
Cardiac Rehabilitation in Peripheral Artery Disease in a Tertiary Center—Impact on Arterial Stiffness and Functional Status after 6 Months

 , , , ,
, , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Statistical Analysis
2.3. Ethics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Gerhard-Herman, M.D.; Gornik, H.L.; Barrett, C.; Barshes, N.R.; Corriere, M.A.; Drachman, D.E.; Fleisher, L.A.; Fowkes, F.G.R.; Hamburg, N.M.; Kinlay, S.; et al. 2016 AHA/ACC Guideline on the Management of Patients With Lower Extremity Peripheral Artery Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2017, 135, e726–e779. [Google Scholar] [CrossRef] [PubMed]
- Calabrese, M.; Garofano, M.; Palumbo, R.; Di Pietro, P.; Izzo, C.; Damato, A.; Venturini, E.; Iesu, S.; Virtuoso, N.; Strianese, A.; et al. Exercise Training and Cardiac Rehabilitation in COVID-19 Patients with Cardiovascular Complications: State of Art. Life 2021, 11, 259. [Google Scholar] [CrossRef] [PubMed]
- Hamburg, N.M.; Balady, G.J. Exercise Rehabilitation in Peripheral Artery Disease: Functional Impact and Mechanisms of Benefits. Circulation 2011, 123, 87–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Golledge, J.; Leicht, A.S.; Yip, L.; Rowbotham, S.E.; Pinchbeck, J.; Jenkins, J.S.; Clapperton, R.; Dally-Watkins, M.; Fiatarone Singh, M.A.; Mavros, Y.; et al. Relationship Between Disease Specific Quality of Life Measures, Physical Performance, and Activity in People with Intermittent Claudication Caused by Peripheral Artery Disease. Eur. J. Vasc. Endovasc. Surg. 2020, 59, 957–964. [Google Scholar] [CrossRef] [PubMed]
- Guidon, M.; McGee, H. Exercise-Based Interventions and Health-Related Quality of Life in Intermittent Claudication: A 20-Year (1989–2008) Review. Eur. J. Cardiovasc. Prev. Rehabil. 2010, 17, 140–154. [Google Scholar] [CrossRef] [PubMed]
- Laurent, S.; Boutouyrie, P.; Asmar, R.; Gautier, I.; Laloux, B.; Guize, L.; Ducimetiere, P.; Benetos, A. Aortic Stiffness Is an Independent Predictor of All-Cause and Cardiovascular Mortality in Hypertensive Patients. Hypertension 2001, 37, 1236–1241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitchell, G.F.; Hwang, S.-J.; Vasan, R.S.; Larson, M.G.; Pencina, M.J.; Hamburg, N.M.; Vita, J.A.; Levy, D.; Benjamin, E.J. Arterial Stiffness and Cardiovascular Events: The Framingham Heart Study. Circulation 2010, 121, 505–511. [Google Scholar] [CrossRef] [Green Version]
- Zahner, G.J.; Gruendl, M.A.; Spaulding, K.A.; Schaller, M.S.; Hills, N.K.; Gasper, W.J.; Grenon, S.M. Association between Arterial Stiffness and Peripheral Artery Disease as Measured by Radial Artery Tonometry. J. Vasc. Surg. 2017, 66, 1518–1526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kals, J.; Lieberg, J.; Kampus, P.; Zagura, M.; Eha, J.; Zilmer, M. Prognostic Impact of Arterial Stiffness in Patients with Symptomatic Peripheral Arterial Disease. Eur. J. Vasc. Endovasc. Surg. 2014, 48, 308–315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Protogerou, A.; Stergiou, G.; Vlachopoulos, C.; Blacher, J.; Achimastos, A. The Effect of Antihypertensive Drugs on Central Blood Pressure Beyond Peripheral Blood Pressure. Part II: Evidence for Specific Class-Effects of Antihypertensive Drugs on Pressure Amplification. Curr. Pharm. Des. 2009, 15, 272–289. [Google Scholar] [CrossRef]
- Claridge, M.W.; Bate, G.R.; Hoskins, P.R.; Adam, D.J.; Bradbury, A.W.; Wilmink, A.B. Measurement of Arterial Stiffness in Subjects with Vascular Disease: Are Vessel Wall Changes More Sensitive than Increase in Intima–Media Thickness? Atherosclerosis 2009, 205, 477–480. [Google Scholar] [CrossRef] [PubMed]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the Management of Arterial Hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Stevens, P.E. Evaluation and Management of Chronic Kidney Disease: Synopsis of the Kidney Disease: Improving Global Outcomes 2012 Clinical Practice Guideline. Ann. Intern. Med. 2013, 158, 825. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khwaja, A. KDIGO Clinical Practice Guidelines for Acute Kidney Injury. Nephron 2012, 120, c179–c184. [Google Scholar] [CrossRef]
- American Diabetes Association 6. Glycemic Targets: Standards of Medical Care in Diabetes—2020. Diabetes Care 2020, 43, S66–S76. [Google Scholar] [CrossRef] [PubMed]
- Dolan, E.; Li, Y.; Thijs, L.; McCormack, P.; Staessen, J.A.; O’Brien, E.; Stanton, A. Ambulatory Arterial Stiffness Index: Rationale and Methodology. Blood Press. Monit. 2006, 11, 103–105. [Google Scholar] [CrossRef]
- Hardman, R.L.; Jazaeri, O.; Yi, J.; Smith, M.; Gupta, R. Overview of Classification Systems in Peripheral Artery Disease. Semin Intervent Radiol. 2014, 31, 378–388. [Google Scholar] [CrossRef] [Green Version]
- Taylor, S.M. Gaps in Public Knowledge of Peripheral Arterial Disease: The First National PAD Public Awareness Survey. Circulation 2007, 116, 2086–2094, Corrected in Perspect. Vasc. Surg. Endovasc. Ther. 2008, 20, 314–316. [Google Scholar] [CrossRef]
- Wenger, N.K. Women and Coronary Heart Disease: A Century after Herrick: Understudied, Underdiagnosed, and Undertreated. Circulation 2012, 126, 604–611. [Google Scholar] [CrossRef] [Green Version]
- Laurent, S.; Boutouyrie, P. Arterial Stiffness and Hypertension in the Elderly. Front. Cardiovasc. Med. 2020, 7, 544302. [Google Scholar] [CrossRef] [PubMed]
- Bulugahapitiya, U.; Siyambalapitiya, S.; Sithole, J.; Idris, I. Is Diabetes a Coronary Risk Equivalent? Systematic Review and Meta-Analysis. Diabet. Med. 2009, 26, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Hap, K.; Biernat, K.; Konieczny, G. Patients with Diabetes Complicated by Peripheral Artery Disease: The Current State of Knowledge on Physiotherapy Interventions. J. Diabetes Res. 2021, 2021, 5122494. [Google Scholar] [CrossRef] [PubMed]
- Zheng, M.; Zhang, X.; Chen, S.; Song, Y.; Zhao, Q.; Gao, X.; Wu, S. Arterial Stiffness Preceding Diabetes: A Longitudinal Study. Circ. Res. 2020, 127, 1491–1498. [Google Scholar] [CrossRef]
- Kim, J.M.; Kim, S.S.; Kim, I.J.; Kim, J.H.; Kim, B.H.; Kim, M.K.; Lee, S.H.; Lee, C.W.; Kim, M.C.; Ahn, J.H.; et al. Relationship between Cardiovascular disease and Brachial-ankle Pulse Wave Velocity (baPWV) in Patients with Type 2 Diabetes (REBOUND) Study Group. Arterial stiffness is an independent predictor for risk of mortality in patients with type 2 diabetes mellitus: The REBOUND study. Cardiovasc. Diabetol. 2020, 19, 143. [Google Scholar] [CrossRef]
- Patoulias, D.; Papadopoulos, C.; Stavropoulos, K.; Zografou, I.; Doumas, M.; Karagiannis, A. Prognostic Value of Arterial Stiffness Measurements in Cardiovascular Disease, Diabetes, and Its Complications: The Potential Role of Sodium-glucose Co-transporter-2 Inhibitors. J. Clin. Hypertens 2020, 22, 562–571. [Google Scholar] [CrossRef] [Green Version]
- Umpierre, D. Physical Activity Advice Only or Structured Exercise Training and Association With HbA 1c Levels in Type 2 Diabetes: A Systematic Review and Meta-Analysis. JAMA 2011, 305, 1790. [Google Scholar] [CrossRef] [Green Version]
- Benetos, A. Influence of Age, Risk Factors, and Cardiovascular and Renal Disease on Arterial Stiffness: Clinical Applications. Am. J. Hypertens. 2002, 15, 1101–1108. [Google Scholar] [CrossRef]
- Strasser, B.; Arvandi, M.; Pasha, E.P.; Haley, A.P.; Stanforth, P.; Tanaka, H. Abdominal Obesity Is Associated with Arterial Stiffness in Middle-Aged Adults. Nutr. Metab. Cardiovasc. Dis. 2015, 25, 495–502. [Google Scholar] [CrossRef]
- Sedaghat, S.; Dawkins Arce, F.G.; Verwoert, G.C.; Hofman, A.; Ikram, M.A.; Franco, O.H.; Dehghan, A.; Witteman, J.C.M.; Mattace-Raso, F. Association of Renal Function with Vascular Stiffness in Older Adults: The Rotterdam Study. Age Ageing 2014, 43, 827–833. [Google Scholar] [CrossRef] [Green Version]
- Husmann, M.; Jacomella, V.; Thalhammer, C.; Amann-Vesti, B.R. Markers of Arterial Stiffness in Peripheral Arterial Disease. Vasa 2015, 44, 341–348. [Google Scholar] [CrossRef] [PubMed]
- Kollias, A.; Stergiou, G.S.; Dolan, E.; O’Brien, E. Ambulatory Arterial Stiffness Index: A Systematic Review and Meta-Analysis. Atherosclerosis 2012, 224, 291–301. [Google Scholar] [CrossRef] [PubMed]
- Blacher, J.; Staessen, J.A.; Girerd, X.; Gasowski, J.; Thijs, L.; Liu, L.; Wang, J.G.; Fagard, R.H.; Safar, M.E. Pulse Pressure Not Mean Pressure Determines Cardiovascular Risk in Older Hypertensive Patients. Arch. Intern. Med. 2000, 160, 1085. [Google Scholar] [CrossRef] [PubMed]
- Mone, P.; Kansakar, U.; Varzideh, F.; Boccalone, E.; Lombardi, A.; Pansini, A.; Santulli, G. Epidemiology of Obstructive Sleep Apnea: What Is the Contribution of Hypertension and Arterial Stiffness? J. Clin. Hypertens. 2022, 24, 395–397. [Google Scholar] [CrossRef] [PubMed]
- Safar, M.E. Arterial Stiffness as a Risk Factor for Clinical Hypertension. Nat. Rev. Cardiol. 2018, 15, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Zhao, X.; Wu, H. Arterial Stiffness: A Focus on Vascular Calcification and Its Link to Bone Mineralization. Arterioscler. Thromb. Vasc. Biol. 2020, 40, 1078–1093. [Google Scholar] [CrossRef]
- Cocciolone, A.J.; Hawes, J.Z.; Staiculescu, M.C.; Johnson, E.O.; Murshed, M.; Wagenseil, J.E. Elastin, Arterial Mechanics, and Cardiovascular Disease. Am. J. Physiol. Heart Circ. Physiol. 2018, 315, H189–H205. [Google Scholar] [CrossRef]
- Safar, M.E. Arterial Stiffness and Peripheral Arterial Disease. In Advances in Cardiology; Safar, M.E., Frohlich, E.D., Eds.; KARGER: Basel, Switzerland, 2006; Volume 44, pp. 199–211. ISBN 978-3-8055-8176-9. [Google Scholar]
- Gambardella, J.; Wang, X.; Mone, P.; Khondkar, W.; Santulli, G. Genetics of Adrenergic Signaling Drives Coronary Artery Calcification. Atherosclerosis 2020, 310, 88–90. [Google Scholar] [CrossRef]
- Wilkins, J.T.; McDermott, M.M.; Liu, K.; Chan, C.; Criqui, M.H.; Lloyd-Jones, D.M. Associations of Noninvasive Measures of Arterial Compliance and Ankle-Brachial Index: The Multi-Ethnic Study of Atherosclerosis (MESA). Am. J. Hypertens. 2012, 25, 535–541. [Google Scholar] [CrossRef]
- Duprez, D.; De Buyzere, M.; De Bruyne, L.; Clement, D.; Cohn, J. Small and Large Artery Elasticity Indices in Peripheral Arterial Occlusive Disease (PAOD). Vasc. Med. 2001, 6, 211–214. [Google Scholar] [CrossRef]
- Lee, M.; Choh, A.C.; Demerath, E.W.; Towne, B.; Siervogel, R.M.; Czerwinski, S.A. Associations Between Trunk, Leg and Total Body Adiposity with Arterial Stiffness. Am. J. Hypertens 2012, 25, 1131–1137. [Google Scholar] [CrossRef] [PubMed]
- Sparks, L.M.; Pasarica, M.; Sereda, O.; deJonge, L.; Thomas, S.; Loggins, H.; Xie, H.; Miles, J.M.; Smith, S.R. Effect of Adipose Tissue on the Sexual Dimorphism in Metabolic Flexibility. Metabolism 2009, 58, 1564–1571. [Google Scholar] [CrossRef] [PubMed]
- Wildman, R.P.; Mackey, R.H.; Bostom, A.; Thompson, T.; Sutton-Tyrrell, K. Measures of Obesity Are Associated With Vascular Stiffness in Young and Older Adults. Hypertension 2003, 42, 468–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montero, D.; Roberts, C.K.; Vinet, A. Effect of Aerobic Exercise Training on Arterial Stiffness in Obese Populations: A Systematic Review and Meta-Analysis. Sports Med. 2014, 44, 833–843. [Google Scholar] [CrossRef] [PubMed]
- Safar, M.E.; Czernichow, S.; Blacher, J. Obesity, Arterial Stiffness, and Cardiovascular Risk. J. Am. Soc. Nephrol. 2006, 17, S109–S111. [Google Scholar] [CrossRef]
- Marcell, T.J.; McAuley, K.A.; Traustadóttir, T.; Reaven, P.D. Exercise Training Is Not Associated with Improved Levels of C-Reactive Protein or Adiponectin. Metabolism 2005, 54, 533–541. [Google Scholar] [CrossRef]
- Howard, G. Cigarette Smoking and Progression of Atherosclerosis: The Atherosclerosis Risk in Communities (ARIC) Study. JAMA 1998, 279, 119. [Google Scholar] [CrossRef] [Green Version]
- Camplain, R.; Meyer, M.L.; Tanaka, H.; Palta, P.; Agarwal, S.K.; Aguilar, D.; Butler, K.R.; Heiss, G. Smoking Behaviors and Arterial Stiffness Measured by Pulse Wave Velocity in Older Adults: The Atherosclerosis Risk in Communities (ARIC) Study. Am. J. Hypertens. 2016, 29, 1268–1275. [Google Scholar] [CrossRef] [Green Version]
- Hennrikus, D.; Joseph, A.M.; Lando, H.A.; Duval, S.; Ukestad, L.; Kodl, M.; Hirsch, A.T. Effectiveness of a Smoking Cessation Program for Peripheral Artery Disease Patients. J. Am. Coll. Cardiol. 2010, 56, 2105–2112. [Google Scholar] [CrossRef] [Green Version]
- Fu, S.; Wu, Q.; Luo, L.; Ye, P. Relationships of Drinking and Smoking with Peripheral Arterial Stiffness in Chinese Community-Dwelling Population without Symptomatic Peripheral Arterial Disease. Tob. Induced Dis. 2017, 15, 39. [Google Scholar] [CrossRef]
- Doonan, R.J.; Hausvater, A.; Scallan, C.; Mikhailidis, D.P.; Pilote, L.; Daskalopoulou, S.S. The Effect of Smoking on Arterial Stiffness. Hypertens Res. 2010, 33, 398–410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kubozono, T.; Miyata, M.; Ueyama, K.; Hamasaki, S.; Kusano, K.; Kubozono, O.; Tei, C. Acute and Chronic Effects of Smoking on Arterial Stiffness. Circ. J. 2011, 75, 698–702. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scallan, C.; Doonan, R.J.; Daskalopoulou, S.S. The Combined Effect of Hypertension and Smoking on Arterial Stiffness. Clin. Exp. Hypertens. 2010, 32, 319–328. [Google Scholar] [CrossRef] [PubMed]
- Randomized Trial of the Effects of Cholesterol-Lowering with Simvastatin on Peripheral Vascular and Other Major Vascular Outcomes in 20,536 People with Peripheral Arterial Disease and Other High-Risk Conditions. J. Vasc. Surg. 2007, 45, 645–654.e1. [CrossRef] [PubMed] [Green Version]
- Hsu, C.-Y.; Chen, Y.-T.; Su, Y.-W.; Chang, C.-C.; Huang, P.-H.; Lin, S.-J. Statin Therapy Reduces Future Risk of Lower-Limb Amputation in Patients With Diabetes and Peripheral Artery Disease. J. Clin. Endocrinol. Metab. 2017, 102, 2373–2381. [Google Scholar] [CrossRef]
- Wang, L.; Zhi, F.; Gao, B.; Ni, J.; Liu, Y.; Mo, X.; Huang, J. Association between Lipid Profiles and Arterial Stiffness: A Secondary Analysis Based on a Cross-Sectional Study. J. Int. Med. Res. 2020, 48, 0300060520938188. [Google Scholar] [CrossRef]
- Kocyigit, I.; Kaya, M.G.; Orscelik, O.; Kaya, C.; Akpek, M.; Zengin, H.; Sipahioglu, M.H.; Unal, A.; Yilmaz, M.I.; Tokgoz, B.; et al. Early Arterial Stiffness and Inflammatory Bio-Markers in Normotensive Polycystic Kidney Disease Patients. Am. J. Nephrol. 2012, 36, 11–18. [Google Scholar] [CrossRef]
- Dias-Santos, E.G.; Farah, B.Q.; Germano-Soares, A.H.; Correia, M. de A.; Souza, A.A.; Hora, J.E.J.; Ritti-Dias, R.M.; Andrade-Lima, A. Effects of Exercise Mode on Arterial Stiffness in Symptomatic Peripheral Artery Disease Patients: A Randomized Crossover Clinical Trial. Ann. Vasc. Surg. 2021, 74, 382–388. [Google Scholar] [CrossRef]
- Brewer, L.C.; Chai, H.-S.; Bailey, K.R.; Kullo, I.J. Measures of Arterial Stiffness and Wave Reflection Are Associated with Walking Distance in Patients with Peripheral Arterial Disease. Atherosclerosis 2007, 191, 384–390. [Google Scholar] [CrossRef]
- Amoh-Tonto, C.A.; Malik, A.R.; Kondragunta, V.; Ali, Z.; Kullo, I.J. Brachial-Ankle Pulse Wave Velocity Is Associated with Walking Distance in Patients Referred for Peripheral Arterial Disease Evaluation. Atherosclerosis 2009, 206, 173–178. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, H.; Dinenno, F.A.; Monahan, K.D.; Clevenger, C.M.; DeSouza, C.A.; Seals, D.R. Aging, Habitual Exercise, and Dynamic Arterial Compliance. Circulation 2000, 102, 1270–1275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moreau, K. Regular Exercise, Hormone Replacement Therapy and the Age-Related Decline in Carotid Arterial Compliance in Healthy Women. Cardiovasc. Res. 2003, 57, 861–868. [Google Scholar] [CrossRef]
- Tanaka, H.; Safar, M. Influence of Lifestyle Modification on Arterial Stiffness and Wave Reflections. Am. J. Hypertens. 2005, 18, 137–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coutinho, T.; Rooke, T.W.; Kullo, I.J. Arterial Dysfunction and Functional Performance in Patients with Peripheral Artery Disease: A Review. Vasc. Med. 2011, 16, 203–211. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Parameter | Initial Evaluation (n = 97) | 6-Month Follow-Up (n = 97) | p Value |
|---|---|---|---|
| Anthropometric Parameters | |||
| Height, cm | 171.44 ± 8.77 | - | |
| Weight, kg | 83.72 ± 15.49 | 73.08 ± 13.52 | 0.708 |
| Body mass index, kg/m2 | 27.74 ± 3.65 | 24.14 ± 3.17 | 0.037 |
| Resting hemodynamics | |||
| Heart rate, bpm | 72.71 ± 12.28 | 68.55 ± 11.98 | 0.096 |
| Systolic BP, mmHg | 140.79 ± 21.56 | 134.73 ± 20.63 | 0.131 |
| Diastolic BP, mmHg | 80.15 ± 14.97 | 77.26 ± 14.43 | 0.485 |
| Sedentary lifestyle | 69 (71.1%) | 51 (52.6%) | 0.032 |
| Smoking | |||
| Active or in the past | 63 (64.9%) | 29 (29.9%) | <0.001 |
| Alcohol | 16 (16.5%) | 9 (9.3%) | 0.973 |
| Parameter | 6-Month Follow-Up (n = 97) | No Clinical Improvement after CR Program (n = 22) | With Clinical Improvement after CR (n = 75) | p Value |
|---|---|---|---|---|
| Comorbidities | ||||
| Hypertension | 61 (62.9%) | 20 (90.9%) | 41 (54.7%) | 0.002 |
| Diabetes mellitus | 56 (57.7%) | 19 (86.4%) | 37 (49.3%) | 0.002 |
| Dyslipidemia | 57 (58.8%) | 17 (77.3%) | 40 (53.3%) | 0.045 |
| Obesity | 61 (62.9%) | 15 (68.2%) | 46 (61.3%) | 0.564 |
| Coronary artery disease | 48 (49.5%) | 13 (59.1%) | 35 (46.7%) | 0.310 |
| Heart failure | 70 (72.2%) | 18 (81.8%) | 52 (69.3%) | 0.255 |
| COPD | 14 (14.4%) | 6 (27.3%) | 8 (10.7%) | 0.052 |
| Chronic kidney disease | 53 (54.6%) | 10 (45.5%) | 43 (57.3%) | 0.330 |
| Clinical picture—improvement of signs and symptoms | ||||
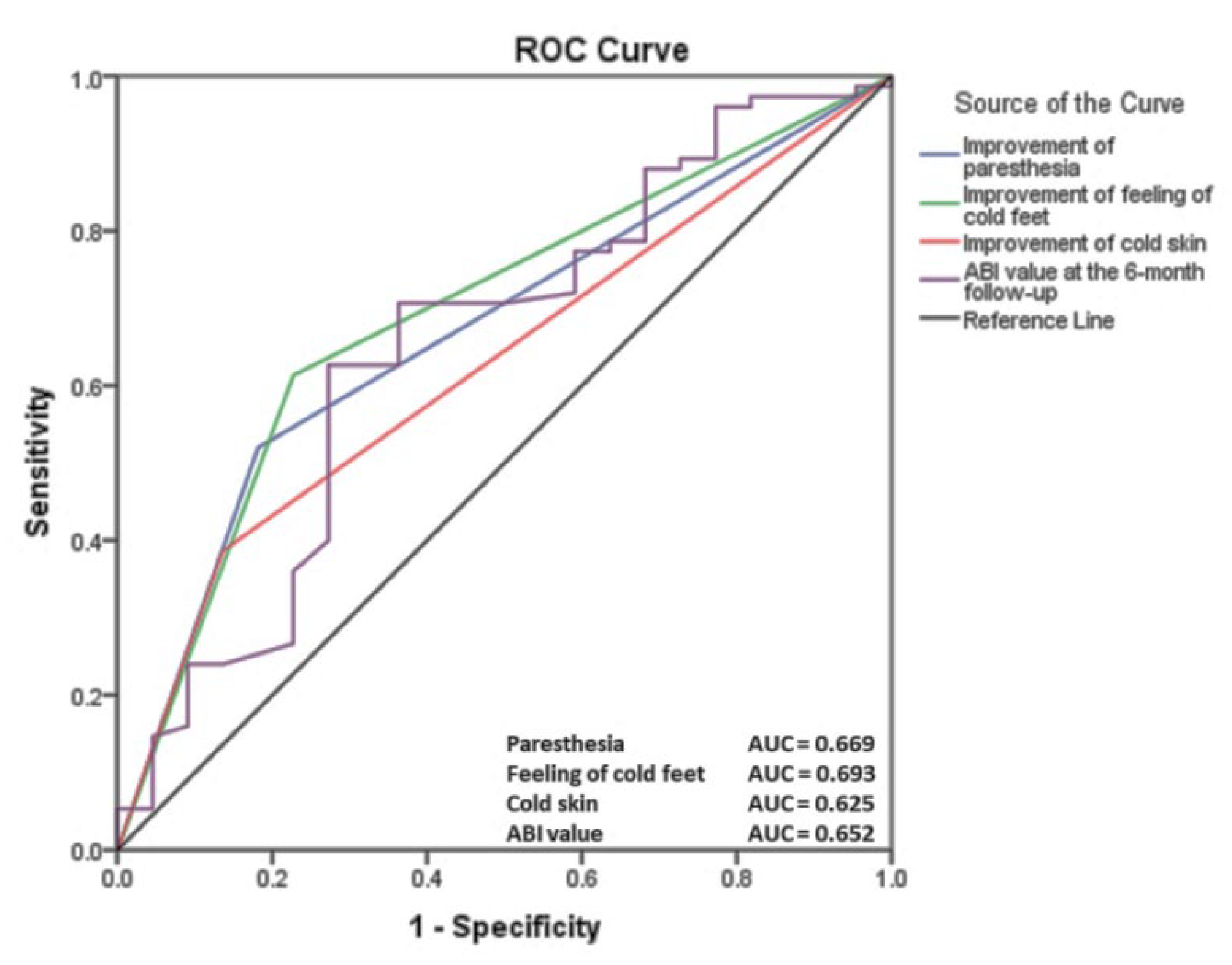
| Paresthesia | 43 (44.3%) | 4 (18.2%) | 39 (52.0%) | 0.005 |
| Feeling of cold feet | 51 (52.6%) | 5 (22.7%) | 46 (61.3%) | 0.001 |
| Pale skin | 35 (36.1%) | 9 (40.9%) | 26 (34.7%) | 0.596 |
| Cold skin | 32 (33.0%) | 3 (13.6%) | 29 (38.7%) | 0.028 |
| Reduced pilosity | 32 (33.0%) | 4 (18.2%) | 28 (37.3%) | 0.254 |
| Subcutaneous atrophy | 21 (21.6%) | 2 (9.1%) | 19 (25.3%) | 0.106 |
| Thickened nails | 22 (22.7%) | 3 (13.6%) | 19 (25.3%) | 0.254 |
| Petechiae | 21 (21.6%) | 4 (18.2%) | 17 (22.7%) | 0.657 |
| Arterial ulcers | 5 (5.2%) | 1 (4.5%) | 4 (5.3%) | 0.885 |
| Dermatitis | 12 (12.4%) | 3 (13.6%) | 9 (12.0%) | 0.840 |
| Quitting smoking | 29 (29.9%) | 15 (68.2%) | 61 (81.3%) | <0.001 |
| Active lifestyle | 51 (52.6%) | 16 (72.7%) | 35 (46.7%) | 0.032 |
| Parameter | Before CR | 6-Month Follow-Up (n = 97) | With Clinical Improvement after CR (n = 75) | No Clinical Improvement after CR Program (n = 22) | p Value |
|---|---|---|---|---|---|
| Blood biochemistry | |||||
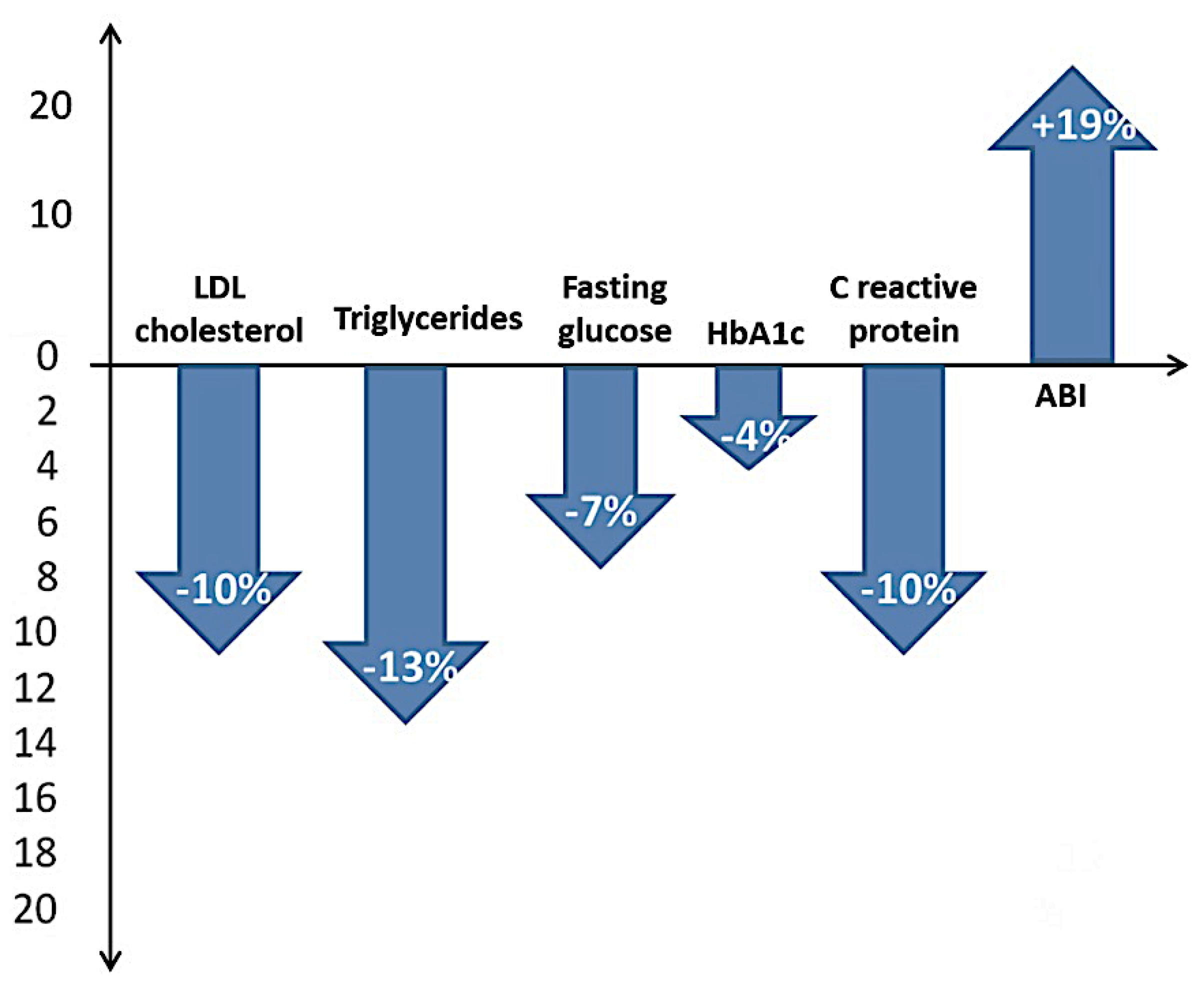
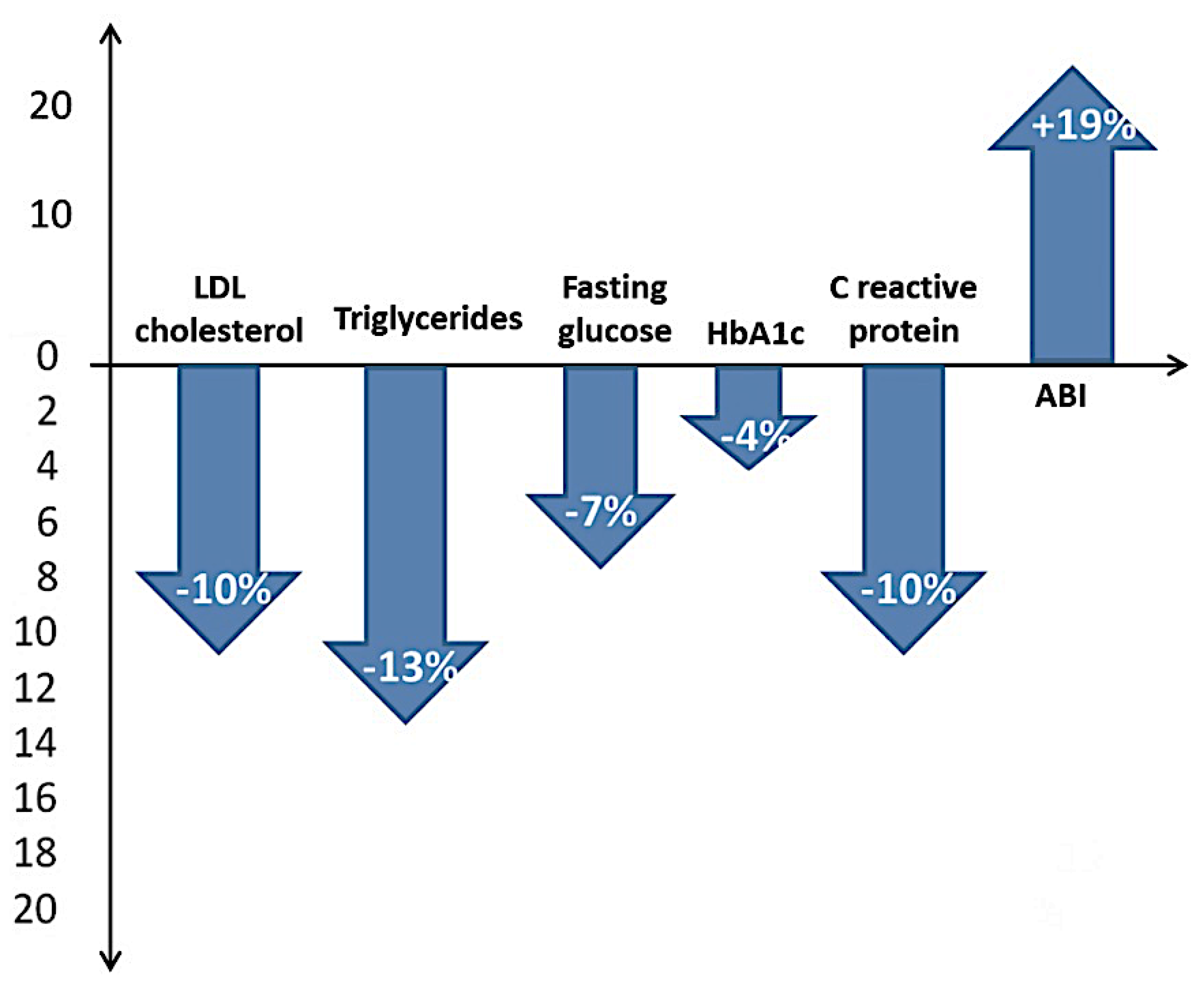
| Total cholesterol, mg/dL | 206.95 ± 75.90 | 172.92 ± 63.12 | 167.95 ± 58.19 | 189.88 ± 76.76 | 0.153 |
| LDL-cholesterol, mg/dL | 135.40 ± 67.79 | 121.86 ± 61.01 | 112.43 ± 43.58 | 154.02 ± 94.47 | 0.004 |
| HDL-cholesterol, mg/dL | 42.84 ± 16.92 | 44.56 ± 17.60 | 44.08 ± 18.66 | 46.18 ± 13.63 | 0.625 |
| Triglycerides, mg/dL | 185.27 ± 122.13 | 161.18 ± 106.26 | 145.10 ± 61.93 | 216.01 ± 184.46 | 0.005 |
| CRP, mg/dL | 5.33 ± 14.30 | 3.42 ± 5.07 | 2.87 ± 2.77 | 5.30 ± 9.26 | 0.047 |
| HbA1C, g% | 7.96 ± 2.23 | 7.64 ± 2.14 | 6.71 ± 1.35 | 10.75 ± 1.16 | <0.001 |
| Fasting glucose, mg/dL | 153.94 ± 63.54 | 146.51 ± 64.19 | 132.65 ± 43.85 | 193.13 ± 94.89 | <0.001 |
| Exercise stress test | |||||
| VO2 peak mL/kg/min | 12.34 ± 4.74 | 14.31 ± 4.74 | 14.95 ± 5.74 | 12.13 ± 3.94 | 0.034 |
| Peak HR, bpm | 118.61 ± 18.81 | 131.66 ± 20.88 | 132.66 ± 21.54 | 128.25 ± 18.48 | 0.386 |
| Peak systolic BP, mmHg | 171.52 ± 27.03 | 157.17 ± 19.78 | 154.94 ± 18.11 | 164.76 ± 23.55 | 0.040 |
| Peak diastolic BP, mmHg | 90.54 ± 13.31 | 88.73 ± 13.04 | 89.40 ± 13.46 | 86.46 ± 11.50 | 0.356 |
| RER | 1.07 ± 0.10 | 1.09 ± 0.10 | 1.076 ± 0.10 | 1.070 ± 0.10 | 0.820 |
| Borg scale | 15.45 ± 1.58 | 13.31 ± 1.14 | 13.12 ± 1.02 | 13.95 ± 1.29 | 0.002 |
| ABI | 0.65 ± 0.21 | 0.66 ± 0.23 | 0.84 ± 0.25 | 0.71 ± 0.24 | 0.031 |
| Walking distance, m | 246.43 ± 185.49 | 274.96 ± 175.52 | 291.33 ± 174.87 | 219.15 ± 169.84 | 0.046 |
| Echocardiography | |||||
| LVEF, % | 46.41 ± 9.74 | 49.37 ± 10.43 | 50.93 ± 9.93 | 44.03 ± 10.55 | 0.006 |
| Blood pressure monitoring, 24 h | |||||
| Systolic BP | 143.60 ± 21.99 | 135.42 ± 20.74 | 129.67 ± 15.52 | 138.27 ± 19.58 | 0.034 |
| Diastolic BP | 81.59 ± 15.24 | 77.59 ± 14.50 | 71.40 ± 11.32 | 79.28 ± 15.17 | 0.009 |
| Pulse pressure | 81.59 ± 15.24 | 77.59 ± 14.50 | 58.65 ± 11.54 | 51.62 ± 12.19 | 0.024 |
| AASI | 0.52 ± 0.18 | 0.46 ± 0.12 | 0.42 ± 0.19 | 0.47 ± 0.11 | 0.008 |
| Logistic Regression | |||
|---|---|---|---|
| Parameter | OR | p Value | 95% CI |
| Decreasing fasting glucose by at least 7% | 0.986 | 0.001 | 0.978–0.995 |
| Decreasing of HbA1C by at least 4% | 1.097 | 0.001 | 1.039–1.159 |
| Changing sedentary lifestyle | 0.328 | 0.036 | 0.116–0.930 |
| Ceasing smoking | 0.107 | <0.001 | 0.037–0.312 |
| Improvement of paresthesia | 4.875 | 0.008 | 1.507–15.775 |
| Improvement of feeling of cold feet | 5.393 | 0.003 | 1.795–16.204 |
| Improvement of cold skin | 3.993 | 0.037 | 1.085–14.699 |
| Decreasing LDL–cholesterol by at least 10% | 0.989 | 0.013 | 0.981–0.998 |
| Decreasing triglycerides by at least 13% | 0.994 | 0.026 | 0.988–0.999 |
| Increasing of ABI value | 10.753 | 0.034 | 1.196–96.685 |
| Increasing Borg Scale score | 0.446 | 0.004 | 0.259–0.769 |
| Increasing of VO2peak mL/kg/min | 1.138 | 0.040 | 1.006–1.287 |
| Decreasing of peak systolic BP, mmHg | 0.974 | 0.045 | 0.949–0.999 |
| Improvement of pulse pressure | 0.954 | 0.028 | 0.915–0.995 |
| Improvement of AASI | 1.127 | 0.021 | 1.069–1.105 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Anghel, R.; Adam, C.A.; Marcu, D.T.M.; Mitu, O.; Roca, M.; Tinica, G.; Mitu, F. Cardiac Rehabilitation in Peripheral Artery Disease in a Tertiary Center—Impact on Arterial Stiffness and Functional Status after 6 Months. Life 2022, 12, 601. https://doi.org/10.3390/life12040601
Anghel R, Adam CA, Marcu DTM, Mitu O, Roca M, Tinica G, Mitu F. Cardiac Rehabilitation in Peripheral Artery Disease in a Tertiary Center—Impact on Arterial Stiffness and Functional Status after 6 Months. Life. 2022; 12(4):601. https://doi.org/10.3390/life12040601
Chicago/Turabian StyleAnghel, Razvan, Cristina Andreea Adam, Dragos Traian Marius Marcu, Ovidiu Mitu, Mihai Roca, Grigore Tinica, and Florin Mitu. 2022. "Cardiac Rehabilitation in Peripheral Artery Disease in a Tertiary Center—Impact on Arterial Stiffness and Functional Status after 6 Months" Life 12, no. 4: 601. https://doi.org/10.3390/life12040601
APA StyleAnghel, R., Adam, C. A., Marcu, D. T. M., Mitu, O., Roca, M., Tinica, G., & Mitu, F. (2022). Cardiac Rehabilitation in Peripheral Artery Disease in a Tertiary Center—Impact on Arterial Stiffness and Functional Status after 6 Months. Life, 12(4), 601. https://doi.org/10.3390/life12040601