
Changes in the Mean of Medical Visits Due to Psychiatric Disease in Korean Children and Adolescents before and during the COVID-19 Pandemic

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics
2.2. Participants and Measurements
2.3. Statistics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dubey, S.; Biswas, P.; Ghosh, R.; Chatterjee, S.; Dubey, M.J.; Chatterjee, S.; Lahiri, D.; Lavie, C.J. Psychosocial Impact of COVID-19. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 779–788. [Google Scholar] [CrossRef] [PubMed]
- Park, J.-H.; Jang, W.; Kim, S.-W.; Lee, J.; Lim, Y.-S.; Cho, C.-G.; Park, S.-W.; Kim, B.H. The Clinical Manifestations and Chest Computed Tomography Findings of Coronavirus Disease 2019 (COVID-19) Patients in China: A Proportion Meta-Analysis. Clin. Exp. Otorhinolaryngol. 2020, 13, 95–105. [Google Scholar] [CrossRef] [PubMed]
- Lee, J. Mental Health Effects of School Closures During COVID-19. Lancet Child Adolesc. Health 2020, 4, 421. [Google Scholar] [CrossRef]
- Ghosh, R.; Dubey, M.J.; Chatterjee, S.; Dubey, S. Impact of COVID-19 on Children: Special Focus on the Psychosocial Aspect. Minerva Pediatr. 2020, 72, 226–235. [Google Scholar] [CrossRef] [PubMed]
- Zhu, K.; Xie, X.; Liu, Q.; Meng, H.; Song, R. Internet Addiction: Prevalence and Relationship with Academic Burnout Among Undergraduates During Widespread Online Learning. Perspect. Psychiatr. Care 2022. online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Dalton, L.; Rapa, E.; Stein, A. Protecting the Psychological Health of Children through Effective Communication about COVID-19. Lancet Child Adolesc. Health 2020, 4, 346–347. [Google Scholar] [CrossRef]
- Herringa, R.J. Trauma, PTSD, and the Developing Brain. Curr. Psychiatry Rep. 2017, 19, 69. [Google Scholar] [CrossRef]
- Meade, J. Mental Health Effects of the COVID-19 Pandemic on Children and Adolescents. Pediatr. Clin. North Am. 2021, 68, 945–959. [Google Scholar] [CrossRef]
- Meherali, S.; Punjani, N.; Louie-Poon, S.; Rahim, K.A.; Das, J.; Salam, R.; Lassi, Z. Mental Health of Children and Adolescents Amidst COVID-19 and Past Pandemics: A Rapid Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 3432. [Google Scholar] [CrossRef]
- Kim, S.Y.; Kim, H.-R.; Park, B.; Choi, H.G. Comparison of Stress and Suicide-Related Behaviors Among Korean Youths Before and During the COVID-19 Pandemic. JAMA Netw. Open 2021, 4, e2136137. [Google Scholar] [CrossRef]
- Pizarro-Ruiz, J.P.; Ordóñez-Camblor, N. Effects of Covid-19 Confinement on the Mental Health of Children and Adolescents in Spain. Sci. Rep. 2021, 11, 11713. [Google Scholar] [CrossRef] [PubMed]
- Nordstokke, D.; Zumbo, B.D. A New Nonparametric Levene Test for Equal Variances. Psicológica 2010, 31, 401–430. [Google Scholar]
- Tang, S.; Xiang, M.; Cheung, T.; Xiang, Y.-T. Mental Health and Its Correlates Among Children and Adolescents During COVID-19 School Closure: The Importance of Parent-Child Discussion. J. Affect. Disord. 2021, 279, 353–360. [Google Scholar] [CrossRef] [PubMed]
- Panda, P.K.; Gupta, J.; Chowdhury, S.R.; Kumar, R.; Meena, A.K.; Madaan, P.; Sharawat, I.K.; Gulati, S. Psychological and Behavioral Impact of Lockdown and Quarantine Measures for COVID-19 Pandemic on Children, Adolescents and Caregivers: A Systematic Review and Meta-Analysis. J. Trop. Pediatr. 2021, 67, fmaa122. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.Y.; Ro, Y.S.; Jeong, J.; Shin, S.D.; Moon, S. Impact of the COVID-19 Pandemic on the Incidence and Characteristics of Patients with Psychiatric Illnesses Visiting Emergency Departments in Korea. J. Clin. Med. 2022, 11, 488. [Google Scholar] [CrossRef]
- Colizzi, M.; Sironi, E.; Antonini, F.; Ciceri, M.L.; Bovo, C.; Zoccante, L. Psychosocial and Behavioral Impact of COVID-19 in Autism Spectrum Disorder: An Online Parent Survey. Brain Sci. 2020, 10, 341. [Google Scholar] [CrossRef]
- Shuai, L.; He, S.; Zheng, H.; Wang, Z.; Qiu, M.; Xia, W.; Cao, X.; Lu, L.; Zhang, J. Influences of Digital Media Use on Children and Adolescents with ADHD During COVID-19 Pandemic. Glob. Health 2021, 17, 48. [Google Scholar] [CrossRef]
- Duan, L.; Shao, X.; Wang, Y.; Huang, Y.; Miao, J.; Yang, X.; Zhu, G. An Investigation of Mental Health Status of Children and Adolescents in China During the Outbreak of COVID-19. J. Affect. Disord. 2020, 275, 112–118. [Google Scholar] [CrossRef]
- Kozloff, N.; Mulsant, B.H.; Stergiopoulos, V.; Voineskos, A.N. The COVID-19 Global Pandemic: Implications for People with Schizophrenia and Related Disorders. Schizophr. Bull. 2020, 46, 752–757. [Google Scholar] [CrossRef]
- Correll, C.U.; Chepke, C.; Gionfriddo, P.; Parks, J.; Foxworth, P.; Basu, A.; Brister, T.S.; Brown, D.; Clarke, C.; Hassoun, Y. The Post COVID-19 Healthcare Landscape and the Use of Long-Acting Injectable Antipsychotics for Individuals with Schizophrenia and Bipolar I Disorder: The Importance of an Integrated Collaborative-Care Approach. BMC Psychiatry 2022, 22, 32. [Google Scholar] [CrossRef]
- Fond, G.; Nemani, K.; Etchecopar-Etchart, D.; Loundou, A.; Goff, D.C.; Lee, S.W.; Lancon, C.; Auquier, P.; Baumstarck, K.; Llorca, P.-M.; et al. Association Between Mental Health Disorders and Mortality Among Patients With COVID-19 in 7 Countries. JAMA Psychiatry 2021, 78, 1208. [Google Scholar] [CrossRef] [PubMed]
- Kahve, A.C.; Kaya, H.; Darben, Y.; Cakil, A.G.; Goka, E. From Predictions to Evidence: Treatment Compliance, Disease Progression and Social Compliance of Patients with Schizophrenia in the COVID-19 Pandemic. Perspect. Psychiatr. Care 2021, 57, 1991–1998. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, S.J.; Barblan, L.P.; Lory, I.; Landolt, M.A. Age-Related Effects of the COVID-19 Pandemic on Mental Health of Children and Adolescents. Eur. J. Psychotraumatol. 2021, 12, 1901407. [Google Scholar] [CrossRef]
- Kim, S.Y.; Kim, D.W. Does the Clinical Spectrum of Coronavirus Disease 2019 (COVID-19) Show Regional Differences? Clin. Exp. Otorhinolaryngol. 2020, 13, 83–84. [Google Scholar] [CrossRef]
- Kurisu, K.; Matsuoka, M.; Sato, K.; Hattori, A.; Yamanaka, Y.; Nohara, N.; Otani, M.; Yoshiuchi, K. Increased Prevalence of Eating Disorders in Japan since the Start of the COVID-19 Pandemic. Eat. Weight Disord. Stud. Anorexia Bulim. Obes. 2021, 1–5, online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Ransing, R.; Ramalho, R.; de Filippis, R.; Ojeahere, M.I.; Karaliuniene, R.; Orsolini, L.; da Costa, M.P.; Ullah, I.; Grandinetti, P.; Bytyçi, D.G.; et al. Infectious Disease Outbreak Related Stigma and Discrimination During the COVID-19 Pandemic: Drivers, Facilitators, Manifestations, and Outcomes across the World. Brain Behav. Immun. 2020, 89, 555–558. [Google Scholar] [CrossRef] [PubMed]
- Aamir, A.; Awan, S.; de Filippis, R.; Diwan, M.N.; Ullah, I. Effect of COVID-19 on Mental Health Rehabilitation Centers. J. Psychosoc. Rehabil. Ment. Health 2021, 8, 97–100. [Google Scholar] [CrossRef]

{kind=link}
| Diseases | Before COVID-19 | During COVID-19 | p-Values of Difference | |||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | Variance | |
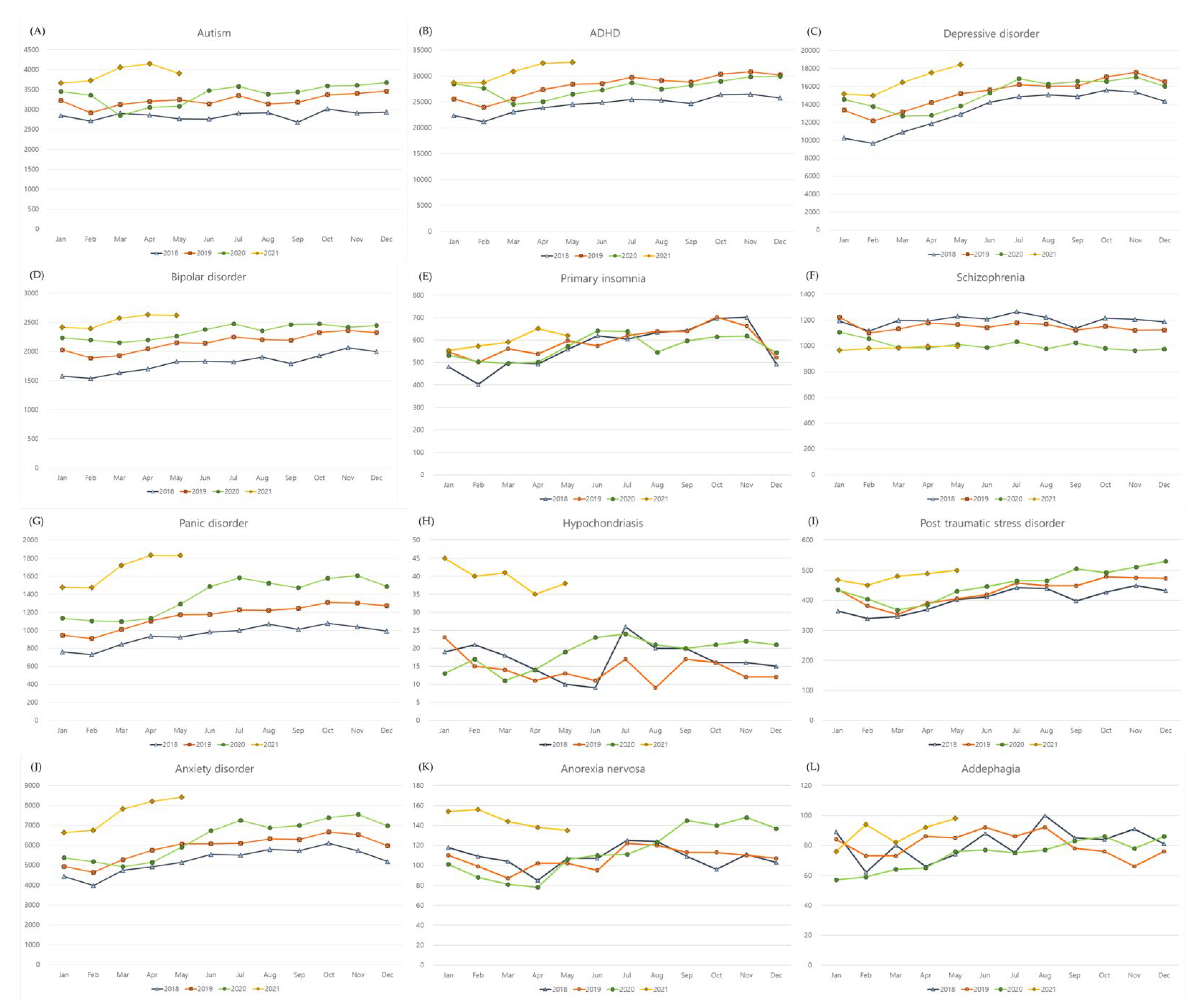
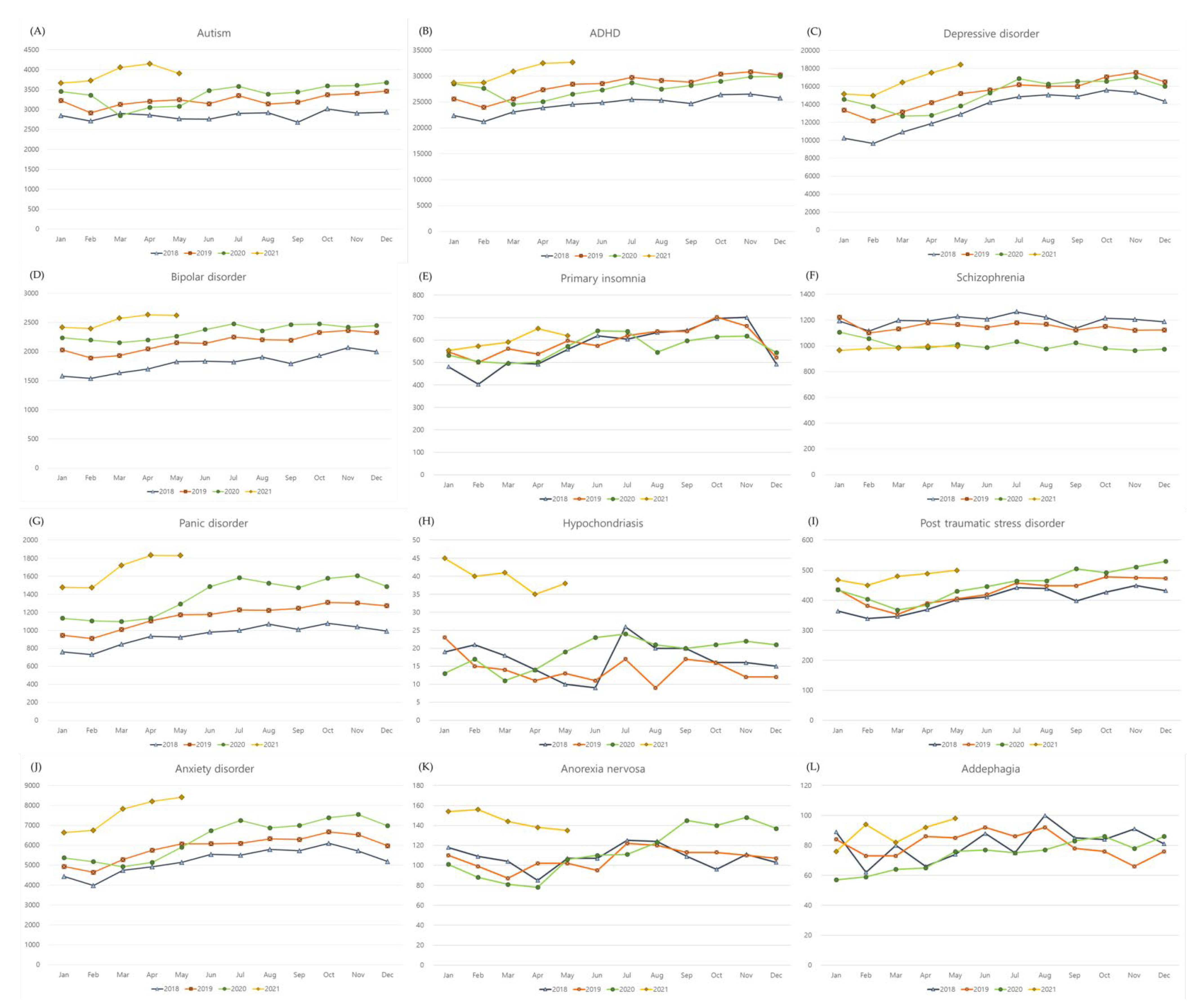
| Autism | 3070.6 | 243.1 | 3550.6 | 359.1 | <0.001 * | 0.936 |
| ADHD | 26498.2 | 2600.5 | 28667.8 | 2332.6 | 0.021 * | 0.480 |
| Depressive disorder | 14273.1 | 2036.9 | 15748.9 | 1656.6 | 0.021 * | 0.856 |
| Bipolar disorder | 1996.0 | 237.7 | 2416.7 | 138.2 | <0.001 * | 0.140 |
| Primary insomnia | 575.5 | 77.9 | 583.9 | 48.5 | 0.745 | 0.037 † |
| Schizophrenia | 1166.4 | 48.9 | 989.1 | 19.7 | <0.001 * | 0.014 † |
| Panic disorder | 1058.0 | 158.5 | 1507.1 | 213.1 | <0.001 * | 0.159 |
| Hypochondriasis | 15.5 | 4.3 | 26.3 | 10.6 | <0.001 * | 0.796 |
| Post traumatic stress disorder | 416.2 | 40.1 | 465.5 | 45.1 | 0.001 * | 0.766 |
| Anxiety disorder | 5536.6 | 675.1 | 6902.7 | 990.8 | <0.001 * | 0.739 |
| Anorexia nervosa | 106.4 | 10.8 | 127.1 | 24.8 | 0.003 * | 0.106 |
| Adephagia | 79.2 | 10.9 | 80.6 | 9.6 | 0.725 | 0.496 |
| Diseases | Before COVID-19 | During COVID-19 | p-Values of Difference | |||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | Variance | |
| Men | ||||||
| Autism | 2595.8 | 201.1 | 2960.7 | 288.3 | <0.001 * | 0.892 |
| ADHD | 21881.1 | 2099.7 | 23093.9 | 1780.9 | 0.093 | 0.187 |
| Depressive disorder | 5427.6 | 630.5 | 5929.5 | 585.5 | 0.014 * | 0.709 |
| Bipolar disorder | 929.0 | 91.7 | 1054.8 | 44.4 | <0.001 * | 0.263 |
| Primary insomnia | 281.3 | 39.5 | 271.7 | 32.3 | 0.379 | 0.763 |
| Schizophrenia | 594.3 | 24.1 | 503.8 | 13.9 | <0.001 * | 0.014 † |
| Panic disorder | 469.8 | 58.6 | 643.7 | 78.8 | <0.001 * | 0.113 |
| Hypochondriasis | 10.0 | 3.4 | 14.1 | 3.4 | 0.001 * | 0.871 |
| Post traumatic stress disorder | 158.8 | 17.1 | 170.3 | 17.8 | 0.066 | 0.762 |
| Anxiety disorder | 2663.4 | 255.7 | 3186.3 | 411.4 | <0.001 * | 0.542 |
| Anorexia nervosa | 13.0 | 2.9 | 12.2 | 3.0 | 0.295 | 0.611 |
| Adephagia | 12.6 | 5.0 | 11.0 | 3.0 | 0.497 | 0.443 |
| Women | ||||||
| Autism | 474.8 | 44.6 | 589.9 | 71.8 | <0.001 * | 0.353 |
| ADHD | 4617.1 | 507.0 | 5573.9 | 562.3 | <0.001 * | 0.425 |
| Depressive disorder | 8845.5 | 1416.1 | 9819.5 | 1074.3 | 0.021 * | 0.973 |
| Bipolar disorder | 1067.0 | 148.0 | 1361.9 | 98.2 | <0.001 * | 0.101 |
| Primary insomnia | 294.2 | 44.3 | 312.2 | 21.9 | 0.159 | 0.003 † |
| Schizophrenia | 572.1 | 27.9 | 485.3 | 10.7 | <0.001 * | 0.017 † |
| Panic disorder | 588.2 | 100.7 | 863.4 | 137.4 | <0.001 * | 0.165 |
| Hypochondriasis | 5.6 | 2.4 | 12.2 | 8.1 | 0.006 * | 0.727 |
| Post traumatic stress disorder | 257.4 | 28.5 | 295.3 | 29.0 | <0.001 * | 0.777 |
| Anxiety disorder | 2873.2 | 422.4 | 3716.3 | 585.5 | <0.001 * | 0.898 |
| Anorexia nervosa | 93.4 | 10.0 | 114.9 | 23.4 | 0.003 * | 0.081 |
| Adephagia | 66.5 | 9.6 | 69.6 | 8.1 | 0.464 | 0.828 |
| Diseases | Before COVID-19 | During COVID-19 | p-Values of Difference | |||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | Variance | |
| Age 0–4 years old | ||||||
| Autism | 300.3 | 29.7 | 384.9 | 74.1 | <0.001 * | 0.526 |
| ADHD | 94.8 | 16.4 | 118.9 | 35.9 | 0.026 * | 0.380 |
| Depressive disorder | 14.2 | 4.7 | 8.5 | 2.5 | <0.001 * | 0.140 |
| Bipolar disorder | 2.1 | 1.3 | 2.3 | 1.3 | 0.592 | 0.651 |
| Primary insomnia | 12.6 | 3.9 | 14.5 | 5.1 | 0.187 | 0.562 |
| Schizophrenia | 0.6 | 0.6 | 0.4 | 0.5 | 0.433 | 0.142 |
| Panic disorder | 0.3 | 0.5 | 0.5 | 0.6 | 0.130 | 0.036 † |
| Hypochondriasis | 0.5 | 0.9 | 0.5 | 0.7 | 0.715 | 0.539 |
| Post traumatic stress disorder | 9.2 | 3.0 | 7.7 | 3.5 | 0.196 | 0.277 |
| Anxiety disorder | 52.8 | 9.1 | 62.1 | 16.9 | 0.136 | 0.432 |
| Anorexia nervosa | 2.7 | 2.1 | 3.1 | 1.9 | 0.473 | 0.803 |
| Adephagia | 4.3 | 4.3 | 3.9 | 1.7 | 0.663 | <0.001 † |
| Age 5–9 years old | ||||||
| Autism | 1141.3 | 143.2 | 1421.1 | 180.5 | <0.001 * | 0.560 |
| ADHD | 9660.0 | 1334.1 | 10395.3 | 915.3 | 0.074 | 0.010 † |
| Depressive disorder | 324.0 | 43.3 | 367.2 | 47.2 | 0.007 * | 0.343 |
| Bipolar disorder | 45.7 | 9.1 | 60.3 | 3.8 | <0.001 * | 0.135 |
| Primary insomnia | 9.6 | 3.7 | 12.4 | 4.4 | 0.009 * | 0.178 |
| Schizophrenia | 8.8 | 2.0 | 9.1 | 3.0 | 0.891 | 0.160 |
| Panic disorder | 7.3 | 2.6 | 6.8 | 1.5 | 0.564 | 0.102 |
| Hypochondriasis | 0.5 | 0.7 | 1.1 | 1.0 | 0.074 | 0.122 |
| Post traumatic stress disorder | 41.8 | 5.7 | 42.3 | 7.1 | 0.989 | 0.360 |
| Anxiety disorder | 372.1 | 32.7 | 454.5 | 70.0 | <0.001 * | 0.422 |
| Anorexia nervosa | 3.2 | 2.2 | 5.5 | 2.3 | 0.003 * | 0.956 |
| Adephagia | 3.3 | 2.9 | 2.5 | 1.6 | 0.618 | 0.594 |
| Age 10–14 years old | ||||||
| Autism | 752.3 | 87.2 | 974.3 | 104.1 | <0.001 * | 0.145 |
| ADHD | 10797.7 | 916.1 | 11839.2 | 1088.5 | 0.004 * | 0.978 |
| Depressive disorder | 2550.7 | 454.4 | 2366.9 | 338.9 | 0.110 | 0.023 † |
| Bipolar disorder | 272.1 | 39.0 | 294.3 | 28.7 | 0.113 | 0.047 † |
| Primary insomnia | 37.5 | 4.6 | 40.1 | 7.4 | 0.316 | 0.195 |
| Schizophrenia | 80.8 | 8.0 | 86.9 | 10.7 | 0.042 * | 0.019 † |
| Panic disorder | 84.2 | 13.7 | 122.1 | 31.4 | 0.001 * | 0.368 |
| Hypochondriasis | 2.2 | 1.0 | 5.1 | 3.0 | 0.001 * | 0.200 |
| Post traumatic stress disorder | 98.9 | 18.4 | 109.9 | 17.8 | 0.070 | 0.608 |
| Anxiety disorder | 920.1 | 110.7 | 1133.1 | 216.6 | 0.001 * | 0.206 |
| Anorexia nervosa | 41.8 | 6.1 | 49.9 | 13.0 | 0.030 * | 0.023 † |
| Adephagia | 7.0 | 1.9 | 8.3 | 3.8 | 0.557 | 0.055 |
| Age 15–19 years old | ||||||
| Autism | 876.7 | 33.9 | 770.3 | 25.8 | <0.001 * | 0.018 † |
| ADHD | 5945.7 | 388.1 | 6314.5 | 375.9 | 0.003 * | 0.776 |
| Depressive disorder | 11384.3 | 1574.8 | 13006.3 | 1292.9 | 0.002 * | 0.861 |
| Bipolar disorder | 1676.0 | 197.1 | 2059.7 | 110.6 | <0.001 * | 0.094 |
| Primary insomnia | 515.8 | 77.2 | 517.0 | 43.2 | 0.935 | 0.010 † |
| Schizophrenia | 1076.3 | 43.4 | 892.7 | 26.2 | <0.001 * | 0.014 † |
| Panic disorder | 966.2 | 146.9 | 1377.7 | 184.0 | <0.001 * | 0.127 |
| Hypochondriasis | 12.4 | 4.3 | 19.7 | 6.9 | 0.001 * | 0.417 |
| Post traumatic stress disorder | 266.3 | 25.4 | 305.7 | 23.0 | <0.001 * | 0.612 |
| Anxiety disorder | 4191.5 | 541.5 | 5252.9 | 716.8 | <0.001 * | 0.975 |
| Anorexia nervosa | 58.7 | 5.8 | 68.6 | 10.7 | 0.001 * | 0.168 |
| Adephagia | 64.5 | 10.2 | 65.5 | 6.4 | 0.818 | 0.087 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.Y.; Lee, N.-E.; Yoo, D.M.; Kim, J.H.; Kwon, M.J.; Kim, J.-H.; Bang, W.J.; Choi, H.G. Changes in the Mean of Medical Visits Due to Psychiatric Disease in Korean Children and Adolescents before and during the COVID-19 Pandemic. Life 2022, 12, 600. https://doi.org/10.3390/life12040600
Kim SY, Lee N-E, Yoo DM, Kim JH, Kwon MJ, Kim J-H, Bang WJ, Choi HG. Changes in the Mean of Medical Visits Due to Psychiatric Disease in Korean Children and Adolescents before and during the COVID-19 Pandemic. Life. 2022; 12(4):600. https://doi.org/10.3390/life12040600
Chicago/Turabian StyleKim, So Young, Na-Eun Lee, Dae Myoung Yoo, Ji Hee Kim, Mi Jung Kwon, Joo-Hee Kim, Woo Jin Bang, and Hyo Geun Choi. 2022. "Changes in the Mean of Medical Visits Due to Psychiatric Disease in Korean Children and Adolescents before and during the COVID-19 Pandemic" Life 12, no. 4: 600. https://doi.org/10.3390/life12040600
APA StyleKim, S. Y., Lee, N.-E., Yoo, D. M., Kim, J. H., Kwon, M. J., Kim, J.-H., Bang, W. J., & Choi, H. G. (2022). Changes in the Mean of Medical Visits Due to Psychiatric Disease in Korean Children and Adolescents before and during the COVID-19 Pandemic. Life, 12(4), 600. https://doi.org/10.3390/life12040600