6, e18111. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, J.; Collins, D.L.; Ducharme, S. Morphometric MRI as a Diagnostic Biomarker of Frontotemporal Dementia: A Systematic Review to Determine Clinical Applicability. NeuroImage Clin. 2018, 20, 685–696. [Google Scholar] [CrossRef] [PubMed]
- Gorgolewski, K.; Burns, C.D.; Madison, C.; Clark, D.; Halchenko, Y.O.; Waskom, M.L.; Ghosh, S.S. Nipype: A Flexible, Lightweight and Extensible Neuroimaging Data Processing Framework in Python. Front. Neuroinform. 2011, 5, 13. [Google Scholar] [CrossRef] [Green Version]
- Subramanian, A.; Lan, H.; Govindarajan, S.; Viswanathan, L.; Choupan, J.; Sepehrband, F. NiftyTorch: A Deep Learning Framework for NeuroImaging. bioRxiv 2021. [Google Scholar] [CrossRef]
- Perone, C.S.; Cclauss; Saravia, E.; Ballester, P.L. MohitTare Perone/Medicaltorch: Release v0.2; Zenodo, 2018. Available online: https://zenodo.org/record/1495335 (accessed on 25 May 2022).
- Gorgolewski, K.; Alfaro-Almagro, F.; Auer, T.; Bellec, P.; Capotă, M.; Chakravarty, M.M.; Churchill, N.W.; Cohen, A.L.; Craddock, R.C.; Devenyi, G.A. BIDS Apps: Improving Ease of Use, Accessibility, and Reproducibility of Neuroimaging Data Analysis Methods. PLoS Comput. Biol. 2017, 13, e1005209. [Google Scholar] [CrossRef] [Green Version]
- Routier, A.; Burgos, N.; Díaz, M.; Bacci, M.; Bottani, S.; El-Rifai, O.; Fontanella, S.; Gori, P.; Guillon, J.; Guyot, A. Clinica: An Open-Source Software Platform for Reproducible Clinical Neuroscience Studies. Front. Neuroinform. 2021, 15, 689675. [Google Scholar] [CrossRef]
- MONAI Consortium MONAI: Medical Open Network for AI; Zenodo, 2022. Available online: https://zenodo.org/record/5728262 (accessed on 25 May 2022).
- Huang, G.; Liu, Z.; van der Maaten, L.; Weinberger, K.Q. Densely Connected Convolutional Networks. arXiv 2016, arXiv:1608.06993. [Google Scholar]
- Hodnett, M.; Wiley, J.F. R Deep Learning Essentials: A Step-by-Step Guide to Building Deep Learning Models Using TensorFlow, Keras, and MXNet; Packt Publishing Ltd.: Birmingham, UK, 2018; ISBN 1-78899-780-8. [Google Scholar]
- Wen, J.; Thibeau-Sutre, E.; Diaz-Melo, M.; Samper-González, J.; Routier, A.; Bottani, S.; Dormont, D.; Durrleman, S.; Burgos, N.; Colliot, O. Convolutional Neural Networks for Classification of Alzheimer’s Disease: Overview and Reproducible Evaluation. Med. Image Anal. 2020, 63, 101694. [Google Scholar] [CrossRef] [PubMed]
- Tustison, N.J.; Avants, B.B.; Cook, P.A.; Zheng, Y.; Egan, A.; Yushkevich, P.A.; Gee, J.C. N4ITK: Improved N3 Bias Correction. IEEE Trans. Med. Imaging 2010, 29, 1310–1320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Avants, B.; Epstein, C.; Grossman, M.; Gee, J. Symmetric Diffeomorphic Image Registration with Cross-Correlation: Evaluating Automated Labeling of Elderly and Neurodegenerative Brain. Med. Image Anal. 2008, 12, 26–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Avants, B.; Tustison, N.J.; Stauffer, M.; Song, G.; Wu, B.; Gee, J.C. The Insight ToolKit Image Registration Framework. Front. Neuroinform. 2014, 8, 44. [Google Scholar] [CrossRef] [Green Version]
- Fonov, V.; Evans, A.C.; Botteron, K.; Almli, C.R.; McKinstry, R.C.; Collins, D.L. Unbiased Average Age-Appropriate Atlases for Pediatric Studies. NeuroImage 2011, 54, 313–327. [Google Scholar] [CrossRef] [Green Version]
- Fonov, V.; Evans, A.; McKinstry, R.; Almli, C.; Collins, D. Unbiased Nonlinear Average Age-Appropriate Brain Templates from Birth to Adulthood. NeuroImage 2009, 47, S102. [Google Scholar] [CrossRef]
- Gotkowski, K.; Gonzalez, C.; Bucher, A.; Mukhopadhyay, A. M3d-CAM: A PyTorch Library to Generate 3D Attention Maps for Medical Deep Learning. In Bildverarbeitung für die Medizin 2021; Palm, C., Deserno, T.M., Handels, H., Maier, A., Maier-Hein, K., Tolxdorff, T., Eds.; Informatik Aktuell; Springer: Wiesbaden, Germany, 2021; pp. 217–222. ISBN 978-3-658-33197-9. [Google Scholar]
- Selvaraju, R.R.; Cogswell, M.; Das, A.; Vedantam, R.; Parikh, D.; Batra, D. Grad-CAM: Visual Explanations from Deep Networks via Gradient-Based Localization. arXiv 2016, arXiv:1610.02391. [Google Scholar]
- Chagué, P.; Marro, B.; Fadili, S.; Houot, M.; Morin, A.; Samper-González, J.; Beunon, P.; Arrivé, L.; Dormont, D.; Dubois, B.; et al. Radiological Classification of Dementia from Anatomical MRI Assisted by Machine Learning-Derived Maps. J. Neuroradiol. 2021, 48, 412–418. [Google Scholar] [CrossRef]
- McMillan, C.T.; Avants, B.B.; Cook, P.; Ungar, L.; Trojanowski, J.Q.; Grossman, M. The Power of Neuroimaging Biomarkers for Screening Frontotemporal Dementia. Hum. Brain Mapp. 2014, 35, 4827–4840. [Google Scholar] [CrossRef] [Green Version]
- Lehmann, M.; Rohrer, J.D.; Clarkson, M.J.; Ridgway, G.R.; Scahill, R.I.; Modat, M.; Warren, J.D.; Ourselin, S.; Barnes, J.; Rossor, M.N.; et al. Reduced Cortical Thickness in the Posterior Cingulate Gyrus Is Characteristic of Both Typical and Atypical Alzheimer’s Disease. J. Alzheimer’s Dis. 2010, 20, 587–598. [Google Scholar] [CrossRef] [Green Version]
- Klöppel, S.; Stonnington, C.M.; Chu, C.; Draganski, B.; Scahill, R.I.; Rohrer, J.D.; Fox, N.C.; Jack, C.R.; Ashburner, J.; Frackowiak, R.S.J. Automatic Classification of MR Scans in Alzheimer’s Disease. Brain J. Neurol. 2008, 131, 681–689. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.P.; Kim, J.; Park, Y.H.; Park, S.B.; Lee, J.S.; Yoo, S.; Kim, E.-J.; Kim, H.J.; Na, D.L.; Brown, J.A.; et al. Machine Learning Based Hierarchical Classification of Frontotemporal Dementia and Alzheimer’s Disease. NeuroImage Clin. 2019, 23, 101811. [Google Scholar] [CrossRef] [PubMed]
- Ma, D.; Lu, D.; Popuri, K.; Wang, L.; Beg, M.F.; Alzheimer’s Disease Neuroimaging Initiative. Differential Diagnosis of Frontotemporal Dementia, Alzheimer’s Disease, and Normal Aging Using a Multi-Scale Multi-Type Feature Generative Adversarial Deep Neural Network on Structural Magnetic Resonance Images. Front. Neurosci. 2020, 14, 853. [Google Scholar] [CrossRef] [PubMed]
- Motamedi, M.; Sakharnykh, N.; Kaldewey, T. A Data-Centric Approach for Training Deep Neural Networks with Less Data. arXiv 2021, arXiv:2110.03613. [Google Scholar]
- Guidotti, R.; Monreale, A.; Ruggieri, S.; Turini, F.; Giannotti, F.; Pedreschi, D. A Survey of Methods for Explaining Black Box Models. ACM Comput. Surv. 2019, 51, 1–42. [Google Scholar] [CrossRef] [Green Version]
- El-Sappagh, S.; Alonso, J.M.; Islam, S.M.R.; Sultan, A.M.; Kwak, K.S. A Multilayer Multimodal Detection and Prediction Model Based on Explainable Artificial Intelligence for Alzheimer’s Disease. Sci. Rep. 2021, 11, 2660. [Google Scholar] [CrossRef]
- Essemlali, A.; St-Onge, E.; Descoteaux, M.; Jodoin, P.-M. Understanding Alzheimer Disease’s Structural Connectivity through Explainable AI. Proc. Mach. Learn. Res. 2020, 121, 217–229. [Google Scholar]
- Kamal, M.S.; Northcote, A.; Chowdhury, L.; Dey, N.; Crespo, R.G.; Herrera-Viedma, E. Alzheimer’s Patient Analysis Using Image and Gene Expression Data and Explainable-AI to Present Associated Genes. IEEE Trans. Instrum. Meas. 2021, 70. [Google Scholar] [CrossRef]
- Varzandian, A.; Razo, M.A.S.; Sanders, M.R.; Atmakuru, A.; Di Fatta, G. Classification-Biased Apparent Brain Age for the Prediction of Alzheimer’s Disease. Front. Neurosci. 2021, 15, 673120. [Google Scholar] [CrossRef]
- Iizuka, T.; Fukasawa, M.; Kameyama, M. Deep-Learning-Based Imaging-Classification Identified Cingulate Island Sign in Dementia with Lewy Bodies. Sci. Rep. 2019, 9, 8944. [Google Scholar] [CrossRef] [Green Version]
- Solano-Rojas, B.; Villalón-Fonseca, R. A Low-Cost Three-Dimensional DenseNet Neural Network for Alzheimer’s Disease Early Discovery. Sensors 2021, 21, 1302. [Google Scholar] [CrossRef] [PubMed]
- Tang, Z.; Chuang, K.V.; DeCarli, C.; Jin, L.-W.; Beckett, L.; Keiser, M.J.; Dugger, B.N. Interpretable Classification of Alzheimer’s Disease Pathologies with a Convolutional Neural Network Pipeline. Nat. Commun. 2019, 10, 2173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, X.; Han, L.; Zhu, W.; Sun, L.; Zhang, D. An Explainable 3D Residual Self-Attention Deep Neural Network for Joint Atrophy Localization and Alzheimer’s Disease Diagnosis Using Structural MRI. IEEE J. Biomed. Health Inform. 2021. [Google Scholar] [CrossRef] [PubMed]
- Jiang, F.; Jiang, Y.; Zhi, H.; Dong, Y.; Li, H.; Ma, S.; Wang, Y.; Dong, Q.; Shen, H.; Wang, Y. Artificial Intelligence in Healthcare: Past, Present and Future. Stroke Vasc. Neurol. 2017, 2, 230–243. [Google Scholar] [CrossRef]
- Kumar, Y.; Koul, A.; Singla, R.; Ijaz, M.F. Artificial Intelligence in Disease Diagnosis: A Systematic Literature Review, Synthesizing Framework and Future Research Agenda. J. Ambient Intell. Humaniz. Comput. 2022. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Train (n) | Validation (n) | Test (n) |
|---|---|---|---|
| FTD | 143 | 19 | 20 |
| NC | 91 | 19 | 20 |
| Transformation | Description | Probability of Application | Specs |
|---|---|---|---|
| Translation | Translate voxels for every spatial dimension. | 1 | ±2 voxels |
| Rotation | Randomly rotate the input arrays. | 1 | ±5 degrees on the x-axis |
| Gaussian noise | Add Gaussian noise to the image. | 0.5 | Mean = 0; standard deviation = 2.5% of the range of activation values in the image |
| Contrast adjustment | Randomly updates each voxel intensity by gamma. | 1 | Gamma range = (0.0, 3.0) |
| Group | Original Images (n) | Augmented Images (n) | Total |
|---|---|---|---|
| FTD | 143 | 257 | 400 |
| NC | 91 | 309 | 400 |
| Total | 234 | 566 | 800 |
| Citation | Comparison | Sample Size | Classification Method | Features | Metric |
|---|---|---|---|---|---|
| Proposed application | FTD vs. NC | 182 FTD 130 NC | HOTS DenseNet121 | 3D T1 MRI scans | Acc = 0.80 |
| Hu et al., 2020 [42] | FTD vs. NC | 552 FTD 354NC | HOTS CNN | Raw 3D T1 MRI images | Acc = 0.93 |
| Bron et al., 2017 [43] | FTD vs. NC | 33 FTD 34 NC | 4-fold CV SVM | Whole-brain VBM volume of GM | AUC = 0.95 |
| Zhang et al., 2013 [44] | FTD vs. NC | 25 FTD 19 NC | 4-fold CV SVM | VBM GM volume on frontotemporal ROI | Acc = 0.66 |
| Muñoz-Ruiz et al., 2012 [45] | FTD vs. NC | 37 FTD 26 NC | HOTS regression | VBM GM volume | Acc = 0.85 |
| Dukart et al., 2011 [46] | FTD vs. NC | 14 FTD 13 NC | LOOCV SVM | ROIs GM | Acc = 0.85 |
| Davatzikos et al., 2008 [36] | FTD vs. NC | 12 FTD 12 NC | LOOCV SVM | PCA on RAVENS GM and WM volume | Acc = 1 |
| Du et al., 2007 [37] | FTD vs. NC | 19 FTD 23 NC | LOOCV LR | Frontal volume | Acc = 0.89 |
| Chagué et al., 2021 [64] | FTD vs. Late Onset AD | 39 FTD 34 AD | 10-fold CV SVM | GM and WM volumes | Acc = 0.72 |
| Chagué et al., 2021 [64] | FTD vs. Early Onset AD | 39 FTD 34 AD | 10-fold CV SVM | GM and WM volumes | Acc = 0.80 |
| Bron et al., 2017 [43] | FTD vs. AD | 33 FTD 24 AD | 4-fold CV SVM | Whole-brain VBM volume of GM | AUC = 0.78 |
| McMillan et al., 2014 [65] | FTD vs. AD | 72 FTD 21 AD | HOTS linear regression | Global ventricles volume | AUC = 0.83 |
| Dukart et al., 2011 [46] | FTD vs. AD | 14 FTD 21 AD | LOOCV SVM | ROIs GM | Acc = 0.60 |
| Lehmann et al., 2010 [66] | FTD vs. AD | 23 FTD 17 AD | CV SVM | Whole brain cortical thickness | Acc = 0.79 |
| Davatzikos et al., 2008 [36] | FTD vs. AD | 12 FTD 37 AD | LOOCV SVM | PCA on RAVENS GM and WM volume | Acc = 0.84 |
| Klöppel et al., 2008 [67] | FTD vs. AD | 19 FTD 18 AD | LOOCV SVM | GM volume | Acc = 0.89 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Termine, A.; Fabrizio, C.; Caltagirone, C.; Petrosini, L.; on behalf of the Frontotemporal Lobar Degeneration Neuroimaging Initiative. A Reproducible Deep-Learning-Based Computer-Aided Diagnosis Tool for Frontotemporal Dementia Using MONAI and Clinica Frameworks. Life 2022, 12, 947. https://doi.org/10.3390/life12070947
Termine A, Fabrizio C, Caltagirone C, Petrosini L, on behalf of the Frontotemporal Lobar Degeneration Neuroimaging Initiative. A Reproducible Deep-Learning-Based Computer-Aided Diagnosis Tool for Frontotemporal Dementia Using MONAI and Clinica Frameworks. Life. 2022; 12(7):947. https://doi.org/10.3390/life12070947
Chicago/Turabian StyleTermine, Andrea, Carlo Fabrizio, Carlo Caltagirone, Laura Petrosini, and on behalf of the Frontotemporal Lobar Degeneration Neuroimaging Initiative. 2022. "A Reproducible Deep-Learning-Based Computer-Aided Diagnosis Tool for Frontotemporal Dementia Using MONAI and Clinica Frameworks" Life 12, no. 7: 947. https://doi.org/10.3390/life12070947
APA StyleTermine, A., Fabrizio, C., Caltagirone, C., Petrosini, L., & on behalf of the Frontotemporal Lobar Degeneration Neuroimaging Initiative. (2022). A Reproducible Deep-Learning-Based Computer-Aided Diagnosis Tool for Frontotemporal Dementia Using MONAI and Clinica Frameworks. Life, 12(7), 947. https://doi.org/10.3390/life12070947